
Abstract
The number of HIV-positive people aged ≥50 years is rising each year. We measured the prevalence of non-infectious illnesses and their risk factors and described healthcare use in this UK population. A cross-sectional, observational study was conducted at an outpatient HIV specialist clinic in south east England. Patients age ≥50 years were invited to complete questionnaires measuring demographics, non-infectious illnesses, medication use, lifestyle and healthcare utilisation. The response rate was 67%. Of 299 participants, 84% reported ≥1 comorbid condition and 61% reported ≥2 (multimorbidity). Most commonly reported were high cholesterol, sexual dysfunction, hypertension and depression. In multivariate analyses, age, number of years HIV-positive and duration of antiretroviral therapy remained significant predictors of comorbidity when controlling for lifestyle factors (exercise, smoking and use of recreational drugs and alcohol). Use of non-HIV healthcare services was associated with increasing comorbidity, a longer duration of HIV and recreational drug use. The majority of HIV-patients aged ≥50 years reported multiple comorbidities and this was associated with polypharmacy and increased use of non-HIV services. Further research examining the quality, safety and patient experience of healthcare is needed to inform development of services to optimally meet the needs of older HIV-positive patients.
Keywords
Introduction
The number of older people living with HIV is increasing,1,2 due both to increased life expectancy with effective antiretroviral therapy (ART) and new infections.3,4 This changing demographic brings new demands to HIV care. While management has traditionally focused on viral load control and treatment of HIV-related infections, HIV services are increasingly involved with management of age-related illnesses including kidney disease, cardiovascular disease, cancer, osteoporosis and cognitive impairment.5–11
Large HIV cohort studies have described increasing rates of non-infectious diseases among older patients. The Veteran's Aging Cohort Study reported that patients aged ≥50 years were more likely than younger patients to experience hypertension, diabetes mellitus and vascular, pulmonary and renal diseases 12 while the Swiss Cohort Study reported increased prevalence of stroke, myocardial infarction, bone fractures, osteoporosis, diabetes mellitus and non-AIDS malignancies among patients aged ≥50 years, compared with those aged <50 years. 13 High levels of multimorbidity – the simultaneous presence of two or more comorbid illnesses – have also been reported.12,14
It has been postulated that HIV itself (even when suppressed) in combination with lifestyle factors and drug toxicities may lead to accelerated ageing. 15 Guaraldi et al. 14 found increased rates of individual comorbid conditions and multimorbidity among HIV-positive patients compared to an age, sex and ethnicity matched general population control group. Whether this difference was due to HIV infection, ART, or lifestyle factors is yet to be clearly defined 16 and is the subject of a number of current prospective studies.
There is currently a need for HIV services to be reconfigured to meet the needs of an ageing population. 17 However, to date, few studies have examined the use of healthcare services among this group. The aims of this study were, therefore, to determine rates of non-infectious comorbidities and multimorbidity, examine risk factors and describe use of healthcare services among HIV-positive patients aged ≥50 years attending an HIV outpatient clinic in south east England.
Methods
This cross-sectional, observational study was conducted at a specialist HIV outpatient clinic in Brighton, UK, between 2008 and 2010. Inclusion criteria were being HIV-positive and aged ≥50 years. The study was approved by the West Brighton Research Ethics Committee: Reference 08/H1111/65.
Eligible patients were informed about the study by their HIV physician. Those who expressed an interest in taking part were given written information and a pre-piloted questionnaire, to be completed either in the clinic or at home, for which a stamped addressed envelope was provided. Consent was gained to access patient notes to obtain clinical data (date of HIV diagnosis and cumulative number of years on ART) from the patient's medical files.
Measures
Each section of the self-report questionnaire included is described below.
Demographics
Participants were asked to indicate their gender, date of birth, sexuality (homosexual, heterosexual or bisexual) and relationship status (single, married, civil partnership, living with a partner, divorced, widowed).
Comorbid conditions
Participants were asked whether they were receiving treatment for high blood pressure, high cholesterol, angina (ischaemic heart disease), heart attack, stroke/transient ischaemic attack, diabetes, osteoporosis, arthritis, depression, memory problems, sexual dysfunction (e.g. erection problems or lack of interest in sex), cancer or prostatic symptoms. Free-text spaces were provided to record any other long-term, non-infectious conditions. Kidney disease and degenerative bone disease were subsequently included. The number of comorbidities was summed to make a continuous variable with possible scores ranging from 0 to 15. Consistent with other research, 14 multimorbidity was defined as the presence of two or more non-infectious comorbid conditions.
Non-HIV medications
Participants were asked to list their current prescription medications. The number of non-HIV medications was summed to make a continuous variable.
Health care utilisation
Participants were asked to indicate whether they were registered with a general practitioner (GP) and whether the GP knew of their HIV status. Participants were asked whether they had used the following services over the past 12 months: HIV specialist unit, GP, other hospital specialist, accident and emergency department, alternative health care professional (e.g. osteopath, acupuncturist), hospital admissions and whether the admission was HIV related. The number of health care services used was summed to make a continuous variable with possible scores ranging from 0 to 6. Participants were asked to indicate which of the following specialist hospital clinics they had attended: cardiology, dermatology, endocrinology/diabetes, ear nose and throat, gastroenterology, neurology, oncology, ophthalmology, orthopaedics, rheumatology, surgery, urology, elderly medicine, psychiatry. The number of specialist services used was summed to make a continuous variable with possible scores ranging from 0 to 14. Participants were asked to indicate which of the following investigations had been performed: blood pressure, chest X-ray, ECG, diabetes test, cholesterol blood test, bone density scan, sexual health screen, prostate blood test (prostate-specific antigen [PSA] test) or mammography (breast scan) (yes/no).
Lifestyle
Participants were asked how often they exercised; ≥3 times a week for 30 min or more (always [scored 4], most weeks [scored 3], occasionally [scored 2] or never [scored 1]), generating a scale with possible scores ranging from 1 to 4, where greater scores indicated a greater frequency of exercise. Participants were asked whether they were currently or had ever been a regular smoker (yes/no) and whether they used recreational drugs (yes/no). Those who had used recreational drugs were asked to state which. Participants were asked to indicate the number of shots of spirits, glasses of wine (175 ml) and pints of beer they consumed each week on average. The number of drinks was converted into units, where 1 = nil; 2 = 1–5 units; 3 = 6–10 units; 4 = 11–14 units; 5 = 15–20 units and 6 = 21+ units.
Statistical analysis
Data were analysed using SPSS version 22. Missing data were handled using listwise deletion, where participants with missing data on one or more variables were omitted. Pearson's correlations and t tests were used to determine associations between the total number of comorbidities/health care utilisation and demographic, clinical and lifestyle factors. Multivariate linear regression was used to determine the association between the number of comorbid conditions reported and other factors. Variables were included based on a conceptual model which proposes that the early onset of age-related conditions among people with HIV may be explained by combination of HIV, normal ageing, ART and behavioural factors including smoking, alcohol and recreational drug use. 15 Relationship status was also included in the regression because being single was significantly associated with comorbidity in the univariate analysis. Given the strong association between the duration of HIV diagnosis and duration of treatment with ART (r = 0.79), these two variables were not entered in the same analysis. Instead, separate regression analyses were run.
Multivariate linear regression was used to determine the association between healthcare utilisation and other factors. Variables were included based on Andersen's Behavioral Model,18,19 a theoretical framework developed explicitly for health service utilisation, which proposes that use of health services can be explained in terms of predisposing factors (age, gender, sexuality, ethnicity), enabling factors (relationship status was included as a proxy for social support) and need factors (number of comorbid conditions, duration of HIV diagnosis, smoking, drug and alcohol use).
Results
Sample characteristics
Of 443 study eligible patients, 320 (72.2%) consented to take part and 299 (67.4%) returned fully completed questionnaires and were included in the analysis. The mean age of participants was 58.0 (standard deviation [SD] = 2.0). The majority of participants were men (283; 94.6%) and described their ethnicity as white or white UK (263; 88.0%). Two hundred and sixty (87.0%) were men who have sex with men. The majority (175; 58.5%) were single (single, divorced or widowed), and 124 (41.5%) were in a partnership (married, in a civil partnership or living with a partner). Participants had been diagnosed with HIV for a mean of 11.9 years (SD = 6.6 years) and had been taking ART for a mean of 9.0 years (SD = 5.3 years).
Comorbid conditions
Two hundred and fifty (83.6%) participants reported comorbid illness. The number of comorbid conditions reported ranged from 1 to 11 (mean = 2.43; SD = 2.03). Sixty-nine participants (23.1%) reported one comorbidity; 59 (19.7%) reported two; 42 (14.0%) reported three; 33 (11.0%) reported four and 47 (15.7%) reported five or more. Multimorbidity was reported by 181 participants (60.5%). Figure 1 shows the prevalence of individual comorbid conditions.
Percentage of participants reporting individual comorbid conditions.
Concomitant medication
Two-thirds (n = 200; 66.7%) of participants reported taking at least one non-ART medication in addition to ART. The number of concomitant medicines ranged from 1 to 11 (mean = 1.97; SD = 2.19). Sixty-one (20.4%) reported one co-medication; 45 (15.1%) reported two; 32 (10.7%) reported three; 22 (7.4%) reported four and 40 (13.4%) reported five or more concomitant medicines (defined as polypharmacy 20 ). The most commonly reported co-medicines were statins (n = 85; 28.4%) and proton pump inhibitors (n = 40; 13.4%). There was a positive correlation between number of comorbidities and number of concomitant medicines (r = 0.526; p < 0.0001).
Lifestyle
Sixty percent of participants (n = 178) reported that they had ever smoked, and n = 90 (30.0%) were current smokers. Alcohol use in excess of 21 units on average per week was reported by 56 participants (18.7%), while a third of participants reported no units of alcohol in a typical week (n = 98; 32.7%). The mean score on the 6-point scale was 3.1 (SD = 1.9). Use of recreational drugs was reported by n = 43 (14.4%). Participants reported using marijuana (n = 24; 8.0%), ecstasy (n = 11; 3.7%), cocaine (n = 8; 2.7%), ketamine (n = 7; 2.3%) and heroin (n = 1; 0.3%). Half of the sample (n = 147; 49.2%) reported engaging in regular exercise (defined as exercising three times per week ‘always’ or ‘most of the time’). The mean score on the exercise scale was 1.7 (SD = 1.1).
Predictors of comorbidity
Associations between clinical, demographic and lifestyle factors, comorbidity and service utilisation (univariate analysis).
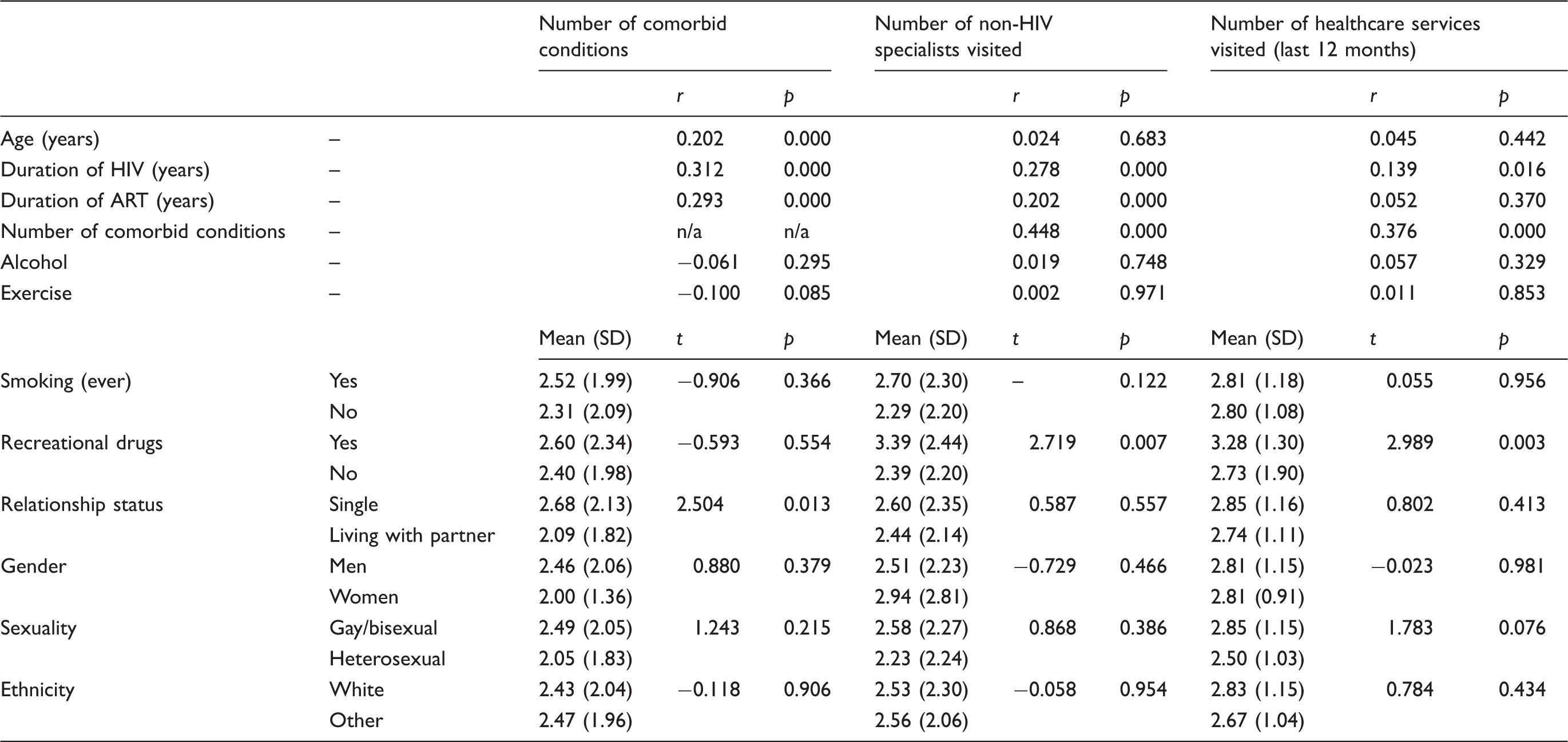
Multiple linear regression analysis of predictors of comorbidity and health service utilisation.

Healthcare utilisation
Services used over the previous 12 months
The vast majority of participants (n = 295; 98.7%) were registered with a GP, and 304 (95.7%) had disclosed their HIV status to their GP. The proportions of participants who reported having visited their HIV clinic, GP, other hospital specialists, Accident and Emergency, alternative health specialists and details of inpatient admissions are shown in Figure 2. The number of different services visited during the past 12 months ranged from 0 to 6 (mean 2.8; SD = 1.1).
Use of healthcare services over the previous 12 months.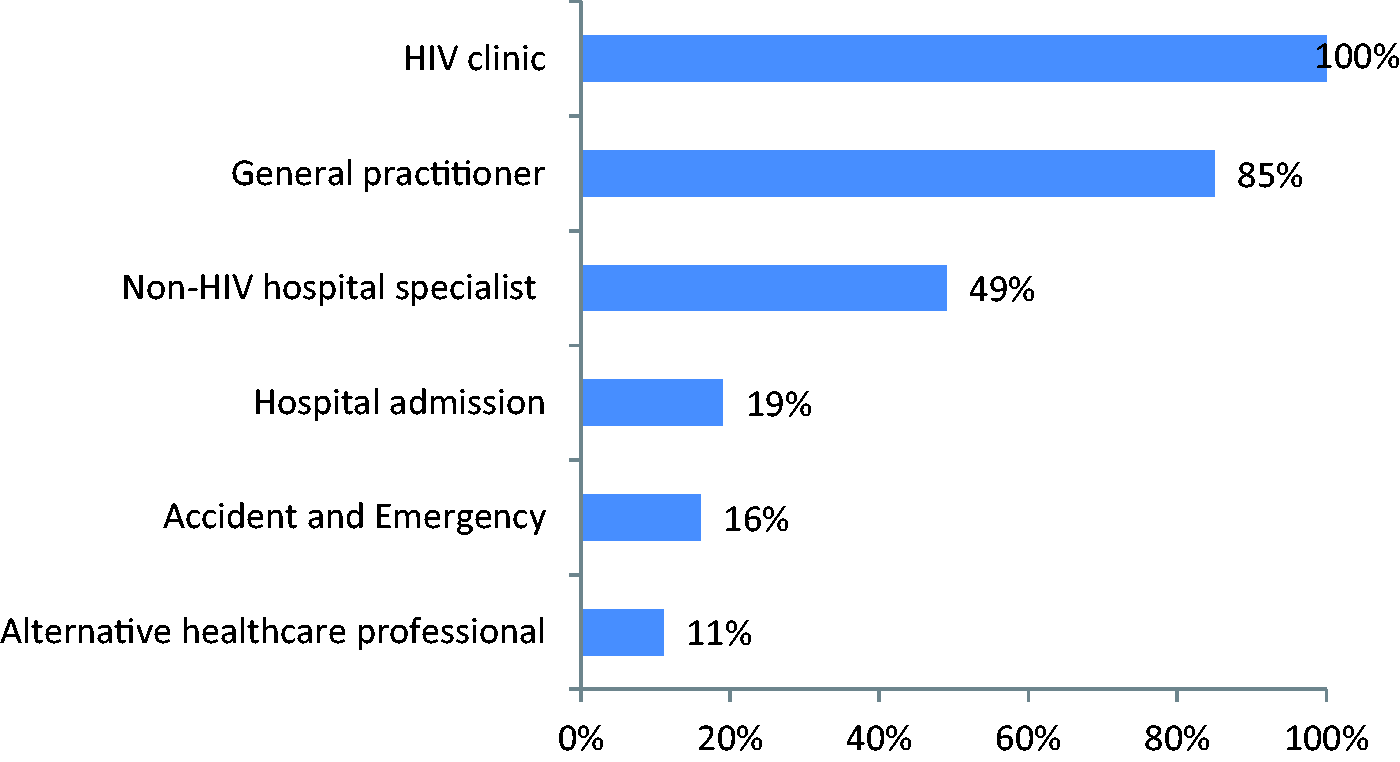
Use of non-HIV specialist services
Use of non-HIV specialist services is shown in Figure 3. The number of non-HIV specialist services visited ranged from 0 to 10; mean = 2.0 (SD = 2.3).
Use of non-HIV specialist services.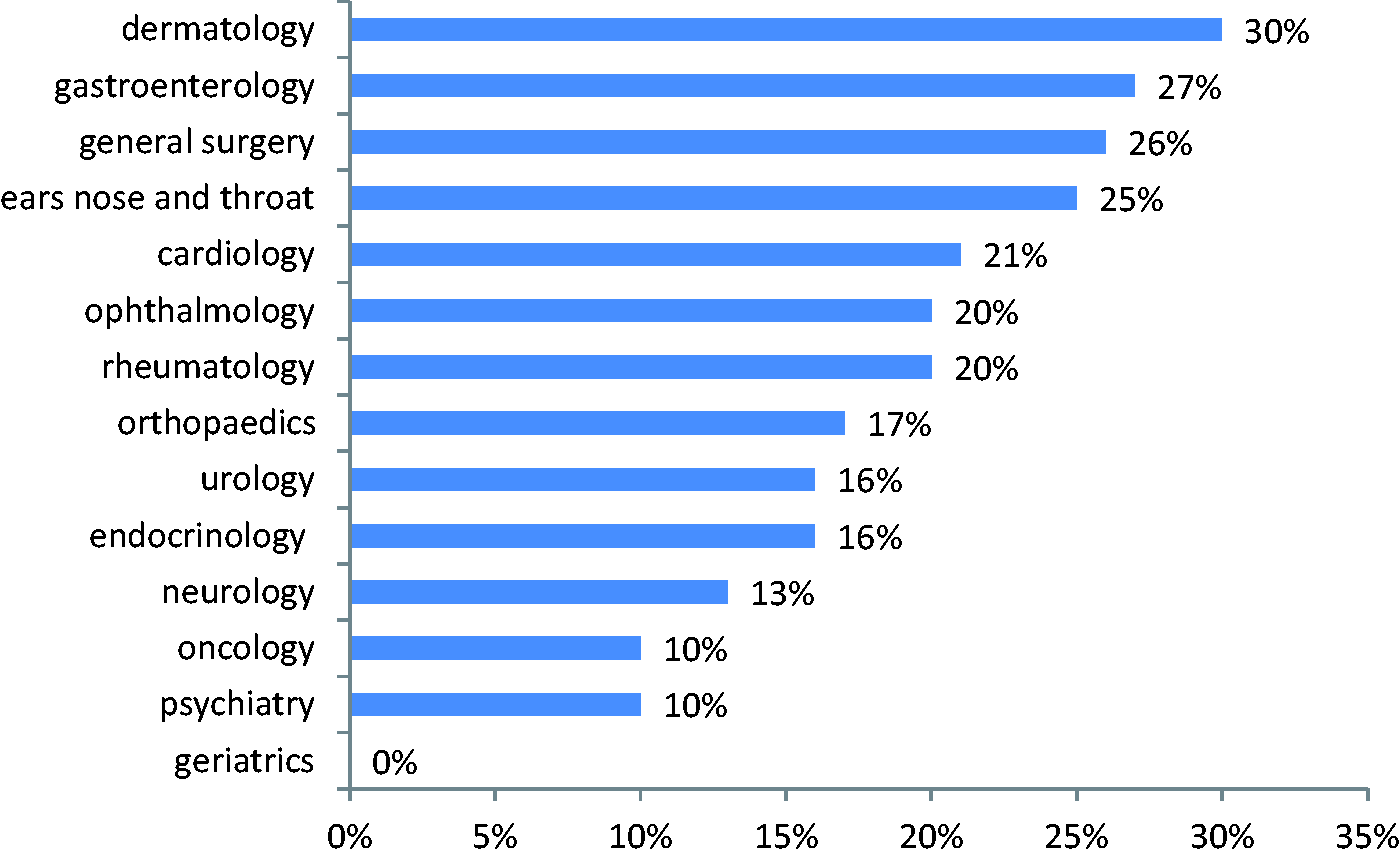
Predictors of service utilisation
Services used over the previous 12 months
In univariate analysis, service use was associated with greater number of comorbidities, a longer duration of HIV diagnosis and recreational drug use (Table 1). In multiple linear regression analysis, only need factors (number of comorbidities and recreational drug use) remained significant predictors (Table 2). The regression model accounted for 16% of the variance (R2 = 0.155).
Use of non-HIV specialist services
In univariate analysis, number of comorbid conditions, duration of HIV diagnosis, duration of ART and recreational drug use were associated with use of a greater number of non-HIV specialist services (Table 1). In multiple linear regression, significant predictors included both predisposing factors (female gender) and need factors (number of comorbid conditions, duration of HIV diagnosis and recreational drug use) (Table 2). The regression model accounted for 24% of the variance (R2 = 0.235).
Screening
Screening tests with high self-reported uptake included blood pressure (n = 290; 97.0%), blood cholesterol (n = 206; 68.9%) and sexual health screen (n = 189; 63.2%). Less than half the sample reported having had a chest radiograph (n = 142; 47.5%), electrocardiogram (n = 119; 39.8%), bone density scan (n = 99; 33.1%) or glucose tolerance test (n = 85; 28.4%), 58 (20.5%) men had a PSA test and 11 (68.8%) women had had a mammogram.
Discussion
Our findings confirm that chronic conditions commonly found in older individuals in the general population are highly prevalent among HIV-positive individuals aged ≥50 years in a UK cohort. The majority of participants reported at least one comorbid condition, while almost two-thirds reported two or more. Comorbidity was associated with polypharmacy and more frequent use of non-HIV specialist healthcare services
Polypharmacy was highly prevalent among our cohort. Whilst we did not estimate the risk of specific drug interactions, the commonly prescribed medications for the most frequent comorbidities seen (statins, PDE5 inhibitors, PPIs and antidepressants), all have potentially significant drug–drug interactions (DDIs) with ART. Indeed, Marzolini et al. 21 showed that HIV-positive patients aged ≥50 years were at an increased risk of potential DDIs compared to younger individuals (51% vs. 35%, respectively). DDIs can lead to toxicity and reduced efficacy of ART.21,22 These findings emphasise the need for awareness among clinicians of potential DDIs with antiretroviral medicines and the need for communication between different healthcare teams.
It has been proposed that HIV, ART, lifestyle and genetic characteristics all place people with HIV at increased risk of age-related comorbidities. 15 We found that both a longer duration of HIV and ART use were associated with a greater number of comorbid conditions; however, we were unable to examine the relative impact of each. Contrary to the findings of previous research,23,24 we did not find an association between comorbidity and lifestyle factors such as the use of recreational drugs, alcohol, smoking and exercise. The reasons for this lack of association are unclear; possible explanations are that patients may have under-reported unhealthy lifestyle activities, the lack of information on current smoking or that the effects of long-term HIV and/or ART on comorbidity are indeed greater than lifestyle factors, particularly in this advanced HIV cohort.
The vast majority of participants reported having registered with and disclosed their HIV status to their GP. These rates of disclosure are higher than those found in other recent studies.25–27 Patients with more comorbid conditions had used a greater number of non-HIV specialist healthcare services over the previous 12 months. We do not know if these attendances were appropriate; however, chronic disease, social isolation and poor co-ordination of care have previously been implicated in inappropriate use of emergency services. 28
We used Andersen's Behavioural Model 18 to explain healthcare utilisation. In multivariate models, need factors, including the number of comorbid conditions and self-reported use of recreational drugs, predicted use of a greater number of services. The relationship between increasing comorbidity and use of services is consistent with previous research in the general population. 29 The finding that recreational drug use was associated with increased use of services warrants further investigation; however, previous studies in the general population have reported greater use of healthcare services among drug users, 30 and drug use has previously been linked to reduced life expectancy among people with HIV. 31 Predisposing factors, including age, were not associated with use of services. The amount of variance accounted for in the regression models may have been limited by the lack of enabling factors included. We included relationship status as a proxy for social support; however, we lacked a validated measure of social support, which may be more predictive of service use. Moreover, health care utilisation may be influenced by health beliefs and self-rated health, neither of which were included in this study.18,19 We measured the number of different healthcare services visited by participants, but lacked data on the frequency with which services were used.
It is noteworthy that the rate of uptake of mammographic screening was sub-optimal (68%), but matched rates were seen in the local general population; in 2011/2012 uptake was 70%. 32 A previous questionnaire-based study reported lower rates up uptake of screening in HIV populations compared to controls. 33 Rates of uptake of mammography between 2011 and 2012 in age-matched HIV-positive patients and HIV-negative controls were 24.3% and 62.3%, respectively, over one year and 42.0% vs. 86.7%, respectively, over five years. 33
Novel strategies that have evolved over recent years to enhance the care of older HIV-positive patients include a wider involvement of primary care in the management of HIV, similar to the integrated model that applies to other long-term conditions in the National Health Service, 34 combined clinics in secondary care including one or more specialist in addition to the HIV clinician 35 and dedicated clinics for the enhanced screening and management of comorbidities. 36 It is important that any new model of care is evidence based and takes account of patient preferences. Research in this area is currently lacking.
The results of this study should be considered in light of its limitations. Self-report measures may be prone to recall and self-presentation bias. This is evident in the low reported uptake of cholesterol screening, which is routine in HIV outpatient care, but which patients may be unaware of. The drug use questionnaire did not include crystal methamphetamine, GHB/GBL and mephedrone; however, the use of these drugs has increased over more recent years among men who have sex with men. 37 Data were collected at a single timepoint; therefore, we were unable to identify the direction of relationships between comorbidity and risk factors. Given the absence of a comparison group, it was not possible to determine whether rates of disease, treatment or health service utilisation were elevated within the HIV-positive population compared to demographically-matched HIV-negative individuals. Moreover, data were collected from a single site, where the vast majority of patients are white men who have sex with men, limiting the generalisability of our findings.
This study confirms high rates of comorbidity among older people with HIV, with risk factors including increasing age, HIV and ART. Furthermore, we have identified high rates of polypharmacy and healthcare utilisation among those with comorbidities. The effective management of chronic comorbid conditions is essential to optimise quality of life and reduce mortality in HIV-positive individuals. These findings indicate the need for accessible, well co-ordinated primary and secondary care, and have implications for future research to inform the design of health services to meet the needs of older HIV-positive individuals.
Footnotes
Acknowledgements
This study was presented at the second joint conference of the British HIV Association and the British Association for Sexual Health and HIV Manchester, UK, 20–23 April 2010; Poster 68.
Declarations of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Brighton and Sussex Medical School Medical Student Research Grant.