
Abstract
Due to demographic changes in people living with HIV (PLHIV), physicians are challenged with age-related comorbidities and their management. In the absence of comprehensive data collection, the burden of comorbidities and co-medication in addition to antiretroviral therapy (ART) remains unclear for the German real-world setting. BESIDE was an observational, cross-sectional study evaluating the prevalence of comorbidities and use of co-medication in treated PLHIV. Regional distribution of study centers (n = 20), consecutive patient recruitment, and age-stratified sampling in alignment with national epidemiologic data aimed to ensure a representative sample (n = 453). The overall prevalence of comorbidities was 91.2%; 31.6% of patients had ≥4 comorbidities. The most common diagnoses were vitamin D deficiency (29.1%), depressive episode (27.8%), arterial hypertension (16.3%), and hypercholesterolemia (10.8%). 83.7% of patients were on co-medication; 21.2% taking ≥4 medications. The most common medications or supplements were vitamins (31.6%), anti-inflammatory agents (16.1%), renin–angiotensin system agents (12.1%), acid suppressants (11.7%), lipid modifying agents (10.8%); 1.3% of patients were on co-medication that should not be co-administered with ART, 41.5% on co-medication with potential for drug–drug interactions. The prevalence of comorbidities and use of co-medication among treated PLHIV in Germany is consistently high and increases across age groups, illustrating the complexity of HIV care involving appropriate ART selection.
Background
Due to improved access and use of effective antiretroviral combination regimens, demographics of people living with HIV (PLHIV) have continuously changed over the last two decades. PLHIV in the 50-year-plus age group are a growing part of the HIV epidemic. Although the overall life expectancy with HIV-1 infection has not yet returned to that of the general population, the gap between PLHIV and HIV-uninfected individuals with access to care has narrowed.1,2 In high-income countries, approximately one-third of all adults living with HIV are aged over 50. In Germany, about 50% of PLHIV belong to this group. 3 Physicians involved in the treatment of HIV are facing new challenges concerning the treatment and management of age-related comorbidities. 4 Moreover, there is evidence that PLHIV are at increased risk of specific age-related chronic comorbidities, namely cardiovascular, neurological, bone or renal diseases, malignancies, and metabolic disorders.2,5–9
Life style factors such as alcohol and tobacco use or the use of recreational or illicit drugs involving drug–drug interactions (DDIs) contribute to specific comorbidities. In the absence of comprehensive national data collection, the extent of the burden of comorbidities in PLHIV and their management in diverse real-world settings is still unclear. The primary objectives of BESIDE, an observational study conducted in 20 centers across Germany, were to quantify the prevalence of comorbidities and the use of concomitant medication in PLHIV on antiretroviral therapy (ART), in total and with respect to age, and thereby, based on a representative sample, provide estimates for the total population of PLHIV in Germany.
Methods
Study design and setting
BESIDE was a cross-sectional multicenter, non-interventional study in PLHIV on ART in Germany. Collection of data was pseudonymized focusing on HIV/AIDS-related and non-HIV/AIDS-related comorbidities and HIV-related and non-HIV-related concomitant medication including prescription and non-prescription (over-the-counter [OTC]) drugs and supplements. The use of recreational, psychoactive, or illicit drugs in the study population was recorded via anonymous patient questionnaires (not allowing linking the data with individual patient records). The evaluation of illicit drugs will be published separately. Regional distribution of study centers, consecutive patient recruitment in the centers, and stratified sampling by age group (in alignment with a demographic data estimation of the Robert Koch Institute, the German federal government agency and research institute responsible for disease control and prevention) should minimize selection bias and ensure a representative sample of PLHIV in Germany. 10 The planned sample size was 450 patients from 20 German centers (with a maximum of 30 patients per center), allowing the detection of concomitant non-HIV co-medication used by as few as 1.0% of the target population with a power of 95%. This takes into account that approximately 25% of the recruited patients are assumed to present missing data and/or incomplete recall information.
Study population
Inclusion criteria were age ≥18 years, confirmed HIV-1 infection, being on ART, and providing written informed consent. The inclusion of patients did not depend on the use of certain medications.
Regulatory requirements and quality control
The observational plan was approved by the competent ethics committee (No. 16046). All subjects had to give written informed consent prior to enrollment in the study. Quality control involved electronic queries and telephone contacts with study sites. Ten percent of the participating study sites were subject to quality assurance audit visits including source data verification.
Outcome measures
HIV/AIDS-related and non-HIV/AIDS-related comorbidities were assessed by the treating clinicians including review of medical history in individual patients’ records. Comorbidities present at the day of the visit or treated within the previous seven days were systematically recorded based on a selection of predefined common diagnoses including free text entries for additional relevant diagnoses. Comorbidities were classified according to International Classification of Diseases-10 codes.
Concomitant medications including contraceptives, OTC drugs, minerals or vitamin supplements currently taken or within the previous seven days were grouped by anatomical therapeutic chemical classes. The use of alcohol, tobacco, psychoactive substances, and various recreational and illicit drugs was assessed by means of an anonymous self-report modified EMIS Questionnaire.11,12 The evaluation of psychoactive substances, recreational and illicit drug use is beyond the scope of this evaluation and will be presented elsewhere. For analyses of potential DDIs between different ART regimens and concomitant medication, the Liverpool HIV Drug Interactions Database was consulted. 13
Statistical methods
All parameters were evaluated in a descriptive manner. For categorical variables, summary tabulations included number and percentage for each category (including a category for missing data). For continuous variables, number of observations, mean, standard deviation, median, minimum, maximum, and number of missing observations were evaluated. Analyses were carried out for the total study population (full analysis set [FAS]) and stratified by age group (<30 years/30–39 years/40–49 years/50–59 years/≥60 years) and gender (male, female). Comparisons of categorical variables between different subgroups were assessed with Chi square test or Fisher’s exact test and comparisons of continuous variables with Wilcoxon Two-Sample test or Kruskal–Wallis test, if applicable. All reported p-values were two-sided, if not stated otherwise. All statistical analyses were performed using the software package SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Study population
Between September 2016 and March 2017, 456 patients from 20 German centers were screened for study participation and 453 eligible patients were enrolled (FAS), with 22% female patients. The median age of the study population was 46 years (range 18–86 years). More than half of the patients were aged between 40 and 59 years. Both, age and gender distribution were representative for the German population of PLHIV (Figure 1). 3 Baseline characteristics of the FAS are shown in Table 1.
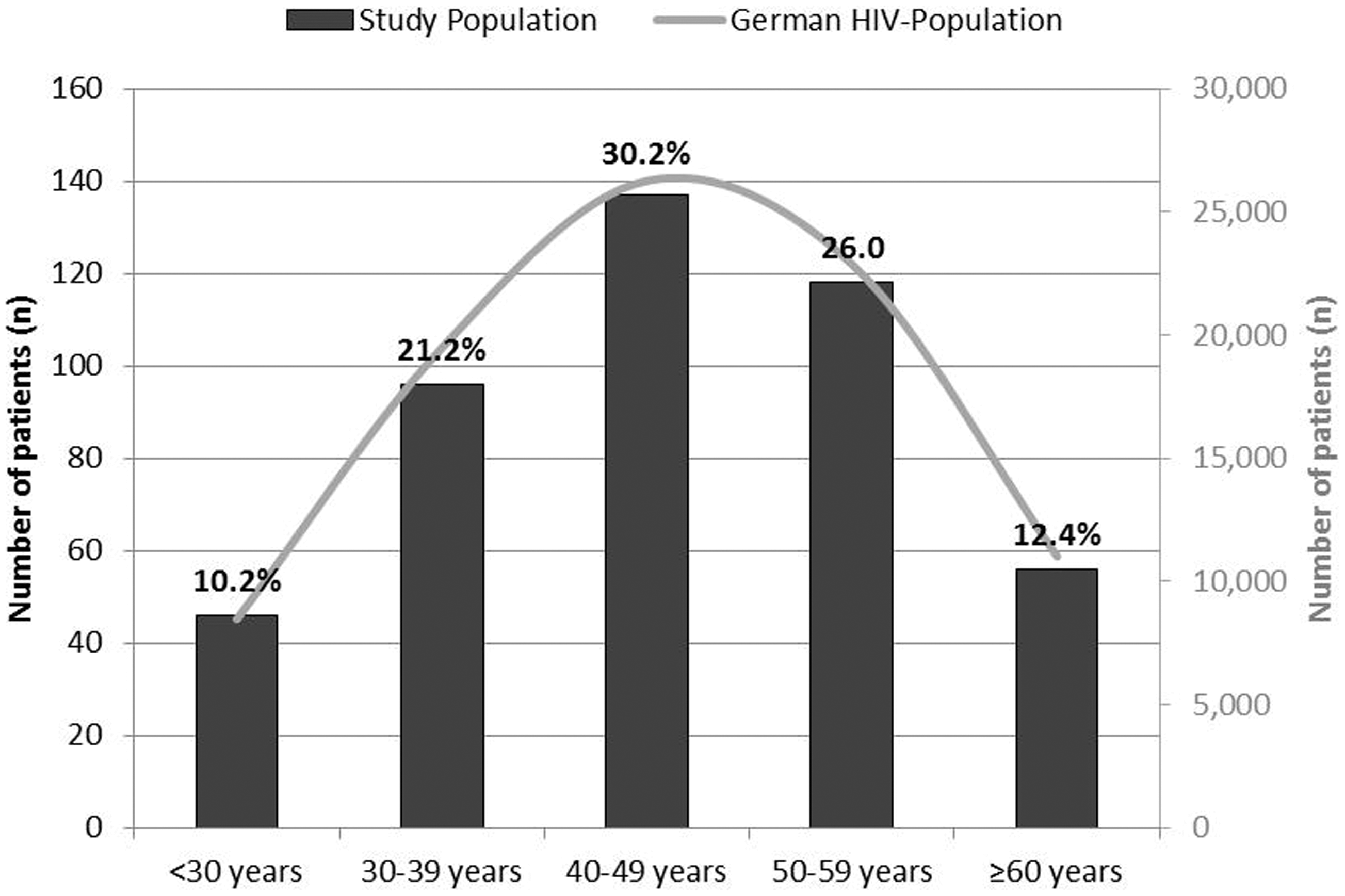
Age distribution in the study population (black bars) in comparison to the population of PLHIV in Germany (grey line (smoothed); based on estimates of the Robert Koch Institute for the year 2017 14 ).
Socio-demographic characteristics of the study population (full analysis set, FAS).
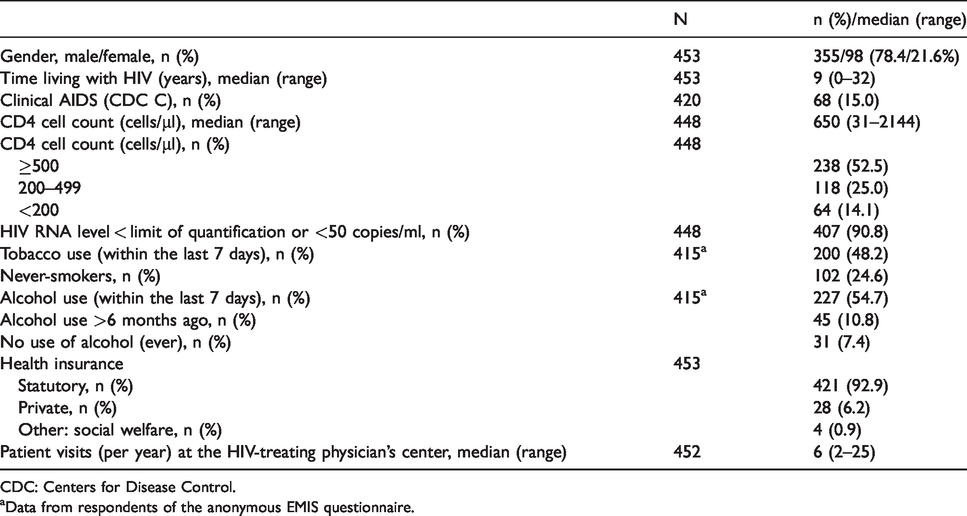
CDC: Centers for Disease Control.
aData from respondents of the anonymous EMIS questionnaire.
More than 90% of patients (92.9%) had statutory health insurance. The median number of patient visits at the HIV-treating physician’s center was six per year, with no significant differences between age groups. Median time living with HIV was 9.0 years, with 3.0–9.0 years in the age groups below 50, 16.5 years in the age group 50–59 years, and 18.5 years in the age group 60-year-plus, respectively. History or presence of clinical AIDS (i.e. Centers for Disease Control classification C) was reported in 15.0% of the study population, with 7.3–13.1% in the age groups below 50, 16.1% in the age group 50–59 years, and 33.9% in the age group 60-years-plus, respectively. The overall median CD4 cell count was 650 cells/µl, with a median of >450 cells/µl in all age groups; 90.8% of patients were on suppressive ART with an HIV RNA level below <50 copies/ml or the limit of quantification of the assays used (96.0% <200 copies/ml).
Antiretroviral therapy
The vast majority of patients (96.7%) were treated with a combination of at least three antiretroviral drugs, either as single tablet (41.6%) or multitablet regimens (58.4%). Two-thirds of patients (66.7%) received triple therapy. Most commonly used nucleoside reverse transcriptase inhibitors were emtricitabine (in 67.1% of patients), tenofovir alafenamide (34.7%), tenofovir disoproxil fumarate (33.3%), abacavir (24.3%), and lamivudine (23.8%). Of other drug classes, the following drugs were used in >10.0% of patients: of integrase inhibitors (INIs), dolutegravir (in 30.4% of patients), cobicistat boosted elvitegravir (14.8%), and raltegravir (12.8%); of protease inhibitors (PIs), darunavir (13.9%); and of non-nucleoside reverse transcriptase inhibitors (NNRTIs), rilpivirine (11.9%) and nevirapine (10.2%).
Comorbidities
The proportion of patients with at least one comorbidity (including laboratory alterations) was 91.2% (women 89.8%, men 91.6%) with a high prevalence in all age groups (Figure 2(a)). The proportion of patients with laboratory alterations only was 11.5% overall but tended to be smaller in patients above the age of 50. Of 1,321 documented comorbidities, 67.3% were classified by the investigators as non-HIV/AIDS associated comorbidities, the remaining were assigned as ‘HIV/AIDS associated’ (14.6%) or the association was ‘non-determinable’ (18.1%). Three hundred and two comorbidities were based on laboratory alterations including vitamin D deficiency, hypercholesterolemia, and hypertriglyceridemia.
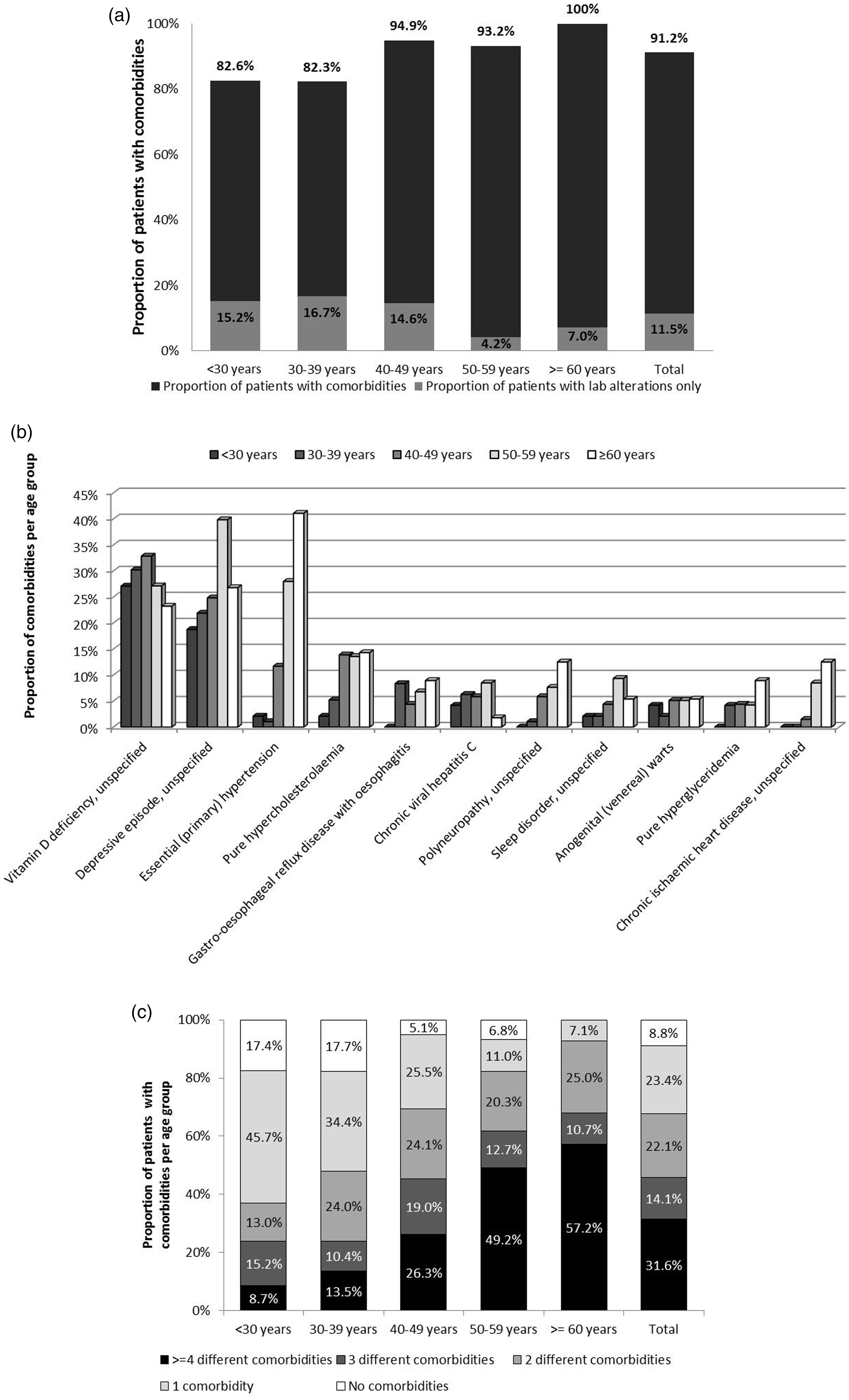
(a) Prevalence of comorbidities (including laboratory alterations) stratified by age group; (b) prevalence of most common diagnoses (>4% of patients) stratified by age group; and (c) proportion of patients with 0, 1, 2, 3, or ≥4 comorbidities stratified by age group.
Most common diagnoses (in >3% of patients) were vitamin D deficiency (29.1%), depressive episode (27.8%), arterial hypertension (16.3%), hypercholesterolemia (10.8%), gastro-esophageal reflux disease with esophagitis (6.0%), chronic hepatitis C virus infection (6.0%), polyneuropathy (5.5%), sleeping disorder (5.1%), anogenital (venereal) warts (4.4%), hypertriglyceridemia (4.4%), chronic ischemic heart disease (4.2%), muscle wasting and atrophy (4.0%), other hyperlipidemia (4.0%), history of psychoactive substance use (4.0%), type 2 diabetes mellitus (3.5%), and chronic kidney disease (3.3%, i.e. <1–3.4% in the age group <60 years and 14.3% in patients aged ≥60 years). The distribution of most common diagnoses (>4%) across age groups is shown in Figure 2(b). The number of comorbidities increased by approximately 0.12 per year, i.e. 1.2 comorbidities per decade. Overall, 31.6% of patients had ≥4 comorbidities, steadily increasing from 8.7% at younger ages (<30 years) to 13.5% between 30 and 39 years, 26.3% between 40 and 49 years, 49.2% between 50 and 59 years, and 57.1% in the 60-year-plus group. The proportion of patients with 0, 1, 2, 3, or ≥4 comorbidities across age groups is shown in Figure 2(c).
Gender differences in comorbidities
The following disease categories showed a higher prevalence of comorbidities in women compared to men with a difference in percentage of >4%: disorders of bone density and structure (osteoporosis with or without documented pathological fracture) (total 3.1%: women 9.2%, men 1.4%), disorders of thyroid gland function (total 5.3%: women 10.2%, men 3.9%), nutritional anemias (total 5.5%: women 11.2%, men 3.9%), other nutritional deficiencies (total 30.2%: women 38.8%, men 27.9%), potential health hazards related to family and personal history and certain conditions influencing health status (total 4.4%: 8.6% women, 3.1% men). Conversely, metabolic disorders (total 18.3%: women 10.2%, men 20.6%) were more common in men.
Non-HIV-related concomitant medication
83.7% of patients (n = 379) took at least one non-HIV-related concomitant medication (including OTC drugs) (women 85.6%, men 83.1%). In particular, 76.1% of patients received prescription medication (23.4% in combination with OTC drugs). Almost three-quarters (71.0%) of non-HIV-related concomitant medication (incl. OTC drugs) were taken due to comorbidities. In total, 1,052 non-HIV-related drugs were documented, which corresponds to an average of 2.8 concomitant medications per patient. The use of non-HIV-related concomitant medication across age groups is shown in Figure 3(a). Of note, prescription drugs (with or without OTC drugs) were used in 63.0% of patients aged <30 years, in 70.8% of patients aged 30–39 years, in 70.8% of patients aged 40–49 years, in 86.4% of patients aged 50–59 years, and in 87.5% of patients aged at least 60 years. About one-third of patients (31.6%) used vitamins (25.6% cholecalciferol), 16.1% anti-inflammatory and anti-rheumatic products, 12.1% agents acting on the renin–angiotensin system, 11.7% drugs for acid-related disorders, and 10.8% lipid modifying agents. Analgesics and antithrombotic agents were each taken by 9.7% of patients. Psychoactive drugs including psychoanaleptics and psycholeptics were taken by 13.5% of patients. Most common co-medications across age groups are shown in Figure 3(b). Non-HIV-related concomitant medication was mainly taken once a day (52.9%), followed by ‘on demand’ (18.7%), and twice a day (10.1%).
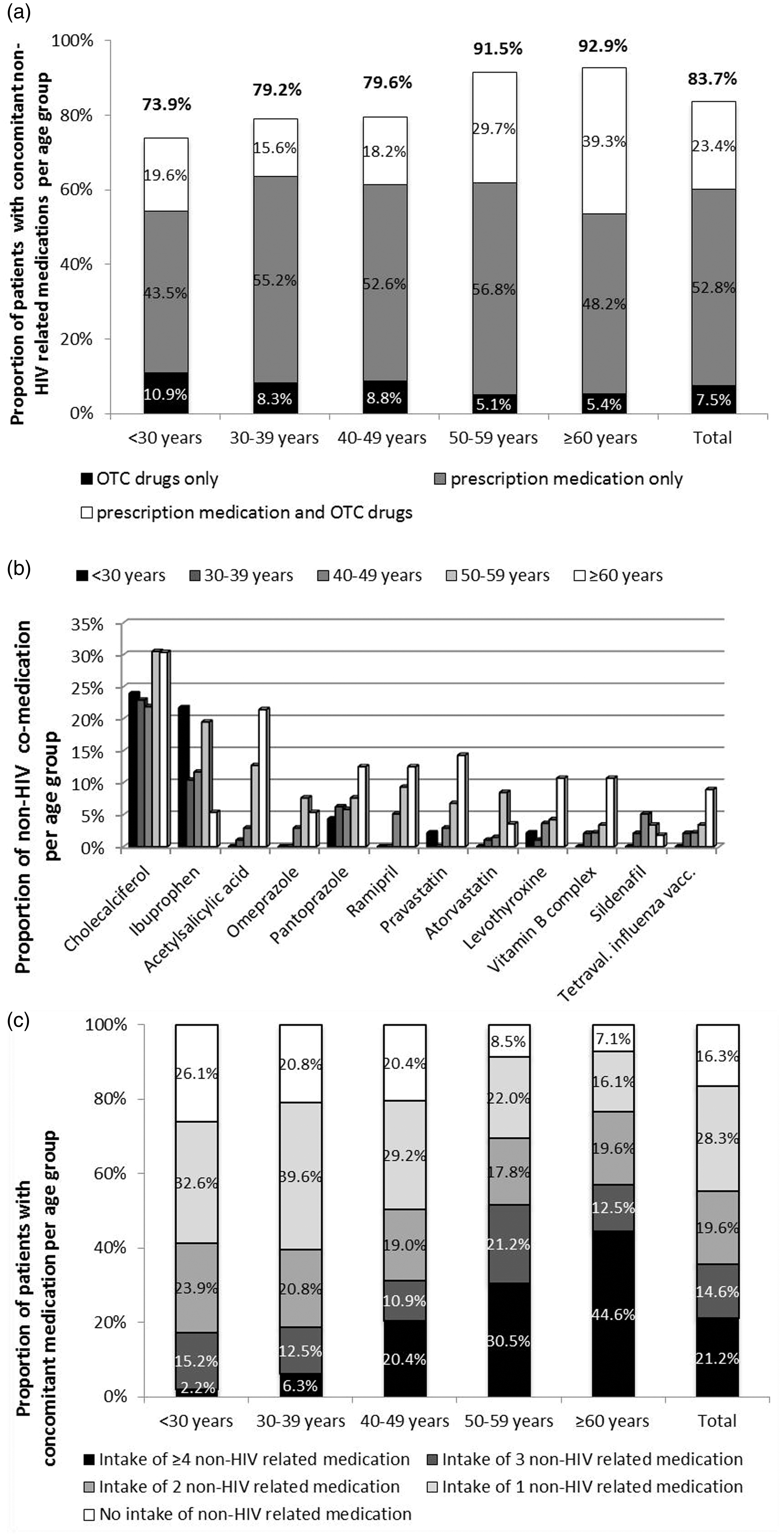
(a) Prevalence of co-medication use stratified by age group; (b) most common concomitant medications (>3% of patients) stratified by age group; and (c) proportion of patients with 0, 1, 2, 3, or ≥ 4 concomitant non-HIV-related medications stratified by age group. OTC: over-the-counter.
Overall, about one in five patients (21.2%) took four or more concomitant medications. The number of non-HIV concomitant medications consistently increased across age groups (Figure 3(c)) by approximately 0.09 for every year of HIV infection.
Gender differences in co-medication
Women more commonly used (with a difference in percentage of >4%) antianemic preparations (total 7.5%: women 14.3%, men 5.6%), vitamins (total 31.6%: women 37.8%, men 29.9%), mineral supplements (total 6.0%: women 10.2%, men 4.8%), and thyroid therapies (total 4.9%: women 8.2%, men 3.9%), and men more commonly used antithrombotic agents (total 9.7%: women 4.1%, men 11.3%), renin–angiotensin system agents (total 12.1%: women 7.1%, men 13.5%), and lipid modifying agents (total 10.8%: woman 6.1%, men 12.1%).
Potential DDIs between ART and concomitant medication
According to the Liverpool HIV Drug Interactions Database, 1.3% of the study population used concomitant medication (including OTC drugs), which should not be co-administered with their antiretroviral regimens (this corresponds to 1.5% of patients taking co-medication). These were mainly proton pump inhibitors in combination with rilpivirine-containing ART.
Four out of ten patients (41.5%) took concomitant medication with a potential for DDIs with their ART requiring closer monitoring or dose adjustments (Figure 4; this corresponds to almost half of the patients [49.6%] taking co-medication). Most combinations with a potential interaction were detected in single patients. However, the following combinations were observed more frequently: divalent cation-containing dietary supplements (e.g. magnesium, calcium, multivitamins) with INIs, statins (e.g. pravastatin, atorvastatin), beta blockers (e.g. metoprolol) or PDE-5 inhibitors (e.g. sildenafil) with CYP3A-inibiting PIs or boosted elvitegravir and calcium channel blockers (e.g. amlodipine) with CYP3A-inducing NNRTIs (EFV, NVP, ETV). Also, the combination of the thyroid hormone levothyroxine with ritonavir-containing regimens, which can lead to increased elimination of levothyroxine due to induction of glucuronidation, as well as the combination of QT-prolonging drugs, namely the antidepressants citalopram and escitalopram with atazanavir or rilpivirine were observed in some patients.
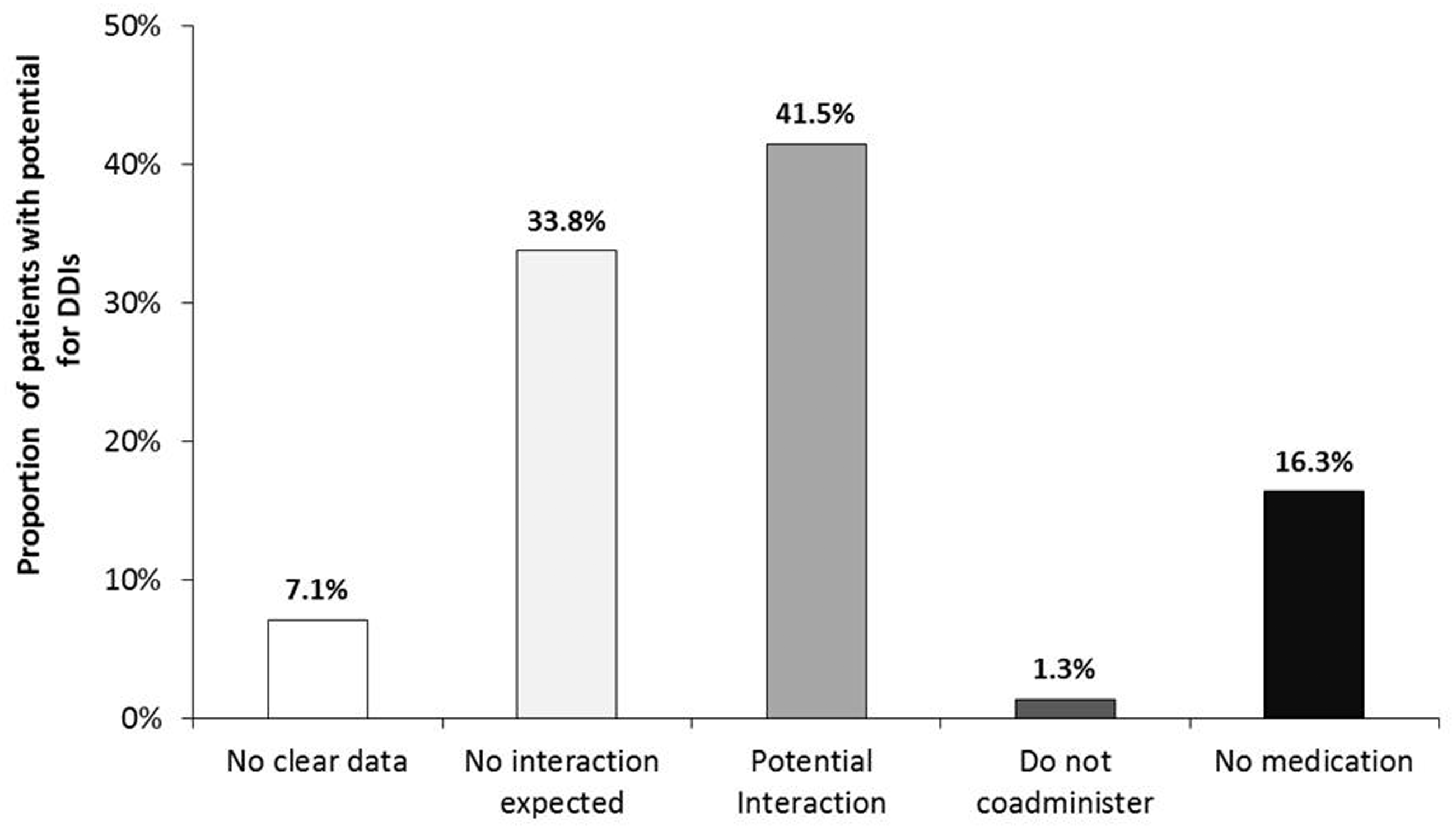
Proportion of patients with and without potential for DDIs between ART and co-medication (according to the Liverpool HIV Drug Interactions Database 13 ). DDI: drug–drug interaction.
Discussion
As observed in other studies,15–18 comorbidities and co-medication use were common in BESIDE, a representative cross-sectional cohort of PLHIV in Germany recruited between 2016 and 2017. Comorbidity prevalence was above 90% and co-medication use was documented in more than 80% of the study population. Four or more comorbidities were documented in one-third of patients, the proportion being highest in the 60-year-plus group with 57%. In comparison, in a large Italian case–control study 29% of patients aged >60 years had four comorbidities (restricted to specific diseases such as hypertension, diabetes mellitus, hypothyroidism, cardiovascular disease, and bone fractures). 19 In BESIDE, most common diagnoses (including laboratory alterations) affecting ≥10% of patients were vitamin D deficiency (29%), depressive episode (28%), arterial hypertension (16%), and hypercholesterolemia (11%), which were also among the most prevalent comorbidities in elderly HIV cohorts of the UK and the Netherlands as well as in Ireland. 18 Of note, although the participating centers were instructed to document any relevant disease, the predefined list of comorbidities in the BESIDE case report form (supplemented by free text entries) may have involved some bias.
Vitamin D deficiency is a world-wide public health challenge in all age groups. In high-income countries, the prevalence of vitamin D deficiency (defined as <25 nmol/l) and hypovitaminosis D (<75 nmol/l) is between 5 and 15% and between 50 and 75%, respectively, and has been observed to be even higher in PLHIV.20,21 Non-HIV-related risk factors such as limited sunlight exposure (of note, the BESIDE enrollment period was in fall and winter from September 2016 to January 2017), female gender, advanced age, black ethnicity, gastrointestinal absorption disorders, liver and kidney diseases, body mass index, diabetes mellitus, or alcohol consumption contribute to vitamin D deficiency as well as several HIV-related factors such as chronic inflammation and immune activation or specific NNRTIs or PIs. 21
Depression was among the most frequently observed comorbidities in BESIDE. Prevalence was in line with other studies using validated questionnaire-based screening instruments to identify symptoms of depression.22,23 A marked increase with age was primarily observed for hypertension, polyneuropathy, ischemic heart disease, and chronic kidney disease and/or renal failure.
More than 80% of male and female patients took at least one non-HIV-related concomitant medication (including OTC drugs). Three-quarters of patients received prescription medication. Patients consumed on average 2.8 concomitant medicines per day. Polypharmacy with potential for DDIs was of the same order as described elsewhere.17,24,25 About one in five patients took four or more concomitant medications. As observed for the number of comorbidities, the number of co-medications increased consistently across age groups. On average, for nearly every decade of age one co-medication was added. About one-third of patients used vitamins (26% cholecalciferol). Several studies have linked vitamin D status with bone disease in PLHIV. Exogenous vitamin D (cholecalciferol) supplementation seems to reverse some alterations of the immune system due to vitamin D deficiency, supporting the use of cholecalciferol as prophylaxis.20,26
About one in six patients took anti-inflammatory or anti-rheumatic products and one in eight patients took agents acting on the renin–angiotensin system. Use of drugs for acid-related disorders and lipid modifying agents was observed in 10–12% of patients. Of note, a small proportion of patients received co-medication which should not be co-administered with ART (<1.5%) and about 40% received co-medication with a potential for DDIs requiring dose adjustments or closer monitoring. This suggests that not only physicians treating HIV-1-infection, but also other specialists whom patients are referred to have to pay attention to potential DDIs with ART when prescribing concomitant medication. Our results are in line with a large retrospective cohort study in France showing a considerable risk of DDIs especially in elderly PLHIV. Of 9,067 PLHIV aged at least 65 years and receiving ART in 2016, 16.8% used drugs that should not have been co-administered according to the Liverpool HIV Drug Interactions Database. 27 Moreover, regarding the fact that almost one-third of the BESIDE cohort took OTC drugs and supplements, physicians should pay attention on their potential for DDIs with ART, e.g. in case of simultaneous use of multivitamins, aluminium/magnesium antacids, or calcium/iron supplements and INIs (see summaries of product characteristics of integrase inhibitors 28 ).
One limitation of the study is that it was a cross-sectional study without a control arm including HIV-negative age- and gender-matched patients to better characterize differences in the comorbidity burden between HIV-positive and HIV-negative individuals. However, the sample size of 453 allows prevalence estimates with 95% confidence interval widths of less than ±5%, ±3%, and ±1.5% for prevalence rates of 30, 10, or 3%, respectively. The strength of the study was the selection of a representative study population in terms of age and gender when compared to the German population of PLHIV. There were no significant differences, neither for gender nor age distribution. In Germany, 75,000 individuals are diagnosed with HIV, the proportion of females being relatively stable at 20.0% during recent years and the vast majority (92%) being on ART. 3
An increased comorbidity burden has been described in several national and international HIV cohorts.5,15,16,19,29 A retrospective matched case–control study in Germany between 2011 and 2014 using health insurance claims data showed a higher prevalence of cardiovascular disease (12.1%), HBV (6.4%) and HCV coinfections (9.0%), bone fractures due to osteoporosis (6.6%), and chronic renal disease (4.1%) in PLHIV (n = 1,627) on ART than in matched HIV-negative controls (n = 3,234; matching was based on age, gender, residence district, health insurance status, and educational level). 30 Similar results were generated from a smaller German prospective multicenter cohort study evaluating the total burden of disease in diverse patient groups aged ≥50 years. Comorbidities such as renal, neurological, and cardiovascular disorders or incident malignant diseases were more common in antiretroviral treated PLHIV than in HIV-negative controls, as was the perceived severity of symptoms of aging. 31 In a large Italian case–control study including PLHIV (n = 2,854) treated from 2002 through 2009 and age-, gender-, and race-matched adults (n = 8,562) from the general population, polypathology involving ≥2 noninfectious comorbidities (such as cardiovascular disease, hypertension, diabetes mellitus, bone fractures, or renal failure) was more common in PLHIV. Male gender, higher age, low CD4 cell nadir, and prolonged ART exposure were associated with polypathology. Polypathology occurred ten years earlier in comparison to the general population. 19 The comparison of two cross-sectional evaluations of the EuroSIDA cohort in adult PLHIV under active follow-up in 2006 (n = 9,798) and 2014 (n = 12,882) showed that between 2006 and 2014 PLHIV aged and experienced an overall higher prevalence of non-AIDS comorbidities, including chronic kidney disease and cardiovascular disease. 32
Finally, it should be noted that this cross-sectional study gives insights into the burden of comorbidities and co-medication use in treated PLHIV representative of the population of PLHIV in Germany with regard to age and gender. The considerable prevalence of multimorbidity and polypharmacy already among younger PLHIV emphasizes adequate screening methods and treatment of comorbidities with particular attention to potential DDIs with ART. Both, the selection of initial antiretroviral regimens as well as an individualized ART modification based on the prevalence of comorbidities and use of co-medication may help to minimize the risk of unfavorable pharmacological effects including adverse drug events.
Supplemental Material
sj-pdf-1-std-10.1177_0956462420942020 - Supplemental material for High prevalence of comorbidities and use of concomitant medication in treated people living with HIV in Germany – results of the BESIDE study
Supplemental material, sj-pdf-1-std-10.1177_0956462420942020 for High prevalence of comorbidities and use of concomitant medication in treated people living with HIV in Germany – results of the BESIDE study by B Funke, CD Spinner, E Wolf, H Heiken, S Christensen, HJ Stellbrink and V Witte in International Journal of STD & AIDS
Footnotes
Acknowledgements
We thank all participating patients, investigators and study nurses involved in the BESIDE study. Statistical analyses were performed by Alcedis GmbH, Giessen, Germany. Support in medical writing was provided by MUC Research GmbH, Munich, Germany.
Declaration of conflicting interests
BF and VW are current employees of MSD Sharp & Dohme GmbH. CDS, EW, HH, SC and HJS have a financial relationship relevant to this publication with MSD Sharp & Dohme Gmb. CSD has received honoraria for consulting or speaking at educational events from AbbVie, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, Hexal/Teva, Hormosan, Janssen-Cilag, MSD Sharp & Dohme, Roche, and ViiV Healthcare. He has received research grants from Gilead, Janssen-Cilag and ViiV Healthcare. EW has received honoraria for consulting or speaking at educational events from AbbVie, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, Hexal, Janssen-Cilag, MSD Sharp & Dohme, Roche, and ViiV Healthcare. MUC Research has received support for clinical research from AbbVie, Gilead Sciences, MSD Sharp & Dohme, Pfizer und ViiV Healthcare. HH has received honoraria for consulting or speaking at educational events from AbbVie, Gilead, GlaxoSmithKline, Hexal, Janssen-Cilag, MSD Sharp & Dohme, and ViiV Healthcare. SC has received honoraria for consulting or speaking at educational events from Abbvie, Gilead Sciences, Indivior, Janssen-Cilag, MSD, and ViiV Healthcare. HJS received honoraria for consulting or speaking at educational events from Gilead, GlaxoSmithKline, Janssen-Cilag, MSD Sharp & Dohme. He has received trial documentation fees from AbbVie, Gilead Sciences, MSD Sharp & Dohme, Janssen-Cilag, GSK, and ViiV Healthcare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The BESIDE study was initiated and funded by MSD Sharp & Dohme GmbH, a subsidiary of Merck & Co., Inc., Kenilworth, NJ USA.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.