
Abstract
Introduction:
HIV is an independent risk factor for cardiovascular diseases (CVD). There is insufficient information regarding comorbidities and cardiovascular risk factors in the Colombian HIV population. The aim of this study is to describe the prevalence of cardiovascular risk factors and comorbidities in patients from the HIV Colombian Group VIHCOL.
Methods:
This is a multicenter, cross-sectional study conducted in the VIHCOL network in Colombia. Patients 18 years or older who had at least 6 months of follow-up were included. A stratified random sampling was performed to estimate the adjusted prevalence of cardiovascular risk factors and comorbidities.
Results:
A total of 1616 patients were included. 83.2% were men, and the median age was 34 years. The adjusted prevalence for dyslipidemia, active tobacco use, hypothyroidism, and arterial hypertension was 51.2% (99% CI: 48.0%–54.4%), 7.6% (99% CI: 5.9%–9.3%), 7.4% (99% CI: 5.7%–9.1%), and 6.3% (99% CI: 4.8%–7.9%), respectively.
Conclusions:
In this Colombian HIV cohort, there is a high prevalence of modifiable CVD risk factors such as dyslipidemia and active smoking. Non-pharmacological and pharmacological measures for the prevention and management of these risk factors should be reinforced.
Keywords
Highlights
• Dyslipidemia and smoking, both modifiable risk factors, are common in this Colombian HIV population. • Measures for the prevention and management of dyslipidemia and smoking must be reinforced. • Monitoring of metabolic comorbidities and cardiovascular risk factors must be assured.
Introduction
With the introduction of antiretroviral therapy (ART), the prognosis of human immunodeficiency virus (HIV) infection has been modified to one of a chronic condition. 1 Despite the effectiveness of ART in reducing HIV-associated morbidity and mortality, HIV itself, the chronic immune activation and immunosenescence induced by it, and some ART have been found to increase the risk of developing cardiovascular disease (CVD) in people living with HIV (PLWHIV).2,3 In this population, dyslipidemia, arterial hypertension (HBP), type 2 diabetes mellitus (T2DM), and chronic kidney disease (CKD) represent the most common comorbidities. Moreover, tobacco smoking tends to be more prevalent in this than in the general population.4,5
Several fundamental elements contribute to the increase of cardiovascular events: high prevalence of conventional cardiovascular risk factors, HIV-induced inflammation, bacterial translocation, endothelial dysfunction, and chronic immune activation; in addition, some antiretrovirals such as darunavir/ritonavir or abacavir have been independently associated with an increase in cardiovascular events.1,2,5–12 Recent studies indicate that CVD contributes more to HIV mortality than previously thought, with reports of mortality rates up to 11%.12–20
PLWHIV have twice the risk of CVD of those who are HIV negative, in spite of viral suppression 11 . However, the estimates are heterogeneous and depend on the population studied and the geographic location.21,22 The global burden of HIV related CVD has tripled in the past two decades with higher impact in sub-Saharan Africa and the Asia Pacific region.23–25 In Latin America, the RAPID II HIV cohort study found a high overall prevalence of dyslipidemia (80.2%), with differences in the frequency of comorbidities between regions. 26
According to what is mentioned above and despite having some data on HIV related cardiovascular risk factors and comorbidities, still there is insufficient information regarding comorbidities in the Colombian HIV population. The aim of this study was to describe the prevalence of cardiovascular risk factors and metabolic comorbidities among PLWHIV from the Colombian HIV Group (VIHCOL).
Methods
We conducted a retrospective, multicenter cross-sectional study of PLWHIV receiving care between June 2019 and January 2020 at 23 HIV clinics of VIHCOL. The study included patients with confirmed HIV diagnosis who were 18 years or older, who had at least 6 months of follow-up, and who were treatment naïve at the time they initiated care at their respective VIHCOL clinic. Those participating in any ongoing clinical trial were excluded.
Setting
In the last 8 years, there has been an increase of HIV cases in Colombia. As of 2020, there were 123,490 reported cases of HIV in Colombia from which 116,868 were affiliated to the health system, 94% were on ART, and 85.18% had viral suppression. 27 The health care system in Colombia is composed by two schemes; the contributory system in which people with jobs have to pay a monthly fee to have health care access when needed, on the other hand, the subsidized system which is composed of people without income and in vulnerable situations where the government supplies the cost of them into the health system. 28
VIHCOL is a collaborative national network of HIV care centers, non-governmental, non-profit, and with the purpose of integrating information related to HIV in order to improve HIV-care in Colombia. PLWHIV attending HIV centers of VIHCOL are mainly from the contributory health system and from numerous cities in the country, principally Bogota and Cali.
Sample design
An estimated 12,500 people living with HIV received care in the VIHCOL network during the study period. To estimate the prevalence of CVD risk factors, we calculated the need for a sample of 1616 patients based on the following parameters: 99% confidence level, maximum expected prevalence of any comorbidity 30%, sampling error 3.5%, non-response 20%. We distributed this sample according to the weight that each clinical center-city had in the total population attended by VIHCOL. The sample at each center (stratum) was selected through simple random sampling of the clinical charts. For one of the centers, all the patients active during the study period were included.
Data collection
All data were obtained via chart review of electronic clinical records and entered into a data collection form created using the software REDCap™ hosted at Hospital Universitario San Ignacio (HUSI). Data were collected by at least one trained research assistant at each VIHCOL clinic. Quality of the data was assured by a second individual reviewing all collected data in a random sample of 10% of all the records.
Sociodemographic variables included age, gender, sexual behaviors, level of education, and type of health insurance. Clinical variables of weight, height, active tobacco smoking, family history of CVDs, date of HIV diagnosis, date of ART initiation, and HIV stage were obtained. Weight and height were used to calculate body mass index (BMI). Markers of HIV disease progression included HIV viral load and CD4+ T-lymphocyte (CD4) count. The limit of detection for HIV viral load was 50 copies/milliliter. Other laboratory values pertaining to CVD risk included high-density lipoprotein cholesterol (HDL), low density lipoprotein cholesterol (LDL), total cholesterol (TC), triglycerides (TG), serum creatinine, blood glucose, and thyroid stimulating hormone. Additionally, cardiovascular risk was calculated according to the adjusted Framingham score validated for the Colombian population. 29
The primary outcomes of interest were the prevalence of the CVD risk factors or comorbidities. A patient was classified as having each condition if their clinical chart included a known diagnosis or if they had clinical data fulfilling the criteria for a diagnosis. HBP was defined as at least one of the following: systolic blood pressure higher than 140 mmHg or diastolic blood pressure higher than 90 mmHg; taking antihypertensive medication; or history of HBP. 30 T2DM was defined as fasting blood glucose >126 mg/dl, post-prandial blood glucose >200 mg/dl, or glycated hemoglobin of 6.5% or higher.31,32 Overweight and obesity were defined as a BMI of 25–30 Kg/m2 and >30 Kg/m2, respectively. PLWHIV were categorized as having dyslipidemia if they had at least one of the following: LDL ≥160 mg/dl, HDL<50 mg/dl in women or <40 mg/dl in men, TC >200 mg/dl, triglycerides >150 mg/dl, a diagnosis in the clinical record, or were receiving lipid lowering medications. 33 Chronic hepatitis C infection was defined as having a positive hepatitis C antibody followed by a positive hepatitis C viral load. 34
Data on metabolic syndrome, osteopenia, osteoporosis, CKD, hypothyroidism, and cardiovascular events including myocardial infarction (MI), unstable angina, history of coronary revascularization either percutaneous or surgical, cerebrovascular accidents and transient ischemic attacks, and peripheral artery disease were obtained from the clinical charts.
Statistical analysis
Sociodemographic and clinical characteristics were summarized using frequencies and central tendency measurements. For continuous variables, the Shapiro–Wilk test was performed to confirm normal distribution. Non-normally distributed continuous variables were described using median and interquartile range (IQR).
Total prevalence estimations were performed considering the compositional effects (according to the weight of each stratum-city of care in accordance to the sampling design) as well as variance estimations.
We described the sociodemographic, CVD risk factors, and comorbidities discriminated by age (<50 years and ≥50 years) and sex.
All statistical analyses were performed with STATA 14 (College Station, TX, USA).
Ethical considerations and confidentiality
Approval for this study was granted by the Institutional Review Board at HUSI and Pontificia Universidad Javeriana (FM-CIE-0006–19). Patient consent was not required given the retrospective nature of the study.
Results
Sociodemographic characteristics of VIHCOL patients.
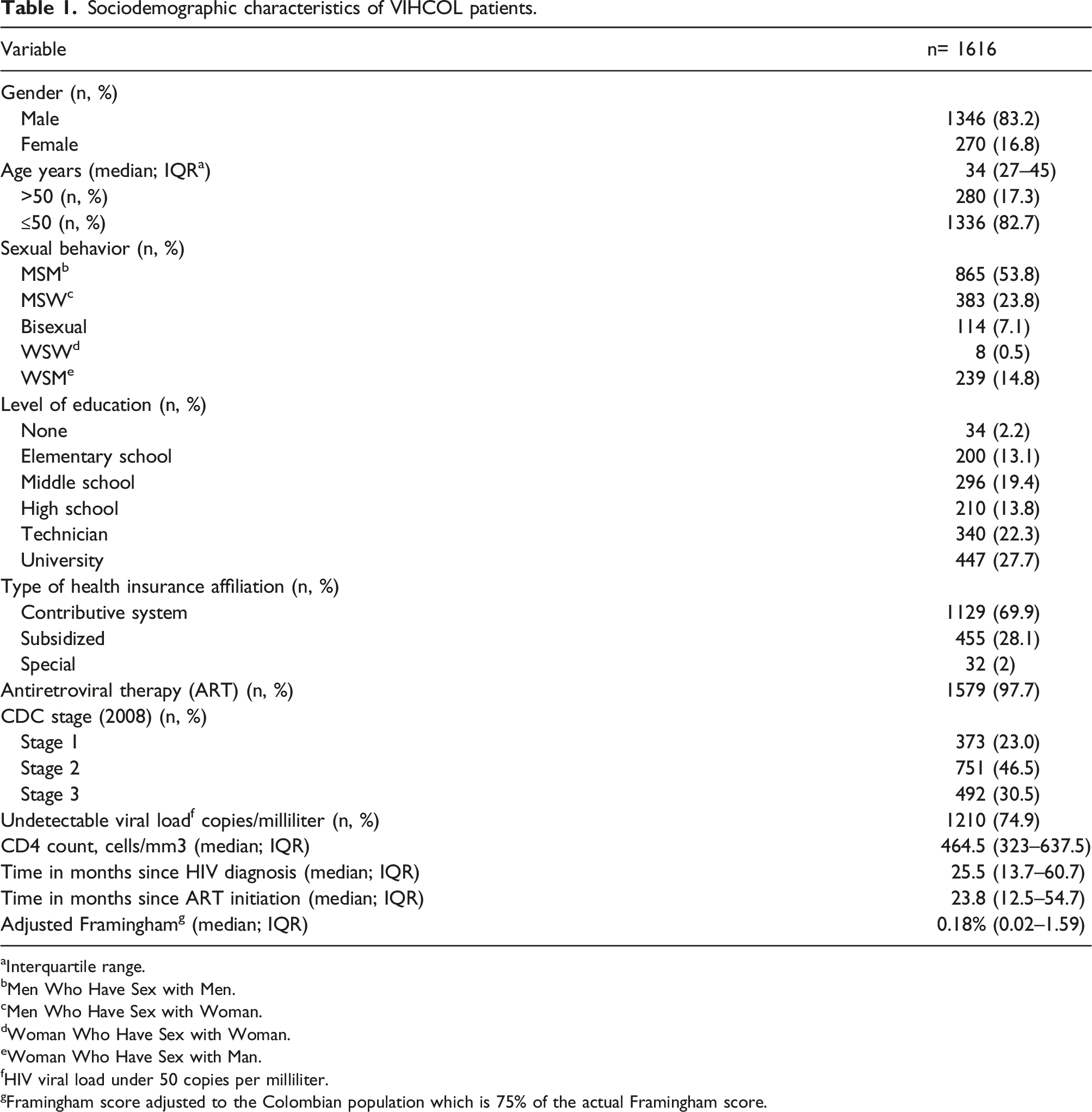
Interquartile range.
Men Who Have Sex with Men.
Men Who Have Sex with Woman.
Woman Who Have Sex with Woman.
Woman Who Have Sex with Man.
HIV viral load under 50 copies per milliliter.
Framingham score adjusted to the Colombian population which is 75% of the actual Framingham score.
Adjusted prevalence of cardiovascular risk factor and comorbidities.

The adjusted prevalence was obtained according to the weight of each stratum-city of care in accordance with the sampling design.
Cardiovascular risk factors and comorbidities according to age
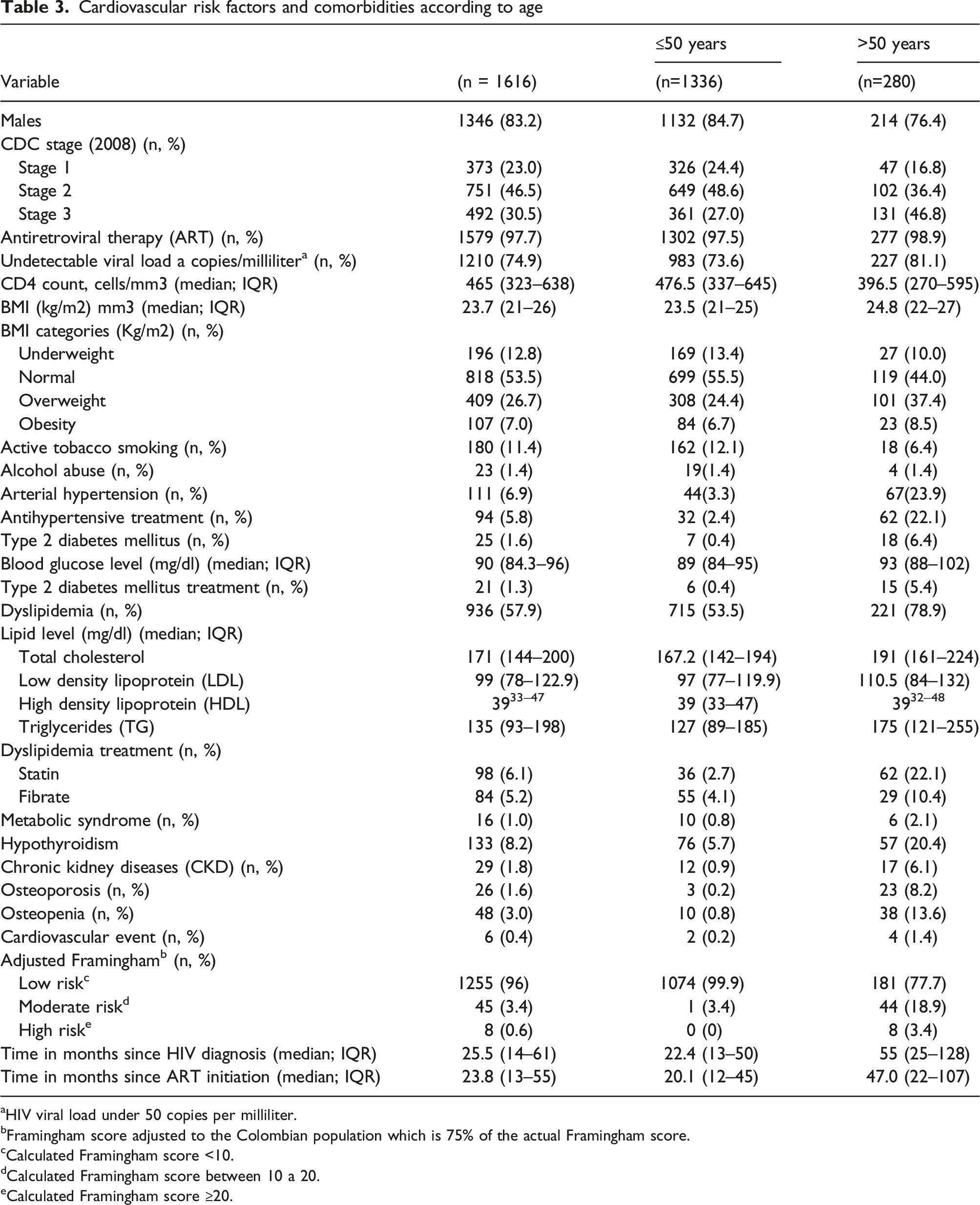
HIV viral load under 50 copies per milliliter.
Framingham score adjusted to the Colombian population which is 75% of the actual Framingham score.
Calculated Framingham score <10.
Calculated Framingham score between 10 a 20.
Calculated Framingham score ≥20.
Cardiovascular risk factor and comorbidities according to gender.

HIV viral load under 50 copies per milliliter.
Framingham score adjusted to the Colombian population which is 75% of the actual Framingham score.
Calculated Framingham score <10.
Calculated Framingham score between 10 a 20.
Calculated Framingham score ≥20.
Discussion
This study is one of the first to analyze the prevalence of CVD risk factors and comorbidities among PLWHIV in Latin America using a stratified random sample of PLWHIV attending a network of HIV centers in the principal cities of the country, which allows the estimations to be more reflective of an adjusted population level prevalence than those stated in previous studies. In our sample of Colombian PLWHIV, the main CVD risk factors and comorbidities found were dyslipidemia, active tobacco smoking, hypothyroidism, and HBP.
Dyslipidemia is linked with many factors including the effect of the virus and the effect of some antiretrovirals35,36. In this study, around 50% of the population had dyslipidemia, which is lower than what has been described for Latin America. 26 Nevertheless, our dyslipidemia prevalence was greater than previously reported in Colombia (15.0%). 37 In PLWHIV in Brazil and Kenya, the reported prevalence of dyslipidemia was 78.9% and 63.1%.38,39 Likewise, in 2015, Shen et al. estimated that the dyslipidemia prevalence in China was 75.6% with no statistically significant differences comparing PLWHIV and people living without HIV. 40 In our study, when evaluating dyslipidemia only by having the diagnosis in the clinical chart, the prevalence was low, whereas, when considering results of the lipid panel as well, prevalence increased to 51.2%. This draws attention to how blood tests are being evaluated in this population and calls for improving guidance regarding laboratory interpretation and patient’s cardiovascular risk assessment.
Regarding tobacco smoking, prevalence in PLWH is highly heterogeneous. For example, the Data Collection on Adverse Events of Anti-HIV Drugs (DAD) cohort reported a 42.8% prevalence of tobacco smoking. 41 Furthermore, De socio et al. described active tobacco use in 51.6%, which is similar to what has been reported in Germany, Spain, France, and Austria42,45. Conversely, tobacco smoking prevalence in African and Latin American countries ranges from 1.8% to 25.8% and 10.3%–50%, respectively46,47. In Colombia, the 2007 national health survey found that the tobacco smoking prevalence was 12.8%. 48 Our prevalence of active tobacco smoking in PLWHIV was 7.6% (CI 99%; 5.9%–9.3%), which is somewhat less than what has been reported for the Colombian general population.
With reference to HBP, Fiseha et al. found a prevalence of 29.7% in northern Ethiopia, similar to the prevalence described in Italy by De Socio et al.49,50 A meta-analysis conducted in 2019 by Dakum et al. showed a global HBP prevalence of 42% in patients older than 50 years, higher in North America (50.2%), followed by Europe (37.8%), sub-Saharan Africa (31.9%), and Asia (31%). 51 Data from Latin America described a 31.5% HBP prevalence and in our study the prevalence was 6.37%, still much lower than what has been reported elsewhere.26,37 Yet, 23.9% of patients older than 50 years in our study presented HBP.
In our study, T2DM prevalence was 1.5%, low compared to other factors, still it is similar to data from the DAD cohort as well as other Latin American studies.8,13,26,52–55 This is probably related to the young median age in our patients and the short median time on ART. Regarding hypothyroidism, the prevalence found in our study was 7.4%, a midpoint when compared with what has been reported. 56 Data on the prevalence of hypothyroidism is controversial. For example, in an Italian cohort from 2005 to 2017 hypothyroidism prevalence was 71.6%, whereas other studies have reported prevalence ranging from 1.3% to 22.1%.56–59
Some differences in overall CVD risk by gender have been previously documented. For example, Cahn P et al. found that men presented more dyslipidemia than women, while women presented more frequently with metabolic syndrome and obesity than men. 26 Our findings show that hypertension, hypothyroidism, osteopenia, osteoporosis, and obesity were more frequent in women than in men, and tobacco smoking was more frequent in men than in women.
Moreover, almost 60% of our patients presented at least one cardiovascular risk factor or comorbidity, which increases the overall cardiovascular risk.60–62 In spite of that, the median adjusted Framingham score for Colombia in our study population is 0.18% (0.02–1.59), which is less than what has been reported in Latin America. 26 It must be considered that a third of our population was younger than 30 years, thus explaining the low result on Framingham risk score. However, the prevalence of the adjusted Framingham risk score higher than 20% was 0.6% and in people older than 50 years was 3.4%, still lower than other cohorts.62–65
On the other hand, the prevalence of metabolic syndrome found in our cohort was lower than what has been reported in both high and low-middle income scenarios.26,65–67 Likewise, almost a third of the population was either obese or overweight which is more consistent with data from high-income scenarios.61,68–70
The reduction of the HIV-associated mortality has allowed PLWHIV to have a longer life expectancy; hence being exposed to aging, chronic inflammation, and ART. We found that the comorbidities were more common in people older than 50 years which has been described previously.35,36 Therefore, active follow-up should be performed in this population in order to establish pharmacological and non-pharmacological interventions for addressing comorbidities and modifiable risk factors.
Our study has several limitations. First, we did not include the type of ART within the variables because the main objective of the study was to describe the prevalence of cardiovascular risk factors and metabolic comorbidities in the population with HIV. Additionally, our retrospective data are limited by what was documented in the electronic medical records; thus, we might have an information bias. Also, the Framingham risk algorithm adjusted to Colombia was selected for the measurement of cardiovascular risk. However, it is known that this type of algorithm can underestimate the risk in PLWHIV, but none of the alternative algorithms proposed, such as pooled cohort equation, the DAD, or others, have proven to be superior.61,70,71
Lastly, the sample size was obtained estimating a prevalence of comorbidities of 30%; however, the majority of the reported comorbidities in our paper are below this percentage which would make our sample to have representativity issues of the studied population. Also, VIHCOL does not include all PLWHIV in the country, people from the subsidized health system represented 28.1% of our sample, whereas in the country they represent 37.2%.. 27 Lastly, some cities such as Barranquilla and Medellin with a high burden of HIV have few centers affiliated to VIHCOL. Therefore, further Colombian comorbidities prevalence studies need to be conducted in order to obtain representativity by using a sample calculation with less estimated frequency of comorbidities and all regions included considering a cluster effect.
Conclusions
In this study of PLWHIV, comorbidities such as HBP, T2DM, and active tobacco smoking were less frequent than what has been described in high-income countries. This might be explained by the median age of our population as well as a short follow-up period from HIV diagnosis.
However, there is a high prevalence of modifiable risk factors such as dyslipidemia and active tobacco smoking, which might be subject to multiple interventions. Most of the cardiovascular risk factors are more prevalent in people older than 50 years, except for active tobacco smoking which is higher in people 50 years of age or younger. In PLWHIV, active screening and treatment of modifiable risk factors must be prompt and comprehensive.
Footnotes
Author contributions
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Merck Sharp and Dohme.