
Abstract
Mother-to-child transmission of HIV (MTCT) accounts for a significant proportion of new HIV infections in Peru. The purpose of this case–control study was to examine maternal and infant factors associated with MTCT in Peru from 2015 to 2016. For each biologically confirmed case infant, we randomly selected four birth year- and birth hospital-matched controls from five hospitals in Lima-Callao. Maternal and infant information were gathered from medical records. Simple conditional logistic regression was utilized to examine possible maternal and infant characteristics associated with MTCT. The rate of MTCT was 6.9% in 2015 and 2.7% in 2016. A total of 63 matched controls were identified for 18 cases. Protective factors included higher number of prenatal visits (odds ratio [OR]: 0.72; 95% confidence interval [CI]: 0.55–0.94, p = 0.012) and having more children (OR: 0.10, 95% CI: 0.01–0.79, p = 0.029). Risk factors included later maternal diagnosis (OR: 1.19; 95% CI: 1.06–1.34; p = 0.001) and greater viral load at the time of maternal diagnosis (OR: 1.05; 95% CI: 1.01–1.10; p = 0.022). Our study highlights the importance of targeting early and continued prenatal care as specific areas to target to prevent gaps in the HIV treatment cascade for pregnant HIV-infected women. These strategies can ensure early screening and initiation of antiretroviral therapy to reduce MTCT rates.
Introduction
Mother-to-child transmission of HIV (MTCT) remains an important public health issue in Peru. Although the HIV epidemic in Peru is concentrated among men who have sex with men (MSM), MTCT remains an important cause of new infections in Peru, accounting for 5.6% of all new HIV infections among children and adults from 1986 to 2012. 1 As outlined in the National Plan for the Elimination of Maternal-to-Child Transmission of HIV, Syphilis, and Hepatitis B (2017–2021), Peru’s Ministry of Health (MINSA) has proposed to reduce MTCT to less than 2% by the year 2021. 2 To achieve this, MINSA utilized the internationally recognized HIV care cascade framework to describe a stepwise progression from HIV screening to engagement in medical care, antiretroviral (ARV) therapy, and ultimately, viral load (VL) suppression. 3 To identify gaps in prevention of MTCT, MINSA explored the possible barriers preventing advancement in the HIV care cascade in pregnant HIV-infected women using programmatic data from 2011 to 2014. Despite efforts to reduce MTCT, more than 5% of exposed children were infected with HIV during this period, compared to approximately 1% in the United States.4,5
In the Global Plan Towards the Elimination of New HIV Infections Among Children by 2015 and Keeping their Mothers Alive, the Joint United Nations Program on HIV/AIDS put forth the objectives of reducing new infections among infants by 90%, and reducing maternal deaths due to HIV by 50%. 6 To achieve these goals, MINSA has set specific landmarks to reach within the HIV care cascade for pregnant women, including: (1) reducing MTCT to 5% by 2015, with a goal of less than 2% by 2021; (2) ensuring that 90% of HIV-infected pregnant women receive ARV prophylaxis during the prenatal period; (3) ensuring that 90% of HIV-positive mothers receive postpartum ARVs; and (4) ensuring that 90% of all HIV-infected pregnant women achieve lifelong ARV adherence. 4 However, in the steps that occur between initial HIV diagnosis in pregnant women and eventual viral suppression, two important impediments have been observed: first, only an estimated 88% of pregnant women receive prenatal care, and second, only about 70% of pregnant women are screened for HIV. 4 This is an important deficiency to address because of the recognized importance of regular attendance at prenatal care visits, both for HIV screening and care but also to ensure optimal perinatal outcomes for the mother and infant. In fact, the World Health Organization recommends that pregnant women have their first prenatal visit within the first 12 weeks of gestation with regular checkups thereafter for a minimum of eight contacts throughout their antenatal care, which has been shown to reduce perinatal deaths by up to 8 per 1000 births when compared to only four or fewer visits. 7
However, though possible gaps in prenatal care and maternal HIV screening have been identified by the Peruvian Ministry of Health, it is unknown whether these factors are significantly associated with increased risk for MTCT. Thus, in order to better understand the factors associated with MTCT, we conducted a small case–control study to further pinpoint maternal, pregnancy, and infant characteristics that may be associated with MTCT. This valuable information can then be used in context to inform resource allocation and intervention implementation leading to subsequent improvements to work toward the goal of the elimination of MTCT in Peru.
Methods
We conducted a case–control study of HIV-infected and HIV-negative, but HIV-exposed children in the metropolitan area of the capital, Lima-Callao during 2015–2016. In the Lima-Callao metropolitan area, the most populous area of the country, a total of 188,373 live births were registered in 2016, accounting for approximately 30% of all live births in Peru in that year. 8 Study cases and controls were drawn from five maternity and general hospitals with maternity wards in metropolitan Lima-Callao. The five hospitals selected accounted for 189 of the 302 (63%) infants born to HIV-positive mothers in 2015 and 186 of the 280 (66%) exposed infants in 2016. Cases were defined as children newly diagnosed with HIV as indicated by measurable quantities of HIV mRNA on two separate mRNA PCR readings before 18 months of age. 9 For each case, we randomly selected four controls when available, defined as children born to HIV-infected mothers, matched with cases on year of birth and hospital of birth. Because all hospitals are required to keep a standardized registry of pregnant mothers with HIV together with information on the newborn infant exposed to HIV (whether HIV-infected or not), we were able to use this pool of children exposed to HIV (i.e. born to HIV-infected mothers) as the source population.
We reviewed medical records, collecting data related to individual factors in four main categories: (1) maternal demographics (maternal age at beginning of pregnancy, highest level of education completed, etc.); (2) prenatal information (number of prenatal visits completed, gravidity, parity); (3) maternal HIV diagnosis information (gestational age at the time of maternal diagnosis, whether ARVs had been prescribed, delivery type, VL, and CD4+ cell count at the time of diagnosis); and (4) infant birth history (gestational age at birth, birthweight, whether infant was breastfed or formula-fed or both, vital status). Data were gathered utilizing a standardized data retrieval form, with infant and maternal information collected on the same document.
Rates of MTCT were calculated by hospital/maternity ward and year, and differences in MTCT rates were assessed using two-sample tests for proportions. Group estimates and distributions of maternal and infant characteristics were described separately for cases and controls based on available data. Our source population was limited to HIV-infected pregnant women who gave birth at any of the five hospitals under study. Women could have been diagnosed as HIV-positive: (a) prior to the index pregnancy, (b) during antenatal care for the index pregnancy, (c) during labor and delivery for the index pregnancy, and (d) in the postnatal period for the index pregnancy. Because of the expected rarity of the event of interest, it was not appropriate to build multivariable models in our analysis. 10 Thus, simple conditional logistic regression was utilized, using birth hospital as the matching characteristic, to examine possible maternal and infant characteristics associated with MTCT. All statistical analyses were performed using Stata 15.0 (StataCorp, College Station, TX). This study was approved by the IRB of the Universidad Peruana Cayetano Heredia.
Results
There was a total of 18 reported cases of MTCT during the study period (13 in 2015 and 5 in 2016) across the five major maternity hospitals/wards in metropolitan Lima-Callao. The vertical transmission rate was 6.9% in 2015 and 2.7% in 2016 (Table 1). There was a wide range in the transmission rate depending on the hospital, from 3.3 to 21.4% in 2015 to 0 to 6.8% in 2016. A total of 63 birth year-matched and birth-hospital matched controls were identified for the 18 reported cases during the study period. Although the collection of maternal and infant data for pregnant women diagnosed with HIV is standardized in Peru, review of medical records revealed incomplete registries of maternal and infant information. Lack of complete records was primarily due to resource limitations leading to multifactorial deficits, including poor organization of records, lack of dedicated nursing and administrative teams for MTCT, and inadequate follow-up of exposed children. Table 2 describes the maternal, prenatal, and infant characteristics for the available samples of cases and controls. Mean maternal age at beginning of pregnancy was 27.1 years for controls, with a standard deviation (SD) of 5.7 years and mean maternal age for cases was 35.8 years with a wider distribution (SD: 23.9 years).
Rates of MTCT by hospital/maternity ward and year.
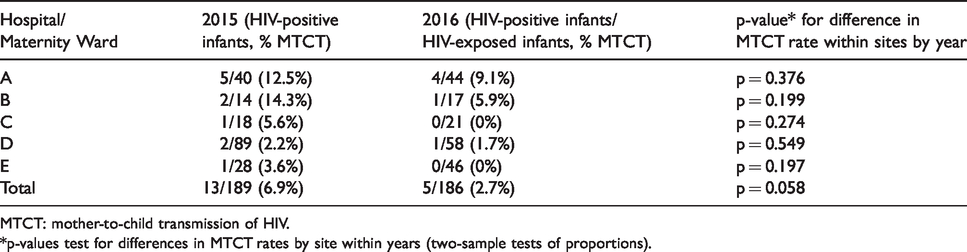
MTCT: mother-to-child transmission of HIV.
*p-values test for differences in MTCT rates by site within years (two-sample tests of proportions).
Infant and maternal characteristics.
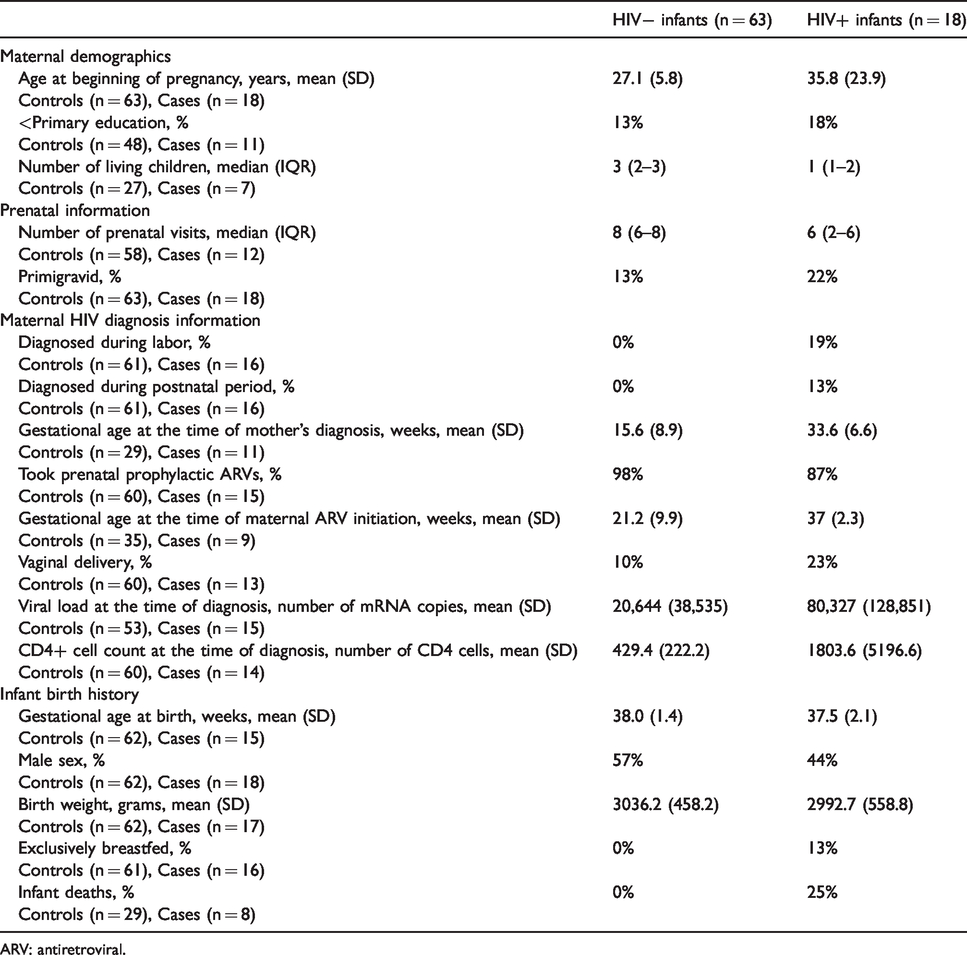
ARV: antiretroviral.
In terms of prenatal data, the median number of prenatal visits attended by control mothers was eight with an interquartile range (IQR) of 6–8 visits, compared to a median of six prenatal visits for case mothers (IQR: 2–6 visits). All (n = 61) mothers of control infants were diagnosed either before the index pregnancy or while receiving prenatal care, whereas 3 of the 16 case mothers (18.8%) were diagnosed during labor, and two cases (12.5%) were diagnosed during the postnatal period. Accordingly, mean gestational age at the time of mother’s diagnosis was 15.6 weeks (SD: 8.9 weeks) for controls and 33.6 weeks (SD: 6.6 weeks) for cases. The majority of control mothers (98.3%) and case mothers (86.7%) were prescribed ARV medications during the prenatal period. The majority of pregnant women who were prescribed ARVs consisted of a regimen that included zidovudine (alone or in combination with other ARVs) to prevent MTCT (data not shown). 11 Mean gestational age at the time of maternal ARV initiation was 21.2 weeks (SD: 9.9 weeks) for controls and 37 weeks (SD: 2.3 weeks) for cases.
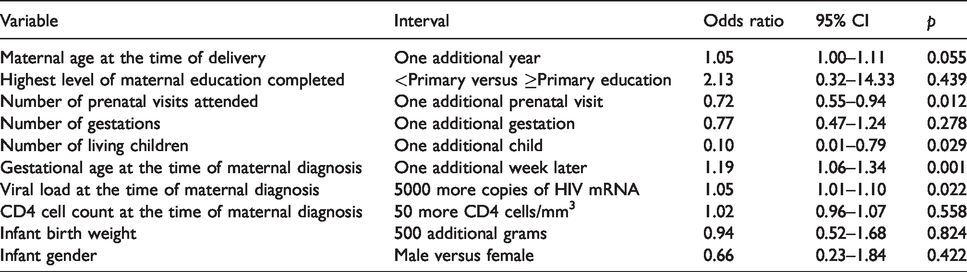
Results of the simple logistic regressions are reported in Table 3. The two protective factors identified were the number of completed prenatal care visits and the number of living children reported by the mother. An increase in one additional prenatal visit was associated with a 28% reduction in odds of MTCT (OR: 0.72; 95% confidence interval (CI): 0.55–0.94; p = 0.012). Each additional living child from previous pregnancies reported by the mother corresponded to an approximately 90% reduction in odds of MTCT (OR: 0.10, 95% CI: 0.01–0.79; p = 0.029). Later maternal HIV diagnosis was a significant factor: each additional week of gestation at HIV diagnosis was associated with a 19% increase in odds of MTCT (OR: 1.19; 95% CI: 1.06–1.34; p = 0.001). Finally, greater VL at the time of maternal diagnosis was also associated with MTCT, with each additional 5000 copies of HIV mRNA associated with a 5% increase in odds of MTCT (OR: 1.05; 95% CI: 1.01–1.10; p = 0.022).
Simple conditional logistic regressions.
Discussion
In this small case–control study of the reported cases of MTCT in Metropolitan Lima-Callao for 2015–2016 and birth year- and hospital-matched controls, we found significant associations between increased odds of MTCT with individual characteristics including delayed maternal diagnosis and later time to initiation of ARV therapy with respect to the length of the pregnancy. We also found decreased odds of transmission in non-primigravid women. It is important to highlight that of the 65 multigravida women, 28 were diagnosed before the index pregnancy, 35 were diagnosed during antenatal care for the index pregnancy, and two were diagnosed in the postnatal period (data not shown). Thus, being multigravida may decrease odds of MTCT because of increased likelihood of being diagnosed during antenatal care visits.
The only characteristics significantly associated with decreased odds of MTCT were total attendance at a greater number of prenatal visits, younger gestational age at the time of maternal diagnosis, decreased VL at the time of maternal diagnosis, and greater number of living children. The last of these factors has been found to be associated with decreased odds of late presentation to antenatal care. 12 Thus, taking these results together, the factors that may help ensure that pregnant women initiate and proceed through the care cascade steps between initial screening/diagnosis and HIV viral suppression include: (a) early and continued attendance at prenatal care visits, which influences (b) earlier gestational age at the time of maternal diagnosis, allowing for (c) decreased VL at the time of maternal diagnosis, and (d) earlier gestational age at the time of ARV initiation. A review of breaches in the MTCT care cascade in Brazil similarly highlighted failure to attend prenatal care, late maternal diagnosis, and an incomplete ART regimen during pregnancy as important risk factors for MTCT. 13
Study limitations
Our study was limited by a small sample size and lack of complete records for all case and control patients. Two of the five hospitals included in this study did not have a full-time team dedicated to MTCT, which likely contributed to poor follow-up of children exposed and poor organization of records. The missing data due to incomplete records limit the statistical power of our analyses by further reducing the sample size. 14 Information regarding ARV adherence was also not available in the records, limiting our ability to comment only on the ARV regimen prescribed to study participants. Additionally, given that the current study only encompassed cases of MTCT in metropolitan Lima, the findings of this study are potentially not generalizable to the entire Peruvian population.
The importance of prenatal care for the prevention of MTCT and possible strategies for improvement
Our findings regarding the protective association between prenatal care visits and decreased odds of MTCT are in line with other studies that have found similar associations.15,16 In fact, a case–control study of 231 women with HIV-infected infants and 154 with HIV-uninfected infants in Johannesburg, South Africa found that accessing prenatal care after 20 weeks of gestation was associated with a 4.3-fold increase in odds of MTCT (adjusted odds ratio: 6.6; 95% CI: 2.4–18.4; p < 0.001). A similar finding has also been described in Brazil, where a retrospective matched case–control study in Rio de Janeiro demonstrated that cases were significantly less likely than controls to receive care throughout the cascade, due to lack of care-seeking. 17 Our finding that women reporting having more living children had decreased odds of MTCT is also supported in the literature, with one study finding that multigravida women were less likely to exhibit late presentation to antenatal care, thereby linking together these two protective factors. 12 It is important to note, however, that all mothers of case infants attended prenatal care visits with the median number of visits being six, compared to eight for mothers of control infants. This may suggest that it is not simply the quantity of prenatal care visits, but also the quality of those visits that may have contributed to this protective association.
In order to potentially encourage early initiation and increased total number of prenatal care visits, interventions focused on training peer health promoters armed with mobile health technology to reach ‘harder-to-reach’ pregnant women who live in shantytowns/slums in the outskirts of metropolitan Lima/Callao may prove to be effective. A similar intervention – the Mama River Program – has been implemented in the Peruvian Amazon with impressive results: the proportion of pregnant women who had their first prenatal visit during the first trimester tripled from 33.3 to 96.1%, and there was also an increase in the proportion of pregnant women who completed six or more prenatal visits (from 70.6 to 96.1%). 18 Additionally, improvements to Peru’s fragmented healthcare system through eHealth interventions like WawaRed to link together prenatal health records at local health centers to regional hospitals and MINSA can also help to improve communication between health centers to better coordinate prenatal care.19,20
The importance of early HIV screening to prevent MTCT and possible barriers in the Peruvian context
Early initiation of prenatal care is a necessary step to ensure early HIV screening of pregnant women. The association between diagnosis at a later stage in pregnancy and increased odds of MTCT in our present study harmonizes with results in the published literature demonstrating that lack of awareness of HIV status and late diagnosis of HIV infection place newborns at increased odds of MTCT.21,22 In a case–control study of 45 cases and 45 controls conducted in rural Kenya, Okoko et al. 21 found that in the extreme case of lack of awareness of HIV status, the odds ratio of MTCT increased by a factor of 5.6 (OR: 5.6; 95% CI: 2.2–14.5). Early screening of pregnant women is a necessary step to ensure lower VL at the time of diagnosis. Similar associations between increased VL at the time of maternal diagnosis and increased odds of MTCT have been reported previously.22,23 In an effort to analyze missed opportunities for prevention of MTCT, Read et al. 22 analyzed cases of MTCT at multiple sites in Latin America and the Caribbean and found that poor control of maternal VL during pregnancy was the most common missed opportunity. Additionally, VL at the time of diagnosis has also been found to be an important factor to consider when examining MTCT. A 2012 study by the London HIV Perinatal Research group demonstrated that when baseline VL is greater than 10,000 copies/ml, the probability of achieving less than 50 copies/ml by the time of delivery is compromised if ARV is initiated beyond 20.4 weeks’ gestation. 24
However, cost is a substantial barrier to the implementation of universal screening for HIV in pregnant women in Peru. A cost-effectiveness analysis conducted by Aldridge et al. 25 evaluating different HIV prevention strategies for various key populations in Peru estimated that to achieve 80% coverage for screening all pregnant women for HIV, it would cost $41.1 million annually, averting 2092 infections yearly. However, of all of the interventions analyzed for different key populations, prevention of MTCT through screening 80% of all pregnant women for HIV had the lowest total cost effectiveness ($5928 per DALY averted, compared to $1330 per DALY averted for screening 80% of Peruvian MSM), though also had a lower total unit cost for treatment ($23.20 per mother and child treated versus $103.00 for every MSM reached). 25 Related to this issue is the observation that there is a relative dearth in research dedicated to MTCT compared to HIV prevention research for other key populations in Peru (MSM, transgender women, female and male sex workers).
Early initiation of ARVs is crucial to prevent MTCT, but so is adherence through the postnatal period and beyond
Early screening and detection of HIV in pregnant women is essential for early initiation of ARVs to prevent MTCT. A cohort study in Rio Grande do Sul, Brazil of 262 pregnant HIV-infected women recruited between 2003 and 2007 by Barral et al. 15 demonstrated that maternal VL of 1000 or greater was associated with a five-fold increase in the prevalence ratio of MTCT. 22 Furthermore, evidence of HIV subtype recombinants has been found in samples of HIV-positive children infected through MTCT in Peru, indicating the continuing evolution of HIV infection in the country. 26 Thus, to prevent issues related to increasing ARV-resistant strains of HIV, it is important to initiate early ARVs, but adherence is just as essential.
The issue of adherence does not end at the time of delivery. Postnatal adherence to ARVs is essential to prevent MTCT if the mother breastfeeds her newborn. In an analysis of ARV adherence among pregnant and postpartum women in Latin America by Kreitchmann et al., 27 there was a statistically significant decline in perfect adherence to ARVs during the postpartum period (80% at 6–12 weeks and 82% at six months) compared to reported adherence during pregnancy (90.4%). This is an important issue to keep in mind in the context of metropolitan Lima-Callao, since the mothers of 2 of the 16 cases of MTCT were diagnosed in the postpartum/breastfeeding period (12.5%). Of note, the official recommendation of the Ministry of Health of Peru is the suspension of breastfeeding in HIV-infected mothers who are instead provided with formula during monthly check-in visits. 9
Thus, although the health systems in Peru have successfully been able to provide access to ARV therapy to pregnant HIV-infected women, significant areas of improvement in the care cascade to ensure greater HIV screening/diagnoses, treatment, and eventual viral suppression for this population remain in three key areas: (1) ensuring early prenatal HIV testing of pregnant women, (2) increasing quality prenatal care visits, and (3) achieving early initiation of ARV therapy for pregnant HIV-infected women. Future studies aimed at closing these gaps and thereby reducing MTCT should focus on evaluating interventions targeting these specific points in the continuum of care.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center of the National Institutes of Health under Kuskaya: an Interdisciplinary Training Program for Innovation in Global Health (award number D43TW009375 supplement).