
Abstract
In response to an increase in heterosexual syphilis notifications in Tokyo, we conducted a questionnaire-based case–control study among women aged ≥20 years and sexually active in the past six months who sought a syphilis test in Tokyo during 2017–2018. Cases were women diagnosed as recent syphilis infection based on serological tests. Controls were serologically non-reactive or those with only a past syphilis infection. We described cases and assessed for risk factors of recent syphilis using logistic regression. A total of 524 women (60 cases, 464 controls) were enrolled. Notably, among cases, 10 (16.7%) were students, 3 (5.0%) had a history of syphilis, and 14 (23.3%) had a single sex partner in the past six months. Female sex worker (FSW) status was strongly associated with syphilis (odds ratio [OR] = 3.40; 95% confidence interval [CI] = 1.96–5.90). In multivariable analysis, recent syphilis was associated with inconsistent condom use for vaginal/anal sex among FSWs (adjusted OR [aOR] = 3.42; 95%CI = 0.92–12.70) and among non-FSWs, with younger age (aOR = 0.36; 95%CI = 0.19–0.70; increase per category from 20–24, 25–29 to ≥30 years) and ≤high school education (aOR = 5.24; 95%CI = 1.95–14.10). A notable proportion of cases were those with first time infection and those with only a single partner. Moreover, risk factors differed between FSWs and non-FSWs, and a multi-pronged approach to prevent syphilis is required.
Keywords
Introduction
Globally, an estimated 5.6 million new cases of syphilis are diagnosed yearly, with the majority in low- and middle-income countries.1,2 In many high-income countries, syphilis control succeeded during the 1990s, 3 but resurgence has been reported since then, disproportionately occurring among men who have sex with men (MSM).3–6 However, more recently, increased notifications among non-MSM populations, particularly women, have been reported.5,7,8 Japan, for instance, has seen an increase in syphilis notifications since 2013, with a substantial increase among both men who have sex with women (MSW) and women who have sex with men (WSM); between 2013 and 2016, cases increased from 304 to 1671 among MSW and 137 to 1077 among WSM. 9
Several studies have reported risk factors for syphilis among women, such as socioeconomic and education status and sexual behavior.10–12 In Japan, such information has been lacking, with only one study reporting young age being associated with higher syphilis positivity in pregnant women. 13 As Tokyo accounts for nearly a third of all reported female syphilis cases in the current outbreak, we conducted a case–control study to identify risk factors for recent syphilis infection among WSM in Tokyo.
Methods
Study population and enrollment
The study was conducted at five women’s health clinics under a single medical association in Tokyo from June 2017 to March 2018. The major reasons for accessing the clinics are for obstetrics (10% for prenatal care, contraception, or abortion) and gynecology (15% sexually transmitted infection [STI]-related and 75% other [i.e. menstrual issues, cancers, menopausal disorder]). For those seeking STI tests, patients with signs/symptoms indicative of STIs are covered by national health insurance, while asymptomatic individuals can self-pay for a screening test. The patient age distribution is young, with more than half in their 20s and the majority of the remaining in their 30s and 40s.
In this case–control study, we adopted a test-negative approach, including all participants who tested negative for recent syphilis infection and satisfying the criteria as controls, based on the following reasons: efficiency, feasibility (considering the timing of patient testing, notification of results, and privacy), and comparability between cases and controls for healthcare-seeking behaviors. Eligible participants were Japanese-speaking women aged ≥20 years who received a syphilis test in these clinics and reported sexual activity (i.e. oral sex, vaginal/anal intercourse) only with men and were not treated for syphilis in the six months prior to study entry. Participants could take part in the study only once.
As commonly practiced in Japan for syphilis serodiagnosis at initial assessment, all participants received treponemal and non-treponemal tests in parallel, both of which measured quantitative titers. A case was defined as a woman diagnosed as syphilis based on serologically reactive results by both treponemal and non-treponemal tests, with or without signs/symptoms; tertiary syphilis cases were not included as the focus was on recent infection. A control was defined as a woman with serologically non-reactive results by both treponemal and non-treponemal tests or those with only an infection history.
When an eligible patient received a syphilis test after clinical examination, a study clinician offered study participation and the patient was enrolled after providing written informed consent. A study clinician provided the participant a questionnaire and an envelope with a label containing participant information, after recording the patient ID and examination date. The participant completed the self-administered questionnaire in a private area, sealed the envelope, and returned it in exchange for a gift card as compensation. On a subsequent day, the clinician entered the serological test results, the status of each participant, and the stage of syphilis if a case (primary, secondary, or asymptomatic, according to the Japanese national surveillance system categories; the asymptomatic category could include early and late latent syphilis) on the envelope label, by patient ID.
Based on initial assumptions that no more than a quarter of participants would test positive for syphilis, ∼30% exposure among controls for a characteristic (e.g. commercial exchange of sexual practices), and a two-tailed significance level of 5% and 80% power, enrollment of 36 cases and 108 controls was expected to detect a minimal odds ratio (OR) of 3. Considering potential missing data and planned subanalyses, we continued recruitment for the duration of the study period even after reaching this target.
Data collection
From the recorded label on the envelope, we gathered the following data: examination date, test results, case status, and stage of syphilis for cases. The enclosed questionnaire confirmed heterosexual activity in the past six months before participation and inquired regarding sociodemographic characteristics, recent sexual activity, history of STIs, the reason(s) for seeking a syphilis test, and awareness regarding an increase in syphilis in Japan. Data on recent sexual behavior included the number of sex partners; frequency of sex and condom use (oral or vaginal/anal; none, inconsistent [sometimes/often], consistent [always]); sex with a casual partner(s); sex with a partner(s) of non-Japanese nationality (who is not a spouse or steady partner); and meeting a sex partner(s) via mobile applications or online social networking services (SNSs).
Additionally, we asked about commercial exchange of sexual practices in the past six months. As Japan’s sex industry is diverse, we classified the various types as follows (partially based on the Metropolitan Police Department categorization): (1) established ‘store’ type (women employed by a company and providing services in a designated building); (2) dispatch type (i.e. escort service, where women are dispatched to an ad hoc location such as a hotel); (3) private (women soliciting sex through mobile applications/SNSs on their own); and (4) other.14,15 Participants fulfilling any of the above were categorized as female sex workers (FSWs). The survey was piloted for a month and revised before implementation.
Laboratory testing
A commercial laboratory performed all tests for syphilis. The laboratory tested serum by using the automated rapid plasma reagin test (RPR; Rapidia Auto RPR®, Fujirebio Co., Tokyo, Japan) as the non-treponemal test and the automated Treponema pallidum latex agglutination test (TPLA; Rapidia Auto TP®, Fujirebio Co., Tokyo, Japan) as the treponemal test.
Data analysis
We analyzed the data using STATA version 13 (StataCorp LP, Texas, USA). First, key characteristics of cases and controls were summarized to describe the background characteristics of the participants and their reasons for seeking syphilis testing. Next, we compared sociodemographic and sexual behavioral characteristics in cases and controls to identify factors associated with syphilis infection. Univariate logistic regression was used to calculate ORs and their 95% confidence intervals (CIs).
As we posited that FSW status would modify the relationship between the factors of interest and syphilis, univariate logistic regression results were stratified by FSW status. Then, based on a hypothesized directed acyclic graph, we analyzed the association between condom use and syphilis case status, accounting for hypothesized confounders of age, educational attainment, number of sex partners, and frequency of vaginal/anal sex, stratified by FSW status.
Results
Description of the study population
A total of 578 women participated. After excluding those that did not fulfill the inclusion criteria (Figure 1), 60 cases and 464 controls remained. The 60 cases (20 primary, 27 secondary, and 13 asymptomatic) accounted for ∼13% of all female syphilis notifications in Tokyo during the study period. With regard to sociodemographic characteristics, most participants were Japanese, Tokyo residents, and unmarried (Table 1).
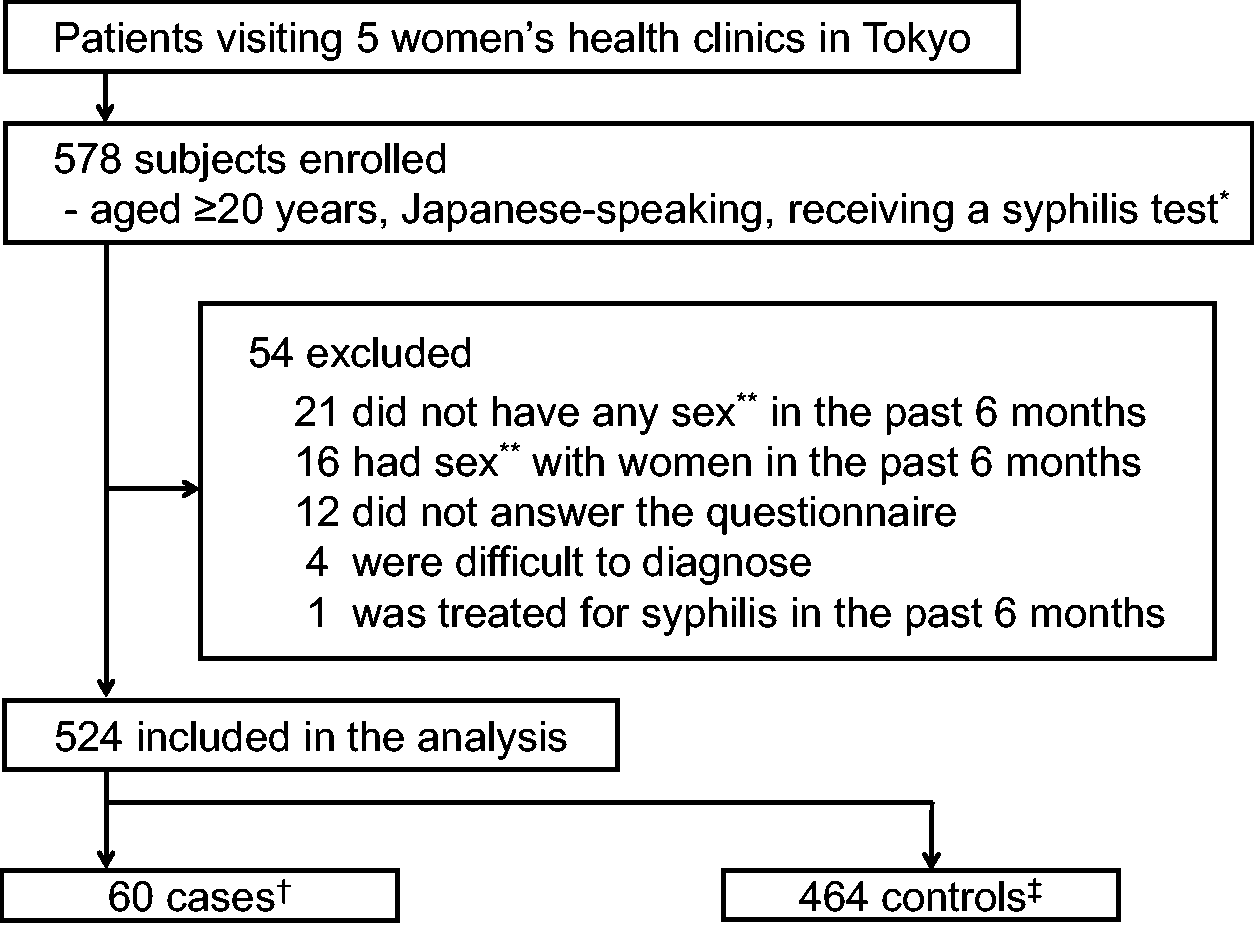
Flow chart of study participant selection.
Sociodemographic characteristics of study participants and reasons for visiting the clinic, by case status.
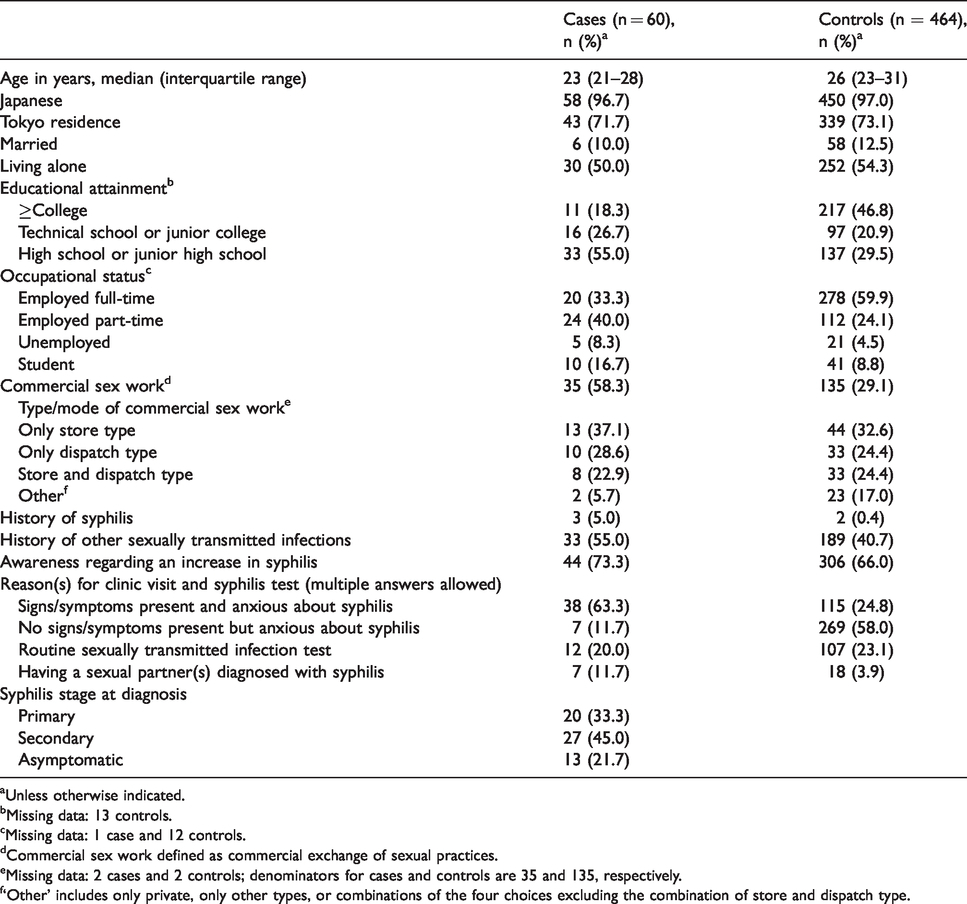
aUnless otherwise indicated.
bMissing data: 13 controls.
cMissing data: 1 case and 12 controls.
dCommercial sex work defined as commercial exchange of sexual practices.
eMissing data: 2 cases and 2 controls; denominators for cases and controls are 35 and 135, respectively.
f‘Other’ includes only private, only other types, or combinations of the four choices excluding the combination of store and dispatch type.
Relative to cases, controls were older, more likely to be working full-time and had higher educational attainment, with nearly half of controls being college graduates. There were nearly twice as many students among cases than controls. Thirty-five (58.3%) cases and 135 (29.1%) controls were FSWs, and there was limited heterogeneity in the type/mode of commercial sex work; the store and dispatch types accounted for 88.6% of FSWs in cases and 81.5% of FSWs in controls (Table 1). Only three (5.0%) cases and two (0.4%) controls had a history of syphilis, considerably lower compared to a history of other STIs for both groups (55.0% and 40.7%, respectively). Awareness of an increase in syphilis was higher among FSWs (cases 82.8%, controls 73.3%) than non-FSWs (cases 60.0%, controls 62.8%). The reason(s) for a syphilis test differed between cases and controls, but FSWs were more likely to test positive regardless of the reason; and, while a routine test was more likely to be reported by FSWs (67/170, 39.4%) than non-FSWs (52/353, 14.7%), FSWs were still more likely to test positive than non-FSWs (9/67 [13.4%] vs. 3/52 [5.8%], respectively). Additionally, restricted to symptomatic patients, 57.9% (22/38) of cases were FSWs relative to 22.6% (26/115) of controls.
Variables associated with syphilis, univariate analysis
Cases were strongly associated with younger age, lower educational attainment, not working full-time, and being an FSW (Table 2). There was a dose–response trend with an increase in the OR with increase in frequency of sex, for both oral and vaginal/anal sex (Table 2). While having ≥6 sex partners was associated with a two-fold increased odds relative to those with one partner (OR = 2.02; 95%CI = 0.97–4.22), 14 (23.3%) cases had a single sex partner in the past six months, and 12 of them reported that the partner was steady. Consistent condom use was uncommon, and inconsistent/no use in vaginal/anal sex was associated with a two-fold increased odds relative to consistent use (OR = 1.96; 95%CI = 0.90–4.27). We had hypothesized that the protective effect of condom use would be most present among FSWs (based on the sexual partners that they would encounter), and restricted to FSWs, the association between case status and condom use increased.
Key sociodemographic and sexual behavior characteristics, univariate analysis.

CI: confidence interval; FSW: female sex worker.
a‘>High school’ includes graduate or current student in technical school, junior college, college, or graduate school.
b‘Other’ includes those employed part-time, unemployed and students.
Variables associated with syphilis, univariate and multivariable analysis, stratified by FSW status
Stratified by FSW status, inconsistent condom use was associated with increased odds of syphilis only among FSWs, while younger age was associated with a greater OR only among non-FSWs (Table 3). Lower educational attainment and non-full-time employment were associated with an increased odds of case status among non-FSWs. Number of sex partners or frequency of vaginal/anal sex were not strongly associated with syphilis in both groups.
Selected characteristics and sexual behavior, univariate and multivariable analysis, stratified by female sex worker status.

aOR: adjusted odds ratio; CI: confidence interval.
aAdjusted for each other for variables listed in the adjusted odds ratio column.
bIncrease per age group based on univariate analysis results.
c‘>High school’ includes graduate or current student in technical school, junior college, college, or graduate school.
d‘Other’ includes those employed part-time, unemployed, and students.
eCategorized dichotomously based on strata distribution or univariate analysis results.
Adjusted for age, educational attainment, number of sex partners, and frequency of vaginal/anal sex, while not statistically significant (p = 0.07), inconsistent condom use remained associated with a three-fold increased odds of syphilis among FSWs. Among non-FSWs, the association between inconsistent condom use and case status remained weak, while the OR decreased with increase in age group (adjusted OR [aOR] = 0.36; 95%CI = 0.19–0.70) and increased with lower educational attainment (aOR = 5.24; 95%CI = 1.95–14.10). Occupational status was not included as we hypothesized that this would be an outcome of education; including it in the model made little difference in educational attainment (aOR = 4.93; 95%CI = 1.79–13.58), while the OR for occupational status was considerably reduced (aOR = 2.29; 95%CI = 0.84–6.24).
Discussion
Our study revealed important sociodemographic, behavioral, and clinical characteristics of WSM with incident syphilis infection in Tokyo. A strength of this study was that we included non-FSWs and identified important differences between FSWs and non-FSWs regarding syphilis infection.
Among the 60 cases, 51 (85.0%) were in their 20s and 47 (78.3%) were symptomatic; these features were similar to syphilis cases reported from Tokyo through notifiable surveillance (data not shown). Only 5% of the women had a history of syphilis, indicating that recent syphilis infections were occurring in a previously uninfected population. Notably, nearly a quarter of all cases had only one sex partner in the past six months; with increased syphilis prevalence, the risk of infection for such women may have increased. Additionally, 17% of the cases were students. Recent syphilis infections in these women in Tokyo suggest that syphilis may have spread into groups traditionally not considered to be at high risk and may require tailored interventions. Importantly, consistent condom use was uncommon, particularly for oral sex.
Previous reports have found FSWs to be associated with non-MSM syphilis outbreaks,12,16,17 and in this study, FSW status was associated with a three-fold increase in the odds of syphilis. As the majority of FSWs was ‘store and dispatch type’, reaching these populations for prevention may be more feasible than ‘private’ FSWs. Moreover, although some recent studies have reported meeting sex partners online as a risk factor for syphilis in MSM,18–20 we did not find this in our population, whether FSW or non-FSW.
Among FSWs, inconsistent condom use during recent vaginal/anal sex was associated with recent syphilis infection, consistent with the literature.7,21Although not statistically significant (p = 0.07), the OR remained high in multivariable analysis (aOR = 3.42; 95%CI = 0.92–12.70), similar to the univariate results (OR = 3.95; 95%CI = 1.44–10.86). Consistent with epidemiologic practice and increasing guidance against interpretations that are based on statistical significance,22,23 we emphasize the magnitude of association, as reflected by the aOR. Moreover, this result was in the context of mostly unprotected oral sex among both cases and controls. We had hypothesized that the protective effect of condoms would be more present among FSWs because of their partners; persons who have sex with FSWs likely represent a higher risk group with higher prevalence of syphilis infection. In addition, despite having high awareness of an increase in syphilis, the proportion of symptomatic cases was 82.8% (29/35) among FSWs, higher than that of women in other developed countries.5,24 As the cost of regular screening tests was pointed out by some participants as a barrier, opportunities for free testing could be increased.
Concerning non-FSWs, young age and lower educational attainment were independent risk factors for syphilis. The association with young age agrees with national surveillance data and findings among pregnant Japanese women.9,13 The strong association with lower educational attainment was also consistent with findings from mothers of congenital syphilis in Japan and reports from other countries.10,11,25 Notably, more than half of the cases among non-FSWs reported only one sex partner in the past six months. While self-reported, these data suggest that, in addition to the rising prevalence of syphilis, the risk for these women is dependent on their partners’ risk for syphilis. We posit that such a partnership is likely to be associated with educational attainment, an indicator of socioeconomic status (SES). Education is a well-established indicator of SES and has frequently been used to evaluate the association between SES and various health issues in Japan.26,27 Moreover, education can affect not only income and employment but also a person’s social network, which could affect syphilis risk. In the current context of a large-scale syphilis outbreak predominantly affecting heterosexuals, those who do not show high-risk behaviors but are of lower SES may be facing an increased risk. Taken together, there are likely social determinants of syphilis in Japan and warrant further research.
Considering these results, we should recognize that there may be an increased risk of syphilis in Tokyo, even in those expected to have relatively low risk, and emphasize preventive measures. Firstly, there should be efforts to increase consistent condom use, particularly among FSWs. There should also be more opportunities for testing (e.g. free or low-cost screening tests), especially for asymptomatic persons; the proportion of cases with symptoms was high and those of lower SES without symptoms may have poor access to testing, potentially contributing to further transmissions. Therefore, we should promote prevention, early diagnosis, treatment, and education,28,29 and reach a wide group of young women, including students (e.g. via collaboration with the education sector).
There are potential limitations to our findings. First, our findings require caution with generalizability given that our study population was mostly unmarried Japanese women ≥20 years of age seeking healthcare at women’s health clinics in Tokyo. While potentially high-risk women who are younger and those who do not readily seek healthcare at these facilities, such as the homeless, 30 would have been missed, 38.0% (134/353) of non-FSWs had a history of STIs, suggesting a fairly high-risk baseline profile of the participants. Moreover, Tokyo has been at the center of the current outbreak in Japan, and the clinic-based design would have removed biases associated with differential healthcare access between cases and controls. Additionally, syphilis notifications from teenagers accounted for only about 5% of annual female cases in Tokyo (data not shown) and >90% of syphilis cases were Japanese in the Shinjuku public health center’s investigation (data not shown), which was not dependent on the case’s language ability. Second, we did not assess some potential risk factors such as drug use, HIV infection, and a history of incarceration.30,31 However, it has been reported that the proportions of injection drug use as a suspected transmission route among WSM syphilis cases in Japan is <2% and that female syphilis cases with HIV co-infection in Tokyo are rare.9,32 Third, as we did not collect data by partner, frequency of sex or condom use could not be analyzed by partner type; for instance, the association between syphilis risk and condom use may differ whether a partner was casual or steady. Fourth, the effect of the number of partners may be underestimated, owing to missing data. These missing data may reflect a number too large to recall, and cases had a higher proportion missing relative to controls (21.7% vs. 6.9%); in fact, 12/13 cases and 28/32 controls missing partner number information were FSWs, with 11/12 (91.6%) and 18/28 (64.3%), respectively, having a high frequency of vaginal/anal sex (>1 time/week). Lastly, we did not collect detailed information about the partner, including his contact with FSWs. Partner characteristics may be especially important for syphilis risk among non-FSWs, and would be important to consider in future studies. Despite these limitations, findings regarding condom use among FSWs and education level among non-FSWs remained similar in several multivariable models explored as sensitivity analyses (including models restricted to symptomatic patients).
Conclusion
Among WSM in Tokyo, a notable proportion of syphilis cases only had one sex partner in the past six months and the majority of cases were those who were infected for the first time. Recent infection was associated with commercial exchange of sexual practices (mainly through the store and dispatch types), and among FSWs, inconsistent condom use was a risk factor, whereas young age and lower educational attainment were risk factors among non-FSWs. In light of these findings, a multi-pronged approach will likely be important to prevent and control syphilis in Tokyo, for both FSWs and non-FSWs, particularly focusing on the young.
Supplemental Material
sj-pdf-1-std-10.1177_0956462420945928 - Supplemental material for Syphilis in heterosexual women: case characteristics and risk factors for recent syphilis infection in Tokyo, Japan, 2017–2018
Supplemental material, sj-pdf-1-std-10.1177_0956462420945928 for Syphilis in heterosexual women: case characteristics and risk factors for recent syphilis infection in Tokyo, Japan, 2017–2018 by Shingo Nishiki, Yuzo Arima, Takuya Yamagishi, Takashi Hamada, Takuri Takahashi, Tomimasa Sunagawa, Tamano Matsui, Kazunori Oishi and Makoto Ohnishi in International Journal of STD & AIDS
Footnotes
Acknowledgements
The authors greatly appreciate all the physicians and supporting staff of Shinjuku Ladies Clinic, Yoshiyuki Sugishita and staff at the Tokyo Metropolitan Government, and the staff at the Shinjuku-ku Public Health Center for their assistance with the investigation.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The National Institute of Infectious Diseases Ethics Committee approved the study (Registration no. 762) and written informed consent was obtained from all participants. The participants received a 500-Japanese-yen gift card as compensation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Ministry of Health, Labour and Welfare of Japan (H29-Shinkou-Ippan-008).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.