
Abstract
Dolutegravir and doravirine are individually safe and effective antiretroviral therapy (ART) components, but their combined use has not been studied in clinical trials and is not recommended in HIV treatment guidelines. We noted persons with HIV (PWH) receiving dolutegravir with doravirine at our Washington, DC, infectious disease clinic and undertook a service evaluation to understand why providers selected this ART, whether HIV virologic suppression was achieved and identify adverse effects of concomitant use. Case registry and prescriptions data identified 21 PWH receiving concomitant dolutegravir and doravirine with mean follow-up 576.1 days (range 413–751); frequent reasons for switching were multiple ART resistance (57.1%), proton pump inhibitor usage (28.6%) and renal failure (28.6%), with 52.4% switched from protease inhibitor or cobicistat-boosted regimens. Dolutegravir with doravirine alone was prescribed for 60%, and additional ART in 40%. During 12 months follow-up mean CD4 was 585.9 (baseline 570.7) with undetectable viral load in 77.8% (baseline 66.7%). No discontinuations for drug-related adverse events or virologic failure occurred. Dolutegravir with doravirine was well tolerated in small numbers of highly treatment experienced PWH at our clinic, achieving virologic suppression in most. Establishing the efficacy and safety of dolutegravir with doravirine for HIV treatment in randomized trials remains important.
Introduction
The SWORD-1 and SWORD-2 clinical trials demonstrated the safety and efficacy of a two-drug single tablet antiretroviral (ART) regimen containing the integrase inhibitor dolutegravir and the non-nucleoside reverse transcriptase inhibitor (NNRTI) rilpivirine. 1 Doravirine, an NNRTI with similar mechanism of action to rilpivirine, is FDA-approved for the treatment of HIV infection individually or co-formulated with tenofovir disoproxil fumarate (TDF) and lamivudine. 2 Doravirine has attractive pharmacologic properties; it is safe in renal impairment and moderate hepatic impairment, has bioavailability unaffected by timing of meals, and unlike rilpivirine has no significant interactions with proton pump inhibitors. 3 It is metabolized by cytochrome P450 CYP3A4 and CYP3A5, but has few significant drug interactions compared to other antiretrovirals. 4 Additionally, the mutations leading to virologic resistance to doravirine are often distinct from other NNRTIs, so doravirine may retain activity in the setting of rilpivirine resistance. 5
Guideline-recommended ART combinations are the preferred approach for treatment of HIV infection, but the reality of patient care is that regimens with limited clinical outcome data may sometimes become necessary. We recently noted that a small number of patients in our clinic were receiving dolutegravir in combination with doravirine for the treatment of HIV. A pharmacokinetic study in healthy volunteers demonstrated no significant drug-drug interactions between dolutegravir and doravirine. 6 Whilst we hypothesize based on the pharmacologic mechanisms of action that dolutegravir taken with doravirine would be safe and effective as HIV treatment, and both agents are FDA-approved individually, no prospective clinical trial data supports use of this combination, with clinical data limited to a single small case series of 18 elderly PWH in Italy who all achieved virologic suppression on dolutegravir with doravirine as a two-drug ART regimen, with one discontinuation for psychiatric side effects. 7 We conducted a service evaluation of dolutegravir with doravirine use in our clinic in order to establish why PWH were switched to this unusual regimen and to verify that this combination was able to safely achieve adequate virologic suppression.
Methods
We performed a service evaluation utilizing our outpatient HIV clinical case registry and prescription data to identify all PWH receiving care in our outpatient clinic who were prescribed dolutegravir and doravirine contemporaneously. We then accessed the electronic medical record data prospectively collected as part of routine clinical care and conducted chart review to verify that the patient had received both dolutegravir and doravirine and whether any other ART agents were utilized in addition to dolutegravir and doravirine. We examined several pre-specified variables of interest including the reasons for switch from other ART to dolutegravir and doravirine, relevant comorbidities and demographic data, HIV resistance mutations, HIV treatment history and any drug interactions precluding the use of standard ART. We also reviewed the medical record for any side effects of dolutegravir or doravirine, adverse events such as death or hospitalization and to ascertain virologic outcomes and reviewed clinic notes and prescription refill data to ascertain adherence. The protocol used for this quality improvement study was reviewed by the institutional review board at the Washington DC VA Medical Center.
Results
Baseline characteristics of persons with HIV switched to dolutegravir with doravirine.
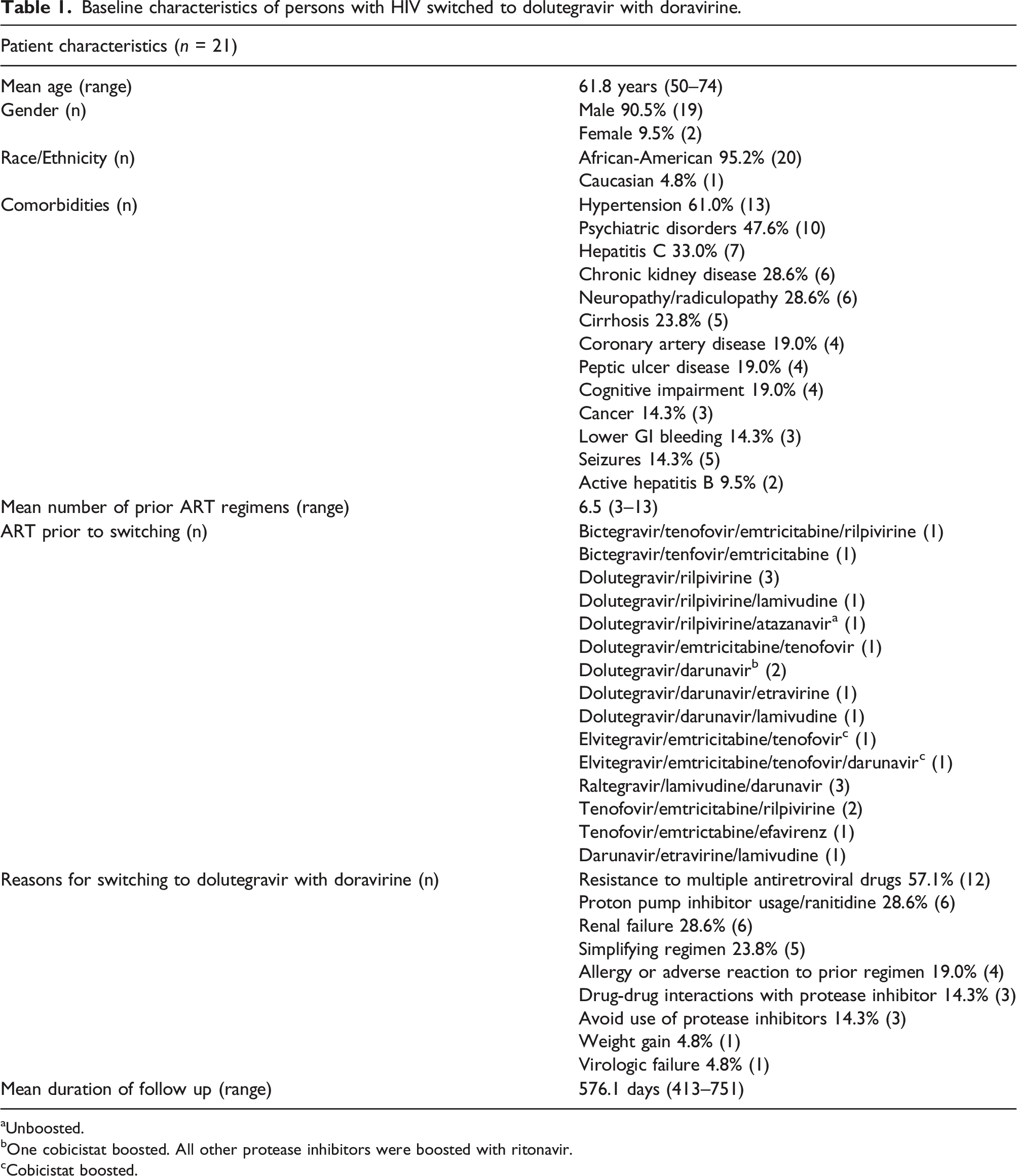
aUnboosted.
bOne cobicistat boosted. All other protease inhibitors were boosted with ritonavir.
cCobicistat boosted.
Virologic suppression and outcomes in persons with HIV receiving dolutegravir with doravirine.
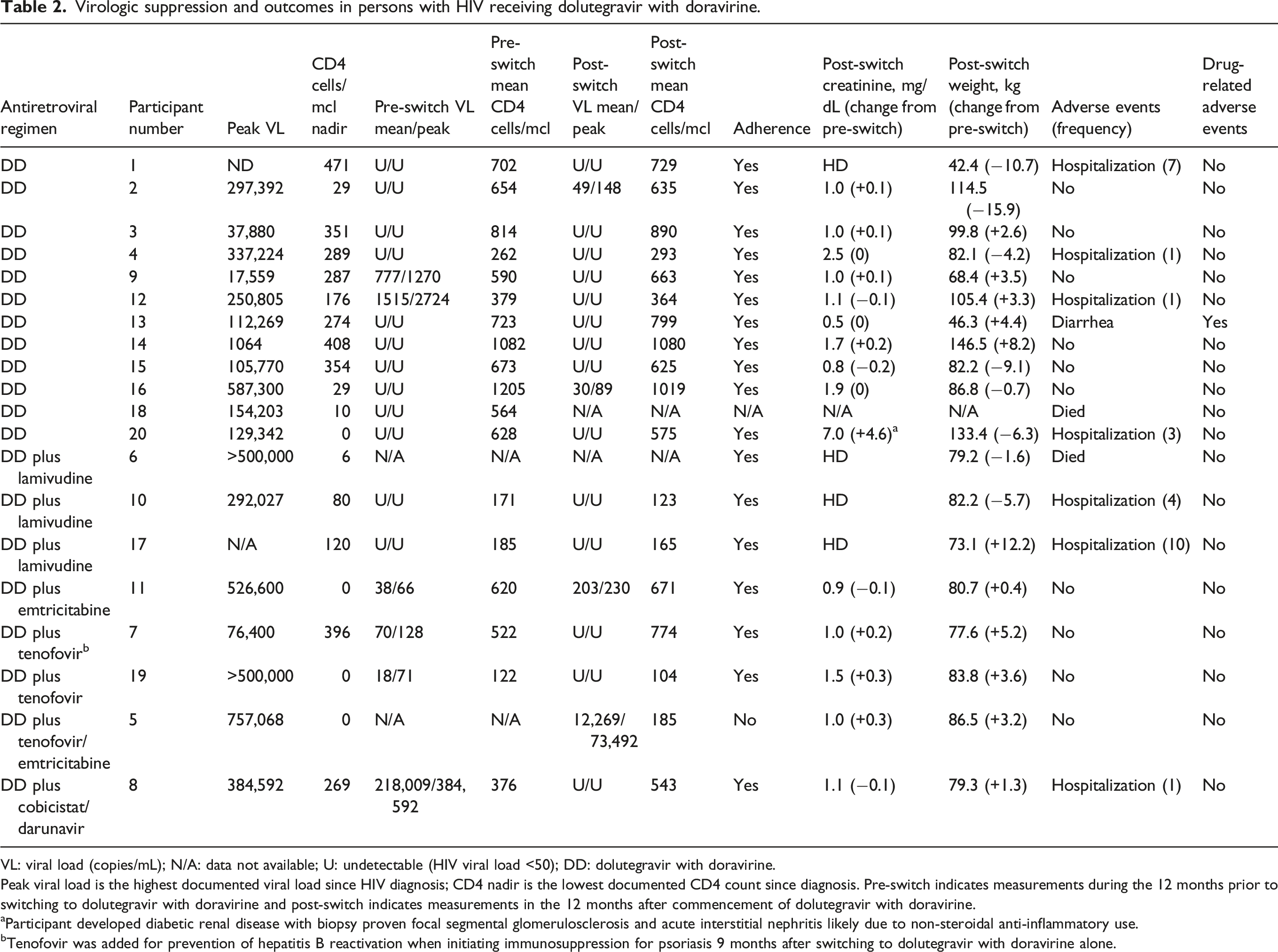
VL: viral load (copies/mL); N/A: data not available; U: undetectable (HIV viral load <50); DD: dolutegravir with doravirine.
Peak viral load is the highest documented viral load since HIV diagnosis; CD4 nadir is the lowest documented CD4 count since diagnosis. Pre-switch indicates measurements during the 12 months prior to switching to dolutegravir with doravirine and post-switch indicates measurements in the 12 months after commencement of dolutegravir with doravirine.
aParticipant developed diabetic renal disease with biopsy proven focal segmental glomerulosclerosis and acute interstitial nephritis likely due to non-steroidal anti-inflammatory use.
bTenofovir was added for prevention of hepatitis B reactivation when initiating immunosuppression for psoriasis 9 months after switching to dolutegravir with doravirine alone.
Two patients died during the follow-up period and had no post-switch CD4 count or viral load data available; one patient switched to dolutegravir with doravirine on admission to ICU in established shock and multiorgan failure and died 4 days later, one further patient died in cardiac arrest due to hyperkalemia, missed dialysis and gastrointestinal bleeding from pre-existing rectal cancer after 5 months of treatment with dolutegravir and doravirine. Seven patients were hospitalized during follow-up for reasons unrelated to their ART regimen including hematemesis from erosive esophagitis, atypical chest pain from gastroesophageal reflux, diarrhea and vomiting, central-line associated bloodstream infection, volume overload due to pre-existing end stage renal disease, bleeding from dialysis line site, arteriovenous graft dysfunction, subcapsular hematoma, seizures, elective spinal stenosis surgery, community acquired pneumonia, traumatic hip fracture with surgical complications, hepatic encephalopathy, Wernicke’s encephalopathy, myocardial infarction, ischemic cardiomyopathy, diabetic nephropathy, and stroke. Participant 13 developed diarrhea as a side effect of his treatment with dolutegravir and doravirine which resolved without discontinuation and did not require hospital treatment. Participant 20 developed worsening of pre-existing renal failure which was unrelated to ART.
Discussion
Our service evaluation highlights a small group of older and highly treatment experienced PWH receiving dolutegravir in combination with doravirine due to severely limited ART choices, defined by a combination of their individual HIV viral genotypic resistance profile, their comorbidities, and consequent drug-drug interactions with co-administered medications. The older age, high frequency of co-morbidities, high number of prior ART regimens (mean 6.5), and frequent ART-unrelated hospitalizations and deaths in this group reflect the high degree of complexity inherent in their care. Guidelines recommend considering NRTI- sparing regimens (such as dolutegravir-rilpivirine) in older PWH, particularly with chronic kidney disease. 8 However, in our service evaluation, rilpivirine was not feasible in many cases due to interactions with proton pump inhibitors or predicted resistance based on HIV genotyping.
The numbers of older PWH in the United States are increasing, with a greater burden of aging-related diseases described in PWH than the general population. 9 We observed that providers switched to dolutegravir with doravirine to simplify the patient’s prior ART regimen in nearly a quarter of cases. Polypharmacy is common in older PWH, and adverse drug events occur more frequently in older PWH than younger PWH. 10 The prior case series of dolutegravir with doravirine in older PWH noted ART simplification as a factor in 69% and polypharmacy in all participants. 7 Dolutegravir and doravirine combinations avoid the drug interaction challenges of cobicistat- or ritonavir-boosted protease inhibitor containing regimens and may mitigate risks from polypharmacy.
Our single-center service evaluation of small numbers of PWH found that dolutegravir and doravirine alone or in combination with other antiretrovirals appeared safe and achieved virologic suppression in most recipients, consistent with the prior case series of PWH receiving dolutegravir plus doravirine. 7 Our experience underscores the importance of close longitudinal follow-up in PWH receiving less studied ART combinations to detect potential adverse effects, especially in older populations with multiple comorbidities. Larger randomized longitudinal research studies such as the planned Efficacy of Doravirine + Dolutegravir Dual Therapy in the Context of Antiretroviral Therapy Switch (DORDOL) study will assess durability of virologic suppression and inform future clinical guidance regarding this ART combination. 11
Footnotes
Acknowledgements
This material is the result of work supported with resources and the use of facilities at the Washington DC VA Medical Center. The authors wish to thank Laura Popielski at the Washington DC VA Medical Center for coordination and liaison with IRB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.