
Abstract
Background
Community pharmacies increasingly serve as access points for HIV pre-exposure prophylaxis (PrEP) in South Africa and understanding how PrEP users in these settings make decisions about condom-use is essential to inform effective combination prevention strategies. This study explored condom-use decision-making among PrEP users accessing pharmacy-delivered services in South Africa.
Methods
This qualitative study formed part of the midline evaluation of the PPrEPP-SA project. In-depth interviews were conducted between March and May 2024. Interviews explored participants’ understanding of PrEP, sexual behaviours, perceptions of HIV/STI risk, and experiences with prevention methods. Audio-recorded interviews were transcribed verbatim and analysed thematically using Braun and Clarke’s inductive approach.
Results
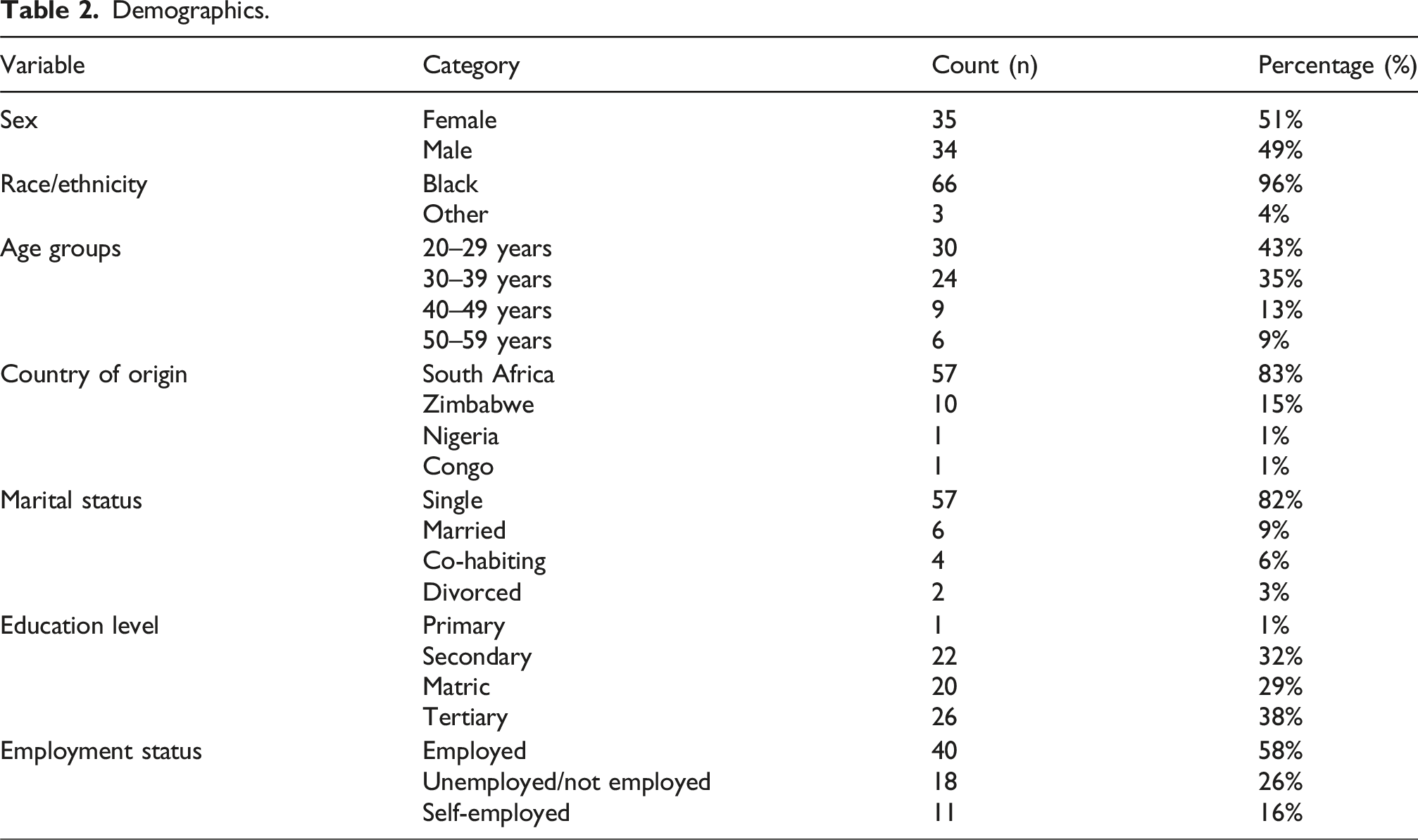
69 PrEP users aged 18–59 years were recruited from 10 community pharmacies across Gauteng and the Western Cape. Participants demonstrated varied and often negotiated condom-use practices while on PrEP. While most understood PrEP as effective for HIV prevention, some held misconceptions regarding its ability to prevent STIs, contributing to reduced condom-use. Decisions to forego condoms were linked to trust in partners, relationship stability, cohabitation, and preferences for condomless physical intimacy. Condom-use was more likely in casual partnerships or when partner HIV status was unknown. Participants also expressed a strong preference for purchased condoms over free public-sector condoms, citing concerns about quality and durability.
Conclusion
Condom-use among pharmacy-based PrEP users is context-dependent, shaped by relationships, risk perceptions, and understandings of PrEP. In South Africa, pharmacy-delivered PrEP programmes provide a critical opportunity to reinforce dual prevention messaging, address misconceptions, and improve access to acceptable, high-quality condoms as part of comprehensive HIV and sexual health prevention.
Keywords
Introduction
South Africa’s HIV epidemic remains a pressing public health challenge, with the country bearing one of the highest prevalence rates globally at approximately 19–20% among adults aged 15–49 years. 1 Since the early 1990s, HIV prevention strategies have evolved considerably. Initial responses focused heavily on condom promotion as a straightforward and accessible way to reduce transmission. 2 Despite widespread condom distribution programmes including free provision by the South African government since 1992, consistent condom use remains uneven, with disparities across populations and geographic areas.3,4 Barriers like limited access in rural regions, cultural myths, misconceptions about condom effectiveness, and entrenched gender inequalities have curtailed condom uptake.5,6
More recently biomedical prevention tools, particularly pre-exposure prophylaxis (PrEP), have gained prominence. Since its endorsement by the World Health Organization (WHO) in 2016, PrEP has demonstrated high efficacy in preventing HIV when taken consistently. 7 South Africa initially introduced PrEP for key populations, including sex workers in 2016, and later expanded access to high-risk groups, such as adolescent girls and young women (AGYW).8,9 Despite these efforts, PrEP uptake has been gradual, and adherence remains crucial to its effectiveness. 8
Given the potential for lapses in condom use or PrEP adherence, WHO recommends their combined use for populations at elevated risk of HIV acquisition. 7 While PrEP reduces HIV risk, it does not protect against other sexually transmitted infections (STIs), for which condoms remain essential. 10 Concerns about risk compensation, where perceived protection from PrEP leads to reduced condom use, have been documented.11,12
Community pharmacies (approximately 3600) have emerged as important access points for PrEP in South Africa, expanding beyond traditional clinics and hospitals. 13 Chain pharmacies like Clicks and Dis-Chem, have an extensive national footprint and provide broad coverage of retail health services, particularly in urban and peri-urban areas. In addition, South Africa has a large network of independent pharmacies (locally owned pharmacies not affiliated with national chains) that also provide both PrEP and condoms, improving access to HIV prevention services.14,15 Even globally, there is an increasing number of pharmacies that are providing PrEP in addition to condoms, thereby increasing access to both these HIV prevention tools. 16 However, pharmacy-based models may differ from public-sector clinics in terms of counselling depth, privacy, and user engagement, potentially shaping how individuals understand and use prevention tools. Despite broader availability, limited knowledge about PrEP among pharmacy clients continues to constrain uptake.17,18
While evidence documents PrEP uptake in pharmacy-based models, less is known about how users understand, negotiate, and practice condom use alongside PrEP.13,16 In particular, there is limited evidence on how perceptions of HIV protection, STI risk, relationship dynamics and PrEP’s scope influence dual methods in this context. This study aimed to explore condom use among pharmacy-based PrEP users in South Africa, describing factors influencing dual-method use or non-use.
Methods
Study design
This was a qualitative study conducted as part of the midline evaluation of the Utilizing
Setting and sampling
Types of pharmacies.
Participants were purposively sampled from clients enrolled in the PPrEPP-SA implementation project. Pharmacy based research staff informed eligible PrEP users about the qualitative study during routine visits. Interviews were set up for interested individuals according to their availability. Sampling aimed to include a balanced group of participants across gender, age groups, and PrEP engagement status (active users, missed appointments, and discontinuers – as determined by the participant adherence to their visit schedule) where possible.
Data collection
Between March and May 2024, in-depth interviews (IDIs) were conducted in person at pharmacies, within quiet and secure settings. Trained interviewers used a pilot-tested semi-structured guide to explore participants’ knowledge of PrEP, sexual behaviour, prevention practices, and recommendations for improving PrEP delivery. Interviewers were matched with the participant for language but not gender. Interviews were conducted in private pharmacy consulting rooms (with only the interviewer and participant were present), lasted 30–60 min, were conducted in English or the participant’s preferred vernacular language, audio-recorded, transcribed verbatim, and translated into English by experienced bilingual protocol trained transcribers. Interviews continued until thematic saturation. Saturation was assessed by the research team (both interviewers and coders) reviewing transcripts iteratively during data collection to assess whether additional interviews yielded novel insights.
Participant demographics, routinely collected by the PPrEPP-SA programme, were extracted from the study database to describe socio-demographic characteristics.
Data management and analysis
Transcripts were quality checked against audio recordings to ensure accuracy and preservation of meaning. An inductive thematic approach, following Braun and Clarke’s six-step process guided analysis. 19 The process comprised getting familiar with collected data, generating codes through transcript review, identifying themes, creating, defining and labelling final themes, and completing an analytical report writing.
Two coders, authors MFM (social scientist) and KEO (mixed-methods public health researcher), both with over 5 years of qualitative analysis experience in HIV implementation studies, conducted initial coding. The coding structure was finalized with input from the third coder, STL-E (mixed-methods public health researcher). Although no formal intercoder reliability metric was calculated, reliability was ensured through independent coding of a 20% transcript subset, followed by iterative consensus discussions to resolve discrepancies and refine the codebook.
The data were analysed using MAXQDA version 22 software.
The interviewers had prior experience in qualitative HIV research and were not involved in participants’ clinical care, reducing the risk of social desirability bias. Reflexive discussions were held during analysis to consider how researchers’ assumptions may have shaped coding decisions.
Ethical considerations
Ethical approval for this study was granted by the University of the Witwatersrand Human Research Ethics Committee (reference number 230107). All participants provided informed consent for both their interview participation and audio recording. Participants were reimbursed ZAR405 (approximately $25), in accordance with the ethics committee guidelines on reimbursement amounts.
Audio recordings, transcripts, and translations were stored securely on password-protected institutional servers accessible only to the study team, with all identifiable information removed and data encrypted during transfer.
Results
Profile of participants
Demographics.
Themes
Although condom use was the primary outcome of interest, participants’ decisions were shaped by broader contexts, including HIV testing practices, understandings of PrEP, and perceptions of sexual risk. These contextual factors influenced how individuals assessed vulnerability to HIV and other STIs and how they negotiated condom use while on PrEP. Four interrelated themes emerged 1 : HIV testing and partner status awareness, 2 PrEP understanding and condom substitution, 3 sexual behaviour and perceived HIV/STI risk, and 4 condom use patterns. Together, these illustrate the behavioural and cognitive pathways through which condom use is adopted, modified, or discontinued among pharmacy-based PrEP users.
HIV testing and partner HIV status awareness
HIV testing practices and awareness of partners’ HIV status played a central role in shaping perceived risk and condom decisions. Many participants described accessible community-based testing, including clinic services and self-test initiatives. Some reported spontaneous testing prompted by outreach workers in temporary tents, while others tested with partners at clinics or using self-test kits. Well, we went together [for testing HIV] the other day…. And you know those people, they used to put tent and then they said, oh no, guys, come. And then we went there, we tested together. (PP-08-0016, Male, 27 years, Johannesburg) “Yes, I do know her status [HIV] because where she works after some time, I don’t know I think it’s three or four months, they use Netcare. They call Netcare to come to the firm and to take everyone’s blood sample. So, she usually comes home with the proof ” (PP-08-0080, Male, 39 years, Johannesburg)
Most had tested prior to enrolment on the project, with many indicating that they tested at least annually. A portion of participants across both genders who chose not to test cited fear of a positive result as their reason. This was especially true for those who experienced condom breakages during sex. Some of the participants had knowledge of their partner’s HIV status.
Several participants expressed uncertainty about when it was appropriate to ask a partner about HIV status, particularly in casual or new relationships, fearing that such questions might signal mistrust. “It's difficult to ask someone about it [HIV status] because in most cases is [it’s] all about one night stand. So, it's difficult to know where that person stands, so it's difficult to know if the person wants to be with you or what... I don't know, maybe today you meet someone, and then, tomorrow, you ask her about her status. It's difficult. I don’t know how long you should be in a relationship, you should ask about her status.” (PP-10-0027, Male, 32 years, Pretoria)
These testing practices and assumptions about partner HIV status often informed participants’ decisions to forego condom use while relying on PrEP.
PrEP understanding and condom substitution
Participants’ understanding and attitudes toward PrEP strongly influenced their condom use behaviours. While most recognised PrEP as an effective HIV prevention tool, misconceptions about its protective scope were evident. Although PrEP prevents HIV acquisition, it does not treat or prevent other STIs, yet several participants interpreted PrEP as sufficient protection and reported reduced condom use.
One participant described observing STIs in young students and expressed a belief that PrEP might help manage mild infections, although they acknowledged uncertainty: “I've seen where young students, because Melville is based with students and you can see when they walk in, the boys walk in and they're walking in with their discomfort and you can see it's an infection in the genitalia area and only to find out that when you mix a certain infection with another one, you're creating a new infection, right? … I'm not saying PrEP doesn't fight, it fights every infection, but I do think like if you have a mild yeast infection, it does kind of get rid of it, or maybe I'm psychologically imagining it.” (PP-07-0132, Female, 31 years, Johannesburg)
Another participant highlighted stigma and misconceptions around PrEP use, noting that PrEP use is sometimes interpreted as evidence of an HIV positive status:: “And I think it's also this thing in people's head that if you're taking PrEP, you're HIV positive”… But I think definitely clearing up the confusion that just because you're taking PrEP means you're HIV positive… And one of the conversations I was having with another guy about PrEP. And he was saying that the only reason why anyone would be taking PrEP is because you're trying to cover up the fact that you actually are HIV positive and you don't want people to know.”. (PP-02-0001, Female, 34 years, Cape Town)
This suggests that PrEP related stigma may indirectly influence condom use decisions by shaping partner communication and perceptions of HIV risk.
PrEP has been seen as the most effective way of preventing HIV. Most of the participants relied on PrEP, indicating that they no longer use condoms because they felt sufficiently protected while taking PrEP. Additionally, some participants mentioned that PrEP offered them protection because they preferred not to use condoms. “To be honest, I don’t like using condoms so, you see, PrEP is the biggest protection for me. It is my biggest weapon because I’m not that kind of person who likes to take condoms. So, I think PrEP is the best way for me to protect myself.” (PP-08-0080, Male, 39 years, Johannesburg)
These understandings and misconceptions about PrEP shaped condom use decisions, with several participants viewing PrEP as a sufficient standalone protection against HIV, thereby reducing the perceived need for consistent condom use.
Sexual behaviour and perceived HIV/STI risk
Perceptions of sexual behaviour and HIV/STI risk informed how participants evaluated the necessity of condoms while using PrEP, particularly in the context of partner type, relationship stability, and self-assessed vulnerability. Unexpectedly, participants who perceived themselves to be at high risk often engaged in sexual activity without using condoms. Participants considered themselves at low risk when they were sexually active with only one partner. Several individuals who consistently used condoms or had a single sexual partner expressed confidence that they were not at risk of HIV infection.
For example, one participant candidly stated, “So, I like, I’ve been very reckless [referring to sexual activity and health], you know …. I mean like not using protection [condoms]. Yeah, that’s what I mean…” (PP-02-0070, Male, 22 years, Cape Town).
Another participant described their behaviour as stable, saying, “My sexual behaviour is, I only have one partner. I don’t have different partners whom I get into sexual intercourse with. So, I would say, in a simple way, my sexual behaviour is just on a normal state. ” (PP-11-0066, Female, 27 years, Pretoria).
Participants were generally aware of the risks associated with unprotected sex or not using condoms, although some practised abstinence to mitigate those risks. One admitted, “Because the one that I went with, I didn’t use protection, so I might be at risk.” (PP-08-0017, Male, 32, Johannesburg), while another affirmed, “Ja [Yes], I abstained and controlled myself.” (PP-08-0009, Male, 59 years, Johannesburg).
Notably, participants demonstrated limited explicit understanding of PrEP’s inability to prevent other sexually transmitted infections (STIs). While most participants described PrEP as effective for HIV prevention, few spontaneously referred to STI risk when discussing condom use decisions. This absence suggests that STI prevention was not a primary consideration when relying on PrEP, and highlights a gap in risk perception beyond HIV. These intersecting factors—HIV testing practices, understandings of PrEP, and perceptions of sexual risk—culminated in varied and negotiated condom use patterns among participants.
Participants’ sexual practices and self-assessed levels of HIV and STI risk directly informed condom use behaviours, with those perceiving themselves to be in stable or low-risk relationships more likely to forego condoms while relying on PrEP.
Condom use patterns
Condom use emerged as a negotiated practice rather than a consistent behaviour. While some participants with HIV-positive partners initially used condoms consistently, trust, intimacy, personal protection and awareness of a partner’s HIV status shaped how participants navigated decisions about the use of condoms, revealing the social and emotional dimensions underlying what might appear as simple behavioural choices. “I was using PrEP, so I was not using condoms, and by that time I was staying with my boyfriend… if you are staying together, it's very hard to use condoms… I don't like condoms…I don’t feel like you are having sex.”(PP-06-11, Female, 32 years, Cape Town) “I only use condoms. The thing is, I refuse. He sometimes says that the condom makes him bloated. And I tell him that if it gets you bloated, then we can forget everything. Or I just play around with him, and he ends up releasing, but not on me.” (PP-07-121, Female, 44 years, Johannesburg) “I am not a woman, my, uh knowledge is that even if I'm using PrEP, but I cannot say it’s 100% safe, but I must take care of myself. The only prevention that I can do is by using condoms. Condoms prevent pregnancy. That’s contraception for men. Pregnancy, STIs and also some of the illnesses.” (PP-08-0026, Male, 48 years, Johannesburg)
Participants expressed a clear preference for condoms purchased from filling stations and pharmacies over those provided at clinics and hospitals, with distinctions drawn solely based on the source of acquisition rather than brands. They perceived the free condoms from healthcare facilities as inferior in quality, often reporting that these condoms were prone to breaking shortly after use. For instance, one participant shared,
“I don’t like those free ones because it’s getting broken. Okay. Those ones that they are giving us by the hospital, we use it just in a few minutes, It’s broken. That’s why I don’t use them. I just buy the one that they do sell. I used to buy especially at the garages. Like Total Garage, Excel Garage. … That’s where you find the good quality condoms.” (PP-05-0006, Male, 29 years, Cape Town).
Overall, condom use among PrEP users emerged as a negotiated and context-dependent practice, shaped by trust in partners, intimacy preferences, perceptions of condom quality, and reliance on PrEP for HIV protection.
Together, these findings demonstrate that condom use among pharmacy-based PrEP users is not a standalone behaviour but is embedded within broader understandings of PrEP, sexual risk, partner dynamics, and access to prevention commodities.
Discussion
This qualitative study examined condom use among PrEP users accessing pharmacy-delivered services in South Africa. Findings show that condom use is not an isolated behaviour but is shaped by HIV testing practices, PrEP understandings, perceived sexual risk, and relationship dynamics. These interconnected factors influence decisions to maintain, reduce, or discontinue condom use while on PrEP.
PrEP understanding and misconceptions
This study found that while participants widely recognised PrEP as an effective HIV prevention strategy, misconceptions regarding its scope were common. In particular, participants rarely demonstrated awareness that PrEP does not prevent other STIs. This gap in understanding has been documented in previous studies12,20–22 and may contribute to reduced condom use among PrEP users. The absence of STI-related risk considerations in participant narratives suggests that HIV prevention may be prioritised over broader sexual health, highlighting the need for clearer dual-protection messaging.
Relationship dynamics and condom negotiation
Condom use was strongly shaped by relationship context, trust, and intimacy. Participants in stable or perceived low-risk relationships were more likely to discontinue condom use, often relying on PrEP for HIV protection. In contrast, condom use was more common in casual partnerships or when partner HIV status was unknown. These findings align with existing literature showing that perceptions of trust, fidelity, and relationship type influence condom use decisions among PrEP users.23,24
Gender differences were also evident. Female participants more frequently emphasised condom use for pregnancy and STI prevention, while male participants were more likely to frame PrEP as a substitute for condoms. These dynamics highlight the importance of considering gendered power and negotiation in sexual health interventions.
Condom substitution, quality, and access
Participants frequently described PrEP as a replacement for condoms, particularly where condoms were perceived to reduce physical pleasure. At the same time, strong preferences emerged for purchased condoms over those distributed through public-sector clinics, which were often viewed as inferior in quality.5,25 While pharmacies were perceived as reliable sources of higher-quality condoms, reliance on purchased products raises concerns about equitable access for individuals with financial constraints.
Implications for pharmacy-based PrEP delivery
The pharmacy-based PrEP delivery model provides an important opportunity to strengthen integrated HIV prevention strategies. While pharmacies offer accessible and less stigmatising environments for PrEP provision, findings suggest that sexual health counselling—particularly around STI prevention and condom use—may require strengthening within this model.13,16 Clear and consistent messaging that emphasises condoms as complementary, rather than substitutive, to PrEP is essential.7,23
Additionally, stigma surrounding PrEP use emerged as a barrier to open discussion and may influence prevention behaviours. Addressing misconceptions about PrEP and normalising its use as a preventive tool could support more informed decision-making.
Overall, this study contributes to the growing body of evidence highlighting the complexity of prevention behaviours in the era of biomedical HIV prevention. Condom use among pharmacy-based PrEP users is shaped not only by perceptions of HIV protection but also by relationship dynamics, STI risk awareness, and access to prevention commodities. Strengthening combination prevention strategies (preferably through policy) that address these social and structural factors will be critical to maximising the public health impact of PrEP.
Limitations
This study recruited participants from selected urban pharmacies in Gauteng and the Western Cape, which may limit generalisability to rural areas or other provinces. Participants were already accessing pharmacy-based PrEP services, and findings may not reflect experiences of individuals using public-sector clinics or those not engaged in PrEP care. Sexual behaviours and prevention practices were self-reported and may be influenced by social desirability bias. Additionally, the urban sampling frame and pharmacy-based PrEP users may be more health-literate or economically advantaged than public-sector clients, potentially limiting transferability. A final limitation is the potential for differing power dynamics in pharmacy settings compared to clinic environments.
Conclusion
Condom use among PrEP users is complex, shaped by personal preferences, relationships, and structural factors. Most participants reported reduced condom use while taking PrEP. Enhanced education on PrEP, dual prevention, and access to high-quality condoms is critical. Integrating clear messaging on dual protection within pharmacy-based PrEP delivery is critical to ensuring that gains in HIV prevention are not accompanied by increases in other STIs.
Footnotes
Ethical considerations
Ethical approval for this study was granted by the University of the Witwatersrand Human Research Ethics Committee (reference number 230107).
Consent to participate
All participants provided written or electronic (internet connectivity dependent) informed consent to participate in the interviews and for the audio recording of their interview.
Consent for publication
All participants provided written or electronic (internet connectivity dependent) informed consent for de-identified analysis and publication of their interview data.
Author contributions
MGM and KEO conceptualised the study and methods. MGM, KEO, NN, TM, LZ, AN and STL-E organised and conducted the data collection. MGM, KEO, LS, and STL-E analysed and interpreted the data. MGM wrote the draft article; KEO, LS, AT and STL-E performed a critical review and provided revisions. All authors have read and approved the final article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Bill and Melinda Gates Foundation (grant number: INV-037064).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the senior author on request.