
Abstract
Background
No vaccine is currently available for syphilis. Research efforts to inform vaccine development are underway. In parallel, understanding factors that would influence willingness to receive a future vaccine can provide useful information for vaccine design and future implementation. This study explored attributes of interest in a hypothetical syphilis vaccine using focus group discussions in Lima, Peru.
Methods
In early 2025, we conducted ten virtual focus group discussions, among five population groups in Lima, Peru: health professionals, sexual/gender minorities, general population, cisgender female sex workers, and parents of minors. Semi-structured guides explored barriers and facilitators to preventive care, attitudes toward vaccines, syphilis knowledge, and desired attributes of a potential syphilis vaccine. Audio recordings were analyzed thematically.
Results
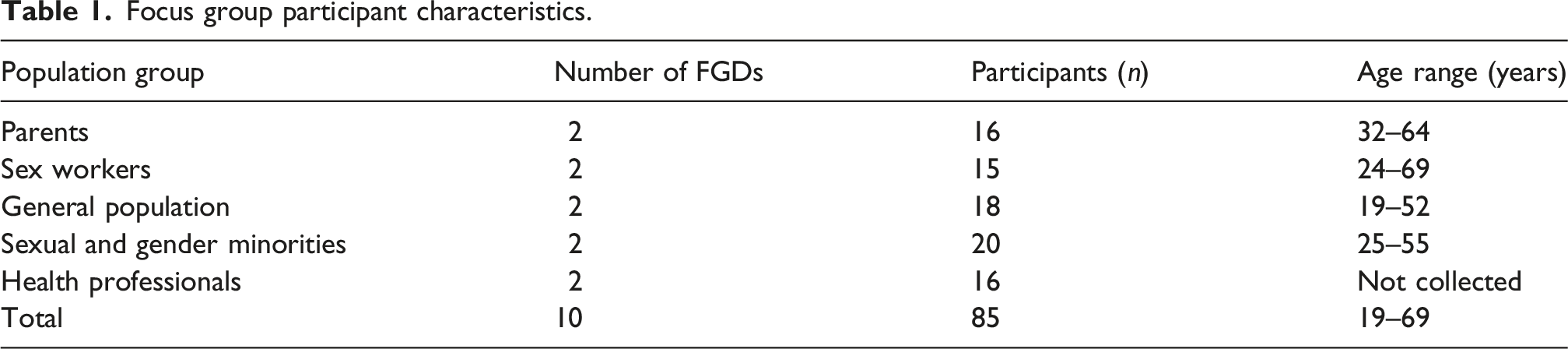
Eighty-five participants took part in the discussions. Despite limited syphilis knowledge among many participants, there was interest in a hypothetical vaccine. Acceptability was shaped by three factors including, vaccine attributes, structural conditions and the healthcare provider-user relationship. In vaccine attributes, participants desired high effectiveness, safety, and a single-dose schedule, while expressing concerns about vaccine-induced persistent seropositivity related to stigma about STI prevention. Structural conditions: free vaccination, endorsement from respected health institutions, information environment and health education were viewed as essential for uptake. Third, the healthcare provider–user relationship emerged as a central mediator influencing how individuals interpreted vaccine information and navigated structural barriers.
Conclusions
Acceptability of a future syphilis vaccine depends not only on its attributes, but also on structural enablers and the quality of provider–user interactions. Strengthening provider communication, addressing structural barriers, and ensuring transparent information dissemination will be essential for equitable implementation.
Introduction
Syphilis, a sexually transmitted infection (STI) caused by Treponema pallidum, causes substantial morbidity and mortality worldwide, with over 6 million new cases reported globally each year and incidence increasing across most regions.1–9 Gaps persist in understanding its pathogenesis and immune response,10,11 and clinical and serological diagnosis remains challenging.12–14 Currently, doxycycline post-exposure prophylaxis (DoxyPEP) has shown effectiveness in reducing bacterial STIs, including syphilis, 15 but remains limited in implementation. 16 Research has focused on understanding of syphilis pathogenesis, with recent progress in Treponema pallidum morphology, including outer membrane proteins as potential syphilis vaccine candidates.17,18 However, due to the biological complexity of Treponema pallidum, an ideal or “perfect” syphilis vaccine is unlikely in the near term. There is no current vaccine and research remain in vitro. In parallel, assessing public and provider responses to potential vaccines and identifying drivers of willingness to receive new vaccines are essential, since vaccine impact depends on uptake. 19 Additionally, as a perfect vaccine (sterilizing immunity) is unlikely, understanding views on vaccine attributes can help to formulate education for a future available, but imperfect vaccine.
In syphilis vaccine research, a review by Valleroy et al. 20 found high acceptability of STI vaccines, including syphilis, although evidence remains limited and factors influencing acceptability are not yet well characterized. Day et al. 21 implemented a qualitative exploratory study among infectious disease and STI clinic patients in North Carolina to assess participation in a syphilis vaccine trial. Most participants (63%) expressed interest in trial participation, although for some (33%) this interest was conditional; perceived physical risks, medical mistrust, and time commitment were key barriers, highlighting the importance of community engagement. This study was focused on vaccine trial participation rather than vaccine acceptability.
Important gaps remain in understanding the intersecting factors influencing willingness to vaccinate, particularly in resource-limited settings and for stigmatized conditions such as STIs. Studies on HPV vaccine uptake—a proxy for STI-related vaccines—identify common barriers including safety concerns, low perceived infection risk, low perceived vaccine benefit, irregular preventive care, and cost.22,23 These barriers may be amplified for new vaccines and/or vaccines that do not provide sterilizing immunity.
Mathematical models indicate that a hypothetical syphilis vaccine could reduce syphilis incidence, 24 however, models and vaccine research suggest that an imperfect vaccine would likely confer only partial protection, reducing symptoms and transmission but not preventing infection entirely, and could also lead to risk compensation behaviors that may offset some of its benefits.25,26 To study this more closely a discrete choice experiment (DCE) will be conducted, to do so we need to understand the vaccine attributes and other health system factors that would be important to include. This study is exploratory formative research to characterize these attributes and factors based on community perspectives, especially among populations disproportionately affected by syphilis. To address this need, we conducted focus groups to explore perceptions of a hypothetical syphilis vaccine, aiming to identify key themes related to acceptability, barriers to uptake, and strategies for equitable implementation.
Methods
Between February and March 2025, we conducted 10 focus group discussions (FGDs) via Zoom to better understand syphilis knowledge, hypothetical syphilis vaccine acceptability, important hypothetical vaccine attributes, and implementation characteristics. This study was done as formative, exploratory research toward the development of a discrete choice experiment on a hypothetical syphilis vaccine to help provide information to vaccine developers. Two FGDs were conducted with each of these five groups: (1) health professionals; (2) sexual/gender minorities; (3) general population; (4) cisgender female sex workers; and (5) parents with children under 18 years old. These groups were selected based as they include potential vaccine recipients, some of whom are at increased vulnerability to syphilis. Parents of children under 18 were included as a vaccine might be recommended for children. Additionally, healthcare professionals were included to gage their views of vaccination. The 10-item CASP checklist for qualitative studies is available in the supplementary materials.
Study population and setting
Potential participants were identified and recruited by study staff working at public STI clinics and a community-based healthcare organization in Lima, Peru. Staff invited potentially eligible individuals to participate, those who were interested and met inclusion criteria were asked to provide their contact information to organize and schedule the virtual focus groups. Purposive sampling was used to ensure include individuals from across the groups of interest. Trained study staff verified eligibility criteria, including being at least 18 years old, willingness to participate, ability to provide informed consent, and identifying as being in the population of interest.
Data collection and analysis
Sessions were facilitated by two native Spanish-speaking researchers trained in social psychology and experienced in qualitative research methods. Sessions were audio-recorded with participants’ permission; cameras remained off, and a code was used for each participant rather than their name to protect confidentiality. Codes were assigned upon entry to the Zoom session by study staff to avoid displaying participants’ names. Semi-structured discussion guides explored barriers and facilitators to accessing preventive health services, vaccine attitudes, syphilis knowledge, and hypothetical syphilis vaccine attribute preferences.
The analysis process was iterative and based on thematic analysis 27 using both deductive and inductive approaches. Thematic analysis provides a flexible, rich and detailed approach to examine the perspectives of research participants, allowing us to emphasize similarities and/or differences in the data and generating themes and thematic interrelations. 28 Audio recordings from the focus groups were transcribed using Zoom’s automated Spanish transcription and analyzed using Dedoose, a secure cloud-based platform for qualitative data analysis. 29 The researchers first independently coded a subset of transcripts and developed a preliminary codebook based on the focus group guide while also incorporating themes emerging from the discussions. They then met regularly to compare coding, refine the codebook, and resolve discrepancies through consensus. The final codebook was subsequently applied to all transcripts to identify patterns and thematic relationships across the focus group data. Selected quotes were translated into English for inclusion in the manuscript.
Ethical review
The study was approved by the Institutional Review Board of UPCH (study code 214,726) and the Ethics Committee of the USC (study code UP-24-01,080). Oral informed consent was obtained before any study procedures. The use of oral informed consent was approved by both ethics committees. Pseudonyms are used in quoted excerpts to protect participant confidentiality.
Results
Focus group participant characteristics.
As shown in Figure 1, results are presented across the three thematic categories that emerged as shaping vaccine acceptability. First, vaccine attributes: participants desired high effectiveness, safety, and a single-dose schedule, while expressing concerns about vaccine-induced persistent seropositivity. Second, structural conditions: free vaccination, health institutions endorsement, information environment, and health education were viewed as essential for uptake. Third, the healthcare provider–user relationship emerged as a central mediator influencing how participants interpreted vaccine information and navigated structural barriers. Preferences regarding a hypothetical syphilis vaccine.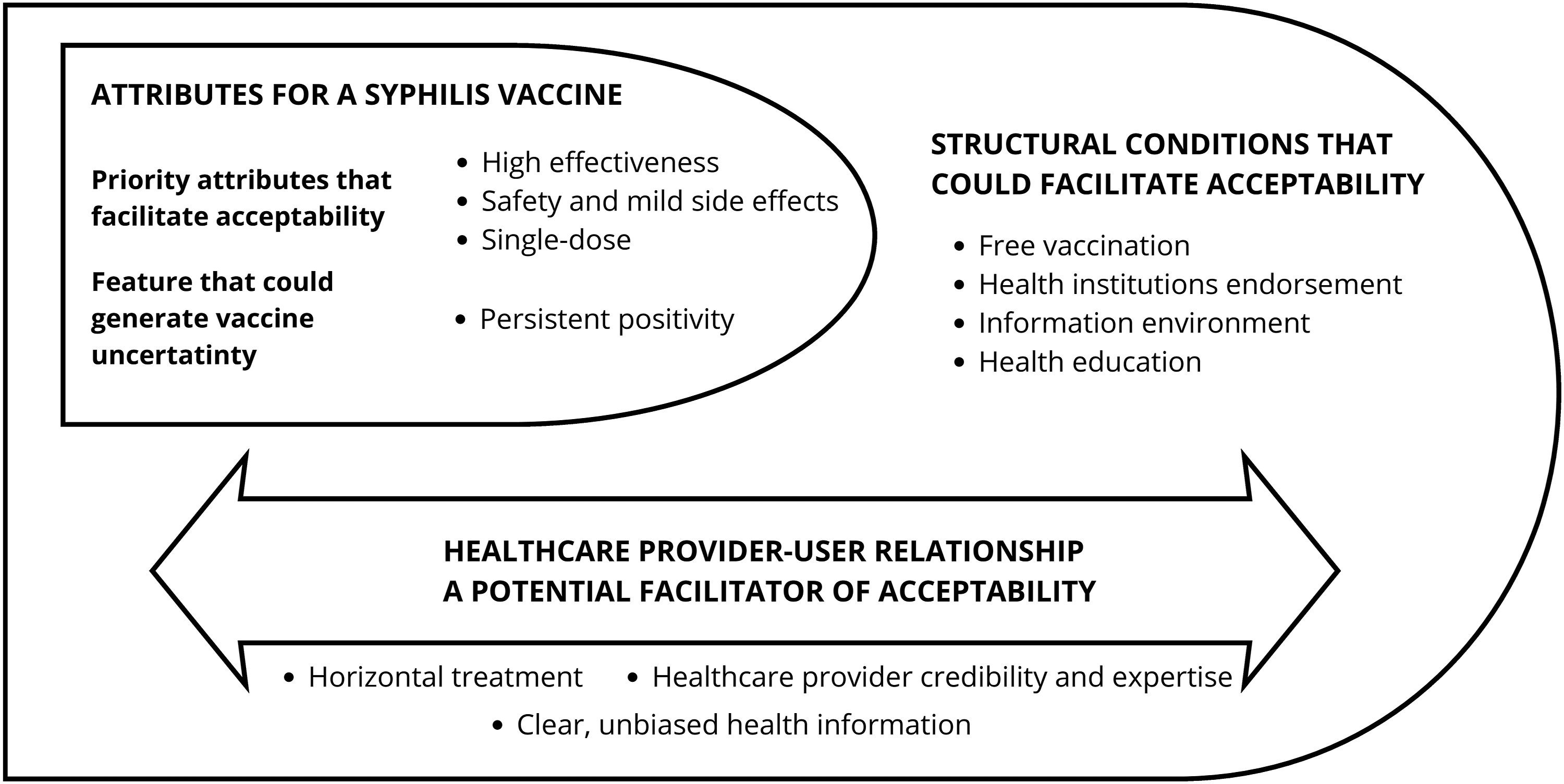
Thematic category 1: Syphilis vaccine attributes
Priority attributes that facilitate acceptability
High effectiveness
Effectiveness was the most frequently valued attribute across groups. Participants expected the vaccine to fully prevent syphilis transmission, valuing effectiveness for personal protection and preventing transmission to sexual partners and the broader community. Some suggested that a highly effective vaccine should be mandatory, not because they supported top-down mandates, but because they viewed vaccination as an act of collective well-being: getting vaccinated oneself was seen as a way to protect the community, not just to avoid individual infection. “What we all expect from vaccines is that they do their job, that they protect us from the disease we might get.” (Gloria* - Parents) *Quotes are identified with pseudonyms
Safety and side effects
Vaccine safety and assurance against serious adverse effects emerged as essential, including concerns about vaccinating children. Participants expressed concern regarding unknown risks and the possibility of harm outweighing benefits. They expect a vaccine to cause no severe complications, while acknowledging that vaccines typically produce mild side effects. Safety concerns would not inherently prevent acceptance, but require strong reassurances. Detailed, transparent information from trusted sources is the primary means to mitigate safety-related fears. “Surely if a vaccine comes out, there will be plenty of information about what it’s like, what effects it has. So even if there are side effects, I think yes, I would get vaccinated, because I think that’s part of what a vaccine is. It’s not like you’re taking a vitamin; these are antibodies that in some people may cause a reaction and in others may not.” (Julio - Sexual minority)
Single-dose
Participants preferred a single-dose schedule over multi-dose regimens. This preference was informed by an understanding based on their own experiences or those of close acquaintances with vaccines such as COVID-19 or HPV, that fewer doses facilitate adherence. Participants had observed or experienced dropout from multi-dose schedules due to access barriers, forgetfulness, or logistical difficulties. However, some participants also expressed tension between preferring a single-dose regimen and believing that multiple doses or booster vaccination could provide greater protection. “Maybe it would be an annual one, because there are always variations. Like all viruses or diseases, they mutate.” (Gina - Sexual minority)
Vaccine attribute that generates uncertainty
Persistent positivity
Participants expressed strong concerns that serologic tests could remain persistently positive after vaccination, causing confusion, emotional discomfort, and fear of stigma or discrimination. Many worried that employers, healthcare providers, or society might misinterpret results as active infection, leading to job loss, social judgment, or missed diagnoses. For some, the distress of testing positive, even if it was vaccine induced, was enough to reject vaccination. “It would be like a mark there, like being flagged, they would be flagged. Of course, it would have an impact.” (Jerson - Parents) “I think that some people still have this mindset that a person who gets those vaccines are promiscuous. So, someone who takes that kind of precaution must have a very active sex life. So… the issue of sexually transmitted infections is still taboo.” (Gonzalo – General population)
These concerns were particularly prominent because syphilis, as a sexually transmitted infection, carries a unique moral weight that other vaccine-preventable diseases (such as influenza or tetanus) do not. Addressing this barrier will require not only scientific communication about the vaccine, but also broader efforts to reduce STI-related stigma.
Thematic category 2: Structural conditions facilitating acceptability
Free vaccination
The cost of a potential syphilis vaccine constitutes a key concern, with participants indicating that free access or affordable price is a determining factor among individuals with limited financial resources. Public vaccination programs offering free vaccines have shaped expectations that vaccine provision is a government responsibility and a reflection of commitment to public health. Participants emphasized that the vaccine should be universally accessible, regardless of individuals’ ability to pay. “[…] if the vaccine were free, it would be easier for more people to get vaccinated. And well, if there were also some costs, if it were reasonable, it could also be considered.” (Luis - General population)
Health institutions endorsement
Institutional and scientific endorsement were necessary for vaccine acceptability to build trust amid the concerns that may arise around a new vaccine. Participants explicitly stated that they would only get vaccinated if the vaccine were approved and its efficacy demonstrated. This validation must come from official and trusted sources, such as the Peruvian Ministry of Health and the World Health Organization. Approval from these entities was perceived as a guarantee of safety and efficacy. The vaccine manufacturer also influenced decision-making, with well-known producers carrying greater credibility. “What would give me more confidence is if the Ministry of Health approves it” (Cata – Sex Workers) “It needs to be endorsed by a good laboratory and the WHO… so that they distribute the vaccines worldwide” (Sandy - Sex workers)
Participants stressed that endorsement must go beyond formal approval and be accompanied by clear, accessible, and verifiable information, including efficacy, short- and long-term adverse effects, supported by publicly available results from large studies.
Information environment
According to participants, misinformation represented a significant barrier to acceptability, often mentioned as a concern even before cost or vaccine efficacy. Participants described encountering deceptive online content from sources they considered untrustworthy, including unverified social media accounts and forwarded messages on WhatsApp. This content, they reported, generated distrust and confusion, directly shaping their views on vaccination. One participant explained how the abundance of information, rather than clarifying, created fear: “The problem is that now we are very advanced in technology and everything we see on social media scares us. Before, why did people get vaccinated normally? Because there was no television, no nothing, and people got vaccinated because they thought first about their health” (Anto - Sexual minority)
Limited knowledge about syphilis and persistent taboos surrounding STIs, particularly moralizing views linking prevention to promiscuity, were described by participants as factors that increased their susceptibility to misinformation. These negative perceptions hinder open discussion and allowed misinformation to circulate unchallenged. “More than anything, what we need is information, because I think that this disease has been somewhat neglected, thinking that this disease only affects so-called promiscuous people… but no, it can happen to anyone” (Daniel –Parents)
Regarding the type of information needed, participants indicated that vaccine acceptance depends on clear, reliable, and accessible information backed by recognized institutions and disseminated through approachable formats, including social media platforms like TikTok and Instagram, to reach diverse audiences, particularly youth and key populations. “[…] I would like to see testimonials from people who have already gotten it, maybe now with social media, the whole thing about YouTubers, influencers, right? They have a lot of influence.” (Katy - Parents)
Trust in effectiveness was closely tied to transparency. Participants expressed interest in knowing whether the vaccine had been tested in a large population and monitored over a considerable period of time, reflecting an intuitive understanding of scientific methodology and the importance of long-term data for reliability “How long have you been testing the vaccine before it came out on the market? How long have you been researching, from the beginning to the end? … I would want to know if it has been tested in a large population and monitored over a considerable period of time” (Fernando – General population)
Health education
Health education emerged as key to facilitate acceptability of a syphilis vaccine through strategies that counter myths and promote STI prevention. Limited knowledge about syphilis appeared as a major barrier to sexual health engagement. Persistent moralizing beliefs linking syphilis to promiscuity, infidelity or personal negligence reinforce stigma, limiting access to information, timely diagnosis, and treatment adherence “I think that some people still hold the belief that if someone received the syphilis vaccine and has a certificate indicating they were vaccinated, then—out of a sense of ‘care’—there remains this kind of immaturity in thinking, that leads people to say that someone who got that vaccine must be a promiscuous person. In other words, someone who takes that kind of precaution is assumed to have a very, very active sexual life.” (Claudia - General population)
Despite having limited and superficial knowledge about syphilis, most participants agreed that a syphilis vaccine should be offered universally to all sexually active individuals, expressing that exposure risk is not confined to specific groups and that prevention should be accessible to everyone.
Thematic category 3: Healthcare provider–user relationship a potential facilitator of acceptability
The interaction between users and healthcare providers emerged as a central component in individuals’ willingness to accept a hypothetical syphilis vaccine. Most participants expressed that contact with health services—even for reasons unrelated to vaccination—represents a strategic opportunity to promote vaccination. The quality of the relationship established between healthcare personnel and users plays a fundamental role in building trust and supporting informed decision-making. Specifically, participants identified three key aspects of the healthcare provider–user relationship that could facilitate vaccine acceptability: horizontal treatment, healthcare provider credibility and expertise, and clear, unbiased health information.
Horizontal treatment
Participants valued healthcare providers who treated them with respect, without judgment, and as equals. This horizontal relationship was seen as essential for building trust and facilitating open communication about sensitive topics such as sexual health and STI prevention. “For me, horizontal treatment would be important, that they don't look down on you, that they don't judge you for what you do or don't do. You go to ask for help, not to be pointed at.” (Sergio – General population)
Healthcare provider credibility and expertise
Participants expressed that healthcare personnel can strongly influence vaccination decisions through direct recommendations and by integrating vaccination into routine care. Their technical authority and professional credibility positioned them as key decision-making actors. Participants emphasized the need for clear and truthful information, viewing healthcare providers not only as vaccine administrators but also as educational agents responsible for addressing misconceptions and supporting informed choices. Healthcare professionals expressed favorable attitudes toward vaccine introduction and anticipated high acceptance, particularly among vulnerable populations. They highlighted the importance of leading by example, noting that receiving the vaccine themselves would strengthen public trust and reinforce an institutional pro-vaccine culture aligned with their ethical commitment to collective health. “Well, health personnel also have sex lives… the professionals themselves who choose to make their experience visible after being vaccinated, how they felt. That also helps bring the population closer to making a decision… I think it’s very positive to start with oneself.” (Cynthia - Health professionals)
Clear, unbiased health information
Both users and healthcare professionals stressed the need for accessible, understandable, and evidence-based information about syphilis. Clear communication was identified as a key element for reducing fears, dismantling myths, and supporting vaccine acceptance. Participants emphasized that healthcare providers must deliver unbiased information about the vaccine, free from stigma, moral judgments, or omissions. They valued transparency and expected providers to communicate in accessible language, avoiding unnecessary technical jargon. In this way, the active participation of healthcare personnel lends legitimacy to the vaccine and strengthens its acceptance. “Before recommending a vaccine, I would like to know the benefits and risks. That they don't hide anything from me, because if later the patient has an adverse reaction and I didn't warn them, trust is broken” (Carmen - Health professionals) “What we need is honest information. If the vaccine has side effects, let them say so. If it hurts, let them say so. But don't lie to us or hide things so we accept. Because afterwards we lose trust.” (Tilsa - Sexual minority)
Discussion
This exploratory, formative study identified attributes and other factors related to acceptability, anticipated barriers to uptake, and strategies to help design a DCE study and to support the equitable implementation of a future syphilis vaccine. Overall, high acceptability was observed across all five populations, with many participants expressing willingness to vaccinate for both personal and peer protection. To support acceptability, clear and concise information from reputable sources was considered highly important, although vaccine doubts were influenced by regional, national, and historical contexts. 30 In general, vaccination decisions were shaped by convenience, confidence, and complacency toward health authorities. 31
This analysis must be situated within the COVID-19 pandemic in Peru and its lasting disruption of public health systems and vaccination efforts, which continues to shape public trust in vaccines more generally. Peru had one of the highest mortality rates worldwide 32 and underwent a prolonged state of emergency, including a lockdown exceeding 100 days. 33 Simultaneously, the circulation of unproven treatments—some promoted even by healthcare professionals—, political instability and a scandal involving the irregular vaccination of government officials outside of a clinical trial 34 eroded public trust. Widespread misinformation further fueled confusion, anxiety, and fear regarding both the disease’s origin and long-term vaccine effects. 35 The rapid development of the COVID-19 vaccines intensified concerns about safety and transparency, the participants reflected this view and identified multiple guarantees required for a new vaccine. They also came to view vaccines as tools for individual and collective protection and reinforced expectations of State-guarantee free access. These factors increased openness toward a syphilis vaccine but also clarified demands for clear and transparent processes to counter misinformation.
As in the present study, other research36,37 has underscored the importance of ensuring vaccine safety and addressing key determinants of acceptability in order to reduce barriers to integration within health systems. Likewise, participants recognized the need to guarantee vaccine efficacy and implement promotional efforts and informational campaigns that strengthen public knowledge about vaccines and STIs, particularly syphilis. Notably, despite high reported acceptability, mixed-methods evidence on how specific vaccine characteristics—such as dosing, timing and cost—influence acceptability remains limited and is critical for effective future vaccination campaigns. 20
Other studies38–40 also identified barriers to acceptability, including concerns about post-vaccination effects, time constraints that limit participation, and distrust or perceived mistreatment by healthcare personnel. In contrast, facilitators included motivation for sexual health self-care and protecting close network, recommendations from healthcare professionals, and positive experiences with health services. These findings are consistent with prior qualitative research on HPV vaccination among men who have sex with men, where perceived susceptibility to STIs, trust in healthcare providers, and concerns about stigma influenced vaccine attitudes and acceptability. 41 In the current research, trust in health authorities and evidence of clinical studies demonstrating vaccine safety and efficacy was reported as increasing vaccination willingness.
The findings carry several potential policy and vaccine design implications. Preference for single-dose regimens suggests that vaccine development should prioritize single-dose formulations, and that multi-dose schedules must include adherence supports. The importance of provider credibility calls for training in empathetic, clear communication that addresses concerns about seropositivity and stigma. Structural barriers (cost, access, information) must be addressed to translate acceptability into uptake. Future research, including the planned DCE can help to determine trade-offs and constraints as it is likely that a syphilis vaccine will not be able to fulfill every desired characteristic. Should focus on four areas: implementation strategies for integrating syphilis vaccination into existing services; communication approaches for vaccine-induced seropositivity; quantitative estimates of risk compensation; and community-based development of culturally appropriate health education.
Finally, these findings should be interpreted as exploratory only and with caution due to the study’s limitations. First, the hypothetical nature of questions on a vaccine is paramount. This research does not capture actual vaccination acceptance or uptake, we can only speak to characteristics expressed as important for future acceptability. Second, participants were recruited from STI health centers in Lima. This strategy only captures individuals accessing these services, which may influence their views of STI care and STI stigma. Third, focus group methodology may have discouraged dissenting views, potentially biasing findings toward socially acceptable responses. Fourth, the study was conducted only in Lima and may not reflect perspectives from other regions with different cultural norms and healthcare access. This research was an exploratory formative study focused on identifying attributes for a future DCE. The goal was to generate baseline evidence on vaccine perceptions to inform future community-engaged participatory research and the co-design of implementation strategies.
Conclusions
There was interest in and acceptability of a hypothetical syphilis vaccine; however, acceptability depended not only on the vaccine’s attributes but also on structural enablers and the quality of interactions between users and healthcare providers. Strengthening provider communication, addressing structural barriers, and ensuring transparent dissemination of information will be essential for equitable future implementation of a syphilis vaccine.
Supplemental material
Supplemental material - Perceptions of acceptability and preferences surrounding a hypothetical syphilis vaccine in Lima, Peru
Supplemental material for Perceptions of acceptability and preferences surrounding a hypothetical syphilis vaccine in Lima, Peru by Valeria Fulqui, Wendy Hamasaki, Jessica Perez, Gilbert A. Orta Portillo, Jeffrey D. Klausner, Kelika A. Konda in International Journal of STD & AIDS
Footnotes
Acknowledgements
The authors thank all individuals who participated in the focus groups for generously sharing their time and experiences. The authors would also like to thank the field staff for their help with the recruitment.
ORCID iDs
Author contributions
JP and KK conceived and designed the study. VF and WH collected the data. VF, WH and GOP performed the data analysis. JP, VF, WH and GOP drafted the manuscript. KK, VF, WH and GOP interpreted the results. KK, VF and WH reviewed and edited the manuscript. All authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health, Grant R01AI139265, awarded to Dr. Jeffrey D. Klausner, University of Southern California. As well as a Dhablania and Kim Family Global Medicine and Health Fellowship grant.
Declaration of conflicting interests
The authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.