
Abstract
Background:
During the early postoperative period, it is important that the patient recovers without pain and inflammation, while preserving their quality of life. In this sense, coated titanium surfaces have been designed to release anti-inflammatory and analgesic drugs during the first postoperative hours.
Objective:
Evaluate the adsorption capacity and release profile of different bioactive titanium surfaces treated with three different drugs: acetaminophen, doxepin and ibuprofen.
Methods:
Four bioactive surfaces (polished, oxidized, hydroxyapatite precipitate, and polyvinyl alcohol coating surfaces) were physiochemically treated and analyzed.
Results:
Hydroxyapatite coatings were the roughest, while PVA coating was the softest. Acetaminophen was the only drug detected on all the surfaces. In contrast, higher drug doses were loaded into the PVA coatings, showing a satisfactory release profile.
Conclusion:
The results suggest that a rougher or ionically charged surface does not guarantee drug adsorption. In contrast, the use of a transport vehicle such as a polyvinyl coating ensures the release of the drug, initiating its therapeutic effect within the first minutes, and maintained for a period of between 120 and 180 min.
Introduction
For treating tooth loss, dental implants and implant-supported prostheses are the most effective options. To ensure the success of the treatment, it is important that the correct osseointegration of the device is achieved. This biological process, as described by Brånemark, involves direct contact between bone tissue and dental implant surface, without fibrous tissue developing at the interface.1–4 It is important that osseointegration occurs as soon as possible to avoid inflammation, bacterial development or fibrous tissue that would interfere with healing.
Titanium and titanium alloys are widely used in the manufacture of dental implants due to their biocompatibility, corrosion resistance, and excellent mechanical properties. Furthermore, the characteristics of the implant surface, including texture, wettability, and chemistry are particularly important at the initial stages of osseointegration, as they are crucial factors for cellular adhesion, proliferation, and differentiation.5–7 However, during the healing process, the presence of pain and inflammation may negatively affect the patient's quality of life, often requiring medication that can reduce or eliminate these symptoms in the postoperative period. It is well known that systemic drug administration can cause side effects when used repeatedly (e.g., headaches, sickness, gastrointestinal irritation).8,9 In this context, strategies have been developed to avoid systemic drug administration, focusing instead on enabling targeted drug delivery.
These strategies range from surface modification that allow the incorporation of drugs onto the titanium surface to polymer-based surface coatings that enable drug delivery and subsequent release. It has been demonstrated that surfaces modified by physical and chemical processes can successfully be loaded with therapeutic agents. Nanoporous surfaces have been described as having the ability to retain drugs on their surface and the release has been controlled using a polymeric matrix that acts as a protective barrier.10–13 Another strategy involves the use of surface coating layers, such as hydroxyapatite precipitates, zeolites, calcium, magnesium, strontium, zinc or polydimethylsiloxane (PDMS) derivatives, which can enhance control over drug delivery.14–21
The use of polymeric matrix, on the other hand, serves as a strategy to mitigate the drawbacks of systemic drug administration. It has been reported that these systems, known in the literature as a drug delivery system (DDS), can enhance the bioactivity and biocompatibility of the drug.22–24 DDSs can be designed by natural o synthetic polymers.13,25 Polyvinyl alcohol (PVA) is a synthetic polymer with bioadhesive properties, shown to be a biodegradable, biocompatible and non-toxic material. It has been used to develop DDSs, showing good results.9,26,27
Acetaminophen and Ibuprofen are commonly used in dental clinic treatments due to their therapeutic properties. Acetaminophen is known for its analgesic and antipyretic effects, while ibuprofen, a non-steroidal anti-inflammatory drugs (NSAIDs), offers antipyretic, analgesic, and platelet-inhibitory properties.17,28–30 On the other hand, doxepin is a tricyclic antidepressant that, when used in small doses, exhibits local analgesic effects when used in small doses. It has been used in combination with NSAIDs for pain management, and it has been reported to help reduce pain when combined with oral rinses.31–34
In this paper, various strategies for loading the titanium surface with analgesic and anti-inflammatory properties have been developed (polished titanium surface, anodized titanium surface, titanium surfaces with hydroxyapatite precipitates, and PVA-coated titanium surface). The surfaces were characterized by scanning electron microscopy (SEM) and whit light confocal microscopy. Surface topography was evaluated through amplitude parameters, while wettability was assessed by measuring the contact angle using the ADSA-CD technique. The release profiles of the surfaces were also assessed.
Material and methods
Study design
The aim of this study was to load titanium (Ti) surfaces with analgesic and anti-inflammatory drugs. Four different surface types were investigated: polished Ti (Ti), anodized Ti (OTi), Ti coated with hydroxyapatite precipitates (HATi), and Ti covered with a polyvinyl alcohol matrix (PVA). Acetaminophen, doxepin and ibuprofen were used to load the surfaces. Topographic profiles, adsorption capacity, and release profiles of the surfaces were measured.
Surface preparation
Cylinders of commercially pure ASTM grade II Ti (Manfredi, S. Secondo di Pinerolo, Italy) were used. (15 mm-diameter and 2 mm-thickness). The samples were cleaned with acetone (99.5%) using ultrasound during 10 min at 36° C. Afterward, acetone was replaced by deionized water, and the ultrasound process was repeated under the same conditions. The samples were removed and allowed to dry for 24 h at 37° C. A metallographic polishing process was applied to treat the titanium surface. Silicon carbide papers with grit sizes of 500, 800, 1200, 2500 and 4000 were used for this purpose. 35 To regulate the polishing process, all samples were examined under optical stereomicroscope (Olympus SZ-PT, Tokyo, Japan) at 100x magnification after each step. The cleaning process was replicated between each silicon carbide paper to remove titanium shavings deposited on the surface of the discs.
Finally, samples were treated with radio frequency plasma of argon (Emitech, KX1050 Plasma Asher) to a power of 25 W at 200°C for 15 min to remove organic impurities. Immediately after the plasma treatment, the oxidation state of the samples was stabilized by immersion in water for 24 h. Next, samples were allowed to dry for 24 h at 37 °C. 36
Design and surfaces treatments
Drug analytical method
Three different drugs were used: Acetaminophen (Fagron, Barcelona, Spain), Doxepin Hydrochloride (Fagron, Barcelona, Spain), and Ibuprofen (Sigma–Aldrich, USA). Initially, the calibration curve of drugs was established, and different concentrations were analyzed in according with Beer-Lambert´s law to determine the drug concentrations. Acetaminophen (27.7 μg/mL,), Doxepin (100 μg/mL), and Ibuprofen (80 μg/mL) concentrations were selected and measured by UV-Spectrophotometry at 257 nm, 292 nm, and 222 nm (λ max), respectively. The method was previously validated and verified for accuracy, precision, and linearity. All measurements were taken using a Perkin-Elmer UV-Vis Lambda 40 UV-spectrophotometer.
Bioactive surfaces
The polished titanium (Ti) disks were divided into three groups (n = 5 per group).
Group Ti: For this group the surfaces were only polished following to metallographic polishing protocol explained above. This group was considered as a control group.
Group OTi: Surface oxidation was achieved by alkaline heat treatment, which consists of immersing the titanium disks in a highly corrosive solution such as 5 M sodium hydroxide at 60°c for 24 h. 37 After this time, the samples were cleaned with acetone and rinsed with water using ultrasound for 10 min. Finally, the disks were dried at 40° C for 24 h. 38
Group HATi: When exposed to simulated body fluid (SBF), the newly anodized surface promotes bioactivation by facilitating the deposition of hydroxyapatite precipitate.39,40 As a first step, a SBF was prepared following the 1.5x Tas-SBF formulation protocol (Table 1). 41
Preparation of the simulated body fluid solution.
Formula; Tas-SBF (pH 7.4 at 36.7° - 37° C).
The samples were treated using the process as the OTi group. Subsequently, the disks were immersed in 0.2% v/v for 15 days at 36°C. Every 24 h, the SBF was removed and replaced with an equal volume of freshly prepared SBF. 41
Polyvinyl alcohol coating design (PVA)
The coatings were elaborated using a solvent evaporation process. 34 First, 3% w/v of PVA was dissolved in deionized water while the solutions were kept on stirring at room temperature until it was fully dissolved. Drug concentrations were added to the PVA solution for incorporation. To remove trapped air bubbles, the mixtures were left to rest for 48 h. After that, the solutions were poured into Petri dishes and dried at 37°C for 24 h.34,42 This group was named PVA.
Topographic analysis and wettability
Topographies were acquired with a white light confocal microscope (PLμ Sensofar-Tech, Barcelona, Spain), examining three discs per group and acquiring three topographies per disc with an EPI x50 objective (scan size area: 285 × 209 μm²). The microscope software provided data on the topographic parameters. 35 Parameters analyzed were average roughness (Ra), peak roughness (Rp maximum relative height), valley roughness (Rv maximum relative depth), absolute height (Rmax / t =Rp + Rv), root mean square (Rq), Skewness (Rsk), and kurtosis (Rku).7,43
Wettability was evaluated in three disks from each group by measuring the contact angle using the ADSA-CD technique (Axisymmetric Drop Shape Analysis-Contact Diameter). The contact angle (θ) was determined from a 1 mL sessile drop deposited on the surface with a micropipette, using Milli-Q purified water for the measurements. Measurements were taken in triplicate for each disk.
Surfaces drug loading
Bioactive surfaces adsorption
The bioactive surfaces were immersed in the concentrations mentioned above. All the samples were placed in a thermostatic bath at 25°C for 24 h. Subsequently, all samples were removed, and the supernatant was analyzed spectrophotometrically. The amount of drug adsorbed onto the surface was calculated by difference using the following formula:
In Vitro drug release assay
A release profile assay was performed to assess the ability of the surfaces to release the adsorbed drug.
For this, samples were placed in beakers and immersed in 3.5 mL of a solution similar in concentration to tissue fluid. Afterwards, solutions were placed in a hot bath, and the samples were shaken at 200 rpm for 6 h at 37 ± 0,5 °C. To determine the release curve at regular time intervals, 1 mL of the solution was withdrawn and replaced with an equal volume of tissue fluid. Samples were analyzed using a spectrophotometric method.
Statistical analysis
The results were observed as significant difference when p < 0.05. Data were analyzed with a Kolomogorov-Smirnov test to confirm that were parametric data. Then, data were analyzed with one-way ANOVA (surface treatment as main factor), followed by the post-hoc Student-Newman-Keuls multiple comparison test.
Results
Topographic characterization and wettability
Table 2 presents the roughness and contact angle values, showing that the Ra, Rq and Rp measurements were higher for HATi compared to the other surfaces. The Rv and Rt values varied across surfaces, with Ti showing the lowest measurements. The Rsk value was significantly negative for PVA and nearly 0 for Ti and HATi. PVA exhibited a platykurtic surface, while Rku values for Ti and HATi were close to 3. Surface wetting was higher for HATi and OTi, which showed similar results. Ti and PVA exhibited comparable but lower wetting values compared to the other two Figure 1. Illustrates the 3D topographic profiles of the surfaces studied.
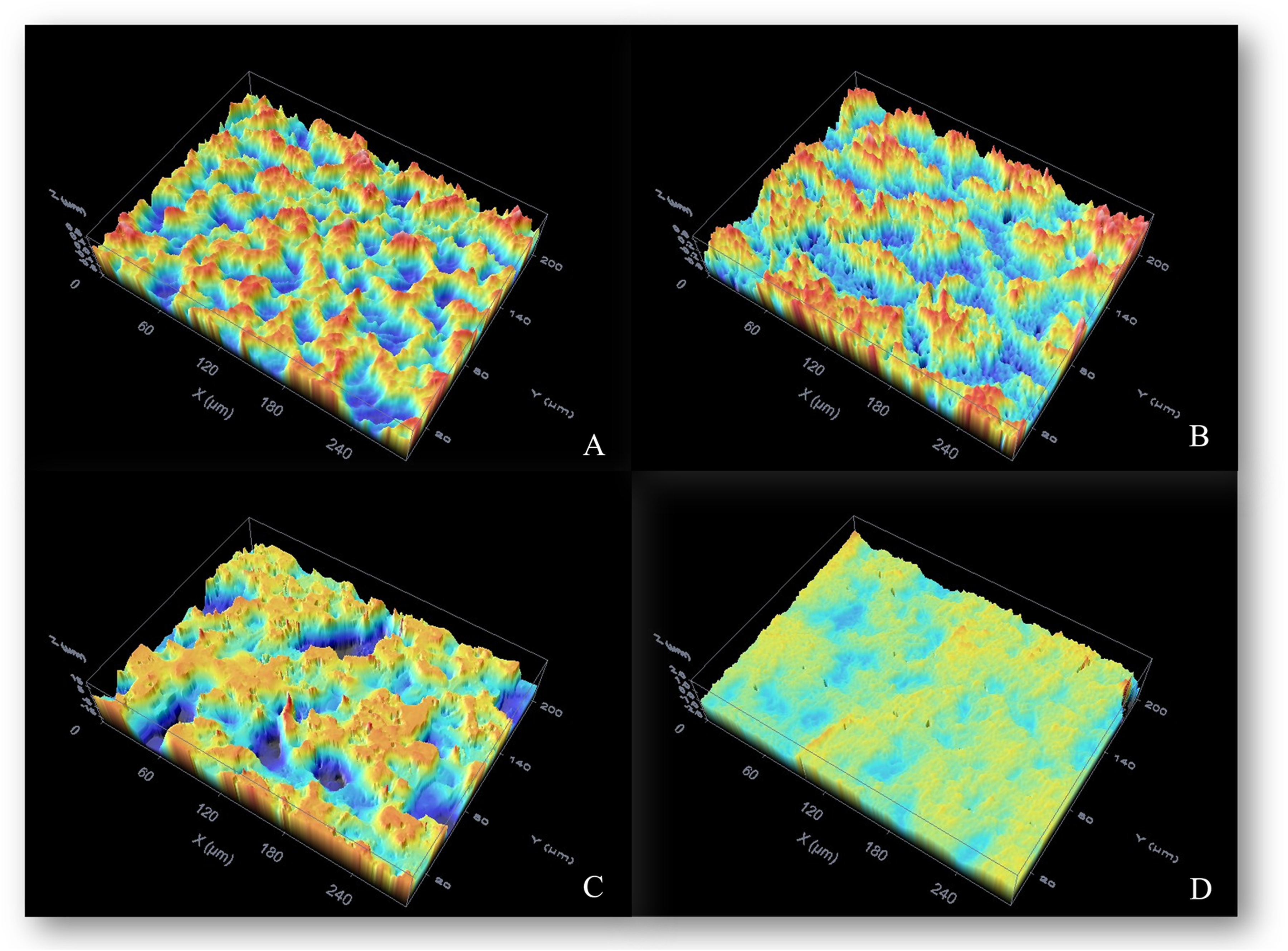
Topographic images of the analyzed titanium surfaces. A) Ti: Titanium Surface, B) OTi: Oxidized titanium surface, C) HATi: Hydroxyapatite precipitates surface, D) PVA: Polyvinyl alcohol surface.
Roughness and contact angle parameters.

Maximum relative height (Rp), Maximum relative depth (Rv), Arithmetic mean roughness (Ra), Root mean square roughness (Rq), Absolute height between the deepest valley and the highest peak (Rmax), the skewness (Rsk) and kurtosis (Rku). All measurements are expressed in nm with its standard deviation. n = 6 . Values in each row with different letters were statistically different (p < 0.05).
Bioactive surface
Figure 2 represents the different surface treatments used in this study. According to the results in Table 3, the modified titanium surfaces did not adsorb ibuprofen or doxepin. Only the machined titanium surface adsorbed a small amount of ibuprofen (0.8 μg/mL) and doxepin (0.77 μg/mL). Among the surfaces, the machined titania surface showed the highest drug adsorption (4.77 μg/mL), followed by the oxidized titania surface (4.36 μg/mL). The surface with hydroxyapatite precipitates exhibited the lowest adsorption dose (<0.1 μg/mL). However, all PVA coatings were successfully loaded. The coating concentrations on the disks were 13.01 ± 1.4 μg for acetaminophen, 47.01 ± 4.2μg for doxepin, and 37.58 ± 3.3 μg for ibuprofen, respectively.
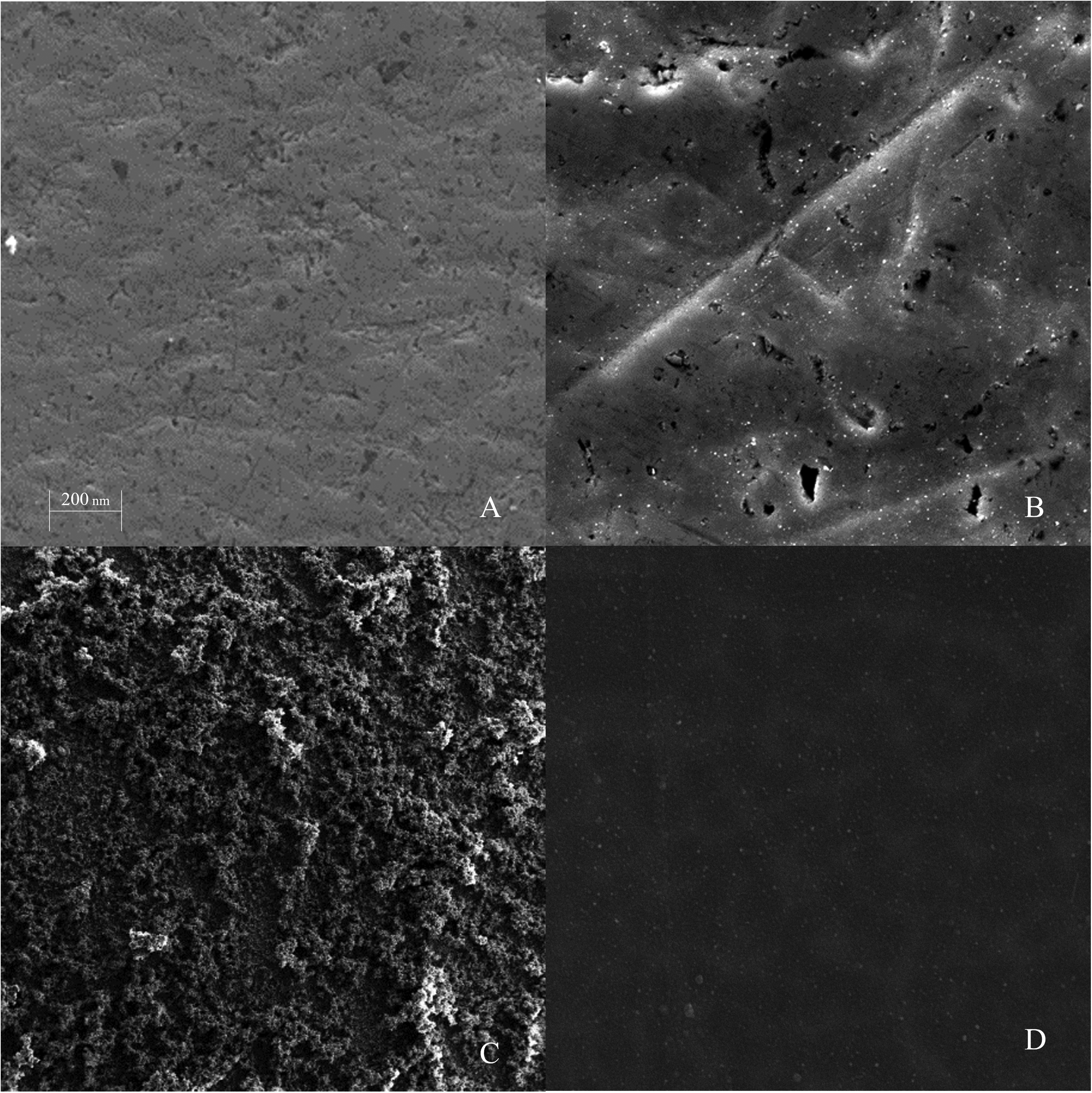
Illustrative SEM images of surface treatments. A) Ti: Titanium Surface, B) OTi: Oxidized titanium surface, C) HATi: Hydroxyapatite precipitates surface, D) PVA: Polyvinyl alcohol surface.
Adsorption capacity of modified surfaces.

All measurements are expressed in percentage (%) with their standard deviation. Metallographically polished titanium surface (Ti), Titanium surface oxidated by alkaline heat treatment (OTi), Titanium surface with hydroxyapatite precipitates by simulated body fluid (HATi), and Titanium surface coated with polyvinyl alcohol (PVA). Concentration: * 20.77 µg/mL, ** 80 µg/mL and *** 100 µg/mL. n = 3.
Drugs delivery
Due to the low or null adsorption percentages observed on the Ti, OTi, and HATi, the release profile could not be detected. In contrast, all surfaces with PVA coatings exhibited a similar release profile. The release profile of all PVA coatings exhibited two phases: a faster phase followed by a slower one. The rapid release occurred within the first few minutes for all PVA systems, with approximately half of the drug released within the first 60 min. This was followed by the second phase, which was slower and more constant over time than the first. All coatings reached their maximum peak at 240 min, and after this point, no drug was detectable in the medium (Figure 3).
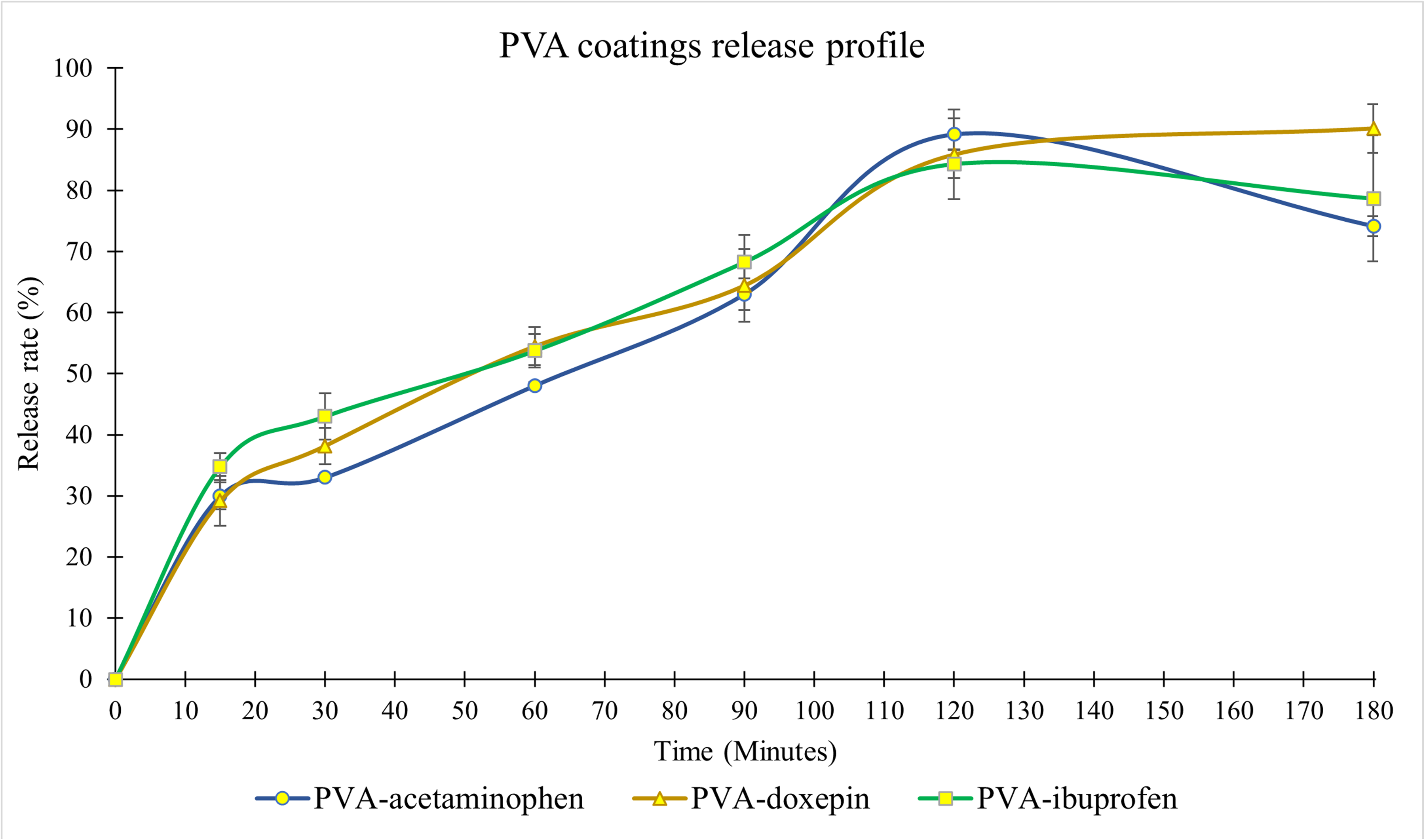
In Vitro testing of the drug release profile of PVA coatings. The release rate is expressed as a percentage (%). The time is expressed in minutes. n = 6.
Discussion
Four different surfaces were used, each with a unique purpose, to achieve targeted drug delivery. One strategy has been to modify wetting properties to promote drug adsorption. For this purpose, the Ti surface was modified to an alkaline heat treatment.37,44 It has been reported that this treatment did not alter the roughness but increased the wettability. 36 After soaking in NaOH solution, a new film consisting mainly of sodium titanate and sodium tantalate together with titanium and tantalum oxides was formed on the surface of the samples. Providing better hydrophilicity and improving its adsorption of water and protein.12,44–47
The titanium surface was successfully modified in this study, the increased hydrophilicity was insufficient to adsorb a significant amount of drug. All three drugs were detected on polished Ti surface, but after alkaline heat treatment, only acetaminophen could be detected, and to a lesser extent. Although ionized surfaces have been reported to be successfully loaded with drugs. These surfaces were coated with a layer of calcium, magnesium, strontium, zinc, or polydimethylsiloxane (PDMS) derivatives. Thus, facilitating the incorporation of the drug into the surface.12,14,21,48 Since the new chemical composition did not allow adsorption of the tested drugs, chemical treatment was not sufficient to improve adsorption. This could be due to the presence of certain functional groups on the surface that influence the interactions between OTi layer, drug molecules, and cells. 12
The drug uptake and release of three commonly used surgical materials, such as CaP, polyetheretherketone (PEEK), and Ti, were evaluated, reporting minimal to no drug release for PEEK and Ti samples. 49 In contrast, a study demonstrated the modification of ibuprofen release profile using an anodic nanoporous TiO2 layer with sodium hydroxide (NaOH) and 3-aminopropyltriethoxysilane (APTES). The results showed that the unmodified surface (ATO) exhibited faster drug release (82%) compared to the modified surfaces (Nam and ANam) with release percentages of 49% and 55%, respectively. 17 However, this surface was porous and allowed the drug to be incorporated into the porous structure.
Another strategy used to increase surface retention was to increase roughness. For this purpose, Ti was coating with Ha, making the surface chemically similar to the bone. It has been reported that an ionized surface can induce hydroxyapatite nucleation and deposition on titanium, as the ionically modified surface has a higher hydroxyapatite nucleation capacity.39–41,50 In this study, hydroxyapatite crystals were successfully deposited on the anodized titanium surface, demonstrating that coating the surface with HA deposits increases the roughness and wettability of untreated Ti, as previously reported by other researchers.36,41
Although the hydroxyapatite coating presented in this study showed physicochemical changes, these were not sufficient to facilitate drug adsorption and subsequent release. However, some researchers have reported drug adsorption and release from an HA coating. However, these surfaces were porous and allowed the drug to enter and deposit by immersion. Additionally, it has been possible to coat the surface with HA and load the coating with the drug by electrochemical deposition, a co-precipitation method in which the drug is mixed with SBF or, in some cases, with a sol-gel solution deposited using a spin-coating technique.16,19,20,51–53
The titanium (Ti) surface was coated with polyvinyl alcohol (PVA), which successfully enabled the loading of all drugs and allowed the release profile of the system to be measured. Using a polymeric matrix, such as polyvinyl alcohol (PVA), as a DDS is an interesting option for modifying surfaces. The effect of surface topography was minimized when the surface was coated with PVA, maintaining wetting values similar to those of the polished titanium sample. This resulted in a surface that was less hydrophilic compared to the Oti and HATi surfaces. Due to its favorable properties, including non-toxicity, biodegradable, bioadhesive, and being water-soluble. PVA has been approved by the Food and Drug Administration (FDA) and widely used in biomedical applications. 54
It has been reported that variations in PVA concentration during the design of polyvinyl alcohol-based DDSs influence the release profile of the system.24,55 The results of a study showed that PVA concentrations of 5% and 7.5% w/v to design buccal films exhibited a rapid release profile of ibuprofen within the first 15 min, during which more than 72% of the total drug was released. 55 Similarly, Salehi et al. (2017) reported that the release profile of rizatriptan benzoate varied depending on the concentrations used in the preparation of a DDS composed of polyvinyl alcohol, polyethylene oxide, and hydroxypropyl methylcellulose. The systems reached their maximum release peak between 40 and 80 min. 24 The release behavior of the PVA coatings was similar for all the drugs tested. However, a 3% w/v concentration of PVA exhibited a rapid release phase after 30 min. Following this point, a sustained release phase began. Peak release of the systems occurred between 120 and 180 min.
The utilization of PVA has proven to be a promising tool in various biomedical applications. It has been evaluated as a potential replacement for albumin in culture media and as a stabilizer for growth factors to facilitate the ex vivo expansion of hematopoietic stem cells (HSCs), with potential clinical implications in the treatment of hematological diseases. Likewise, its application in polymeric scaffolds has been investigated for the development of three-dimensional structures that support cell proliferation and differentiation, making it a promising option for the regeneration of damaged tissues. Additionally, studies have explored strategies to overcome the inert nature of PVA through its functionalization with biomolecules, bioactive nanoparticles (such as hydroxyapatite and chitosan), and the combination with osteogenic polymers, aiming to enhance cell adhesion and tissue integration. These modifications seek to expand the applicability of PVA in biomedical implants, scaffolds, and regenerative medicine. Further research is required to optimize these strategies and validate their efficacy in clinical settings. However, the advances in biomaterials engineering and nanotechnology continue to position PVA as a material with significant potential for biomedical and tissue engineering applications.56–59
Although PVA modifications aim to broaden its application in biomedical implants and regenerative medicine, its intrinsic bioinertness could hinder crucial elemental interactions at the implant-tissue interface in titanium-based systems, potentially affecting osseointegration. Therefore, controlling PVA removal or degradation after drug release is essential to ensure functional implant integration. Future research should optimize these strategies and validate their clinical effectiveness. Nevertheless, advancements in biomaterials engineering and nanotechnology maintain PVA as a material with significant potential in biomedicine and tissue engineering, including prosthetic coatings and advanced bone regeneration therapies. Despite its advantages, clinical studies are needed to confirm its efficacy and safety in humans, and to optimize specific formulations for different biological environments. The incorporation of biodegradable polymers in dental implantology represents a promising strategy for targeted drug delivery, potentially improving postoperative quality of life and tissue healing.
Conclusions
Physical or chemical treatment of the Ti surface does not guarantee surface drug loading. Although the wettability of the surface increased after alkaline heat treatment as well as with hydroxyapatite precipitate coating, the adsorption capacity of the surface was not changed. Hydroxyapatite precipitates make the surface very rough, but the change in roughness does not facilitate drug loading. Therefore, a rougher surface does not guarantee the adsorption of the drug on the titanium surface and a transport system is necessary to deliver the drug to the desired site. In this sense, it was necessary to coat the surface with a PVA matrix. PVA has proven to be a stable system over time, and its preparation and incorporation of the drug into the matrix is simple. PVA based DDSs are an alternative to improve clinical implant proprieties.
Footnotes
Abbreviations
Acknowledgments
Pablo Yael Carrazco Ávila acknowledges Universidad Autónoma de Sinaloa (México) for funding and supporting with a scholarship his studies of PhD program clinical medicine and public health at the University of Granada, Spain.
ORCID iDs
Author contributions
Funding
This work was supported by the Project PID2020.116082GB.I00 (MCIN/ AEI/10.13039/501100011033), Project C-CTS-305-UGR23 (University of Granada, Spain) and the research group CTS-974 (Junta de Andalucía, Spain).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available on request.