
Abstract
Background:
Ethical sensitivity has been identified as a foundational component of ethical action. Diminished or absent ethical sensitivity can result in ethically incongruent care, which is inconsistent with the professional obligations of nursing. As such, assessing ethical sensitivity is imperative in order to design interventions to facilitate ethical practice and to ensure nurses recognize the nature and extent of professional ethical obligations.
Aim:
To review and critique the state of the science of nurse ethical sensitivity and to synthesize findings across studies.
Research design:
Whittemore and Knafl’s revised framework for integrative reviews guided the analysis.
Research context and data sources:
A comprehensive, computer-assisted search of literature published in Cumulative Index of Nursing and Allied Health Literature and PubMed was performed. A systematic approach was used to extract, reduce, and synthesize the data.
Findings:
Four major conceptualizations of ethical sensitivity emerged from the literature. A sample of 25 reports met inclusion criteria, including 17 empirical reports and 8 theoretical reports.
Discussion:
Despite the existence of a concept analysis and a validated tool, ethical sensitivity remains a highly theoretical concept with multiple, and at times competing, conceptualizations. Ethical sensitivity has been assessed extensively in the context of ethical dilemmas; however, little attention has been paid to the way the concept operates in day-to-day practice.
Conclusion:
Future research should focus on better ways to operationalize and assess the concept, with particular attention to nurse awareness of the ethical content of everyday practice.
Introduction
The number of nurses implicated in malpractice payouts and adverse action reports has nearly doubled in the past decade in the United States (US). 1 A large portion of negligence lawsuits against nurses arise from “failure to act as a patient advocate.” 2 Additionally, recent media coverage has highlighted the inappropriate use of social media by nurses, such as posting photos of patient care areas after lifesaving situations 3 or posts about feeling bored at work and wishing for a “code.” 4 Most recently, an anonymously written piece in the Annals of Internal Medicine 5 described shocking vignettes in which sedated gynecological patients were treated as less than human in operating rooms, and witnesses failed to speak up. In each of these situations, practitioners failed to recognize the ethical implications of their actions or of their inaction.
Nurse ethical sensitivity can be defined as that which enables nurses to recognize the essentially ethical nature of practice 6 and of every practice action. The aim of every nursing action is to meet nursing goals as determined over time and as explicated in codes of ethics, which serve “as the profession’s nonnegotiable ethical standard(s).” 7 Ethical sensitivity is a necessary but insufficient antecedent to moral agency. 8,9 Nurse moral agency includes the willingness and ability to provide good patient care, which takes patient needs and values into account within the context of the care environment. 10
Ethical sensitivity has been identified as a foundational component of ethical action. 8 Diminished or absent ethical sensitivity can result in ethically incongruent care, which is inconsistent with the professional obligations of nursing. 7,11 As such, assessing ethical sensitivity is imperative in order to design interventions to facilitate ethical practice and to ensure nurses recognize the nature and extent of professional ethical obligations.
Ethics versus morals
Ethical sensitivity has also been termed “moral sensitivity” in many studies of the concept. Some have argued that there is a distinction between moral and ethics; others, however, have argued that in the context of “professional judgment and action” 12 the terms are synonymous. Using this line of reasoning, ethical sensitivity and moral sensitivity will be used interchangeably throughout this review, in accordance with the term used by the authors being referenced.
The review
Aim
The aim of this integrative review was to review and critique the state of the science of nurse ethical sensitivity and to synthesize findings across studies.
Design
The integrative review was the method of choice for this review of the literature, as this is the only approach that allows for the incorporation of various methodologies in order to develop a comprehensive understanding of the phenomena under investigation. 13 Ethical sensitivity is a theoretical concept, and as such, there are a variety of methodological approaches to assessing it. The methodology described by Whittemore and Knafl 13 was used to structure and conduct the review.
Whittemore and Knafl’s 13 framework was created to increase the rigor of integrative reviews in nursing. Their framework is widely cited in the nursing literature and was chosen based on their explicit description of the integrative review process and applicability of this process to the topic under investigation. Whittemore and Knafl’s process begins with the identification of a specified review purpose and variable of interest (in this case, ethical sensitivity). After this identification, the database search is conducted, using two to three strategies. The next stage is data extraction guided by the review’s purpose. After data extraction, data analysis may begin. It is at this phase that quality scoring of selected studies (both theoretical and empirical) occurs in order to evaluate the “authenticity, methodological quality, informational value, and representativeness” of sources 13 (p. 550). Data analysis involves arriving at a “unified and integrated conclusion” 13 (p. 550) about the problem of interest through data reduction, data display, data comparison, and conclusion drawing and verification. The following sections will describe the process used for this review, and the steps taken to ensure fidelity to Whittemore and Knafl’s method.
Search methods
A comprehensive, computer-assisted search was undertaken by the author. Databases used included Cumulative Index of Nursing and Allied Health Literature (CINAHL) and PubMed. These databases were chosen based on previous literature, suggesting the use of CINAHL and PubMed in conjunction to maximize the accuracy of the search. 14 Two databases were chosen based on Whittemore and Knafl’s guideline of two to three sources. Keywords included moral sensitivity, ethical sensitivity, moral sensitivity OR ethical sensitivity, and moral sensitivity OR ethical sensitivity AND nursing. Initial searches included articles published between 2009 and 2015 but were then expanded to include relevant literature with any date of publication. Reports were excluded if they were not about ethical sensitivity, were not about nursing, or were not published in English. Unpublished articles and gray literature were also excluded. 13 Included reports were not delimited to a target population. Findings from the database search were reviewed with content experts in order to ensure the reliability of the search.
Search outcome
Before eliminating duplicates, 272 abstracts were identified from CINAHL. Results from CINAHL searches included moral sensitivity (66 articles), ethical sensitivity (76 articles), ethical sensitivity OR moral sensitivity (71 articles), and ethical sensitivity OR moral sensitivity AND nursing (59 articles). The final yield of potentially relevant articles from CINAHL after title and abstract screening was 24, after eliminating duplicates. PubMed was then searched using the terms: ethical sensitivity OR moral sensitivity AND nursing (190 articles). Six new articles were found from this database through title and abstract screening, after eliminating duplicates. Subsequently, relevant articles were read in their entirety in accordance with Whittemore and Knafl’s recommendations. After full-text screening, an additional five articles were eliminated which did not meet the inclusion criteria of relevance to both ethical sensitivity and nursing. The final sample included 25 studies (17 empirical reports and 8 theoretical reports; see Appendix 1).
Quality appraisal
Quality scoring is complex, particularly in a review with a diverse sample such as this, and there is no gold standard for this process. 13 Whittemore and Knafl recommend that authors undertake a meaningful consideration of the quality of primary sources. In a review including both theoretical and empirical reports Whittemore and Knafl suggest several options, including the use of a separate quality instrument for papers of each type. Rather than using two instruments, this author chose to use the Johns Hopkins Evidence Appraisal Scale. 15 This scale was chosen because in addition to the strength score (1 (highest)–5 (lowest)), a quality score (A (high quality), B (good quality), or C (low quality)) was also incorporated, which enabled theoretical literature to be graded for quality in addition to strength of evidence. After database searching, the author graded reports for quality and strength. All reports deemed relevant were included in the review; however, the quality score was taken into consideration in the data analysis stage. 13 Grading and strength scores were also discussed with content experts in order to ensure objectivity (see Appendices 2 and 3).
Data abstraction
The data abstraction phase, conducted by the author and discussed with a nursing ethics content expert, proceeded according to Whittemore and Knafl’s 13 phases of data reduction, data display, and data comparison. Data from primary sources were included in the analysis if they met the inclusion criteria: reports written about ethical sensitivity, related to nursing, and published in English. Data were extracted and entered into a literature review matrix in the data reduction phase by the author (one matrix for empirical reports and one for theoretical reports), resulting in a “data display” table. Empirical sources were compared in the data comparison phase according to method, population, framework/conceptualization of ethical sensitivity, and major findings by the author. Theoretical sources were compared according to framework/conceptualization of ethical sensitivity and major arguments. After initial data abstraction, sources were coded by the author according to the framework/conceptualization of ethical sensitivity used by authors and subsequently clustered into groups based on this coding scheme.
Results
The final sample contained 25 relevant articles (see Appendix 4) published between 1983 and 2015. Seventeen empirical reports, including both qualitative and quantitative methods, were included in the sample, along with eight theoretical articles. The majority of empirical reports were descriptive, cross-sectional, or correlational studies and received strength scores of three (moderate strength) and a quality score of B (good quality). Theoretical reports largely received strength scores of four to five (low strength); however, these reports received high-quality scores (A’s to B’s).
Four major conceptualizations of ethical sensitivity emerged from the literature: Rest, 8 Lutzen et al., 16 Ersoy and Goz, 6 and Weaver et al. 17 As such, findings will be arranged based on these frameworks (summarized in Table 1). For each framework, related tools and/or methods for assessing ethical sensitivity will be introduced, along with relevant studies using these tools/methods. The purpose of reviewing these tools is primarily to describe their focus and context. A critique of the tools/methods will be offered in a later section. Reports discussing both ethical and moral sensitivity were included in the sample and the terms will be used interchangeably, as the terms are conceptually similar and distinctions between the two remain unclear.
Major frameworks, tools, and definitions.

NA: not applicable.
Ethical sensitivity: major frameworks and tools
Rest: Four-Component Model
Based on theories of moral development, Rest 8 developed his empirically supported Four-Component Model. Rest’s model includes moral sensitivity, moral judgment, moral motivation, and moral character. Moral sensitivity is defined as “the awareness of how our actions affect other people” and “involves being aware of the different possible lines of action and how each line of action could affect the parties concerned.” 18 Ethical (moral) sensitivity is a precursor to moral judgment (judging which action is right and wrong), moral motivation (prioritizing moral values over other personal values), and moral character (having strength of convictions, courage, persisting, overcoming). As such, ethical sensitivity is a crucial antecedent for moral action. While Rest’s 8 definition of ethical sensitivity was only explicitly used by two studies in this sample, 19,20 his definition of ethical sensitivity and his identification of its role in ethical decision making influenced the development of other prominent conceptualizations of ethical sensitivity. 6,16,17 There are no existing measures specific to Rest’s 8 model.
Lutzen
Lutzen et al. 16 developed a conceptual framework connecting the interrelated concepts of moral stress, moral climate, and moral sensitivity in a study of mental health nurses. Moral sensitivity is defined as “an understanding of patients’ vulnerable situation as well as an awareness of the moral implications of decisions that are made on their behalf” (p. 216). Moral stress is defined as “efforts to make clinical decisions involving conflicting ethical principles where patients’ autonomy is at risk” (p. 215) and is differentiated from moral distress. Moral climate is recognized as the context in which nurses practice and is defined as “the implicit values that drive health care delivery and shape the workplaces in which health care is delivered” (p. 215).
Moral Sensitivity Questionnaire
Lutzen et al. 21 –23 conceptual framework evolved from their previous work developing and using the Moral Sensitivity Questionnaire (MSQ). The authors’ definition of moral sensitivity (previously described) was the most commonly used in this sample, as was the MSQ as a measure. The MSQ assesses several dimensions of moral sensitivity: interpersonal orientation, structuring moral meaning, benevolence, modifying autonomy, experiencing moral conflict, and trust in medical knowledge and principles of care. 21
Since the original development for psychiatric nurses, the scale has been revised for use in other populations and settings. 23 The most recent version of the scale 23 was revised based on two samples of healthcare workers, including nurses, physicians, and nursing assistants (n = 278) resulting in a 9-question instrument with Likert scoring (1 = total disagreement to 6 = total agreement). Three major factors of moral sensitivity were identified in this analysis: moral burden (eigenvalue = 2.849), moral strength (eigenvalue = 2.184), and moral responsibility (eigenvalue = 1.368). 23 The authors conclude that the instrument is “a valid instrument for assessing moral sensitivity” (p. 193); however, statistics on reliability and the procedures for establishment of validity were not reported. 23
Five other studies in this review utilized the MSQ, reporting varying levels of reliability. 24 –27 In 2010, Han et al. 28 revised the MSQ for application in a Korean setting (alpha = 0.76). The revised version 28 was used by three studies in this sample. 24,29,30 A Chinese version has also been created (alpha = 0.82). 31
Despite its widespread use, findings from the use of this tool have varied widely. Furthermore, as the scale has been revised over time, the method of scoring responses has been inconsistent, making comparisons between cohorts of responders a challenge. Lutzen et al., 22 for example, found that there were differences between the moral sensitivity in medical nurses and psychiatric nurses and further differences between both types of nurses and physicians. In other words, nurses of different specialty areas and physicians are sensitive to different dimensions of the questionnaire (interpersonal orientation, structuring moral meaning, benevolence, modifying autonomy, experiencing moral conflict, and trust in medical knowledge and principles of care).
In later work, Lutzen et al. 16 found that moral stress was impacted by moral climate (r(43)= −0.398, p = 0.004) and certain aspects of moral sensitivity (r(48) = 0.414, p = 0.002). Stated differently, experiencing a negative moral climate increased moral stress, and nurses who were more “morally aware” (or ethically sensitive) were more morally stressed. 16 Similarly, Weaver et al. 17 found a significant relationship between job stress, anxiety, and moral conflicts (r = 0.28, p < 0.01). These findings were validated in a 2005 study of Norwegian nurses in which moral sensitivity in ethical conflicts was significantly negatively correlated with job stress and anxiety (r = −0.33, p < 0.05). 26 In a study evaluating the impact of clinical nursing supervision on moral stress, Severinsson and Kamaker 32 also found that the work environment has an impact on moral sensitivity, as reflected in various dimensions of MSQ scores.
As described, the MSQ has been revised for use with Korean nurses as well. The Korean revision of MSQ (K-MSQ) produces an overall score for moral sensitivity, ranging from 0 to 7. Findings using this tool have also varied. Ahn and Yeom 24 found low moral sensitivity scores in nursing students (2.83/7), while Kim et al. 29 found scores in Korean nurses to be high (5.14/7) and to be significantly positively correlated with knowledge of codes of ethics (r = 0.336, p < 0.001). Park et al. 30 evaluated the relationship of ethics education on moral sensitivity and moral reasoning and found that senior nursing students had higher scores on certain dimensions of moral sensitivity but that more hours of ethics content had no effect on the overall score on the MSQ.
In a study of Chinese nurses, Huang et al. 31 found relatively high levels of ethical sensitivity (scores based on an adapted scale; mean = 40.22 ± 7.08, range = 20–54), but that the conceptual understanding of the construct is not consistently reflected in practice. In qualitative interviews, the authors identified major barriers to ethical sensitivity, including lack of ethical knowledge and experience as a nurse, hierarchical organizational structure, and a conformist working attitude. 31
Ersoy and Goz
Ersoy and Goz 6 assessed the ethical sensitivity of nurses in Turkey by scoring nurses’ responses to hypothetical scenarios or “vignettes” of ethical dilemmas. The authors used the International Council of Nurses (ICN) Code of Ethics 11 as the ethical framework for their study. Ethical sensitivity is defined as “the capacity or ability to recognize an ethical problem (or an ethical dimension when an ethical conflict is not present)” (p. 300). 6 The scenarios evaluated were developed based on a survey of 22 nurses who had encountered “ethical problems” in practice. The final sample in this study consisted of 165 nurses in a variety of settings who were asked to provide written responses to three hypothetical scenarios. 6 Nurses were found to be sensitive to different ethical principles depending on the context of the dilemmas they were evaluating. For example, in one scenario, benevolence was the predominant consideration in decision making, and in a second scenario, autonomy was the most common principle used. 6
Vignettes
The vignette method of assessing ethical sensitivity has been used in other studies, particularly in evaluating physicians. 33,34 Borhani et al. 35 used Ersoy and Goz’s 6 conceptualization of ethical sensitivity in qualitative, semi-structured interviews of nursing students in Iran. The authors identified major influential factors, including individual and spiritual characteristics, education, mutual understanding, internal and external controls, and the experience of an immoral act. 35
Weaver et al
Weaver et al.
17
developed a conceptual model of the dimensions of ethical sensitivity.
36,37
Ethical sensitivity is defined as the capacity to decide with intelligence and compassion, given uncertainty in a care situation, drawing as needed on a critical understanding of codes for ethical conduct, clinical experience, academic learning and self knowledge, with an additional ability to anticipate consequences and the courage to act. (p. 610)
17
The authors identify preconditions (i.e. client perspective, suffering, vulnerability, and professional perspective), attributes (i.e. moral perception, affectivity, and dividing loyalties), and outcomes (integrity-preserving decision making). Positive outcomes (person-led care, client and professional comfort, and well-being) and negative outcomes (routine-oriented care, client suffering unrelieved, professional distress, and attrition) are identified. Positive outcomes are associated with self-transcendence and practical wisdom, whereas negative outcomes are associated with professional moral residue.
This conceptualization was also used by Jackson et al. 38 to argue that ethical sensitivity shapes the everyday work environment. It has not, however, been used in the development of measures to assess the concept. No empirical studies included in this sample utilized this framework.
Van Der Zande et al
Van Der Zande et al. 39 used Weaver et al.’s 17 definition to develop a new theoretical framework of ethical sensitivity. The authors conceptualize Professional Moral Sensitivity and Institutional Moral Sensitivity. Within each category, ethical sensitivity is divided into explicit and tacit moral knowledge. Moral sensitivity influences practice, which is considered the point of entry for research. The model’s focus is on Professional Moral Sensitivity. The new theoretical framework attempts to ameliorate the methodological difficulties of existing conceptualizations, particularly the difficulty in measuring the tacit nature of ethical sensitivity. 39 It has not been used in the development of measures.
Synthesis
Based on the results of the data abstraction phase, a synthesis in the form of a conceptual model was developed. The author extracted major concepts from the four major frameworks, and the relationships of these variables were diagrammed in order to explore their connections. The linkages shown in the model (below) are based on the theoretical or empirical relationships outlined in the 25 selected articles. The model underwent several iterations and was revised in response to discussions with colleagues who have familiarity with nursing ethics literature.
Conceptual model
The model (Figure 1) first examines context of the healthcare environment, 17 with emphasis on professional responsibilities as outlined by codes of ethics. 7,11 Context is followed by perception, in which ethical sensitivity 6,8 is either present or not. When ethical sensitivity is not present, the response is either inaction or routine-oriented action, which may lead to care that is incongruent with patient and professional goals. 17 Even if rote action occasionally leads to care that meets patient wishes and needs, without ethical sensitivity this will not universally occur.
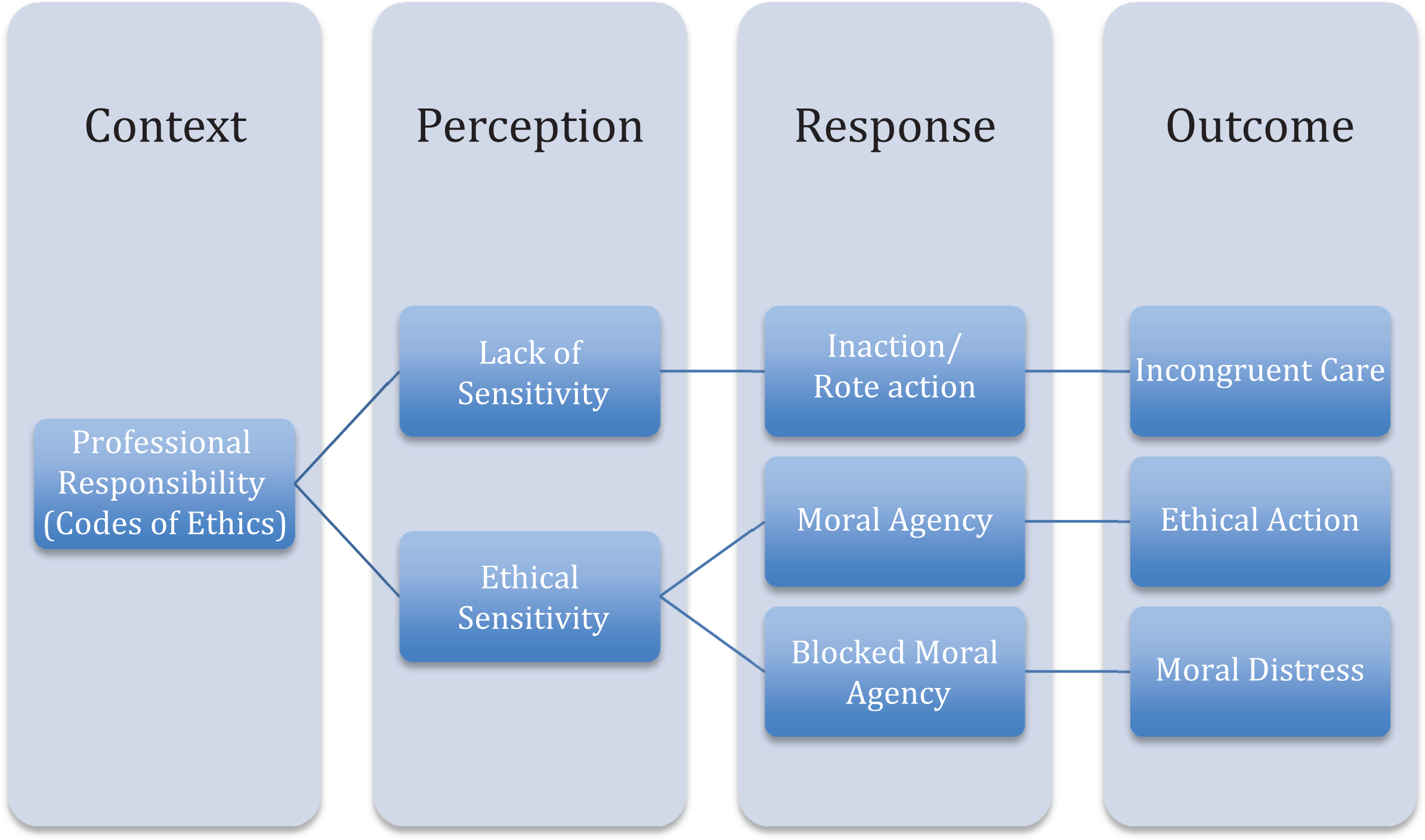
Conceptual Model.
When ethical sensitivity is present, there are several possibilities. First, ethical sensitivity can lead to moral agency. 9,17,23 Moral agency, in turn, leads to ethical action. 9 The presence of ethical sensitivity, however, is not sufficient for ethical action, particularly when context is prohibitive. This results in blocked moral agency and subsequent moral distress. 9
Discussion
As described, four major conceptualizations of ethical sensitivity exist in the extant literature and have resulted in the development of a major tool (the MSQ) and various qualitative methodologies for assessing the construct. Empirical articles generally are of moderate methodological strength and quality, and theoretical articles are of low methodological strength, but high conceptual quality. Despite the breadth and depth of research that has been done, several critical areas remain unaddressed. This section will explore the limitations of these previous studies, the challenges with existing measures, and the context in which previous research has been performed.
Ethical sensitivity has been conceptualized in multiple ways in existing literature. Despite a concept analysis identifying this challenge, 17 and a validated tool, 21,23 difficulties remain in assessing ethical sensitivity in a way that allows the translation of findings into practice. The concept of ethical sensitivity is defined as “the capacity or ability to recognize an ethical problem,” 6 “the capacity to decide with intelligence and compassion,” 17 “an understanding of the patients’ situation,” “an awareness of the moral implications of decisions,” 16 and finally “the awareness of how our actions affect other people.” 8 It remains unclear whether ethical sensitivity is a skill in recognition to be developed, a decision-making ability, or an awareness of the implications of nursing actions. While achieving conceptual clarity about ethical sensitivity requires further efforts, it is evident that a defining attribute across definitions of ethical sensitivity is an “awareness” of the ethical implications of nursing actions. Current measures suffer from limitations in terms of application to practice, and the context of previous studies has focused nearly explicitly on ethical sensitivity in the setting of ethical dilemmas.
Limitations of current measures
MSQ
Despite the wide use of the MSQ in this sample, the tool is not without limitations. Items on the MSQ are theoretical in nature. 27 This makes the translation of findings into relevant practice-based interventions difficult. Furthermore, many studies in the literature suffer from methodological challenges, including non-reporting or relatively low levels of reliability (approximately 0.76–0.82). These methodological issues pose major concerns in terms of the accuracy and reproducibility of findings using the tool.
Several authors have pointed out challenges with the MSQ. Baykara et al. 25 used the MSQ to assess the effects of ethics training on nursing students’ ability to recognize ethical violations and develop moral sensitivity. Findings of this study were inconclusive, as ethical sensitivity increased in the experimental group; however, this finding was not significant. 26 Similarly, Hebert et al. 33 adapted the measure to assess undergraduate and graduate nurses’ moral sensitivity and found that it was “not possible to draw conclusions based on the tool” (p. 116). Comrie 40 suggests the need for further tool development. Lutzen et al. 16 have, in fact, suggested revising the MSQ to assess both actions taken as well as the “sensing” of moral problems.
Qualitative methods
Other methods 6,35 have been used in attempting to measure ethical sensitivity, particularly the qualitative evaluation of “responses to actual or hypothetical vignettes involving dilemmas” (p. 196). 37 The limited generalizability of these findings and rather subjective approach of scoring responses is one drawback to this method. However, the results of these analyses are less theoretical in nature, and more attention is given to the ethical principles used in decision making.
In addition to the need for revised measures, there is a need to develop empirical-based interventions to support the development of ethical sensitivity. 41 Ethical sensitivity is a necessary first step in ethical action and moral agency and as such is a crucial attribute of ethically competent nurses. The design of interventions to improve ethical sensitivity, however, is a challenge without conceptually clear measures.
Context of previous studies
The MSQ and vignette methods both focus on measuring ethical sensitivity in the context of ethical dilemmas such as hiding a diagnosis from a patient 6 or giving medications by force if a patient refuses to take them orally. 22 Current methods of assessment do not explicitly assess nurse awareness of the ethically laden nature of everyday practice actions.
As Van Der Zande et al. 39 suggest, the “daily practice of care should be the point of entry for ethical sensitivity research” (p. 75). The importance of ethical sensitivity in the context of everyday practice cannot be over emphasized; as Austin 42 argues, “ordinariness of everyday ethical issues means their moral significance goes unrecognized” (p. 82). The early recognition of the ethical content of practice is important in nurses effectively acting as moral agents. 9
Without ethical sensitivity (in terms of recognizing ethical content) moral agency will likely not take place 9 as nurses need to recognize the ethical content of a situation before taking ethical action. Without moral agency, the resulting care may be incongruent with patient preferences and professional goals. 17 Furthermore, when ethical sensitivity does not result in moral agency, nurses may experience moral distress, 4 which has been tied to attrition, nurses distancing themselves from patients, and other deleterious outcomes. 43
Anecdotal evidence suggests that ethical sensitivity to the content of everyday practice is not well developed. According to Troug et al., 44 “clinicians commonly do not recognize the ethical elements underlying everyday clinical encounters” (p. 12). Despite professional expectations 7 establishing that good nursing practice is good ethics, 45 it is unclear whether nurses recognize nursing as an ethically laden practice. 9
Limitations of the review
There were several limitations to this review. The exclusion of gray literature introduces the risk of publication bias; 46 however, a meta-analysis was not performed, thus gray literature is unlikely to have drastically changed these results. The use of a single reviewer may be considered a limitation. Given this drawback, rigorous adherence to inclusion and exclusion criteria, along with adherence to the chosen methodological framework, was a priority.
Finally, the use of a quality and strength appraisal scale that encompasses both empirical and theoretical literature could be considered a limitation. It is well established that appraising the quality of qualitative literature is a controversial process. 47 Using purely empirical methods, theoretical and qualitative literature rank lower in strength than traditionally empirical studies. As previously described, the Hopkins Evidence Appraisal Scale 15 was chosen because in addition to the strength score, a quality score was also incorporated. This enabled theoretical literature to be graded for quality in addition to strength of evidence.
Strengths of the review
This review is the result of the author’s lengthy and continuing immersion in the extant ethical sensitivity literature. Despite the use of a single reviewer, the process of article selection, data abstraction, and synthesis into a conceptual model was the subject of ongoing discussion between the author and several colleagues who are content experts in both nursing research and nursing ethics, which ensured rigor and fidelity to the process. These colleagues also reviewed drafts of this article. Finally, an earlier version of the conceptual model was presented at an interdisciplinary conference and was revised based on audience feedback.
Conclusion
This review of the literature identified multiple conceptualizations of ethical sensitivity. Future research should focus on better ways to operationalize and assess the concept, as definitional clarity is needed in order to design valid and reliable measures. Additionally, the focus of most studies thus far has been on ethical sensitivity in the context of ethical dilemmas and has been theoretical in nature. Despite the understanding of its important role in dilemmas and in enacting moral agency, there is a lack of understanding regarding how ethical sensitivity operates in day-to-day practice.
Furthermore, it remains to be established whether or not nurses have awareness of the inherently ethical nature of every practice action. Awareness emerged as a defining attribute of ethical sensitivity in this review. Ethical awareness is a necessary, albeit insufficient, component of and precursor to ethical sensitivity, subsequent moral agency, and moral action. 48 Before interventions aimed at improving ethical decision making and enacting moral agency can be sufficiently designed, it is necessary to establish whether or not nurses recognize the ethical content of everyday practice. Without this awareness, the other components of ethical sensitivity will not be activated.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1
Appendix 2
Appendix 3
Appendix 4
Theoretical literature.

| Reference | Framework | Argument |
|---|---|---|
| Baeroe and Norheim, 19 Norway | Rest |
Clinical ethics support services must pay attention to real-life ethical issues Outline of ethical tensions in clinical care Identify neglected areas for ethical research |
| Jackson et al., 38 USA | Weaver |
ES should shape every action and interaction ES affects the everyday lives of nurses and should be enacted every day ES can be used to describe people who embody positive ethical relationships, adhere to a personal set of ethics in dealings with others Poor ethical sensitivity may result in people becoming inured to bad behavior |
| Lutzen and Ewalds-Kvist, 9 Sweden | – Lutzen – Victor E. Frankl |
Explore interconnection between moral distress, ES, and moral resilience using Frankl’s existential philosophy Argue concepts are theoretically related using hypothetical scenarios Moral sensitivity can lead to moral distress in cases in which one is unable to enact moral agency |
| Robichaux, 20 USA | Rest |
Uses Rest’s Four-Component Model as a framework for helping practitioners develop skills to recognize and engage in both critical and everyday ethical scenarios Ordinary, everyday ethical occurrences may go unrecognized but are ethically important |
| Weaver and Morse, 37 USA | Weaver |
Analysis of ES using the pragmatic utility method ES identified as a quality similar to a virtue or caring attitude Emphasize the importance of courage and uncertainty in ethical decision making Identify characteristics of ES: Preconditions: suffering and vulnerability cues, uncertainty, relationships characterized by receptivity, responsiveness, and courage Attributes: moral perception, affectivity, dividing loyalties Outcomes: client comfort and well-being, professional learning, self-transcendence, integrity-preserving compromise |
| Weaver, 36 USA | Weaver (Rest, Lutzen) |
Review of ES literature Recognized as first component of ethical decision making ES has competing descriptors, inadequate exploration of crucial issues, and threats to generalizability and validity Three competing frameworks: Rest, Lutzen et al., business/journalism Further analysis needed: if ES is innate/acquired, how it relates to agency What exactly must occur for the individual components to come together as an instance of ES is not known Predisposing conditions/consequences unclear |
| Weaver et al., 17 USA | Weaver |
Concept analysis of ES ES develops in contexts of uncertainty, client suffering and vulnerability, and through relationships characterized by receptivity, responsiveness, and courage on part of professionals Essential attributes: moral perception, affectivity, dividing loyalties Outcomes: integrity-preserving decision making, comfort and well-being, learning and professional transcendence Argue ES as a type of practical wisdom |
| Van Der Zande et al., 39 Netherlands | Weaver adaptation |
Development of conceptual model of ES Argue little attention paid to tacit dimension of ethical knowledge and discuss methodological difficulties of current conceptualization Make distinction between explicit and tacit moral knowing Focus on explicit and tacit moral knowing in decision making and daily care practices |
ES: ethical sensitivity.