
Abstract
Background:
There is growing awareness that patient care suffers when nurses are not respected. Therefore, to improve outcomes for patients, it is crucial that nurses operate in a moral work environment that involves both recognition respect, a form of respect that ought to be accorded to every single person, and appraisal respect, a recognition of the relative and contingent value of respect modulated by the relationships of the healthcare professionals in a determined context.
Research question/aim:
The purpose of this study was to develop better understandings of perceptions of nursing’s professional respect in community and hospital settings in England.
Research design:
The research design was qualitative. Focus groups were chosen as the most appropriate method for eliciting discussion about nursing’s professional respect.
Participants and research context:
A total of 62 nurses who had been qualified for at least a year and were working in two localities in England participated in this study.
Methods:
Data were collected using 11 focus group sessions. The data were analysed by means of an inductive content analysis, extracting meaning units from the information retrieved and classifying the arising phenomena into conceptually meaningful categories and themes.
Ethical considerations:
To conduct the research, permission was obtained from the selected universities.
Results:
Recognition respect of human beings was perceived as ingrained in the innermost part of nurses. Regarding appraisal respect, a great importance was placed on: the interactions among healthcare professionals, the time to build trust in these relationships, the influences of the workplace characteristics and nurses’ professional autonomy and decision-making.
Conclusion:
Recognition respect of persons was embedded in the inmost part of nurses as individuals. Concerning appraisal respect, it was thought to be deeply enshrined in the inter- and intra-healthcare professional interactions. The forging of trusting relationships over time was deemed to be strongly associated with good quality interactions with other healthcare professionals.
Keywords
Introduction
Research shows that patient outcomes are worse when nurses work in a disrespectful environment.
1
This study evaluates nursing’s professional respect in community and hospital settings in the United Kingdom, specifically in England. Understanding the determinants of professional respect as perceived by nurses will help to develop methods to improve their professional respect in the work environments where they practice. Before speaking of nursing’s professional respect as an underexplored and underestimated central ethical phenomenon of the nursing discipline, it is important to not forget the meaning of the word respect for the ethical epistemologies of the caring disciplines. In fact, much of the debate since the inception of nursing has focused on how nurses conveyed respect to persons they care for. It is in this very active respect of humanity – in the relational ethics
2
–5
of care approach – that professionals can find the moral underpinnings of nursing. To care for others means to take care of human beings actively and not merely as passive objects of morality. Hence, respect for recipients of care constitutes a basic moral value of nursing and has been discussed in the literature as a vital concept fundamental to nursing practice in different fields.
6
–8
In this regard, Browne
9
(p. 213) defined respect in the context of nursing as, Respect is a basic moral principle and human right that is accountable to the values of human dignity, worthiness, uniqueness of persons and self-determination. As a guiding principle for actions toward others, respect is conveyed through the unconditional acceptance, recognition and acknowledgement of the above values in all persons. As a primary ethic of nursing, respect is the basis for our attitudinal, cognitive and behavioural orientation toward all persons.
Peter et al. 15 define the moral work environments as ‘those in which differently situated people experience their responsibilities as intelligible and coherent fostering recognition, cooperation and shared benefits’ (p. 356). Thus, the characteristics of morally healthy environments are being recognized as critical to prevent moral distress, 16,17 to promote higher job retention and to lower staff turnover. 18 Studies of violence and bullying 19,20 demonstrate that when a workplace lacks moral fitness, nurses experience emotional distress. In disrespectful settings, intra- and inter-professional relationships can be characterized by indifference and contempt through the use of ridicule, objectification and discrimination. 21
Hence, it is possible to conclude that nurses desire to work and thrive 22 where they are able to develop respectful relationships with peers and other healthcare professionals and are able to practice in accordance with the basic moral values of their profession. 23
Background
The concept of respect
The etymology of respect comes from the Latin respicere, which means ‘treat with deferential regard or esteem’. 24 Although many philosophers give respect a central place in ethics, they differ regarding its meaning.
Darwall, a leading philosopher regarding the concept of respect, posits two forms: recognition respect and appraisal respect. Recognition respect is seen to be ‘that persons as such are entitled to respect…that they are entitled to have other persons take seriously and weigh appropriately the fact that they are persons as such’ (p. 38). 25 Darwall clearly asserts that moral recognition respect is a form of respect that ought to be accorded to every single person and is not a matter of degree. Moral recognition respect is an acknowledgement of the essential, intrinsic and irreducible dignity of each individual and is therefore non-comparative; it is not contingent on social roles, positions or any other contextual personal features. 25 In the context of moral recognition respect, disrespect entails a failure to recognize the humanity of another person and treat him or her accordingly.
Appraisal respect, conversely, is a recognition of relative and contingent value and is determinative of esteem, deference and honour. Appraisal respect ‘consists in a positive appraisal of a person, or his [sic] qualities’ (p. 39). 25 Therefore, conferring appraisal respect is a facet of relational engagement: it is a matter of degree and is connected to the social contribution and character traits of the person being appraised. This form of respect is conferred in grades or on a continuum. Therefore, unlike recognition respect, there can be discontinuity in the amount accorded and the amount deserved. That is, there can be a difference in the degree of respect one person accords another. In the context of appraisal respect, disrespect is the negative end of the continuum in which a person is appraised as deserving condemnation. Appraisal respect could also be applied to a profession, in our case nursing.
As a facet of relational engagement, appraisal respect is embedded in time and place and is identified and expressed at various levels; it is conferred by actions of reciprocity in the social context. In this sense, as a relational engagement, appraisal respect will value morally virtuous personal attributes such as honesty, integrity, fairness, compassion, reciprocal trust and responsibility. 26
Respect: its relationship to dignity and the concept of professional respect
Definitions of respect all entail a person recognizing value in another person, that is, giving dignity to the human being, to the other. Respect for persons is a foundational principle of morality. Hence, demonstrations of respect are a pre-eminent normative construct of the moral existence of human beings. 27,28 Among others, Kant recognized in the inner part of this subject (and only in the very internal part of the subject) the basis of respect. Respect, for Kant, is born in human beings as respect of themselves and of their dignity as persons.
Kant
29
wrote in the Grounding for the Metaphysics of Morals: In the realm of ends, everything has either a price or a dignity. Whatever has a price can be replaced by something else as its equivalent; on the other hand, whatever is above all price, and therefore admits of no equivalent, has a dignity.
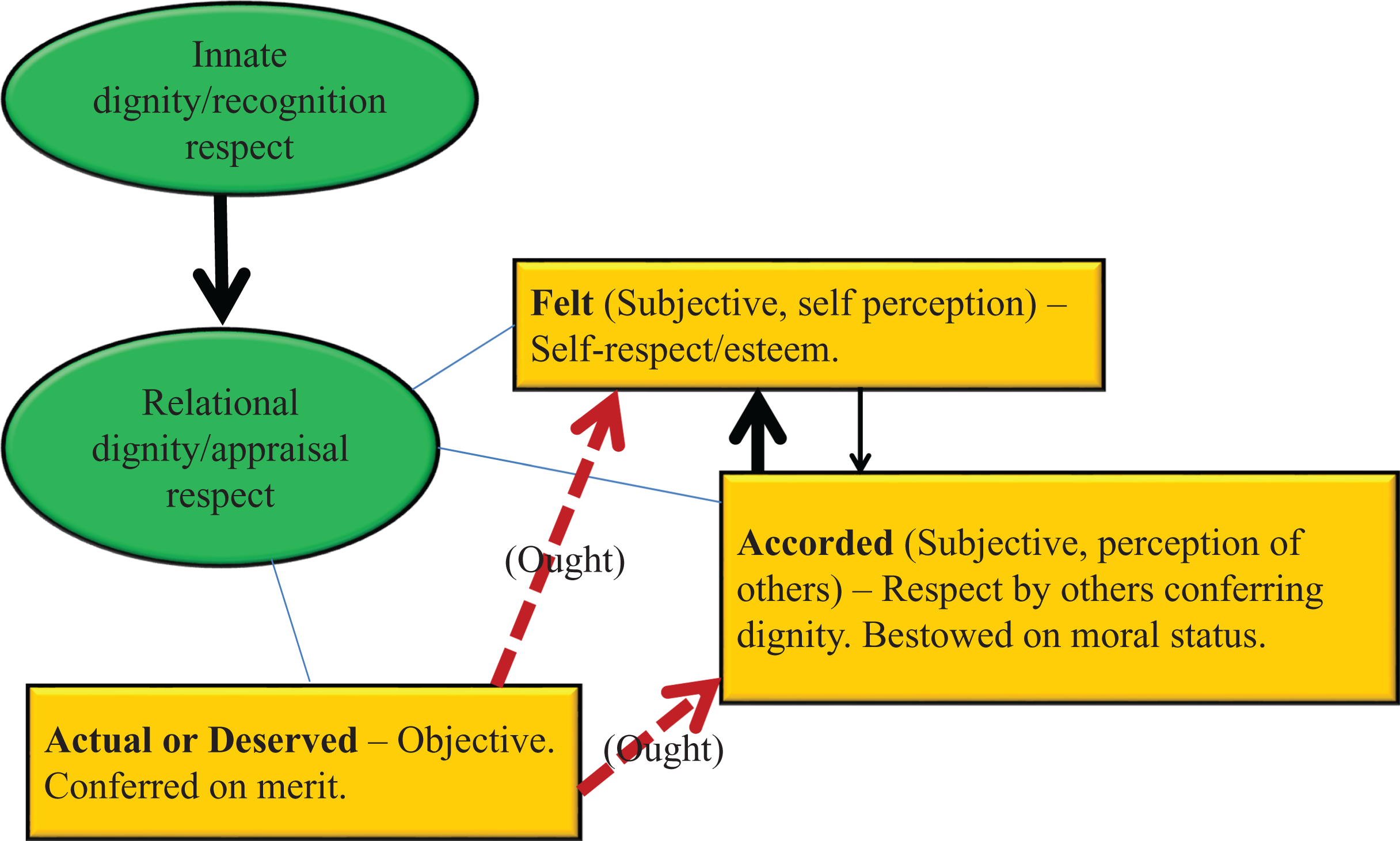
Main attributes of the concepts of moral recognition respect and appraisal respect connected to innate and relational dignity.
As already mentioned, respect can be shown in relations between professions and professionals. Such respect would be a combination of recognition and appraisal respect. The respect due to any person, based on their humanity, that is, recognition respect, should be shown to other caregivers in the workplace. Belittling, incivility 33 and other forms of disrespecting another’s basic humanity are inappropriate in any human relationship and it is even more harmful in health professional relations because of the potential damage to patients. 34 Additionally, the value of a profession should be recognized in relations between professions so that the values brought to patient care by nursing, for example, are acknowledged. Unfortunately, barriers developed historically 35 and perpetuated by factors of gender and social class have been elements that have consolidated the professional boundaries among health professions. 36 Although relationships in the healthcare arena have evolved over time and have become more teamwork based, nursing has always endeavoured to define its identity primarily because other disciplines such as medicine were thought to possess exclusive knowledge that conferred primacy even in inter-professional teams. 37 In recent years, there has been a greater focus on inter-professional education 38 and inter-professional and inter-agency collaboration 39 to foster patient-centredness and to overcome the imbalances of power in the relationship between nursing and medicine. 40,41 However, there is a growing body of literature that suggests that although the situation is slowly changing, especially in nursing advanced countries, the nursing profession continues to lag behind medicine in receiving the respect it deserves. 42,43
For this reason, and despite scarce empirical research in the last 10 years, the importance of feeling respected by nurses and other healthcare professionals in the work environment has become an important issue for the nursing profession and for better healthcare outcomes. Studies have linked a better work environment as conducive to better patient outcomes; 44 the extent to which nurses feel respected intra- and inter-professionally is likely to be a highly influential factor on their professional practice. However, the way nurses construct meanings of professional respect has been neglected in the literature. This research group, therefore, sought to elucidate the significance of nursing’s professional respect perceived by nurses working in community and hospital setting in some parts of England.
Aims of the study
The aim of this study was to describe nursing’s professional respect in community and hospital settings in England from the perceptions of nurses who had been qualified for at least 1 year. These nurses were attending post-qualifying courses in two English universities.
Four interview questions were formulated to allow nurses to describe their experience of nursing’s professional respect: The concept of professional respect has received little attention and is not identified as a key nursing value. Could you describe some indicators of nursing’s professional respect in degrees of importance? Regarding moral self-respect, the American Nurses Association Code of Ethics for nurses states that ‘moral respect accords moral worth and dignity to all human beings irrespective of their moral attributes or life situation. Such respect extends to oneself as well; the same duties that we owe to others we owe to ourselves’. Have you witnessed an episode where nursing’s professional respect was violated? Have you witnessed an episode where nursing’s professional respect was regarded as an important value by other professionals working in the same context? Have you ever seen a nurse whose behaviour could be considered as lacking or reinforcing nursing’s professional respect? Have you ever witnessed a situation where the behaviour of a health professional (physiotherapist, speech therapist, radiographer, etc.), support staff or clerical staff, damaged or reinforced nursing’s professional respect? Could you give some examples?
Method
Design
A descriptive qualitative method was adopted as a research strategy. In this study, we used an inductive approach through focus group data collection to allow insights to emerge about professional milieu for nurses working in community and hospital settings.
Sample
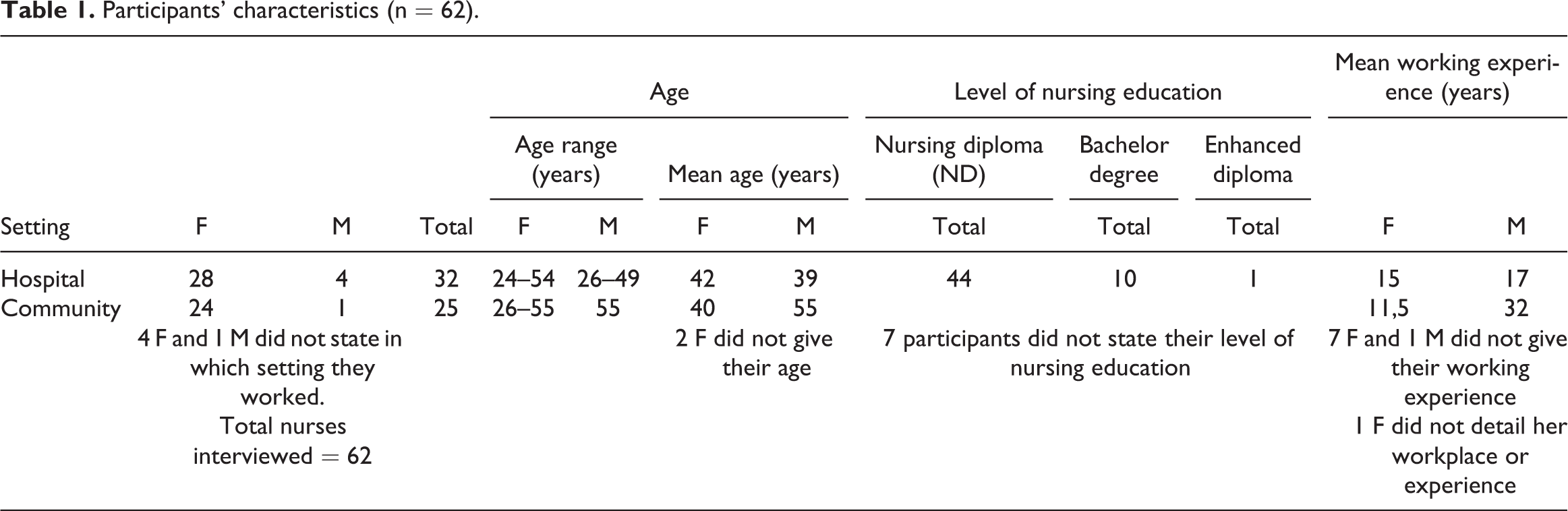
Data were collected from October 2010 to March 2013, from clinical nurses who were attending post-qualifying courses at universities in the South and the North of England through purposive, convenience, non-probability sampling. In total, 62 nurses took part in the research. In all, 25 nurses were working in the community and 32 nurses were working in hospitals. Five nurses did not declare the setting where they were practicing.
A socio-demographic data sheet was used to document basic information (Table 1).
Participants’ characteristics (n = 62).
Inclusion and exclusion criteria
Participants were selected to ensure they had relevant experience in the clinical fields under consideration. The criteria for participation were (1) clinical registered nurses and (2) working in community or in hospital settings for more than 1 year on a stable basis. Exclusion criteria were (1) being in a managerial role and (2) working in the same community district or hospital department as two or more nurses in the same focus group.
Data collection
Participants were recruited on a voluntary basis. Data were collected using 11 focus group discussions to allow interactions among the informants on this complex topic.
Although focus groups are historically rooted in the marketing sector, their efficacy in producing validated results in the nursing field is extensively documented. 45,46
Focus groups were conducted to develop a better understanding of the dynamics, experiences and values connected to nursing’s professional respect. We believed that to have a planned debate and nurses’ interactions on this specific issue could unveil important meanings and beliefs on this underexplored issue for the nursing profession.
Each focus group had between four and eight participants. 47 Potential participants were informed of the study by a detailed information sheet sent by email. Mailings were sent to nurses who expressed a wish to take part in an informal meeting held in the university classrooms where they were attending courses before the possible agreed sessions. An information sheet was also handed out during the focus group sessions. A semi-structured focus group format was employed to stimulate group debate and discussion.
Focus groups were held in dedicated lecture rooms at the universities involved and were digitally audio-recorded. At the end of each session, the lead interviewer summarized the discussion and solicited further commentary to ensure a comprehensive data collection process.
After having conducted many focus groups with nurses, who had experiences of nursing in diverse environments in England, data were saturated. Even if the concept of saturation as a quality marker for qualitative research is debatable, 48 the research group felt that the depth and the breadth of information that had been retrieved in more than 2 years could give sufficient depth of information to illuminate the topic under scrutiny.
Data analysis
The researchers decided to use an inductive approach to gain fresh insights for this study from this novel socio-cultural context. The data collected were coded using an inductive content analysis 49 extracting meaning units from the information retrieved, that is, ‘a word or short phrase that symbolically assigns a summative, salient, essence-capturing, and/or evocative attribute for a portion of language-based or visual data’ (p. 3). 50
The transcribed data consisted of 5334 lines and 137 A4 pages with 1.5 line spacing. Codes were reduced, connected together based on their similarities and differences, and abstracted into 14 main categories. Six connecting themes were identified (Figure 2).

Elements that influence nursing’s professional respect: summary of the analysis.
Immediate verbatim transcriptions were read and reread several times in order to obtain a holistic impression of the content. Checking the content was done by the members of the research team enabled identification of key concepts. During several days of research retreats in Greater Manchester, the meaning units were discussed, clarified and reconceptualized into broader categories and themes describing the characteristics of nursing professional respect in hospital and community workplaces. The meaning units reflected the nurses’ perceptions about professional respect and constituted the manifest content. The development of inferred interpretations that went beyond the content of original segments of data emerged through abstraction and were contextualized to the data. 51
Consideration of rigour
To ensure rigour in our descriptions of nurses’ experiences of professional respect, we employed the principles of credibility, dependability, confirmability and transferability developed by Lincoln and Guba. 52 Credibility was established by accurate purposive sampling of nurses and prolonged engagement in the environments considered. The meeting of the dependability criterion is always thorny in qualitative work although researchers should at least strive to enable a future investigator to repeat the study. Dependability also addresses the fact that the research context is open to change and variation. In this framework, the research group tried to connect credibility with dependability, having in mind that, ‘a demonstration of the former goes some distance in ensuring the latter’ 53 (p. 71). In this logic, dependability was assured by the stability of data collected from October 2010 to March 2013. In fact, although the collection data was carried out over a long period of time, and healthcare organizations change rapidly, the main factors that were perceived to hinder respect for the nursing profession remained stable over time. Many similarities along the period of data collection could be detected even before the in-depth analysis of data.
Confirmability, which refers to the potential congruence that data accurately represent the information that the participants provide, was accomplished through in-depth discussion among the research team. A member of the research group who had neither participated in the focus groups nor in prior analysis read the original un-coded transcripts of the focus groups to validate the results. Collecting data in two zones of England assured data transferability.
Ethics
Ethical approval was obtained from the review committees of the universities involved: approval number NMSCC/07/11/6/A from University of Hertfordshire and ethics application approval HSCR12/87 from University of Salford. Before the study, participants were advised that they were free to refuse to participate or withdraw at any time. Consent forms were signed. Nurses who participated in the study were asked to use a fictitious name in recorded sessions; participants were asked to respect the confidentiality regarding the workplace experiences of other colleagues in the focus groups. All the details relating to the participants of the study were kept in locked cabinets and all information remained anonymous.
Findings
Once the data were analysed, nurses’ perceptions of professional respect were grouped into six themes. The themes are shown graphically in Figure 3.
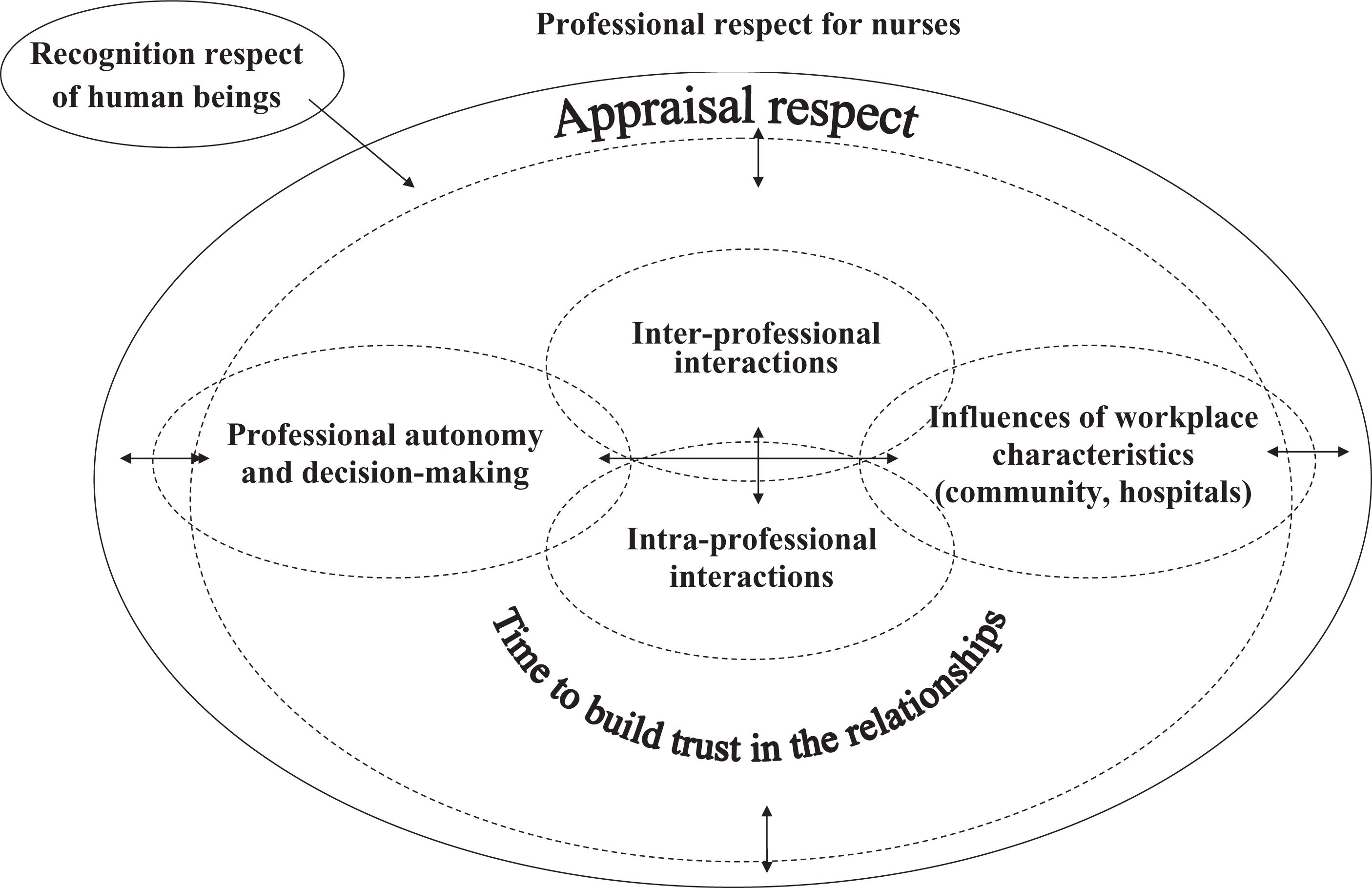
Professional respect for nurses in hospital and community settings.
The first theme was linked to: Recognition respect of human beings.
The other five themes were part of appraisal respect and were as follows: Inter-professional relationships; Intra-professional relationships; Time to build trust in the relationships; Influences of workplace characteristics (community, hospitals); Autonomy and decision-making.
The recognition respect of human beings
The first part of the concept of respect, that is, recognition respect is intrinsic to and inherent in persons irrespective of their social roles. In this sense, it is a respect based in the very internal essence of the human being that can never be lost or gained; it is simply in the essence of people as it was exemplified by this quote: Professional respect is respecting individuals in their field, whatever they do, they have to be respected whether they are on a higher or lower position, it’s about respecting everyone, whatever they do. (FG 8) Professional respect is treating people how you would expect to be treated. (FG 8) I find that I get quite a lot of respect and give a lot of respect professionally to whatever grade of staff or other allied health professionals…because everyone has their own experiences to bring and if we all work together than it’s always for the benefit of the patient. (FG 9)
Themes connected with appraisal respect
Elements of professional respect were connected with appraisal respect in the following domains: interactions among healthcare professionals, time to build trust in the relationships, the influences of the workplace characteristics (community, hospitals) and nurses’ professional autonomy and decision-making. These were described as follows:
Inter-professional relationships
Participants described a range of experiences with other healthcare staff: senior and junior doctors, general practitioners (GPs), allied health professionals and healthcare assistants.
Nurse–doctor relationships
Some participants located their experiences of working with doctors within the context of an erosion of the traditional dominance of the medical profession within the British National Health Service (NHS). One nurse stated that One time doctors did seem to be on that pedestal…now the new doctors [are] coming, I think they are much more approachable. (FG 6) There are some consultants…who are absolutely brilliant, and you can just speak quite freely…but the older chaps that I work with, you still have to make them feel like it’s their decision. (FG 10) We have a situation where the doctors are able to vent their feelings inappropriately sometimes and as a nurse, when you’ve got the patient there, you’re unable to say ‘well, that wasn’t the right thing to say’ you have to maintain a silence. (FG 6)
Nurse–GP relationships
Participants’ experiences of professional respect during interactions with GPs were diverse, yet bore some similarities to relationships with hospital doctors. For instance, the nurses’ need to develop a range of strategies to approach individual GPs was expressed in the following way by a nurse: If I have a feeling that a patient needs something specific, a patient needs a review because I feel they are in pain, it very much depends on how I approach that GP to know what the outcome would be. (FG 4) I find some of them quite disrespectful…they feel they’re entitled to ask you to do things or demand you to do things…they’d do a procedure and expect you to clear up after them. (FG 7)
Nurse–allied health professional relationships
Although some nurses expressed the opinion that nurses and allied health professionals were mutually respectful and were equivalent in terms of their role status and within the NHS, others perceived that allied health professionals located themselves in a higher stratum than nurses: Even the physios, the dieticians, when they come onto the ward they look at you as if they are higher than you. (FG 7) On the whole I find that they are respectful…but the thing I do notice is I feel they never have anything to learn from us it’s always just us that can learn from them…they don’t have an expectation that we have anything to teach them. (FG 7)
Nurse–healthcare assistant relationships
Even if some nurses reported very respectful relationships with healthcare assistants, these inter-professional interactions were perhaps the most likely to be characterized by contention and a level of disrespect towards nurses. For instance, one nurse perceived that it was … harder to get respect from the clinical support workers than it was from anyone else…you’ve kind of got to prove yourself to them to be competent, prove yourself to be assertive…there’s a kind of initiation, subtly done, but an initiation process that you go through. (FG 10) You want things done in a certain way…they think you are asking too much of them, they don’t like you, because you are checking everything to see things are done…and then they turn it round the other way that you are lazy because you always ask us to do it. (FG 6)
Intra-professional interactions
Staff shortages and high workloads seemed to create the context for resentment in intra-professional interactions when nurses were either late for shifts or unable to continue working beyond the end of their shift. For instance, a nurse commented that Everyone can have problems…but then it’s always the same people who arrive late, and they rarely apologise. (FG 3) One thing that I’ve experienced is that…we have some nurses who always manage seemingly to get off on time…and I end up staying longer…it seems very unfair. (FG 6) In front of everybody (charge nurses) will abuse…verbally: ‘that’s not how to do it’ to the new person that does something wrong. (FG 7)
Time to build trust in the relationships
Trust was perceived as an intrinsic element of professional respect by some of the participants in this study. Trust developed over time and in particular as a consequence of good nursing care. One nurse stated that The consultants, I think…get to know you, and then quickly they realize they can trust you…you’re looking after their patients, the patients are happy. (FG 6) I feel that in the community setting I had good relationships with some of the doctors I worked with for the last six years and yet some of them who I worked with over the last year, who don’t really know me, don’t show me that same respect. (FG 4)
Influences of workplaces characteristics (community, hospitals)
Nurses who had experienced working in both community and hospital environments perceived a greater degree of respect in community settings: I felt that my professional dignity or my professional opinion was much more valued in the community setting than in the hospital setting. In the community setting as nurses we work autonomously; I feel much more respected by other health professionals than I personally felt working in a hospital. (FG 4) In hospitals I felt much more that it was a hierarchical system from the dignity/respect point of view I felt that the doctors didn’t respect me as much whereas in community I feel I have earned that respect. (FG 4)
Professional autonomy and decision-making
While many participants described good working relationships between themselves and doctors it appeared that there were some tensions around autonomy and decision-making processes. This experience was perhaps best described by a nurse who affirmed that You (as a nurse) are autonomous to an extent…the doctors, when they come, they just take over, and when they are away you carry on as an autonomous practitioner. (FG 7) If you see a patient deteriorating, I will do certain things myself before I even ring the team…quite often I…wait that extra hour to confirm, because they’re just going to say ‘do it again in half an hour’. What’s the point? I know what to do, I know what I’m looking for. (FG 6)
Discussion
This study provided insights into understanding nursing’s professional respect in community and hospital environments in England and enabled key perceptions of it to be described. The construct examined was embedded in the innermost part of individuals, which is where the basis of respect for every person resides according to many scholars. 54,55
The authentic respect comes from recognition in persons and in their inner essence as persons and this tenet was clear in the perceptions of the nurses interviewed. In this connection, we can notice the strict interweave between intrinsic dignity of human beings and the recognition respect embedded in every individual. 25 In the context of recognition respect, social rank and position of individuals are irrelevant. Valuing persons in their inner aspects is at the core of respect for all persons as persons. This conceptualization, often referred to as the Golden Rule, 56 bears strong similarity to Darwall’s notion of recognition respect, as it would apply to all persons regardless of acquaintance, attainment, expertise or role status.
Concerning appraisal respect, 25 an extrinsic respect for the qualities of other individuals – generated asymmetrically in the relationships among persons – was thought to be deeply enshrined in the relationships among healthcare professionals. These interactions qualified the respect for nurses. In fact, it was during these interactions between nurses and other healthcare professionals, primarily physicians, that the respect was defined, could be lost or violated, or possibly never recognized. This was decisive because the realization of the appraisal respect for nurses was clearly figured out so as not to dismiss others or to ignore others or to keep distance in virtue of a superior rank, or to objectify others who were regarded just for their usefulness and not as ends in themselves.
Therefore, to overcome this dearth of respect, a crucial factor for nurses was the forging of trusting relationships over time. With stable relationships created and sustained over years, even rude interactions could become more symmetric. The recognition of appraisal respect took place when the job strain and the burdens of patient care were well managed by all the staff and when the environments (either hospital or community) supported real interdisciplinary teamwork. 57 Equally essential were the relationships with nurse managers that were often perceived as unsupportive in the context of the high levels of stress experienced by nurses. Last but not least, the possibility to express autonomy and decision-making without being constrained by rigid disciplinary boundaries, especially with physicians, was deemed decisive to obtain nursing’s professional respect.
Inter-professional interactions and intra-professional interactions
Verbal abuse is the most common form of disruptive behaviour experienced by nurses worldwide and in any setting. 58,59 In our study, physicians, especially some senior consultants, were a predominant source of verbal abuse, in particular in hospitals. 60,61 In fact, in a few cases they reprimanded nurses in front of everybody, used top-down communication exemplifying the asymmetry of disrespectful interactions, showed undermining behaviours and sometimes intimidated nurses. Luckily, this was not common and was observed especially by nurses working in particularly stressful hierarchical hospital environments, while in the community settings the inter-professional relationships were based more on mutual respect although a few interactions, especially with GPs, were problematic.
Regarding intra-professional relationships, for example, horizontal violence, peer hostility, bullying, many studies have detailed destructive activities in health settings. 11,62 In our study, nurse–nurse relationships were mostly described as relationships of collaboration but, unfortunately, were also very problematic for different reasons: punctuality during shift change; lack of collaboration during high demand work shifts or in stressful environments; or in difficult to manage situations. A lot of nurses complained about a gossipy attitude that characterized many hospital and community environments where peers were used to criticism and back-stabbing. Nurse managers were often accused of a lack of responsiveness towards nurses and were often not willing to listen to and recognize nurses’ concerns. Although nurse leaders have crucial roles in improving the organizational climate for nurses, they were often perceived as not committed enough to initiating change in challenging work environments.
Time to build trust in the relationships
Trust is a decisive moral value of human beings that underpins the way healthcare professionals engage with one another and lies at the heart of appraisal respect. Mutual respect has to be built on relationships of honesty and trust, especially if there are power differentials between persons and disciplines. 63 However, generating and maintaining relationships of deep mutual trust needs time, because people have to get to know each other. This was one of the main attributes stressed by nurses when they experienced difficult relationships with other healthcare professionals or with patients. In fact, physicians tended not to trust newly qualified nurses or nurses just arrived in a new setting and this reproduced the difficulties encountered by newly graduated nurses in many settings and in many research studies. 64,65
Influences of workplaces characteristics (community, hospitals)
Hierarchical boundaries, heavy workloads, lack of support by managers and lack of possibility to have enough breaks during the shift work were present in healthcare facilities and diminished the professional respect perceived by nurses themselves. Fortuitously, this was not common, because the nurses perceived that the old organizational culture based on the biomedical model had been declining in recent years. However, elements of this old culture were still strongly present in some workplaces, especially in healthcare organizations and in particular in demanding environments. In community environments, nurses reported enjoying substantial levels of respect especially when they had prior experience of working in hospitals. However, relationships with GPs were sometimes more complex and gaining their trust was perceived to be less straightforward.
Professional autonomy and decision-making
Autonomy and shared decision-making approaches are key elements to express professionalism. 66 Professional autonomy is the ‘freedom to make discretionary and binding decisions consistent with one’s scope of practice and freedom to act on those decisions’ 66 (p. 15) and can be defined as ‘an independent and interdependent practice-related decision-making based on a complex body of knowledge and skill’ 67 (p. 26). Professional autonomy is evident through communication of reciprocal respect in professional relationships. 68
Problems with nurses’ claims to professionalism in the context of medical domination were clearly articulated by Freidson 69 who suggested that simply meeting ‘criteria’ such as codes of conduct and advanced training would never meet the need. He argued that professionalism is only obtained when an occupation attains complete freedom from control of work by others, that is, ‘legitimate organized autonomy’.
Nurses in our research sometimes perceived that their autonomy and decision-making processes were restrained by rigid barriers with other professions, especially medicine. The moral suffering of many nurses, especially those working in hospitals, was linked to the devaluation of decision-making approaches and professional autonomy. In the community setting, the situation was different, with nurses often emphasizing that they were satisfied to have the chance to put in practice professional autonomy and the possibility to express themselves within the context of a shared decision-making approach.
Expressions of professional respect for nurses in hospital and community environments: commonalities and differences
Commonalities
Nursing’s professional respect was emphasized by the interviewees both in hospital and community settings through teamwork. The concept of working in closely knit teams was always present in the minds of nurses, but its application in practice was very difficult and many times there was not a real interdisciplinary teamwork, especially between doctors and nurses in hospitals in high stressful units. 70
Another element of commonality among nurses was that the role of nurse leaders was ineffective in promoting change in the organizational climate or to listening to the concerns of nurses themselves. Nurse managers rarely or never praised the good work done by nurses and this did not foster respectful working environments and did not promote better cooperation among the members of staff. 71
Differences
One of the decisive differences that came to light was that the concept of respect in inter-professional relationships with consultants was more common in community districts with GPs than in hospitals in high demand context-units. The organizational elements of the hospitals’ workplaces, such as the strain of work shift, work overload and poor nurse ratios, were thought to be pivotal in improving nurses’ respect as persons and professionals and avoiding verbal abuse from physicians. These results were totally consistent with the findings reported by Mihyun Park et al. 72,73 in South Korea.
Autonomy and decision-making were more present in community environments. However, the nurses working in community settings also complained about discrimination compared with specialist nurses, who they thought, had a higher level of autonomy and better extrinsic values, such as a higher income.
Limitations and strength of the study
Several potential biases could be detected in the preparation, organization and reporting phases of this research. 74 For example, in the preparation stage, the researchers did not reflect enough on the utilization of focus groups as the only method to collect data. Single interviews or mixed methods could have elicited deeper perceptions on the topic. In the organization phase, during the analysis of raw data, the rich description of the meaning units was not displayed graphically and hence not reported in this article.
In the reporting phase, not all similarities and differences among the setting examined were compared with other studies carried out in other countries because of the intrinsic socio-historical complexities that characterize each and every context.
We are aware that theory and empirical data are related in different ways. One of the strengths of this study was, hence, to clearly address the theoretical link with empirical data. In fact, in agreement with Bradbury-Jones et al. 75 typology of theoretical visibility, theory was ‘consistently applied’ rather than anticipating the data collection or arising wholly out of it.
Conclusion and recommendations to take forward
Nursing’s professional respect is embedded in nurses as persons and as workers. When nurses are engaged in their clinical activities, inter- and intra-professional interactions are pivotal to qualifying the respect of other occupations for them. These relationships have to be based on mutual respect 76 and concerning different healthcare disciplines, on overcoming the cultural boundaries, especially between nurses and physicians, 77,78 that are experienced globally in relation to the impact on the quality of patient care. 79,80 Regarding specifically intra-professional interactions, these have to be based on the comprehension of the changes of the healthcare macro-systems and the ageing population. These global issues demand new responsibilities among nurses in different functions. In this sense, the role of nurse leaders is fundamental. They have to behave as role models for all the staff and strongly support ethical nursing practice.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from the Centre of Excellence for Nursing Scholarship in Italy (Research Grant number 2.10.03).