
Abstract
Background:
An ethical climate has been described as a working climate embracing shared perceptions about morally correct behaviour concerning ethical issues. Various ethical climate questionnaires have been developed and validated for different contexts, but no questionnaire has been found concerning the ethical climate from an inter-professional perspective in a healthcare context. The Swedish Ethical Climate Questionnaire, based on Habermas’ four requirements for a democratic dialogue, attempts to assess and measure the ethical climate at various inter-professional workplaces. This study aimed to present the construction of and to test the psychometric properties of the Swedish Ethical Climate Questionnaire.
Method:
An expert group of six researchers, skilled in ethics, evaluated the content validity. The questionnaire was tested among 355 healthcare workers at three hospitals in Sweden. A parallel analysis (PA), an exploratory factor analysis and confirmatory factor analysis were performed.
Ethical considerations:
The participants included in the psychometric analysis were informed about the study, asked to participate in person and informed that they could withdraw at any time without giving any reason. They were also assured of confidentiality in the reporting of the results.
Findings:
The parallel analysis (PA) recommended one factor as a solution. The initial exploratory factor analysis with a four-factor solution showed low concordance with a four-factor model. Cronbach’s alpha varied from 0.75 to 0.82; however, since two factors only consisted of one item, alpha could not be reported. Cronbach’s alpha for the entire scale showed good homogeneity (α = 0.86). A confirmatory factory analysis was carried out based on the four requirements and showed a goodness-of-fit after deleting two items. After deletion of these items, Cronbach’s alpha was 0.82.
Discussion:
Based on the exploratory factor analysis, we suggest that the scale should be treated as a one-factor model. The result indicates that the instrument is unidimensional and assesses ethical climate as a whole.
Conclusion:
After testing the Swedish Ethical Climate Questionnaire, we found support for the validity and reliability of the instrument. We found the 10-item version of Swedish Ethical Climate Questionnaire satisfactory. However, we found no support for measuring different dimensions and, therefore, this instrument should be seen as assessing ethical climate as of whole.
Introduction
Ethical climate has been defined as a form of working climate that embraces shared perceptions about what constitutes the correct behaviour, which in turn influences ways ethical issues and decision-making are handled. 1 Ethically difficult care situations challenge moral values and sometimes lead to consequences such as feelings of uncertainty, loneliness and powerlessness. 2 –4 To date, only a few ethical climate scales applicable to healthcare workers have been developed, mainly investigating nurses’ perceptions. 5 This study reports the construction and validation of an inter-professional ethical climate scale, based on Habermas’ theory of communicative actions.
Ethical climate has been described in various contexts, for instance, in business and trade, 6,7 leadership–employee relations, 8 organizational characters 9 and in the context of resource management. 10 The ethical climate has been described as a form of the organization’s working climate and concerns how codes of ethics, perceptions of norms and policies influence employees’ ethical behaviour. 1,9 Silverman 11 defines ethical climate as shared understandings and perceptions of certain values. Studies show a positive relation between the organization and the leadership’s perception of ethical climate and the employees’ ethical behaviour. 1,8,12 Martin and Cullen, 1 have developed an ethical climate model, built on the ethics of utilitarianism and deontology, related to the dimensions of egoism, benevolence and principle. In a healthcare context, the ethical climate is described by Olson, 5,13 as shared values, perceptions and decisions in the relations among healthcare professions, patients, managers and organizations and a mutual respect concerning ethical issues. In a study by Silén et al. 14 Resident nurses (RNs) described an ethical climate as positive if they were able to meet the patients’ needs and Hart 15 showed that ethical climate was one important factor in RNs remaining in their positions.
Ethical climate is a complex and subtle phenomenon as the clinical work with patients and their families involves a number of professionals. According to Jameton, 16 each professional group has its own identity and codes of ethics and meets patients in different situations or contexts. In studies by Grönlund 4,17 nurses and physicians have described ethical difficulties in the same situations but from different perspectives. They reported difficulties in communicating their concerns and expressed a need to achieve a broader understanding of the situation. Similar results are reported by Silén et al., 14 who described inter-professional collaborations and shared responsibility as a prerequisite for a positive ethical climate, which has proved to be a problem due to a lack of mutual understanding among the professional groups. 4
Efforts have been made to develop various forms of clinical ethical support (CES) in order to increase understanding of what constitutes ethical practice. A compilation of the documented effects of CES shows a complex and wide range of knowledge and skills. 18 The difficulties in evaluating CES seem to stem both from the fact that participants are not always aware of all aspects of the skills and knowledge they practice and provide and from the lack of suitable instruments. Weidema et al., 19 however, showed that inter-professional communication in CES promoted increased inter-professional collaboration, reflection and shared perceptions that led to the breaking of unethical habits. Grönlund et al. 20 carried out a series of CES interventions, inspired by Habermas’ theory of communicative actions, and showed that during the process the participants’ language successively changed from expressions of frustration and individual understandings to wider views and the achievement of a common understanding of the situation. Previous studies (Grönlund et al. 4,17 ), however, show that it was difficult to discuss ethical problems between different healthcare professional groups because of the variety of perspectives. We, therefore, looked for a model that could promote dialogue among different professional groups with varying perspectives on the situation. Habermas et al.’s 21 four requirements for a democratic dialogue seemed to meet this criterion.
In Habermas et al.’s 21 theory, communicative actions mean maintaining a democratic dialogue to achieve new and common knowledge built on a common consensual understanding of the issue of concern. This communication approach implies revealing the problem and moving on towards recognizing common values. The prerequisite for such an approach is openness, which means that side effects, any consequences of validity claims and suggestions need to be presented, revalidated, clarified and accepted by all those concerned. 22 Communicative actions require equality among the participants to be maintained so that all can feel free to express themselves and are met with respect. 21 Grönlund et al. 20 showed that a permissive communication climate is an essential prerequisite for dialogue in the CES intervention. The results of this study motivated further investigations concerning how relations between inter-professional communications can open a pathway for establishing an ethical climate, in line with Habermas’ theory of communicative actions. Already existing ethical climate scales are adapted to various contexts. Within the business and trade sectors, a theory-based ethical climate questionnaire developed 6 and used by Engelbrecht et al. 12 was modified and adapted to a caring context by Tsai and Huang. 23 Other scales investigate how individuals’ perceptions of values, norms and procedures govern their decisions, 24 recognition of ethical issues and maintenance of ethical standards 8 . Trevino 10 combined ethical climate and ethical culture issues and Bartells 9 studied employees’ ethical conduct in relation to the character of the organization they work in.
All the ethical climate scales mentioned above investigate how the leadership, organization and workplace culture are related to the perception of the ethical climate and the employees’ ethical conduct. Within the healthcare context, a Hospital Ethics Climate Survey (HECS) was developed and validated by Olson 5,13 concerning nurses’ relationships with peers, patients, managers, physicians and the hospital. The HECS is aimed at nurses and has been used to investigate nurses’ perceptions of the ethical climate in clinical practice. 25 However, in the healthcare context, there are several professional specialities involved in patient care. 26 According to Höglund, 27 it is important to involve the various professional groups in a democratic dialogue concerning ethically difficult care situations, in order to promote shared perspectives and allow the making of well-founded decisions. Such a dialogue can be based on the theory of communicative action and discourse ethics. 28 In the theory of communicative action, four principles underpin an ideal dialogue situation, namely: equality, review, openness and the will to reach a reflective consensus.
According to Habermas et al., 21 ‘Equality’ means that all the participants in a discourse should have the ability to communicate by freely initiating, debating, asking and answering questions. ‘Review’ means that all participants should have the ability to interpret, state, propose, argue and problematize or refute all claims for validity, so that no preconceived opinions evade criticism. In a process using arguments, motives and counterarguments the validity of aspects and statements may be validated. 21,22 ‘Openness’ means that access is given to all equally to express their views through statements that are truthful, sincere, valid and comprehensible. This freedom is important because it alone can ensure that the participants are both true to themselves and are prepared to reconsider their standpoints. 21 Finally, ‘Consensus’ means that everyone who participates should be willing to seek solutions that most can accept. 21 These requirements form the starting point for Habermas and colleagues 21,22 version of discourse ethics, focusing on the communication procedure that leads to reasonable ethical norms and a morally correct act that can be accepted by those involved. This procedure is in itself normative, as it is based on the principle of human dignity, equality and openness.
Because ethical climate is a complex and subtle phenomenon, the question is how can changes in the ethical climate at a workplace be assessed and measured. Our own experiences of working as a clinical ethics support group suggest that the ethical climate comprises almost the same four aspects or prerequisites as Jürgen Habermas’ four requirements for democratic dialogue. Since we were unable to find any instrument for assessing an ethical climate with an inter-professional focus, an ethical climate scale based on Habermas’ theory of communicative actions was developed.
This study aimed to present the construction of and test the psychometric properties of the Swedish Ethical Climate Questionnaire (SwECQ).
Development of the Swedish Ethical Climate Questionnaire (SwECQ)
Item development
The SwECQ was constructed using Habermas’s 21 four requirements for a democratic dialogue as a starting point/base for the items. Possible items were brainstormed, suggested and formulated within the research team. The items were then condensed into three questions related to each of Habermas’ four requirements for a democratic dialogue. The research team then examined and further revised the items.
The final version of the SwECQ comprises 12 items answered on a six-point scale (‘Not at all’ to ‘To a large extent’.) One of the items (item 12) is inverted. A total score is calculated by adding items 1–11 and the inverted item 12.
Item validation
Content validity on item (I-CVI) and scale level (S-CVI) were first tested by ethical agents within the various healthcare professions, such as registered nurses, enrolled nurses, physicians, physiotherapists and occupational therapists. After participating in clinical ethics support sessions, these professionals answered the questionnaire and wrote comments and suggestions. After some minor adjustments to the statements, a panel of six experts represented by one professor emerita, two professors and three senior lecturers with expertise in the areas of ethics and scale development were consulted in order to evaluate the content validity of the items 29 The expert panel represented the following professional areas: ethics/philosophy, physiotherapy, psychology, nursing, psychiatry and anaesthesia. For each item, they were asked to assess its relevance for the ethical climate according to the following alternatives: ‘Not relevant’, ‘less relevant’, ‘quite relevant’ and ‘very relevant’. The percentage of items deemed to be relevant for each expert was computed, and an average of the percentages across the experts was calculated. 29 A first version of the items showed a low Content Validity Index (S-CVI = 0.68). After rewording some of the items, the S-CVI increased to 0.88 with an I-CVI ranging from 0.8 to 1.0. Items 1 and 6, respectively, can serve as examples of rewording; from ‘Can you start a discussion about difficult situations at your workplace?’ to ‘Do you support each other in difficult situations at your workplace?’; and from ‘Do people take time to discuss difficult / sensitive topics in your workplace?’ to ‘Do you take the time to discuss difficult or sensitive topics at your workplace?’
Procedure
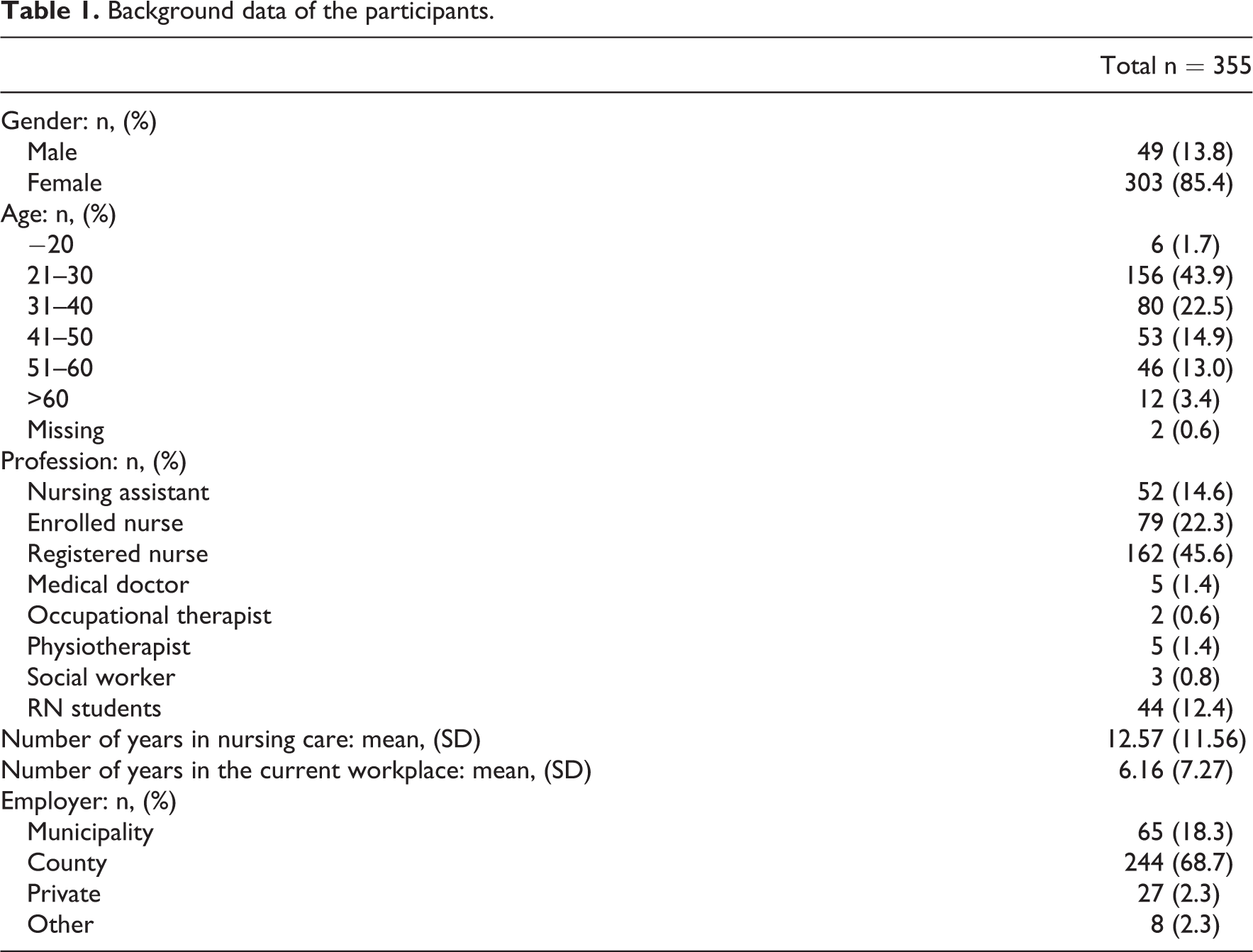
The final version of SwECQ was tested by a convenience sample of various groups of healthcare workers (n = 355), comprising 162 (46%) nurses, 79 (22.4%) enrolled nurses and 52 (14.8%) care assistants. The remaining 62 (16.8) participants were medical doctors, physiotherapists, occupational therapists and others. The participants were recruited from the northern, central and southern parts of Sweden to obtain maximum variation 30 (Table 1). This design provided a subject-to-item ratio of 29:1, well over the recommended 20:1 criterion. 31
Background data of the participants.
Statistical analysis
An initial analysis included assessment of the distributional properties of each item (i.e. distribution in per cent, skewness and kurtosis for each item). A parallel analysis (PA) was performed to determine the number of common factors in the SwECQ 32 Exploratory factor analysis (EFA) was used to explore the underlying structure of the 12-item SwECQ while confirmatory factor analysis (CFA) was performed to evaluate the model fit.
In the EFA, the factors were extracted based on eigenvalues greater than 1, using principal axis factoring as the extraction method, with direct oblimin rotation. 31 The extraction method was chosen because it was assumed that the data would not be normally distributed; direct oblimin rotation was chosen since the factors were expected to correlate with each other. Deletion of items from the 12-item SwECQ was performed based on the model fit in the CFA. Two items were deleted because it was not possible to obtain an acceptable goodness-of-fit in the CFA. Statistics used to assess goodness-of-fit were chi-square (χ2) and chi-square/degrees of freedom (χ2/df), the Tucker–Lewis index (TLI), normed fit index (NFI), comparative fit index (CFI) and root mean square error of approximation (RMSEA). Internal consistency was estimated by Cronbach’s alpha.
SPSS version 23.0 and AMOS version 23.0 (SPSS Inc., Chicago, IL, USA) statistical software packages were used for the statistical analyses. parallel analysis (PA) was performed using FACTOR version 8.02 (Rovira i Virgili University, Tarragona, Spain).
Ethical considerations
Those included in the psychometric analysis were informed about the study, asked in person to participate, informed that they could withdraw at any time without giving a reason and were assured of confidentiality throughout. According to the Swedish Act concerning ethics in research, 33 this analysis, which is an analysis of the psychometrics of the instrument, does not require its own specific ethical approval.
Result
An initial analysis of the distribution of responses showed moderate skewness in some items. However, all skewness was below 1.0. The number of missing items was low (Table 2).
Median and distribution in per cent for each item and response alternatives of the Swedish Ethical Climate Questionnaire (SwECQ). English version in plain text, Swedish in italics.
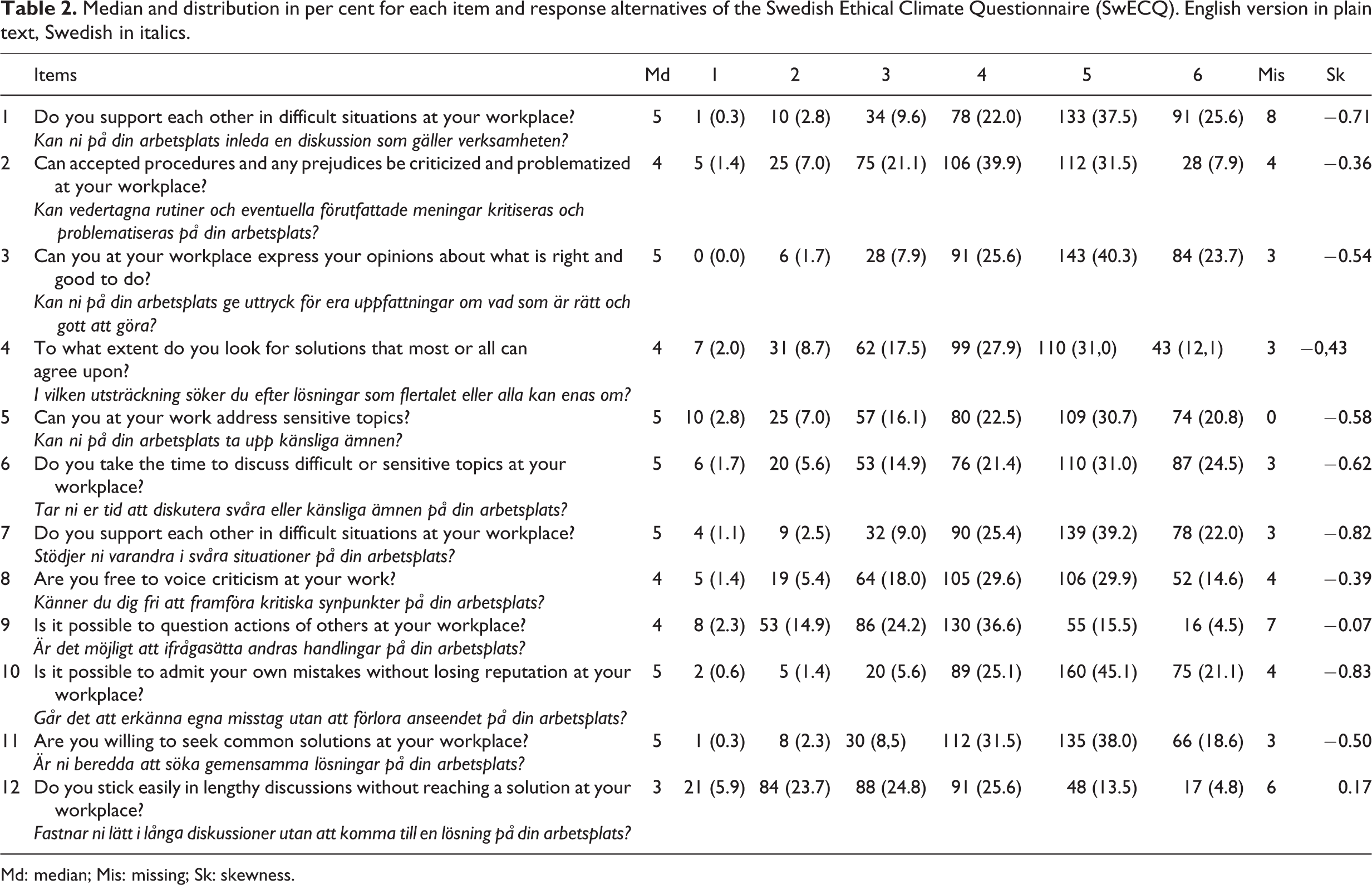
Md: median; Mis: missing; Sk: skewness.
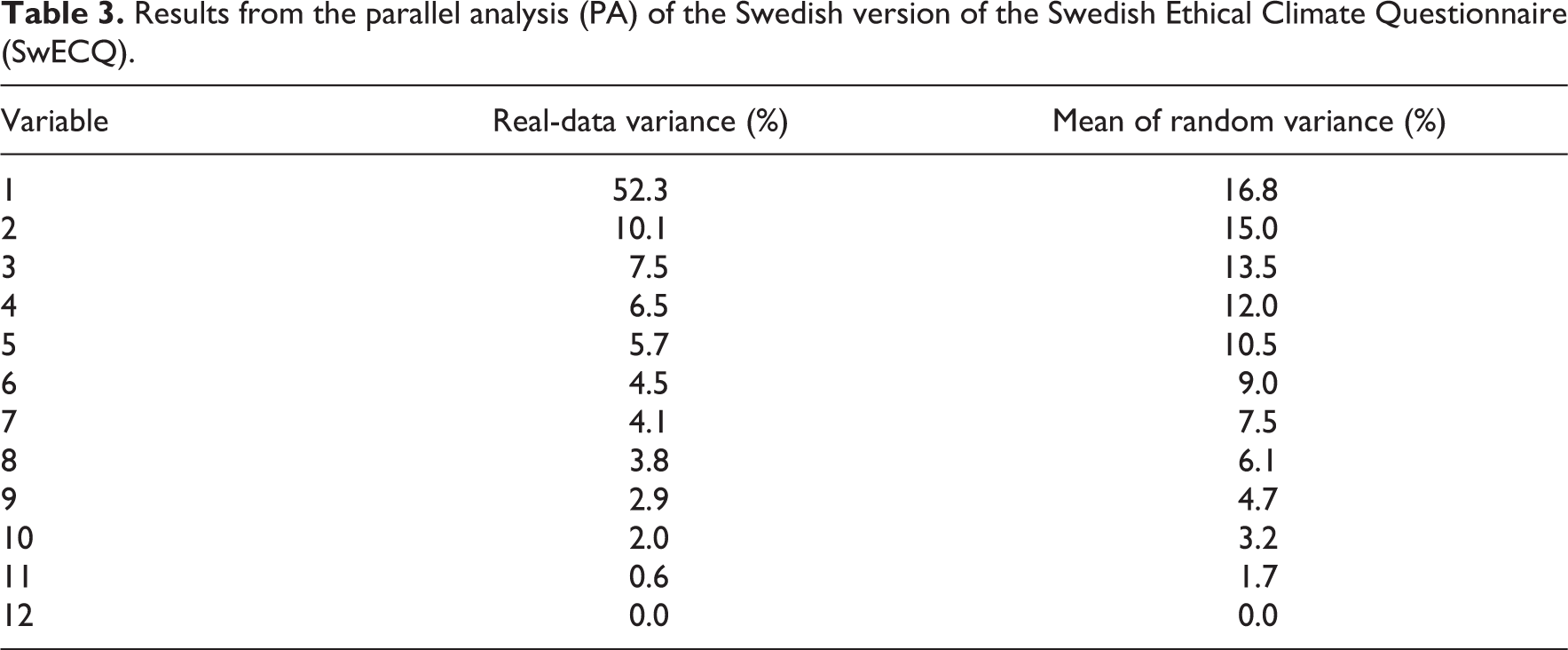
A parallel analysis (PA) based on minimum rank factor analysis was carried out to determine the minimum number of factors in the SwECQ. The result shows that the recommended number of factors was one (Figure 1; Table 3).

Scree plot of parallel analysis (PA) of the Swedish version of the Swedish Ethical Climate Questionnaire (SwECQ).
Results from the parallel analysis (PA) of the Swedish version of the Swedish Ethical Climate Questionnaire (SwECQ).
An initial EFA showed a model where two factors had eigenvalues of 1 or more. However, there were multiple crossovers between the factors where only one item loaded on one factor. A second EFA, forced into a four-factor model, showed low concordance since one factor included only one item and another only two items. Furthermore, there were some crossover charges between the factors (Table 4). Cronbach’s alpha varied from 0.75 to 0.82, however; since two factors consisted only of one item, alpha could not be reported. Cronbach’s alpha for the entire scale showed good homogeneity (α = 0.86).
Items, factor loadings, total variance explained, Cronbach’s alpha and content validity index on item and scale level for the four-factor structure of the Swedish Ethical Climate Questionnaire (SwECQ).

X: items deleted in the SwECQ.
CFA was performed on the final version to test its goodness-of-fit. After deleting two items (items 2 and 4), the chi-square was significant (p < 0.001); however, the relative chi-square (χ2/df), applied to make a test less dependent on sample size, was 3.07. The TLI was 0.92, NFI was 0.93, CFI was 0.95 and exceeded the necessary 0.9 for acceptable model fit; and, finally, RMSEA was 0.08. The final model is shown in Figure 2, including the path coefficients (standardized regression weights and correlations). Correlations between the factors were in the interval of –0.05 to 0.56, with the highest correlation between ‘Review’ and ‘Equality’. All of the path coefficients were significant at the p < 0.001 level. After deleting items 2 and 4, Cronbach’s alpha was 0.82.

Model of the final 10-item SwECQ with standardized regression weights and correlations.
Discussion
This study aimed to present the construction of and test the psychometric properties of the SwECQ.
Six experts in the field assessed content validity. According to Polit and Beck, 34 standard acceptability for S-CVI is 0.80, while Waltz et al. 35 argue that S-CVI should be 0.90 or higher. The S-CVI for the SwECQ was 0.88, which could be seen as acceptable.
The variation between the different response alternatives showed that the median response was at the higher end of the scale. However, skewness was below 1.0, indicating that the distribution was only moderately skewed.
The parallel analysis (PA) suggested a one-factor solution. However, Hayton et al. 36 argue that in some situations parallel analysis (PA) can under-factor. One of these situations is when there is a high correlation between factors, as in this case.
The reliability of the EFA four-factor model was quite low since one factor loaded with only one item and for another factor one item loaded under 0.3. Based on an EFA, we suggest that the scale should preferably be treated as a one-factor model. This indicates that the instrument is unidimensional and only assesses ethical climate and not the subscales: ‘Equality’, ‘Review’, ‘Consensus’ and ‘Openness’.
The goodness-of-fit (TLI, NFI, CFI and RMSEA) in the CFA was acceptable. However, the result of the chi-square test was high and showed a significant p value, which is non-preferable. However, since the chi-square test is sensitive to sample size 37 and this study had a large sample (n = 355), we did not expect a non-significant chi-square value. The relative chi-square was 3.4, that is, well within the recommended range of 2.0–5.0. 36,38
Our result shows that we had relatively few missing items in the SwECQ, possibly indicating that the respondents did not find the questions difficult to answer.
In this study, SwECQ was validated as a theory-based instrument for investigating how healthcare professionals perceive the ethical climate in their everyday clinical practice. The use of SwECQ allows the possibility of assessing interventions related to communicative actions among healthcare professionals by means of measuring the ethical climate before and after a problematic situation. Silverman 11 believes that open inter-relationships and communications among employees are an essential part of an ethical climate. According to Brinkmann and Ims 39 the motivation for having an ethical climate may vary and therefore needs to be re-evaluated. In an ethical discourse the participants can revalue their standpoints and discover what norms and interests are morally accepted. This can be seen in relation to Habermas and colleagues, 21,22 arguing that through communicative actions we may test our inter-subjective viewpoints in relation to those of others and then further re-evaluate our own standpoints in relation to their inconsistencies. These various standpoints form the basis for a new knowledge and common understanding of the situation. We argue that the SwECQ instrument functions as an important cornerstone in assessing how professionals, that is, healthcare professionals, experience an ethical climate. Furthermore, this knowledge may inspire insights among the professionals concerning how to promote an ethical climate in the workplace, especially when it comes to dealing with ethically difficult situations.
Methodological discussion
One strength of our study is that we have tested the instrument in different groups of people. As we wanted to discover whether it can be used in different groups and contexts, we decided to use a diverse sample since validity and reliability aspects can be new for each setting and different groups. However, since the participants in this study were not only basic caring staff but also paramedical personnel who have a consultative status and are not constricted to one workplace/ward, the participant selection may have affected the results because of the different perspectives they brought to bear when responding to the instrument. Nevertheless, these staff are a part of the organization and, in our view, also part of the ethical climate. Furthermore, this sample mirrors a diverse population comprising people from both sexes, of various ages, with various educations and backgrounds – characteristics that we see as strengths in a study aiming to test the psychometric properties of a questionnaire. Further studies in various contexts are recommended in order to evaluate the validity of the instrument in other professions involving caring for people with various needs.
One weakness in this study is that both the EFA and the CFA was performed using the same dataset. This is unfortunate, but our sample was considered to be too small for a split half. Nevertheless, this is something that has to be done in future research. We also performed the CFA in order to confirm our hypothesis that this instrument is able to capture different domains in the ethical climate. When carrying out the CFA, we found that goodness-of-fit was not acceptable unless two items were deleted. Hence, this instrument has to be tested further in order to determine whether the four different domains can be assessed.
Conclusion and relevance for clinical practice
We found this instrument suitable for identifying an ethical climate. After testing the SwECQ, we found support for the validity and reliability of the instrument and that the revised 10-item version is satisfactory. However, we found only weak support for measurement of the different dimensions and we, therefore, recommend that this instrument should be deemed to assess ethical climate as of whole. Since Habermas stresses the argumentation process as a way of testing the validity claims of various statements, further development of the instrument should include items concerning this process. Furthermore, it would also be of interest to develop an instrument focusing on the views of patients and stakeholders about the ethical climate.
Footnotes
Acknowledgements
The authors would especially like to thank the participants for their contribution to the study. Study design: U.I., A.S. and V.D.; data collection: A.S., U.I., C.F.G. and V.D.; data analysis: U.I. and manuscript preparation: U.I., C.F.G., L.A., A.S. and V.D.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Department of Nursing at Umeå University, Sweden.