
Abstract
Background:
It is stated that high ethical sensitivity positively affects the quality of nursing care. However, the relationship between nursing care quality and ethical sensitivity has not been clearly demonstrated in researches.
Aim:
This study was carried out to determine the relationship between surgical nurses’ care behaviors and their ethical sensitivity.
Method:
The sample of this cross-sectional, descriptive-correlational study consists of 308 nurses who worked at the surgical departments in four Turkish hospitals. The data were collected using the “Nurse Description Form” developed by the researcher, “Caring Behaviours Inventory-24” and “Ethical Sensitivity Questionnaire.” Data were evaluated by the Mann Whitney U test, Kruskal Wallis one-way analysis of variance and Spearman correlation analysis.
Ethical considerations:
The study was approved by the ethics committee. Verbal and written consent was received from the nurses.
Results:
It was found in the study that nurses’ Caring Behaviours Inventory-24 total score median was 5.25 (4.83–5.58), nurses’ perception level of caring quality was high, median of Ethical Sensitivity Questionnaire total score was 89.00 (75.00–101.00) and nurses’ ethical sensitivity was moderate. A negative significant relation was found between nurses’ Caring Behaviours Inventory-24 total score and Ethical Sensitivity Questionnaire total score (r = -0.162; p = 0.009). A negative relation was also detected between nurses’ working period at the current clinic and providing benefit (r = -0.147; p = 0.012), holistic approach (r = -0.139; p = 0.018) and orientation (r = -0.175; p = 0.003) scores of Ethical Sensitivity Questionnaire sub-scales.
Conclusion:
Nurses’ perception levels of caring quality were high and their ethical sensitivity levels were moderate. It was found out that nurses’ ethical sensitivity increased together with their perception of caring quality, and as their working period at the current clinic increased, the ethical sensitivity also increased in terms of the sub-scales of providing benefit, holistic approach, and orientation. The factors that adversely affect the quality of nursing care and ethical sensitivity should be examined and attempts should be made to improve the working environment.
Introduction
Ethics concerns what should be done and what to avoid. In relation to care and medical interventions, this concerns what is beneficial for patients and this is particularly important in relation to surgery. 1,2 Since the individuals, who will undergo surgical intervention, will experience anesthesia, the advocacy role of the nurse comes to the forefront in this period. 2 It is also very important to obtain the informed consent of the patient in the surgical units, where an invasive procedure is the main concern, and the ethical responsibility of the nurse in this regard is to ensure that patients understand the procedure after they have been informed about the surgical treatment. Within the scope of ethical principles, it is also the responsibility of nurses to ensure confidentiality when patients fail to maintain their privacy, depending on their consciousness, during the surgical preparation period, during the procedure and in the recovery unit. 3
The therapeutic nature of the nurse–patient relationship is based on care ethics. Florence Nightingale envisioned nursing, as an art and science, to be a blend of humanist, compassionate, evidence-based knowledge and excellent skills. Nursing uses the concept of ethics to standardize moral accountability for nursing care practices. It is stated that nurses who apply care practices together with moral integrity feel also stronger because they are consistent in their work. 4
Ethical problems arise in surgical units, since nurses and the patients at the surgical units bear high risks of injury, infection and encountering hazardous substances, and unexpected and life-threatening situations require quick decision making. In cases, where ethical problems arise, nurses need to have improved ethical sensitivity in order to provide an ethical decision-making. 5,6
Ethical sensitivity is the method and skill that the healthcare professionals employ in order to provide compassionate care for the patients and to understand them. Ethical sensitivity is the professional aspect of moral sensitivity. 7 Moral sensitivity, on the other hand, is the ability to detect an ethical problem and to understand the ethical consequences of a decision made on behalf of the patient. 8 A high ethical sensitivity contributes to vocational professionalism as well as it directly affects the quality of the nursing care, which will be provided for the patients. 5,9,10 In the integrative review by Milliken, 11 where nurses’ ethical sensitivity was examined, it was emphasized that lacking or decreasing the ethical sensitivity of the nurses could result in care, which is inconsistent with the vocational responsibility and unethical.
It was stated that determining the nurses’ attitudes and behaviors toward the ethical sensitivity, which is an important component of the quality nursing care in professional nursing practices, can contribute to the identification of the needs and errors on this matter and to take the necessary measures, and can also help the perception levels of the nurses to increase and will consequently improve the provided nursing care quality. 12,13
Nurses, which constitute a large part of the health care service, also play an important role in the quality of health care.
14
It was reported in the studies that the ethical sensitivity of the nurses affects directly the quality of the care.
14,15
Plenty of studies examining nurses’ ethical sensitivity levels
2,11,15
–20
and reporting that an improved ethical sensitivity also improves the vocational professionalism and the quality of nursing care
5,9,13
appear in the literature. However, the number of studies examining the ethical sensitivity levels of the nurses, who work at surgical units where ethical problems arise frequently
2,19
and the studies examining the relationship between the ethical sensitivity levels of the nurses and their perception of caring quality
15,21
is very scarce. In addition, in most of the studies, we encounter the suggestion that this relationship isn’t clear and therefore should be further investigated/qualified.
21
When related studies are taken into consideration, this study will also make an important contribution to the ethical sensitivity of the nurses and its effect on nursing care. Hence, this study was planned with the aim of revealing the relationship between the ethical sensitivity levels of the surgical nurses and their perception of nursing care quality. The following questions guided this study: What is the surgical nurses’ perception level of caring quality? What is the surgical nurses’ ethical sensitivity level? Is there a relationship between surgical nurses’ perception level of caring quality and their ethical sensitivity? Is there a relationship between surgical nurses’ perception level of caring quality and their ethical sensitivity as per their working characteristics?
Materials and methods
Study design
The study was conducted as a cross-sectional, descriptive-correlational study with the aim of evaluating the perception of nursing care quality and ethical sensitivity of nurses working in surgical units.
Sample and setting
The research data were collected between February 2018 and January 2019. The research was conducted in four hospitals in the provinces of Kocaeli and Eskişehir: one public hospital, two university hospitals, and one private hospital. The research population consisted of 308 nurses working in all surgical units (including surgical intensive care units). The power of the study was assessed via Post hoc Power Analyses and calculated as 0.99. No sampling selection was made as we aimed to reach all nurses working in these units. Nurses who volunteered to participate in the study were informed that they had the right to withdraw at any stage they requested.
The acceptance criteria of the research were to be working in surgical units. The researcher received verbal and written informed consent from volunteer nurses after explaining the purpose, scope, and content of the study. After receiving the necessary permits for the study, the researchers visited the surgical units by checking the nurses’ working chart and observing their availabilities and referred to the nurses as an individual. The administrative staff assisted the researcher in determining the number of nurses working in the units. No specific procedure was implemented to ensure nurse involvement.
Data collection tools
Data were collected between the dates of February 2018 and January 2019. In data collection “Nurse Demographic Information Form,” “Caring Behaviours Inventory-24 (CBI-24)” and Ethical Sensitivity Questionnaire (ESQ)’ were used. Data collection tools were provided by the researchers for the nurses who agreed to participate after they were informed about the study and were collected after they were finished.
Nurse demographic information form
The form includes questions regarding age, gender, educational status, marital status, working period at the clinic, working shift, weekly working hours, number of beds in the clinic, number of daily surgical interventions in the clinic and the scores given for the nursing care quality.
CBI-24
CBI-24 was structured by Wu et al. 22 and is the short form of the 42-item “Caring Behaviours Inventory” which was developed by Wolf et al. 23 and is suitable for bi-directional diagnosis by nurses and patients. The validity and reliability study of this inventory was conducted by Kurşun and Kanan. 24 For the total of the inventory, the Cronbach’s alpha value was determined as 0.97 in patients and as 0.96 in nurses. The inventory consists of 4 sub-categories of assurance (8 items), knowledge-skill (5 items), being respectful (6 items) and commitment (5 items) and 24 items. Six-point Likert-type scale (1 = never, 2 = almost never, 3 = sometimes, 4 = generally, 5 = most of the time, 6 = always) was used for the answers. The total score of all items was divided by 24 and scale total score between 1 and 6 was obtained; the total score of all items in the sub-scales was divided by the number of the items and sub-scale scores between 1 and 6 were obtained. As the sub-scale and total scale scores increase, the level of perception of the caring quality of patients or nurses increases.
ESQ
Developed by Lutzen, the ESQ was used in 1994 to determine the ethical sensitivity of the physicians and nurses who worked primarily in Karolinska Institution of Nursing (Sweden-Stockholm) and then in other units in the ethical decision-making process. ESQ is a 7 points Likert-type scale, which consists of a total of 30 items and 6 subscales (autonomy, providing benefit, holistic approach, conflict, practice, orientation). Questionnaire includes six subscales, which are “autonomy” (reflects showing respect for the autonomy principle and patient’s choice), “providing benefit” (reflects the action aimed to improve the benefit of the patient), “holistic approach” (reflects the actions which will both not harm the patient and also ensure the patient’s integrity), “conflict” (reflects the experience of an inner ethical dispute), “practice” (reflects considering the ethical aspect in decision-making and practice), “orientation” (reflects the healthcare professionals’ interest in the actions which will affect their relationship with the patients). 25,26 The validity and reliability study of ESQ was performed by Tosun in 2005 and the Cronbach’s alpha value was found as 0.84. In the calculation of the scale, the expressions are evaluated between 1 point (strongly agree) and 7 points (strongly disagree). One-point represents the high sensitivity for complete agreement and 7-point represents the low sensitivity for complete disagreement and the total score varies between 30 and 210. The total score is evaluated. A high score indicates a low ethical sensitivity and a low score indicates a high ethical sensitivity. 26
Ethical considerations
In order for the research to be conducted, institutional permission from the hospitals, a written permission including the 29 November 2017 dated and KÜ GOKAEK 2017/16.21 numbered decision by the Kocaeli University Non-Invasive Clinic Research Ethical Committee with the 28 November 2018 dated and 34059705-799 decision by Kocaeli Local Health Authority, and also written and verbal informed consents from the participants were obtained.
Data analysis
Statistical evaluation was performed via IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA) package program. The normal distribution suitability test was evaluated by Kolmogorov-Smirnov Test. Numerical variables were demonstrated as medians (25 and 75. percentile) and frequency (percentages). Non-normally distributed variables were assessed via Mann–Whitney U Test, Kruskal–Wallis one-way analysis of variance and Dunn’s multiple comparison test. The relationship between the numeric variables was obtained via the Spearman correlation analysis. For two-way tests p < 0.05 was considered as statistically significant.
Results
Participant characteristics
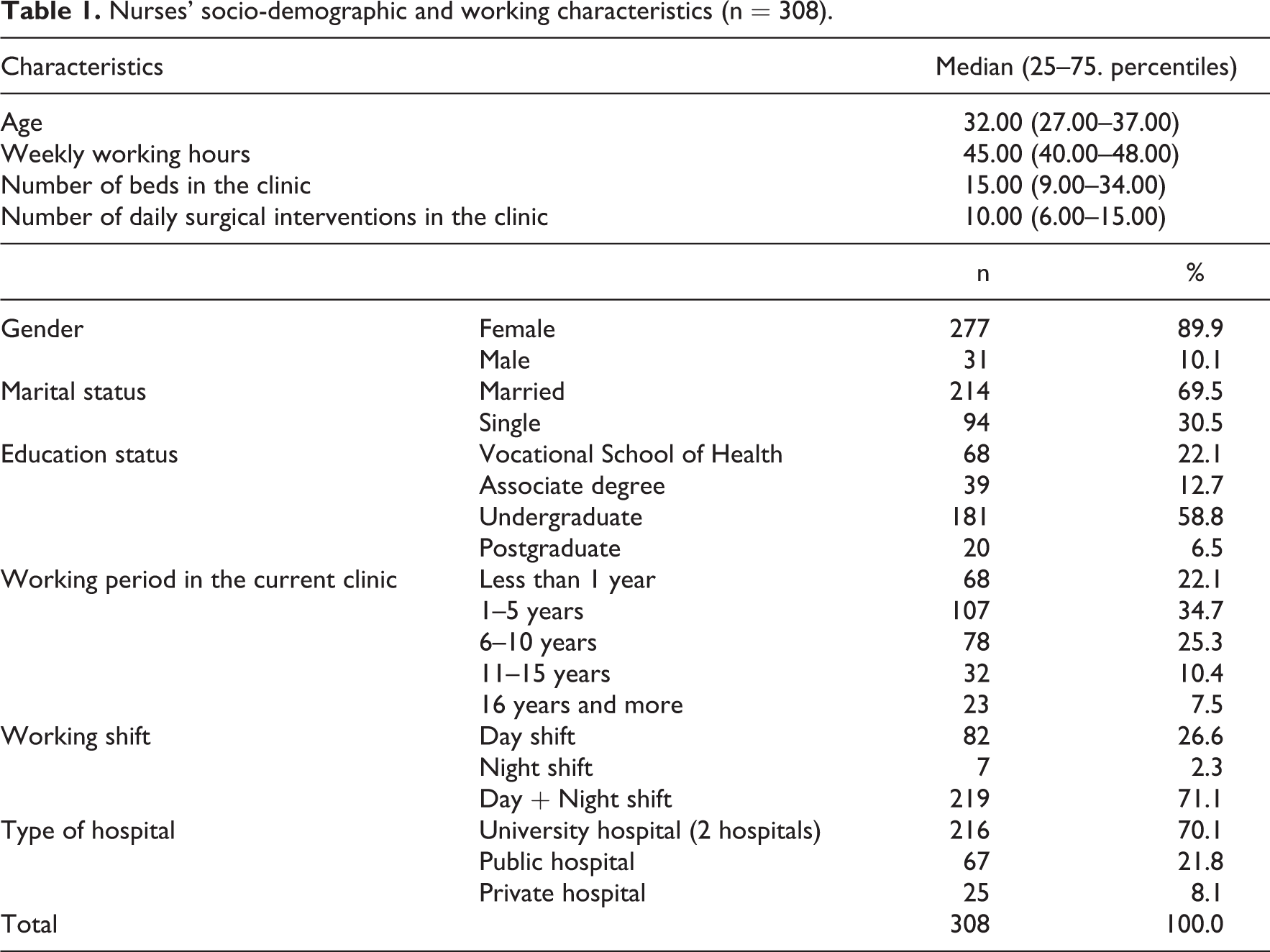
It was found that the median of nurses’ ages was 23.00 (27.00–37.00), weekly working hours were 45.00 (40.00–48.00), the number of beds in the clinic was 15.00 (9.00–34.00) and the number of daily surgical interventions in the clinic was 10.00 (6.00–15.00); 89.9% of the patients were female, 69.5% were married, 58.8% had a bachelor’s degree, 34.7% of the nurses had been working in the current clinic for 1–5 years, 71.1% of the nurses were working at day + night shifts and 70.1% were working at the university hospital (Table 1).
Nurses’ socio-demographic and working characteristics (n = 308).
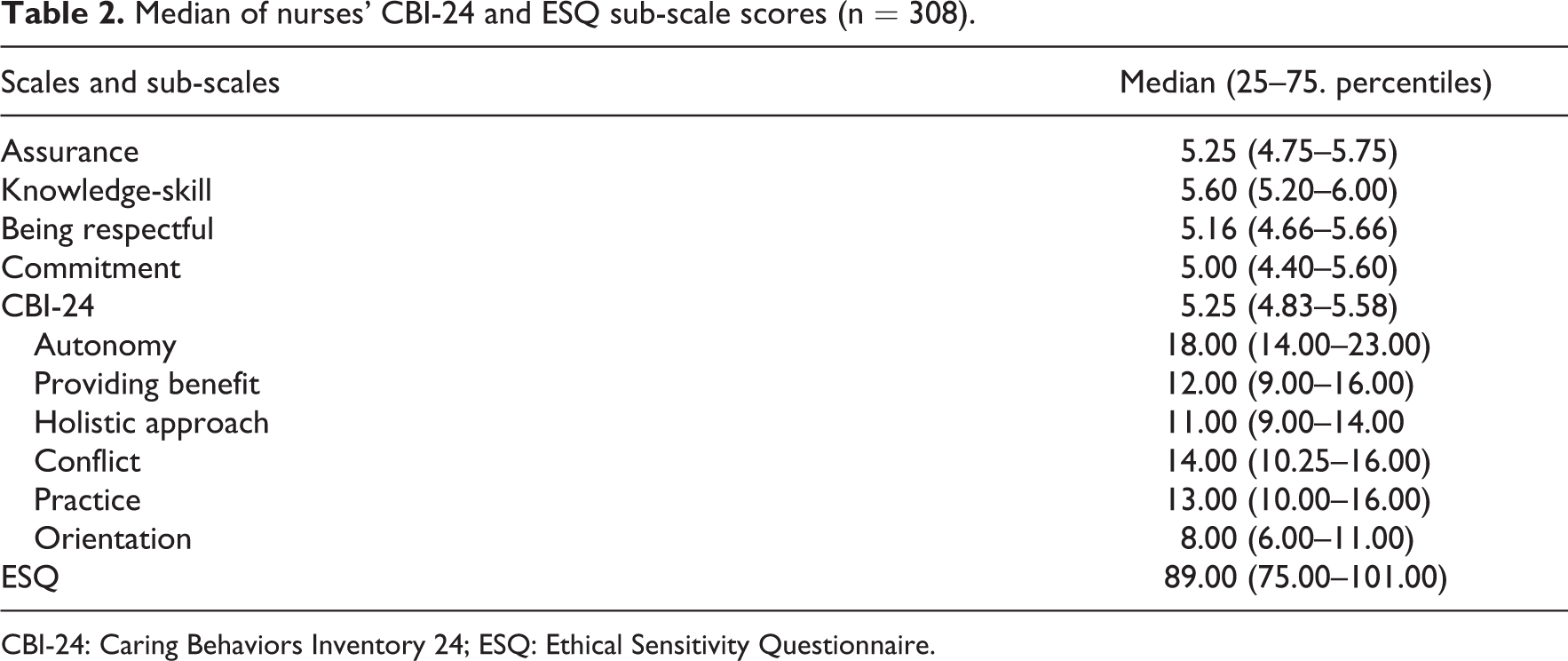
Median of nurses’ CBI-24 and ESQ scores
It was detected that in nurses’ CBI-24 total score the median was 5.25 (4.83–5.58), nurses’ perception levels of caring quality were high; ESQ total score median was 89.00 (75.00–101.00) and ESQ sub-scale and total scores were at a moderate level (Table 2).
Median of nurses’ CBI-24 and ESQ sub-scale scores (n = 308).
CBI-24: Caring Behaviors Inventory 24; ESQ: Ethical Sensitivity Questionnaire.
The correlation between CBI-24 and ESQ and scale subdimensions
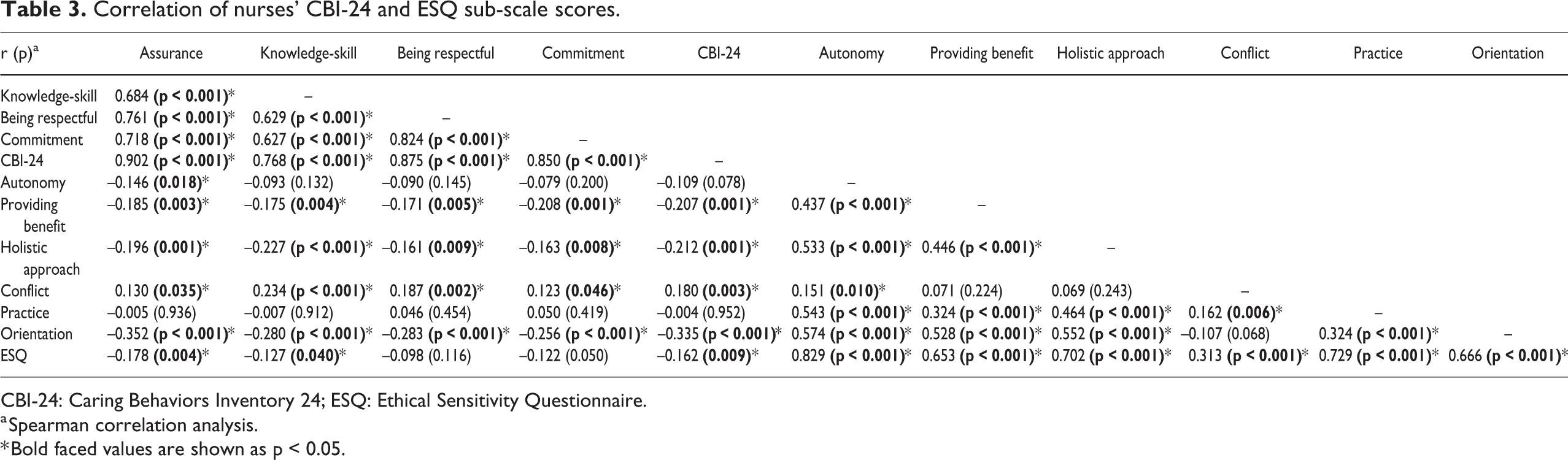
It was found that there was a significant positive correlation between CBI-24 total score and scale sub-dimension scores of nurses (p < 0.001); as the total score of CBI-24 increased, the scale subscale scores also increased, there was a negative significant relationship between assurance (r = -0.178; p = 0.004), knowledge-skill (r = -0.127; p = 0.04), subdimensions of CBI-24 and CBI-24 total score (r = -0.162; p = 0.009), and ESQ total score; as the total score of assurance, knowledge-skill, and CBI-24 increased, ESQ total score decreased.
There was a positive significant relationship between ESQ total score and all of its subdimensions (p < 0.001); as ESQ total score increased, scale subdimension also increased. A negative significant relationship was found between providing benefit (r = -0.207, p = 0.001), holistic approach (r = -0.212, p = 0.001), orientation (r = -0.335, p < 0.001), and subdimension scores of ESQ and CBI-24 total score; as the scores of providing benefit, holistic approach and orientation increased, CBI-24 total score decreased. However, there was a positive significant relationship between the conflict subdimension and CBI-24 total scores (r = 0.180, p = 0.003); as the conflict score increased, CBI-24 total score also increased (Table 3).
Correlation of nurses’ CBI-24 and ESQ sub-scale scores.
CBI-24: Caring Behaviors Inventory 24; ESQ: Ethical Sensitivity Questionnaire.
a Spearman correlation analysis.
* Bold faced values are shown as p < 0.05.
The correlation between certain work characteristics and CBI-24 and ESQ scores
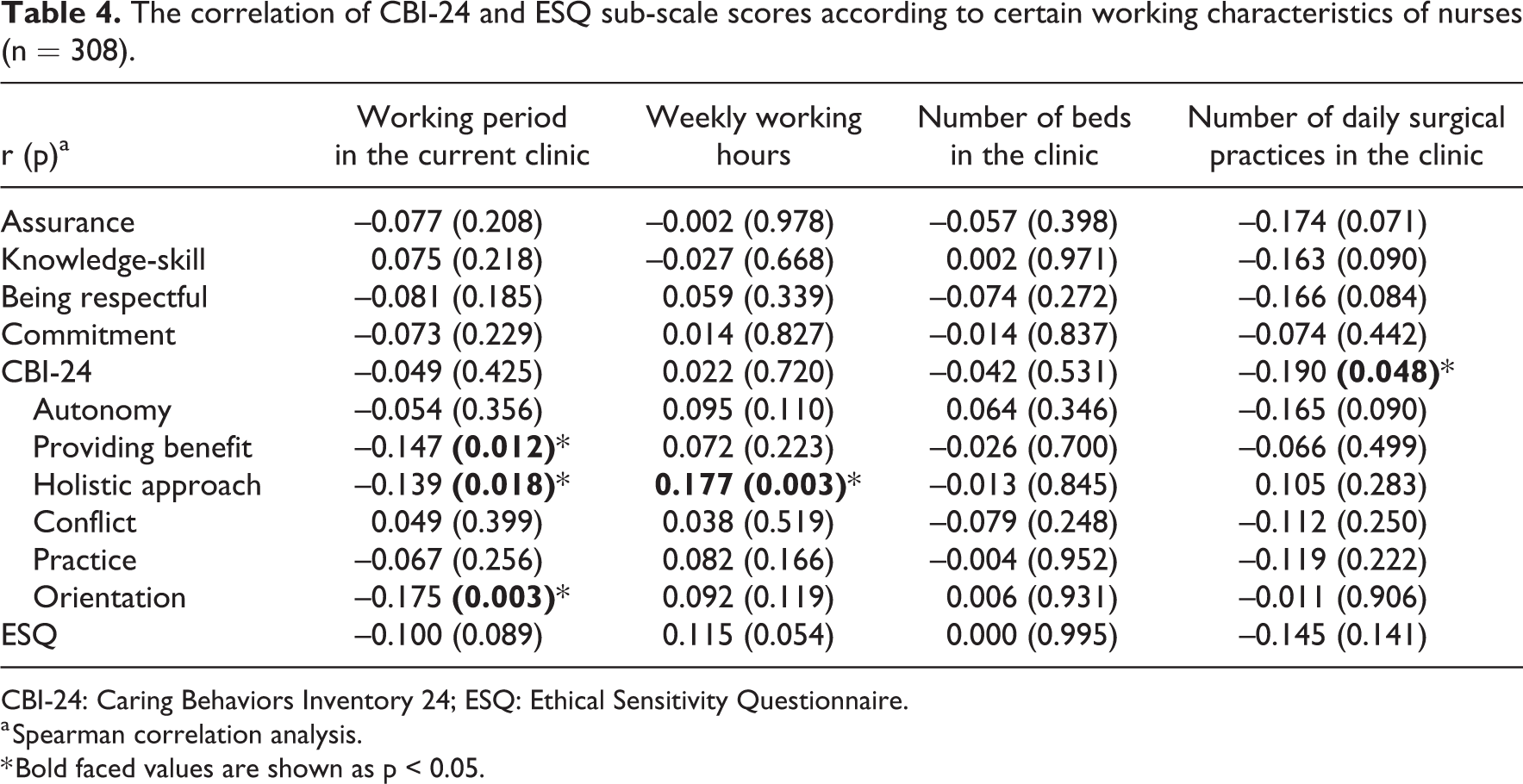
It was found that there was a negative significant relationship between nurses’ working periods in the current clinic and ESQ sub-scales of providing benefit (r = -0.147; p = 0.012), holistic approach (r = -0.139; p = 0.018) and orientation (r = -0.175; p = 0.003); as the working period in the current clinic increased, the scores of providing benefit, holistic approach, and orientation decreased. There was a positive significant relation between weekly working hours and ESQ sub-scale of holistic approach (r = 0.177; p = 0.003); as the weekly working time increased, the holistic approach score also increased.
There was a negative significant relationship between the number of daily surgical practices in the clinic and CBI-24 total score (r = -0.190; p = 0.048); as the number of daily surgical practices in the clinic increased, CBI-24 total score decreased (Table 4).
The correlation of CBI-24 and ESQ sub-scale scores according to certain working characteristics of nurses (n = 308).
CBI-24: Caring Behaviors Inventory 24; ESQ: Ethical Sensitivity Questionnaire.
a Spearman correlation analysis.
* Bold faced values are shown as p < 0.05.
The comparison of CBI-24 and ESQ scores according to certain work characteristics
The findings showed that there was a significant difference between the item of working at the current clinic wilfully and CBI-24 sub-scales of “assurance” (p = 0.007), “knowledge-skill” (p = 0.002), “being respectful” (p = 0.013) and CBI-24 total score (p = 0.015), nurses working at the current clinic wilfully had higher assurance, knowledge-skill, being respectful and CBI-24 total scores. There was a significant difference between the hospital type and CBI-24 sub-scales of “assurance,” “being respectful,” “commitment” and “CBI-24” total scores: Nurses working at a private hospital had higher “assurance” scores than the nurses working at a university hospital (p = 0.005) and also the “assurance” scores of the nurses working at private hospital were higher than scores of the nurses who worked at a public hospital (p = 0.047); Nurses working at a private hospital had higher scores in the item of “being respectful” than the nurses who worked at a university hospital (p = 0.002) and also the scores of “being respectful” were higher in the nurses who worked at a private hospital than the scores of the nurses working at a public hospital (p = 0.038); “Commitment” scores of the nurses working at a private hospital were higher than the scores of the nurses who worked at a university hospital (p = 0.003); In terms of “CBI-24” total scores, nurses who worked at a private hospital had higher scores than the nurses working at a university hospital (p = 0.001) and the nurses working at a public hospital (p = 0.009) (Table 5).
Comparison of the sub-scales and the scores of CBI-24 and ESQ as per some nurses’ working characteristics (working characteristics where a significant difference was observed) (n = 308) (Median (25–75 percentiles)).
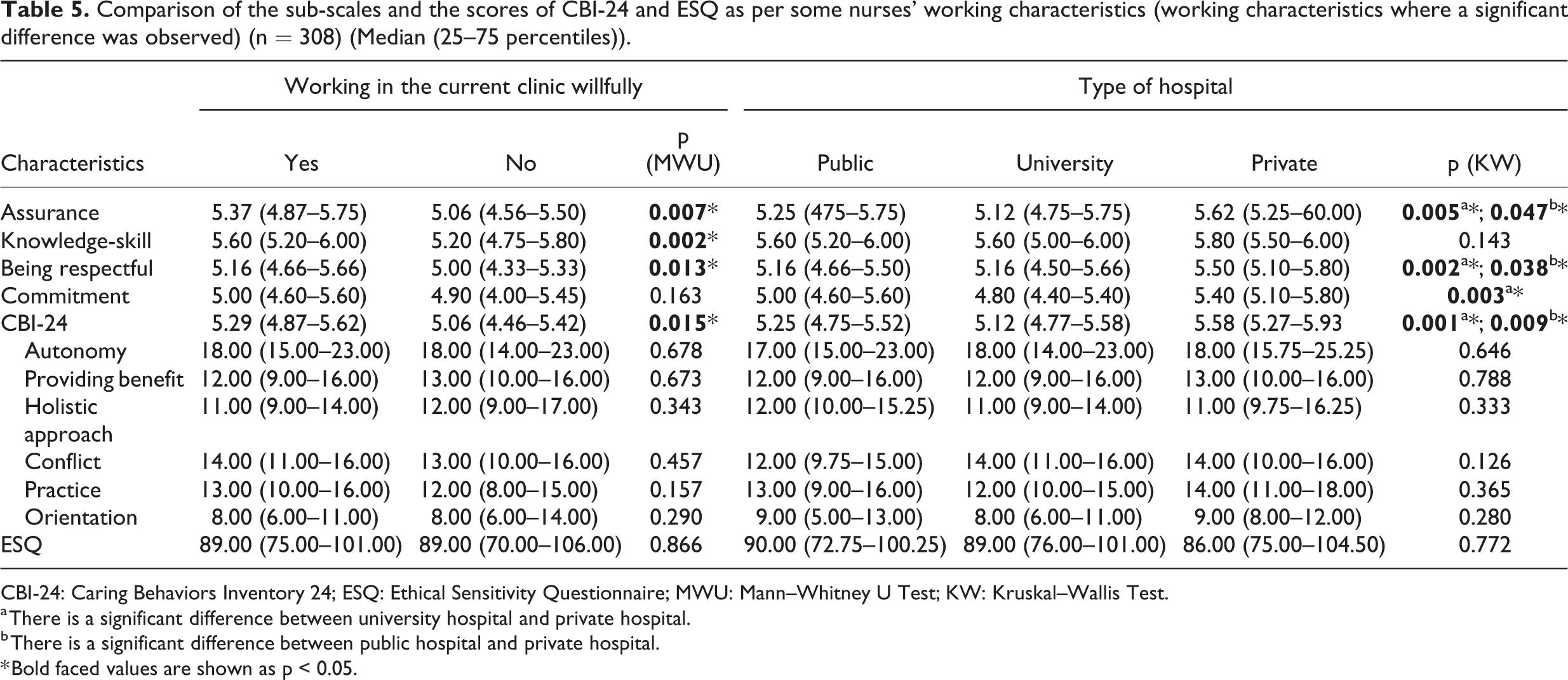
CBI-24: Caring Behaviors Inventory 24; ESQ: Ethical Sensitivity Questionnaire; MWU: Mann–Whitney U Test; KW: Kruskal–Wallis Test.
a There is a significant difference between university hospital and private hospital.
b There is a significant difference between public hospital and private hospital.
* Bold faced values are shown as p < 0.05.
Discussion
It is important that the nurses have an improved ethical sensitivity, which is defined as the ability to identify an ethical problem, in order for the nurses to recognize the ethical problems and be able to make correct decisions. 5 It was determined in the study that surgical nurses’ perception levels of caring quality were high and their ethical sensitivity levels were moderate. Similar to this finding, studies carried out by Pauly et al., 27 Temiz et al., 2 Rokhafrooz et al., 28 Nora et al., 29 Basar and Cilingir 19 also reported that nurses’ ethical sensitivity levels were moderate. It can be stated that in order to increase the moral sensitivity of the nurses, factors that negatively affect sensitivity should be identified and precautions should be taken against these factors.
Nora et al. 29 conducted a study determining the ethical sensitivity of the primary health care nurses (n = 100) and found out that nurses’ ethical sensitivity score was 4.5 (out of 7), and it was stated that a moderate level of ethical sensitivity decreases the quality of preventive health services. In our study, it was found that as the nurses’ scores regarding the CBI-24 sub-scales of assurance and knowledge-skill increased, their ethical sensitivity levels also increased, and as the scores obtained from ESQ sub-scales of providing benefit, holistic approach, orientation, and ESQ total score increased, the scores regarding the nurses’ perception of caring quality also increased. Therefore, it was concluded that nurses’ perception of caring quality increased as the nurses’ ethical sensitivity levels. Contrary to our findings, Amiri et al. 21 reported in their study, in which they investigated the relationship between nurses’ ethical sensitivity and the caring quality, that there was no significant relationship between the quality of care and the nurses’ ethical sensitivity. The sample size (n = 198) might be the reason for these results obtained from the study of Amiri et al. 21 The results obtained from this study support the findings of some of the studies 11,15,29 whereas they do not support the findings of Amiri et al. 21 study. In this respect, it can be stated that ethical sensitivity is an important determinant of the quality of nursing care.
Duration of professional experience was reported as an important determinant in the acquisition of ethical sensitivity skills. 2,9 It was found that nurses’ ethical sensitivity levels in ESQ sub-scales of providing benefit, holistic approach and orientation increased as the nurses’ working period at the current clinic (p < 0.05). In the studies by Lutzen et al. 30 and Buyuk et al., 10 it is reported that people with more experience have higher moral sensitivity in making the right decision when faced with ethical dilemmas. In the study conducted by Ulrich et al. 13 on ethical problems and stress in nursing practices, it was reported that young and less experienced nurses experienced more ethical problems and higher stress. This result suggests that working in the same unit for a long time results in a more accurate/clear/analytical approach because of the better recognition and adoption of the clinic.
It was determined that nurses working at the current clinic wilfully had higher assurance, knowledge-skill, being respectful and CBI-24 total scores (p < 0.05). It can be said that the high level of job satisfaction of nurses who love their profession and work willingly in their current clinics has an effect on this result. It was also detected that nurses working at a private hospital had higher scores of assurance, being respectful, commitment and CBI-24 total scores than the nurses who worked at a university or public hospitals (p < 0.05). The workload, the number of the in-patients, lower levels of job-loss fear and higher levels of hierarchy in the public and university hospitals might be the reasons for this situation. In addition, the findings in Table 5 and the lack of literature limited the discussion of these findings.
Limitations of the study
The study can be repeated with a higher sample to generalize the results of the study to surgical nurses in this country.
In addition, it may be suggested that qualitative studies may be more useful in order to determine the relationship between nurses’ level of ethical sensitivity and perceptions of care quality, and also different affecting variables.
Conclusion and implications for nursing practice
It was detected in this study that Nurses’ perception levels of caring quality were high, and their ethical sensitivity levels were moderate; ESQ total score decreased as CBI-24 total score increased; ESQ total score decreased as the scores regarding CBI-24 sub-scales of assurance and knowledge-skill increased; CBI-24 total score decreased as the scores of ESQ sub-scales of providing benefit, holistic approach and orientation increased; CBI-24 total score increased as the conflict score increased; As the score regarding the item of the working period at the current clinic increased the scores of the ESQ sub-scales of providing benefit, holistic approach and orientation decreased; the score regarding ESQ sub-scale of holistic approach increased as the weekly working hours increased; Nurses working at the current clinic wilfully had higher assurance, knowledge-skill, being respectful and CBI-24 total scores; Nurses working at a private hospital had higher assurance, knowledge-skill, being respectful, commitment and CBI-24 total scores.
Accordingly, it is suggested that in order to increase the level of ethical sensitivity of nurses, continuity of ethical trainings should be ensured, ethical sensitivity skills should be acquired and employees should be monitored whether they can reflect this skill to their behaviors, institutions should take supportive initiatives to reduce workloads such as reducing the number of weekly working hours and the number of daily surgical interventions in the clinic, which adversely affect nursing care quality and ethical sensitivity. In addition, it is considered that it is important to carry out qualitative studies in order to determine the relationship between nurses’ ethical sensitivity levels and their perception levels of caring quality and also the different variables that affect these conditions.
In addition, standard forms/scales on ethics should be included in every clinic in the world, as the issue of ethics provides a moral diagnosis of care. This concept, which is considered as abstract, will also be evaluated in terms of quantity, and numerical value will be provided to enable nurses to express themselves more effectively and to have confidence in themselves.
Footnotes
Acknowledgements
The authors thank all the surgical nurses who participated in this study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
This study was presented as a verbal paper at the 9th EORNA Congress, Haque, the Netherlands between 16 and 19 May 2019.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The budget of this project was allocated by Kocaeli University Scientific Research Projects Coordination Unit (Project Number: 2018/044).