
Abstract
Background:
Nurses need moral courage to ensure ethically good care. Moral courage is an individual characteristic and therefore it is relevant to examine its association with nurses’ socio-demographic factors.
Objective:
To describe nurses’ self-assessed level of moral courage and its association with their socio-demographic factors.
Research design:
Quantitative descriptive cross-sectional study. The data were collected with Nurses’ Moral Courage Scale and analyzed statistically.
Participants and research context:
A total of 482 registered nurses from a major university hospital in Southern Finland completed the Finnish language version of Nurses’ Moral Courage Scale in autumn 2017.
Ethical considerations:
Ethical approval was obtained from the university ethics committee and permission for the data collection from the participating hospital. Ethical principles and scientific guidelines were followed throughout the research process.
Findings:
Nurses’ self-assessed level of moral courage was rather high. On Visual Analogy Scale (0–10), the mean value was 8.20 and the mean score of the four dimensional, 21-item Nurses’ Moral Courage Scale was 4.09 on a 5-point Likert-type scale. Respondents’ gender, present work role, ethical knowledge base, additional ethics education, self-study as a means to acquire ethical knowledge, and frequency of work situations needing moral courage were statistically significantly associated with nurses’ moral courage.
Discussion:
Strongest association was found between nurses’ higher moral courage level and formal and informal ethics education. Honesty and patient’s humane and dignified encounter received the highest scores indicating respondents’ internalization of the core values of nursing.
Conclusion:
Although nurses were fairly morally courageous, moral courage should be a part of nurses’ basic and continuing education thus covering its theoretical and practical learning. Since moral courage is a virtue that can be taught, learnt, and practiced, education is a relevant way to maintain and further strengthen nurses’ moral courage.
Introduction
Ethical conflicts are part of everyday nursing and therefore moral perspective is inherent in all nursing activities. 1 Thus, moral competence is fundamental in nursing, and moral courage is a key element of moral competence. 2 In nursing, moral courage denotes knowledge of one’s own ethical and professional values and principles and fortitude to stand up for them in ethically conflicting situations. 3 Moral courage is a virtue, an individual characteristic manifested as actions in the practice of nursing. 2 Moral courage, like other virtues, can be practiced, developed, and strengthened. 4
However, it is not always easy to do the right thing, that is, to act according to one’s values and principles. Taking the morally right course of action might require standing up against others, and it can cause harm to the actor.2,5 This requires moral courage of the nurse which is needed to ensure quality nursing care. 5 Courageous action requires overcoming fear, and a morally courageous nurse is aware of the personal risk involved in defending good and ethically high-quality care as the goal of healthcare. 6
Nursing environment is a complex system, also ethically.7,8 Several organizational and individual factors are associated with ethical questions, which arise daily in different nursing contexts and levels of care. Moral courage is a way to address these ethical issues, and it is a manifestation of values which the nurse is not willing to compromise. 9 Nursing and ethical decision-making do not take place in a vacuum. The nurse is always a part of the wider care environment, and every nurse can contribute to promoting, or conversely to undermining the culture of moral courage by displaying moral courage in multiple ways.5,10 Speaking up her concerns, pointing out and intervening in unethical practices, and admitting her own mistakes are all morally courageous actions for safeguarding good care. 10
However, research of moral courage in nursing has been scarce. Most of the previous studies of nurses’ moral courage have approached the concept using qualitative research designs.11–22 Studies have revealed that moral courage appears as a desire to protect patients and to defend their rights.10,13,17,19 Studies have identified moral courage as a personal virtue. Some socio-demographic factors, such as nurses,’ length of work experience,19,20 higher level of education,23,24 age, 24 the frequency of encountering ethically challenging situations, 20 and education in ethics25–27 have been associated with nurses’ level of moral courage.
Notwithstanding, assessing and developing moral courage would benefit from further evidence-based knowledge of nurses’ moral courage and from valid and reliable instruments to measure it. Scales to measure moral courage have been previously developed in the field of psychology27,28 and medicine. 29 Nurses’ moral distress have been studied and measured fairly much, but moral courage as a mitigating factor to it has received fairly little attention.30–32 A questionnaire to measure perioperative nurses’ moral courage has been developed, but the instrument has not been validated.33,34
The Nurses’ Moral Courage Scale© (NMCS) 35 is a new, validated35,36 instrument intended to measure nurses’ self-assessed moral courage. The NMCS enables the examination of associations between nurses’ socio-demographic factors’ and their moral courage. In order to strengthen nurses’ ability to defend ethically good care, and to stand up for their values, it is crucial to examine nurses’ perceptions of their moral courage and what kind of factors are associated with it using a valid and reliable instrument developed especially for nursing context.
Objective
The aim of this study is to describe nurses’ self-assessed level of moral courage and to find out whether their socio-demographic factors are associated with it.
Methods
Research design
This was a quantitative descriptive cross-sectional study. The data consisted of nurses’ socio-demographic factors and their responses to the structured NMCS 35 self-assessment questionnaire. The data were analyzed with the SPSS 22.0 (IBM Corporation) program.
Participants and data collection
The data were collected in September–October 2017 from a major university hospital in Southern Finland. Hospital’s human resource manager, acting as the study’s liaison person, defined four clinical areas for data collection. The selected areas were (1) children and adolescents; (2) operating room, intensive care, and pain management; (3) psychiatry; and (4) head and neck center (Figure 1). The clinical areas were of different sizes in terms of the number of nursing staff and provided a representative sample of nurses representing a large variety of different care contexts
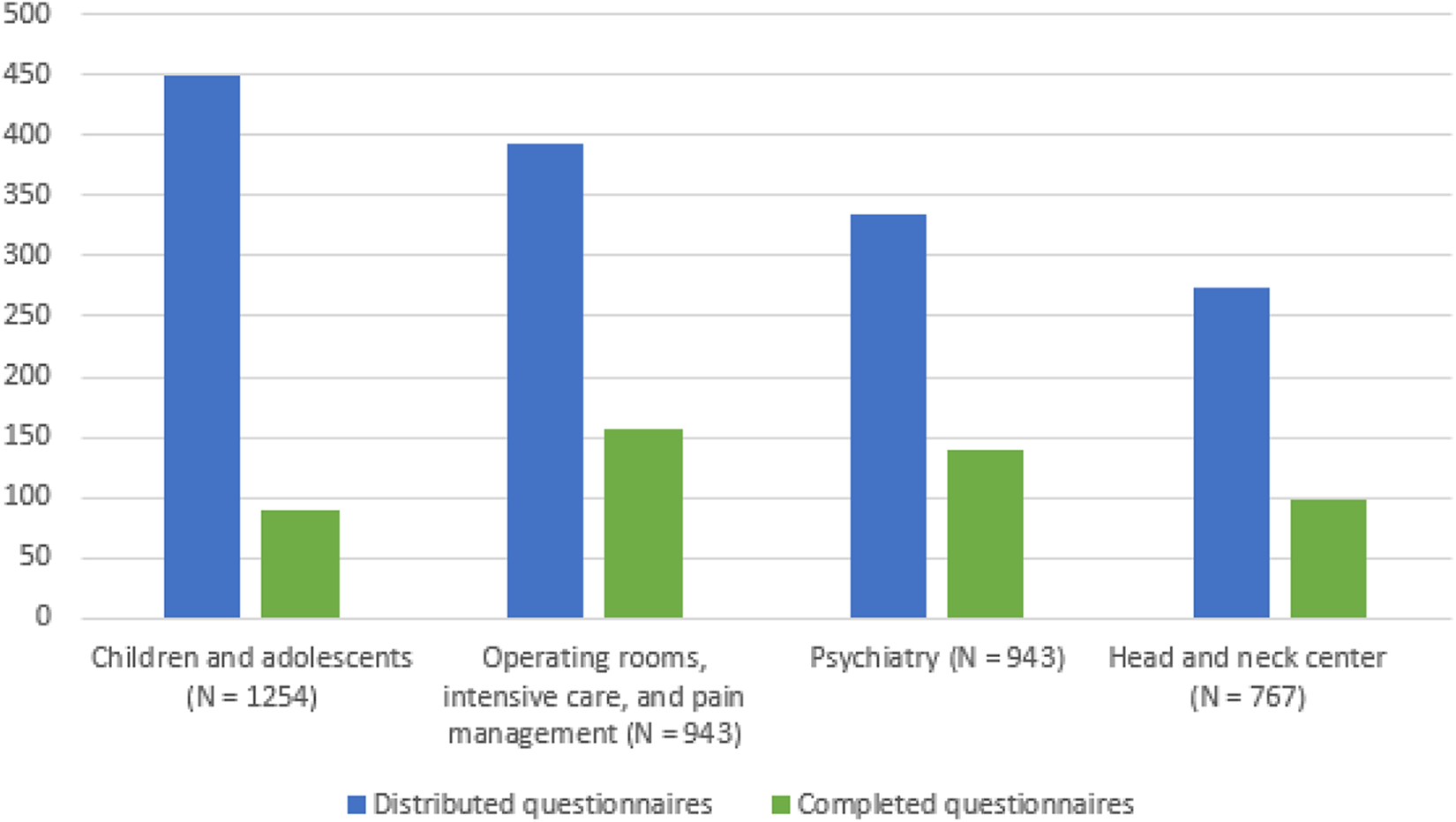
The total number of nurses in clinical areas, and distributed and completed questionnaires.
The total number of nurses in the four units was 3907. Based on the statistical power analysis, the required number of the participants was 402 nurses at 90%; 0.05 significance level. The estimated response rate was 30% based to previous knowledge. 37 The questionnaires were distributed in proportion to the total number of the nursing staff in the four units, and as many as was estimated to reach the minimum 30% response rate. The final response rate was 34.2 %.
Inclusion criteria for the participants were (1) registered nurses, midwives, or public health nurses licensed by National Supervisory Authority for Welfare and Health (http://Valvira.fi); (2) currently employed at one of the four clinical areas; and (3) sufficient Finnish language skill to complete the questionnaire.
Instrument
Data were collected with the original Finnish language version of NMCS. 35 The scale consists of 21 items measuring nurses’ self-assessed level of moral courage in four dimensions: (1) compassion and true presence (5 items), (2) moral responsibility (4 items), (3) moral integrity (7 items), and (4) commitment to good care (5 items) (Table 1). The Cronbach’s alpha values of the four dimensions in the original NMCS 35 were, respectively, 0.81, 0.81, 0.82, and 0.74. The Cronbach’s alpha value of the total scale was 0.93.
Nurses’ socio-demographic background variables (n = 482).

SD: standard deviation.
The items are presented in a random order so they cannot be associated directly with the dimensions they belong to. Items were assessed on a 5-point Likert-type scale (from 1 = does not describe me at all to 5 = describes me very well). In addition to the NMCS, the questionnaire comprises 10 socio-demographic questions and a VAS (Visual Analogy Scale: 1–10) requesting nurses to assess their overall moral courage (Table 1). A detailed description of the NMCS is presented elsewhere. 35
Questionnaires were distributed to the head nurses of the four clinical areas to be forwarded to nurses working in the wards of each clinical area. Participating nurses received a pen-and-paper version of the questionnaire to obtain a better response rate than using an electronic questionnaire.38,39 The cover letter contained instructions for completing the NMCS, information of the purpose of the study, of voluntary participation, and of the guarantee of anonymity of the participants. Completed questionnaires were returned in a sealed envelope to the human resource manager, from whom the researcher picked them up for analysis. 35
Data analysis
The data were analyzed with the SPSS 22.0 (IBM Corporation) program. Description of the data was carried out by examining the frequency distributions of variables and parameters. The sum of different variables was formed by summing the response codes of the variables related to the equivalent dimension of moral courage and dividing it by the total number of variables. To test the internal consistency, the Cronbach’s alpha coefficient was computed. The association of socio-demographic variables with summed variables describing the self-assessed level of moral courage was tested by multivariate analysis of variance (MANOVA). For a significant categorical explanatory variable for categorical variable, pairwise comparisons were performed using Sidak’s multiple comparison test. For a significant numerical explanatory variable, the correlation was interpreted using a regression coefficient. The statistical significance level was set at p-value < 0.05.35,40
Ethical considerations
The principles of good scientific practice were followed throughout the research process. 41 An ethical approval was obtained from the Ethics Committee of University of Turku (No. 63, 12 December 2016). 35 Permission to conduct the study was obtained from the participating hospital (No. 71; 15 March 2017). Participants were informed in the cover letter of voluntary participation, anonymity, confidentiality letter, and possibility to withdraw from the study any time. 36 Completion of the questionnaire was considered a consent to participate. 42
Results
Participants
The majority of the respondents were female (88.6%); registered nurses, midwives, or public health nurses by their highest degree (89.2%); and currently working as staff nurses (87%). Most of the respondents estimated that their knowledge base in healthcare ethics was at a good (69.3%) or excellent level (13.9%). The vast majority of respondents had not been actively involved in activities related to healthcare ethics or its development (92.6%). Most of the respondents had encountered situations requiring moral courage at work sometimes (51.2%) or quite often (33.2%) (Table 1).
Nurses’ self-assessed moral courage level
The overall level of nurses’ self-assessed moral courage measured using Visual Analogue Scale (VAS 0–10) was quite high (mean = 8.20; SD = 0.973). The lowest single rating was 5.0 and the highest 10.0.
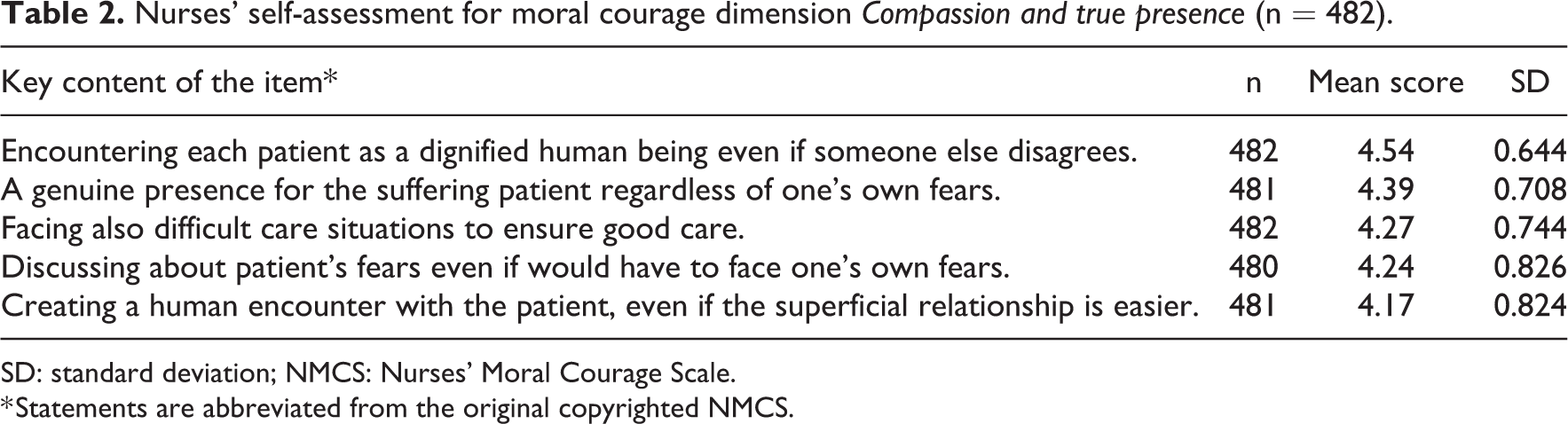
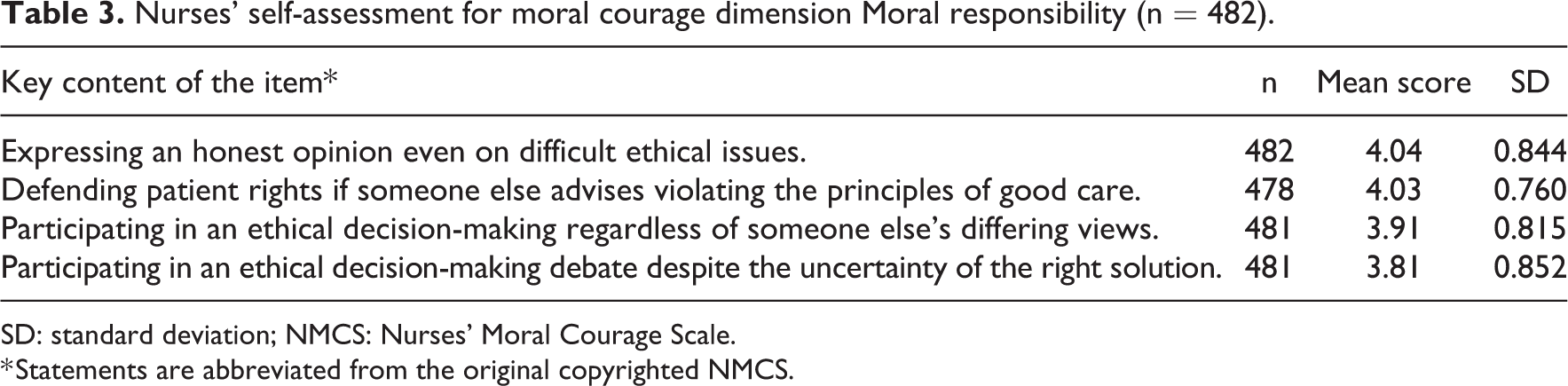
The mean score from the four dimensional, 21-item scale NMCS, assessed by 5-point Likert-type scale, was also quite high, 4.10 (SD = 0.498). The lowest single value of the summed averages of all items was 3.60 and the highest 4.70. Of the four dimensions, the highest mean score of the answers was 4.32 in compassion and true presence (Table 2), and lowest 3.95, in moral responsibility (Table 3).
Nurses’ self-assessment for moral courage dimension Compassion and true presence (n = 482).
SD: standard deviation; NMCS: Nurses’ Moral Courage Scale.
* Statements are abbreviated from the original copyrighted NMCS.
Nurses’ self-assessment for moral courage dimension Moral responsibility (n = 482).
SD: standard deviation; NMCS: Nurses’ Moral Courage Scale.
* Statements are abbreviated from the original copyrighted NMCS.
The overall level of self-assessed moral courage (VAS 0–10) was associated with all four moral courage dimensions. Nurses who had higher overall moral courage had better compassion and true presence (p < 0.001), moral responsibility (p < 0.001), moral integrity (p < 0.001), and commitment to good care (p < 0.001).
Compassion and true presence
The first dimension, compassion and true presence, was evaluated by five items*. On average, the highest score was obtained for the statement that nurse would treat the patient with dignity even if someone else disagreed (4.54). The second highest rating was given for the statement that the nurse tends to be genuinely present for the patient despite her own fears (4.39) (Table 2).
Moral responsibility
Of the four statements* indicating nurses’ moral responsibility, the highest rating was given to the item describing the nurse’s courage to express her own views on difficult ethical issues (4.04). The second highest rating was given to the item, that the nurse advocates for the patient’s right to good care even if someone else involved in the patient’s care disagrees (4.03) (Table 3).
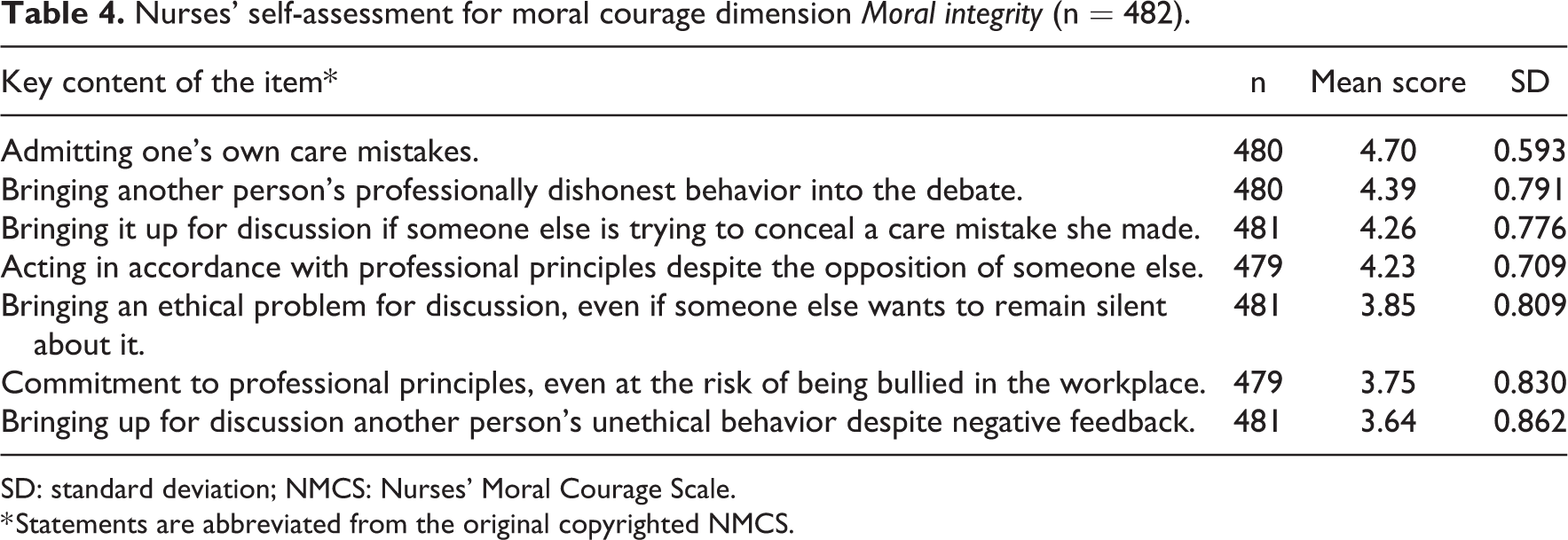
Moral integrity
Moral integrity was assessed with seven items*. The highest score of the dimension and the entire NMCS concerned the item that a nurse would admit her own care mistake (4.70). The standard deviation of the answers in this item was also the smallest (0.593), which could be interpreted that very few of the respondents would be concealing a care mistake. The second highest score in the dimension got the item pointing out the nurse’s willingness to broach someone else’s professionally dishonest conduct (4.39) (Table 4).
Nurses’ self-assessment for moral courage dimension Moral integrity (n = 482).
SD: standard deviation; NMCS: Nurses’ Moral Courage Scale.
* Statements are abbreviated from the original copyrighted NMCS.
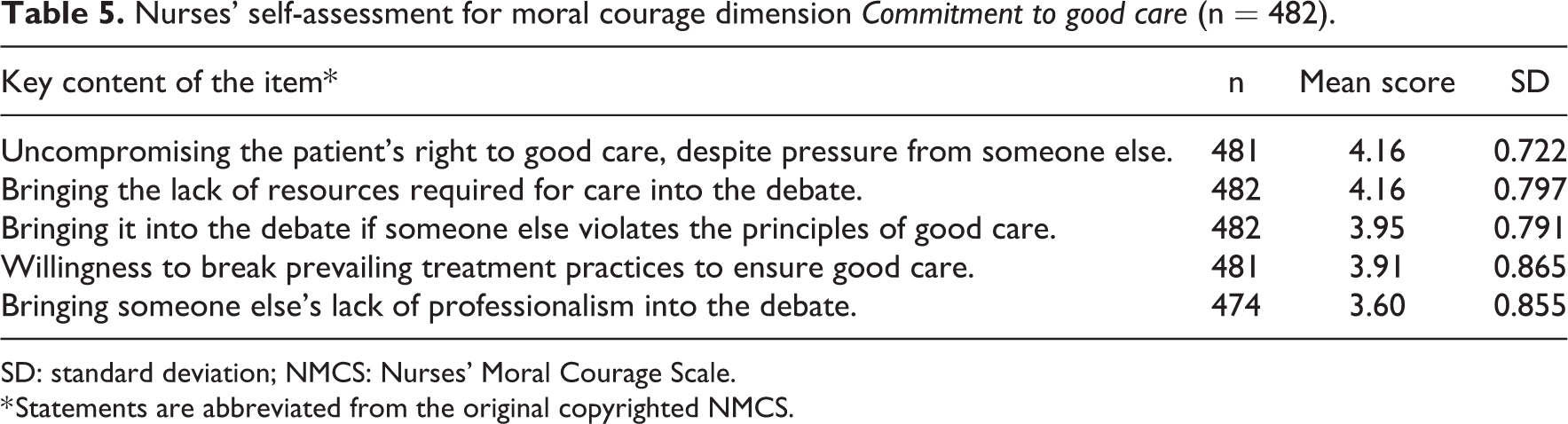
Commitment to good care
The fourth dimension, commitment to good care, was assessed in five items*. Two of the items received equal and the highest scores (4.16). The first item concerned the nurse’s unwillingness to compromise on a patient’s right to good care even if someone else urges to do otherwise, and the second item declared that a caregiver is willing to bring to discussion the lack of resources necessary for good care (Table 5).
Nurses’ self-assessment for moral courage dimension Commitment to good care (n = 482).
SD: standard deviation; NMCS: Nurses’ Moral Courage Scale.
* Statements are abbreviated from the original copyrighted NMCS.
Nurses’ socio-demographic factors associated with their self-assessed moral courage
Socio-demographic factors which were statistically significantly associated with nurses’ self-assessed moral courage were gender, present work role, ethical knowledge base, additional ethics education, and self-study as the means of acquiring the ethical knowledge base, as well as the frequency of situations needing moral courage at work (Table 6).
Socio-demographic variables and their correlations with dimensions of moral courage based on MANOVA (n = 482).
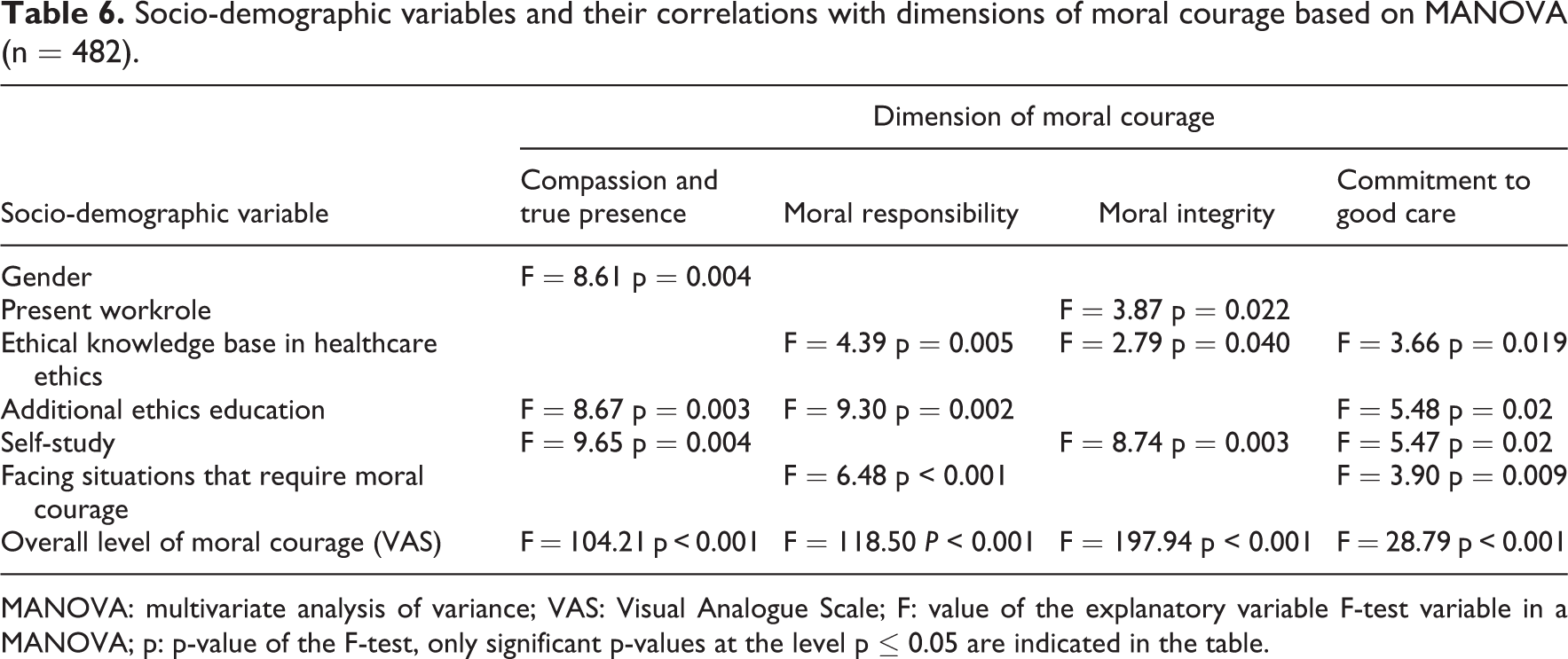
MANOVA: multivariate analysis of variance; VAS: Visual Analogue Scale; F: value of the explanatory variable F-test variable in a MANOVA; p: p-value of the F-test, only significant p-values at the level p ≤ 0.05 are indicated in the table.
According to the results, female nurses had stronger compassion and true presence than male nurses. Furthermore, the present work role was a statistically significant background factor, since assistant nurse managers had higher moral integrity than staff nurses. There were no statistically significant differences between the other work roles (Table 6).
As to ethical knowledge base, nurses who had acquired additional ethics education were more compassionate and truly present, more morally responsible, and more committed to good care than nurses who didn’t have any additional ethics education (Table 6). Slightly less than a half (44.4%) of nurses had acquired additional knowledge of nursing ethics through some additional ethics education, such as formal education, courses, or advanced education. Also, nurses who had studied ethics independently were more compassionate and truly present and had higher moral integrity and commitment to good care. Furthermore, nurses who had faced challenging situations very often were statistically significantly more morally responsible than nurses who had faced challenging situations sometimes or only seldom (Table 6). Also previous studies have shown that encountering ethically challenging situations enables nurses’ to identify and reflect on their values which strengthens their moral courage. 20
Socio-demographic factors that were not statistically significantly associated with nurses’ moral courage were nurses’ age, work experience, highest degree, working department, and participation in activities related to ethics.
Discussion
This study described nurses’ self-assessed level of moral courage and examined its association with their socio-demographic factors. Overall, nurses considered themselves to be morally quite courageous. Ethical knowledge base and encountering situations requiring moral courage were positively associated with nurses’ moral courage.
Nurses’ level of moral courage
Nurses’ fairly high level of moral courage was not a surprising finding, because moral courage is an admired and appreciated attribute and probably everyone would like to consider themselves to be morally courageous.43,44 And there is always a risk of response bias in subjective evaluation because a self-assessment instrument allows the response to be adjusted unconsciously to a socially desirable level. 45 Also, to achieve a reliable assessment, understanding the complex concept of moral courage and behavior 28 is essential and that may vary between nurses, needing further investigation.14,45,46
Particularly, nurses’ courage focused on the patient’s humane and dignified encounter as the center of care, and on honesty as moral integrity. Respect for the patient and defending it was central; nurses dared to commit to confidentiality, honesty, and advocacy for the patient. Respect for human dignity is a core ethical principle which guides nurses’ action. 47 The principle includes values such as confidentiality, honesty, and the promotion of individuality. 48 Thus, nurses who have internalized the values and principles of nursing are likely to be committed to them and courageous to act according to them. 14
Previous studies indicate that nurses’ moral courage is manifested in a desire to protect patients and defend their rights.10,13,17,19 It becomes visible as actions in accordance with one’s own values, such as telling the truth19,24 and intervening in the shortcomings of the care environment.14,17,23,44 The nurse’s personal qualities, such as empathy, 21 honesty, 19 perseverance,13,15 and sensitivity to perceive the patient’s vulnerability 11 have been found to promote moral courage.
The lack of moral courage was associated to interfering with other professionals’ behavior, fear of other professionals’ opinions and attitudes toward the nurse herself, and resorting to conventionalism in ethical decision-making. Earlier research has shown that nurses’ ethical decision-making is conformist, nurses feel themselves insecure and that they are not involved in the decision-making49,50 manifesting as moral distress and lack of moral courage.14,20,51,52 Furthermore, within the nursing profession, collegiality is an important value for many. In some situations, it can be distorted in such a way that one does not want to question a colleague’s actions or ideas. 53 Based on previous research, intervening in unethical behavior can be influenced by several factors.14,22,23 For example, nurse’s own assessment of the severity of harm to the patient, their personal feeling of uselessness, 23 or interfering with another person’s activities may be perceived as difficult, and remaining silent may be desired to avoid conflicts.23,24 Whistle blowing as a form of moral courage can have a number of adverse consequences, such as criticism, bullying, or discrimination. 8 However, it should be noted here that the lowest levels of moral courage did not indicate clear lack of moral courage. For example, nurses’ ethical and responsible action during the present global Covid-19 pandemic in taking care of their patients at the same time risking their own health and even life manifests nurses’ generally morally courageous action.54,55
Factors related to moral courage
Education in ethics, including both formal and informal learning methods, was one of the strongest factors associated with moral courage, its value in strengthening nurses’ moral courage should not be neglected. The outcome affirms the notion that moral courage is a personal quality and a virtue that can be learned and developed. 4 Also previous studies have reported that ethical decision-making and moral courage as a part of it can be taught and learned.26,27
Another important association concerned frequency of facing situations requiring moral courage at work which seemed to increase moral responsibility and commitment to good care. Similar results have been reported also in previous studies.18,20,25,26,56 Also, according to Aristotle, virtues must be constantly practiced and developed. An image of a brave person is formed when she repeatedly acts courageously. 4
Teaching moral courage and facing morally challenging situations may be effectively combined in the ethics education using multiple methods in teaching such as simulations and vicarious learning, 57 digital stories, 26 ethics workshops, 58 and narrative writings. 59 Based on previous research, reflecting on ethical problem situations in the work team is important and promotes learning20,25,26,56 and various safe practical exercises and simulation instructions contribute to the development of nursing students’ ethical competence.18,25,26,42 Model learning is also important for the development of nurses’ moral courage.12,17,20,23 It is suggested, that ethics education should be eclectic 60 and continue beyond graduation. 56
As to associations between moral courage and socio-demographic variables, women appeared to be more compassionate and more genuinely present than men. This finding should be interpreted with caution. Just a minority of participants in this study were male providing too small a sample to be representative of the male gender. Thus, such conclusion that women are generally more compassionate and truly present than men cannot be drawn from this finding. Larger samples and multidisciplinary approach including psychological research would be needed to examine the differences in characteristics between genders in more detail. Also, previous studies have indicated that gender does not appear to be a significant background factor to nurses’ moral courage.12,17,20
Assistant ward managers were more morally uncompromising than staff nurses. There were no significant differences between the other work roles. Assistant ward managers typically work at the interface between administrative tasks and clinical nursing forcing them to have an insight into the ethical quality of care and taking wider responsibility. Therefore, assistant ward managers may be more accustomed to interfering with another person’s actions and to see and raise ethical issues into the debate. 61
Nurses’ age, work experience, highest degree, working department, and participation in activities related to ethics were not related to their self-assessed moral courage level. However, these findings are inconsistent with some previous research findings.22–24
In studies concerning nursing students, short work experience has been found to be a debilitating factor in moral courage. Student nurses’ have reported a perceived lack of appreciation and sense of not being qualified to attend moral debate in work community, which causes them to remain silent.20,22,23 However, nurses’ older age has actually been found to be a debilitating factor in willingness to report on inadequate acts of their colleagues and risk their own, usually already well established position in the work community. 24
Higher educational level has previously been associated with a more positive attitude toward bringing an ethical problem for discussion in work community despite the risk of negative consequences. 24 Also, a higher education level tends to strengthen the position in a work community and may boost persons’ self-confidence to act bravely.22,23 However, our findings did not confirm these findings and more research is needed.
Interestingly, in this study, participation in activities related to ethics was not a significant factor on moral courage although person’s ethical activity in form of self-study was associated with moral courage. Whether the finding is a consequence of lack of supply or opportunities in participation in ethical activities would need further research.
Limitations
A relatively low response rate (34.2%) limits the generalization of the results. In future survey studies, attention should be paid to the rigor of data collection. Furthermore, the data were collected from a single hospital offering tertiary level care, but comprised a representative sample of nurses working in various professionally and ethically demanding nursing care environments. The risk of the social desirability response bias should be acknowledged in relation to self-assessment instruments. 45
Implications and further research
Education was significantly related to enhancement of nurses’ moral courage. Consequently, further research of moral courage from the viewpoint of education is important and it should cover both basic and continuing nursing education. Educational research should focus on evaluation of teaching contents, teaching methods, and evaluation itself. Target groups should include nursing students, nurse educators, and practicing nurses. Various educational intervention studies and their impact on and efficiency in developing nurses’ moral courage at all organizational and educational levels should be considered in addition to measuring the level of moral courage.
Also, nurse leaders’ role in enhancement of practicing nurses’ moral courage was found important. Nurse leaders’ moral courage and its role in good ethical leadership needs exploring including nurse leaders’ knowledge base concerning the concept of moral courage, and how courageous they are as leaders and in their role as role models.
Moral courage was also related to nurses’ ethical sensitivity to observe situations needing moral courage. Various factors in the process involving the movement from an observation of ethical problem into action needs exploring. 28
Measuring nurses’ moral courage could be extended also to various nursing environments and other professional groups in healthcare team, because moral courage manifests itself differently in different environments and care contexts.10,11,28
Furthermore, ethical decision-making and moral courage as a part of it does not concern only nurses and nursing profession, but all professionals and participants involved in ethical situations. Nurses’ ethical decision-making and its relation to nurses’ moral courage in the multi-professional healthcare team should be further studied, since nurses often feel themselves suppressed in these situations, and they need moral courage to speak out their opinions in ethical questions. 23 An open and multidisciplinary approach to research in moral courage would be useful bringing in a larger perspective and depth to our understanding of moral courage in nursing and in healthcare environment in general.
Conclusion
Nurses assessed themselves to be morally quite courageous. Their level of moral courage was related most importantly with multifaceted ethics education, good ethical knowledge base, and frequency of encountering situations requiring moral courage. Personal activity and interest in ethical issues as well as ethics education seems to be factors that promote nurses’ moral courage. Consequently, attention should be paid to both basic and continuing ethics education to maintain and develop nurses’ moral courage as part of their ethical competence both in theoretical and practice contexts. Future studies should focus on other contextual factors in nursing environment related to moral courage.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.