
Abstract
Background
Professional misconduct undermines safe and quality care; however, little is known about its nature and influential factors.
Aim
This study aimed to explain the factors influencing professional misconduct in nurses.
Research Design
This qualitative study was conducted using the conventional content analysis method.
Participants and Research Context
Data were collected using semi-structured interviews with 19 nurses working in the hospital selected through a purposeful method and analyzed by Graneheim and Lundman approach.
Ethical Considerations
The ethics committee of Tehran University of Medical Sciences approved this study with the ethics code IR.TUMS.FNM.REC.1400.187. Informed consent was obtained from all participants. Participants were assured of confidentiality.
Findings
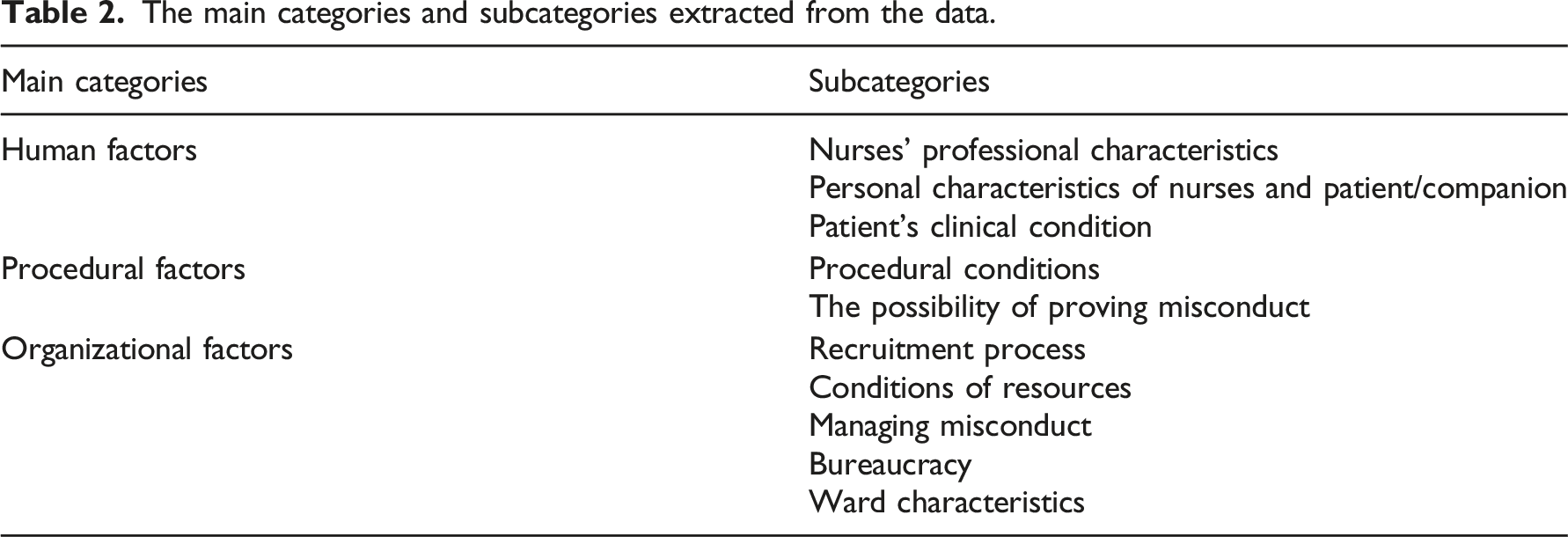
Factors influencing professional misconduct by nurses were categorized into three main categories: human factors (nurses’ professional characteristics, personal characteristics of nurses and patient/companion, patient’s clinical condition), procedural factors (procedural conditions, possibility of proving misconduct), and organizational factors (recruitment process, conditions of resources, managing misconduct, bureaucracy, and ward characteristics).
Conclusion
This study assists in explaining the factors influencing professional misconduct by nurses. Therefore this study’s results can help managers and planners develop interventions to prevent and correct factors that contribute to misconduct and strengthen factors that prevent misconduct in order to ensure quality and safe patient care.
Introduction
Professional misconduct undermines safe and quality care; however, little is known about its nature and influential factors. If we tend to reduce professional misconduct by nurses and its harmful consequences, we need to first identify its influential factors. Therefore, we used a qualitative approach and interviewed nurses to explain their understanding of factors influencing professional misconduct.
Background
Professional misconduct is a heterogeneous and complex phenomenon that includes a variety of illegal, unprofessional, or unethical acts and is a deviation from benefiting the client and society. 1 In other words, professional misconduct includes what is created due to irresponsible and unqualified care of health workers and puts patients at risk and harm. 2
Due to insufficient resources and the vulnerability of service recipients, professional behavior is of critical importance in the healthcare sector. 3
Poor and ineffective care is a global phenomenon; in some studies, the rate of exposure to professional misconduct, poor care, or unsafe practice by nurse colleagues or other healthcare workers was reported as 42, 31, 66, and 88% in different countries.2,4–6
Professional misconduct by nurses is associated with negative consequences such as ineffective health care, 7 increased burden of disease, jeopardizing patient safety, and wasting scarce resources. 8 Professional misconduct also undermines public trust in healthcare professions and institutions. In this way, it is important for regulators to identify professional misconduct and its influencing factors in order to protect patients and safeguard public trust. 3
In some studies, underlying factors of professional misconduct have been reported to arise from the “bad apple” or “bad barrel” hypotheses. The “bad apple” hypothesis considers professional misconduct to result from the actions of unruly individuals who act for their benefit and against professional norms and standards. On the other hand, based on the “bad barrel” hypothesis, professional misconduct occurs due to underlying causes, including culture, incentive system, management methods, and ineffective structures.1,9 Another study introduces four approaches, including individual differences, social learning, ego depletion, and ecosystem as the underlying factors of misconduct. 10 It seems that healthcare workers’ professional incompetence in providing care is one of the important issues that can expose them to professional misconduct. Professional competency includes all the primary abilities nurses need to perform their role.11,12 However, graduates often lack the required competency to begin their careers. 13
There is limited evidence about the factors influencing professional misconduct. Although the few studies in this field have provided valuable insight, they have been mainly conducted quantitatively harm2,4–6,14–16 using researcher-made questionnaires in different contexts.
Furthermore, considering nurses' critical role in healthcare systems, their perceptions and experiences of the factors influencing professional misconduct have yet to be considered. Accordingly, explaining nurses' perceptions and perspectives through a qualitative approach is beneficial in explaining the factors influencing professional misconduct. It also provides the basis for improving the quality of care and patient safety by developing existing knowledge. Therefore, this qualitative study was conducted to explain the nurses’ perception of the factors influencing professional misconduct.
Methods
Research design, context, and participants
This qualitative study was conducted using the conventional content analysis method.
Demographic data of the participants.
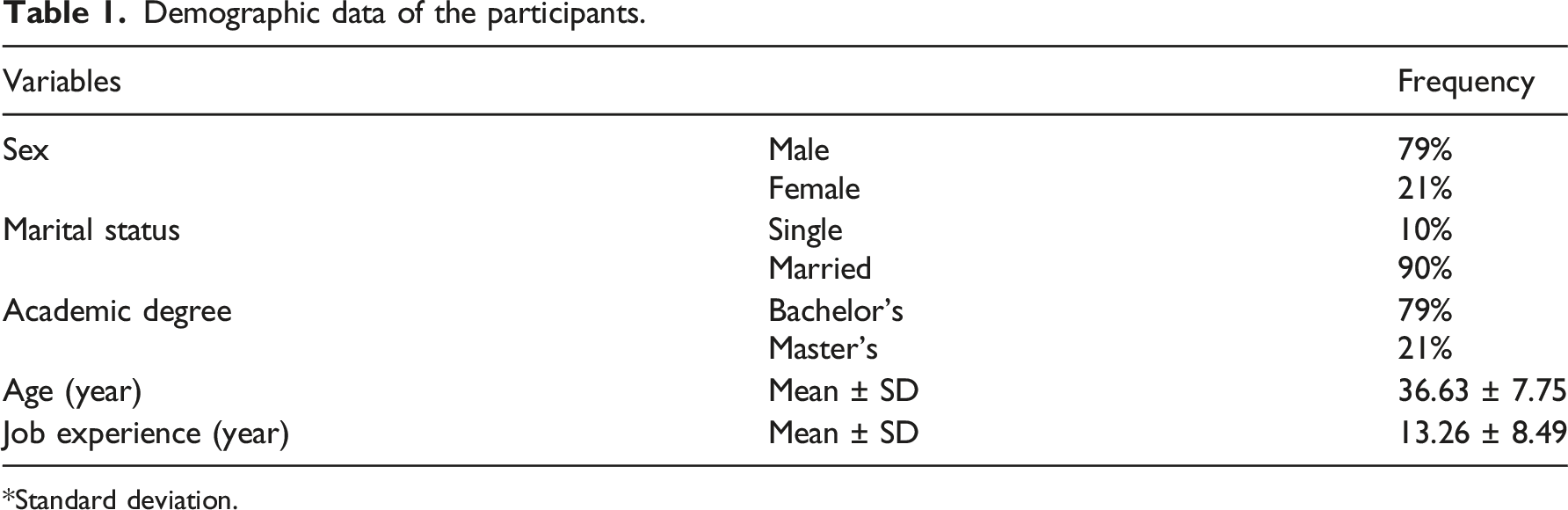
*Standard deviation.
Data collection
Interview questions were prepared using the expert opinions of the research team and previous studies.17,18 Data were collected through semi-structured in-depth interviews from February to August 2022. The interview commenced with personal profile questions followed by more specific questions related to the purpose of the study. The participants were asked: “What factors influence the professional misconduct you have experienced?” “What factors can prevent professional misconduct? Please explain?” Exploratory questions were used to clarify the issue further and obtain deep and rich information. The interviews were voice-recorded with the participants' permission. A total of 22 interviews were conducted with 19 participants at their workplace as was coordinated. The interviews lasted for 63 min on average.
Data analysis
The conventional content analysis method of Graneheim et al. (2017) was used to analyze the data. 19 Content analysis is a qualitative research method 20 that aims to organize and extract meaning from the collected data and draw realistic conclusions. 19 In all stages of the study, we made an effort to follow the items of The Consolidated Criteria for Reporting Qualitative Research (COREQ). This checklist indirectly improves the trustworthiness and reliability of interview-based studies. 21
To this end, within 24 h after each interview, the contents recorded were transcribed verbatim in Word software ver.13 and read several times. Consequently, meaning units were identified and coded. The codes were then compared for similarities and differences, and similar codes were categorized into a subcategory. In the end, the subcategories were compared and merged to form the main categories. Data collection and analysis were performed simultaneously. Data collection continued until data saturation, when no new category appeared. 22 MAXQDA10 software was used for data management.
Trustworthiness
To ensure data trustworthiness, criteria proposed by Guba and Lincoln were used to check scientific accuracy in qualitative research, including credibility, dependability, confirmability, transferability, and authenticity, during the study. 22
Ethical considerations
The ethics committee of Tehran University of Medical Sciences (TUMS) approved this study according to the Code of Ethics IR.TUMS.FNM.REC.1400.187. Informed consent was obtained from all the participants after explaining the study objectives. Participants were assured of confidentiality and anonymity of information. The time and location of the interviews were determined in consultation with the participants, and permission was obtained to record the interviews.
Findings
The main categories and subcategories extracted from the data.
Human factors
The findings showed that some factors influencing misconduct were human-related. This category contained three subcategories:
Nurses’ professional characteristics
Nurses’ inadequate knowledge and awareness of job descriptions, professional ethics, experience, motivation, and professional commitment, and the gap between theory and practice may contribute to professional misconduct. On the other hand, nurses’ professional commitment and high knowledge and skill can play a preventive role. “When the doctor orders a high-potassium gavage for a patient, a nurse won’t perform it if she/he doesn’t know the complications of high or low potassium.” (P. 11)
According to the participants, conforming to wrong behaviors executed by many employees was one of the critical factors contributing to misconduct. “Experienced colleagues combine several antibiotics and infuse them simultaneously, and novice nurses learn from them.” (P. 10)
Personal characteristics of nurses and patient/companion
Nurses’ personality traits such as indolence, impatience, low resilience, carelessness, irresponsibility, fear of being humiliated, false self-confidence, especially in nurses working in the ICU, lack of empathy, and weak work conscience might contribute professional misconduct. According to the participants, these characteristics are more commonplace in the new generation. “To abandon care and reduce their responsibility and workload, some colleagues encourage patients to get discharged on personal consent without careful assessment.” (P. 1)
Moreover, the participants stated that other personality traits such as moral sensitivity, honesty, sense of responsibility, patience, empathy, caution, respect for human dignity and humanity, a sense of duty toward providing quality care, feeling guilty for misconduct, and fear of legal and financial consequences and others’ reprimand and reaction could prevent professional misconduct by nurses.
Besides, they acknowledged that nurses’ belief in the patient’s involvement in the disease occurrence, such as suicide attempts or being hysterical, the belief in the futility of care, in cases such as caring for or resuscitating terminally ill patients or the elderly, or caring for COVID-19 patients, especially in the early stages of disease outbreaks, could be significant factors contributing to professional misconduct. “In my idea, if a 90 year-old patient with a history of diabetes and kidney and liver failure dies, it’ll be better for him and his family. What if this patient survives with so many complications?” (P. 10)
According to the participants’ perspective, other factors, such as the motivation to be transferred to better or non-clinical wards and embellishment to avoid facing legal issues, might create a foundation for professional misconduct.
Some participants believed professional misconduct was related to nurses’ individual-social characteristics, such as gender, work experience, employment status, religious beliefs, and relationships. Most participants had witnessed a higher rate of misconduct in male nurses and believed that the type of misconduct varied across genders. “Men are more negligent; they take everything more easily. I remember an old man in the ward who said to his wife: ‘I hope today’s nurse is female because they are more careful’.” (P. 13)
Other participants’ experiences indicated that inexperienced nurses, due to less clinical experience, and experienced staff, due to conforming to their peers’ misconduct, and high job security, were prone to misconduct. On the other hand, some inexperienced staff committed less professional misconduct due to their high motivation to attract positive opinions and have better working conditions. They also stated that nurses with no organizational attachment were less committed to the organization and prone to professional misconduct. “We had a colleague who worked overtime. He wasn’t careful at all in implementing medication orders and antibiotics. Well, he didn’t really care what the officials thought or how they reacted.” (P. 11)
The participants pointed to nepotism and intimate relationships or conflict between colleagues as other factors influencing professional misconduct. “One of the colleagues always leaves the shifts earlier than expected because she’s certain that the matron won’t criticize her.” (P. 6)
Most participants believed some professional misconduct was rooted in nurses’ dissatisfaction, possibly due to various factors, including shift arrangement, long shifts, compulsory overtime, insufficient support, and low or delayed payments. “I work overtime today, but I’ll be paid nine months later, so there’s no motivation to work.” (P. 2)
According to participants, similar to other people, nurses have a series of background problems such as economic, psychological, family problems, addiction, and difficulty commuting to work, which could influence their professional behavior. “We have a colleague who often has arguments with her husband, so she’s usually distracted.” (P 8)
According to them, previous experiences, such as an addicted spouse, might also contribute to misconduct. “A colleague of us who was separated from her addicted husband was aggressive and mistreated every addicted patient she met.” (P. 13)
Moreover, the participants stated that patients’ and companions’ personality traits, such as aggression, rage, resistance to certain treatments or care, including serum or specific breathing masks, or observing bed rest, lead them to professional misconduct. “There was an old male patient with COVID-19. This patient was very resistant to use an NIV (non-invasive ventilation) mask, so the nurse beat him and shouted at him.” (P. 17)
On the contrary, the patient’s and companions’ high awareness and demands could prevent nurses’ professional misconduct. “One of the diabetic patients’ wife was well-informed; she asked why we didn’t check her patient’s blood sugar; his blood sugar got high. My colleague said he didn’t check patients' vital signs or blood sugar unless they asked for it.”
Furthermore, participants admitted that some nurses humiliated patients with particular cultures and dialects and did not provide quality care. Nurses might also commit misconduct toward the elderly due to a lack of motivation to provide optimal care or toward babies who cannot communicate and defend themselves. “An elderly patient in the inpatient ward was ridiculed because of his different dialect. He said that nurses laughed at him and made fun of him; they said they wouldn’t answer him if he didn’t speak Farsi.” (P. 17)
The patient’s clinical condition
The participants stated that patients with a decreased level of consciousness who lacked the power to complain or defend themselves, or patients with behaviors caused by changes in the level of consciousness, such as aggression and delusions, were victims of nurses’ misconduct. Obese patients with inaccessible veins, addicts, end-of-life patients, or those with poor prognoses or infectious diseases such as tuberculosis, AIDS, hepatitis, and COVID-19 were sometimes subjected to professional misconduct by nurses due to their clinical conditions. “A colleague didn’t inject packed cell to the critically ill and unconscious patient with a history of addiction, hepatitis, and AIDS and threw it away.” (P. 10)
Procedural factors
Other factors influencing professional misconduct were those related to the procedure. This category was divided into the following subcategories:
Procedural conditions
The participants acknowledged that the procedural conditions, such as the difficulty of gavage of some pills, the rare side effects of the simultaneous injection of some drugs, or, on the contrary, the prevalent side effects of some drugs, such as vancomycin, the repetitiveness of some measures such as controlling vital signs or some conditions such as blood transfusion or patient transfer were factors influencing professional misconduct by nurses. “In such a busy emergency room, we don’t administer antibiotics like Vancomycin, which has common side effects, because if it causes complications, we have to follow it up, but we usually administer Ceftriaxone because it doesn't cause any trouble.” (P. 16)
The possibility of proving misconduct
According to participants’ statements, the possibility of proving misconduct could be the basis for committing or not committing it. “One of our colleagues said if the patient’s blood sugar was, for example, 800, record it as 200 in the file; who will know that?” (P. 10) “We definitely do all the lab tests carefully because they are documented, but in the case of medication, because it can't be proven, we do whatever we are able to.” (P. 14)
Organizational factors
Some factors influencing nurses’ professional misconduct were related to the organization. This group of factors included the following subcategories:
Recruitment process
The participants acknowledged that recruiting individuals with low interest and motivation to the nursing profession, disregarding clinical professional issues, and changing nurses’ employment status regardless of professional behavior were important factors influencing professional misconduct, especially in inexperienced nurses. “Nurses who are hired all at once permanently do not observe professional behavior very much.” (P. 14)
Conditions of resources
Inadequate facilities and treatment equipment, such as dressing and urinary catheterization devices, sphygmomanometers, glucometers, arterial line devices, and beds, were among the factors leading to misconduct by nurses. “The equipment isn’t enough. Sometimes there’s some equipment, but it’s broken down.” (P.16)
Furthermore, they mentioned inadequate nurse staffing and time, fatigue due to work burden and high workload, and a low nurse-to-patient ratio as other factors. “In this internal ward, each nurse is responsible for ten patients. Nurses here are the busiest staff; we don’t have a chance to see some patients at all, which is a disaster.” (P. 10)
Managing misconduct
The participants stated that the system’s inappropriate behavior, leniency, improper reaction, and discrimination in dealing with some offending nurses were among the organizational factors influencing professional misconduct by nurses. They considered timely detection of misconduct, investigating the root causes of the incident, addressing the performer decisively and appropriately, and paying attention to misconduct without questioning the person’s character as important factors in preventing professional misconduct. “I’ve experienced many times; the officials don’t specifically deal with the one who commits misconduct.” (P. 12)
Monitoring nurses’ professional practice is also a crucial and influential issue in preventing professional misconduct by them. The participants believed that the lower prevalence of misconduct during the hospital inspection and accreditation programs and more cases in the evening and night shifts and on holidays when there was less supervision proved it. “There was a supervisor who asked us for details very carefully. Low levels of misconduct occurred because she was strict.” (P.15)
Bureaucracy
According to the participants, prioritizing comprehensive reports and completing various forms over clinical care by officials could also lay the groundwork for professional misconduct by nurses. “Writing reports is my concern during the whole shift. Nurses have become story writers. So, they’re short of time and have to leave clinical tasks incomplete.” (P. 19)
Ward characteristics
Based on participants’ opinions, the cause, type, and level of misconduct varied in different wards. Psychiatric, pediatric, infectious disease wards, ICUs, and emergency departments were among the wards where the higher level of misconduct occurred for various reasons. The distinct conditions of each ward, including facilities and equipment, number and type of patients, workload, ward management, and the presence or absence of companions, could influence professional misconduct. “In the ICU, the patients are usually not conscious and have no companion. For example, when a patient is hungry but can’t say it, a nurse with a low conscience may not administer one gavage dose.” (P. 11)
In teaching hospitals, multiple visits by medical students of different levels and frequent changes in the physician’s orders were the basis for professional misconduct. “Sometimes the residents make a new order every fifteen minutes or half an hour. I have to do the more important ones.” (P. 16)
Discussion
The results of this study revealed the role of numerous human, procedural, and organizational factors in the occurrence and prevention of professional misconduct by nurses.
In this study, one of the factors influencing misconduct by nurses included the level of professional knowledge, experience, and commitment, referred to as professional competence. Similarly, a study showed an inverse relationship between a nurse’s professionalism and the possibility of malpractice. 23 Moreover, in a systematic review, inappropriate nursing competence was introduced as a crucial factor that contributes to missed nursing care. 31 Empowering the nurses is a factor in improving patient safety culture. 24 Moreover, continuous and specialized learning is essential to professional commitment in nursing. 25 It can be concluded that one of the crucial factors preventing misconduct is the promotion of professional competency through holding related workshops.
Another professional characteristic contributing to the misconduct was conformity. In a study, professional blindness or learning erroneous behaviors from others was mentioned as one of the factors in rationed nursing. 17
In line with this study, nurses’ personal characteristics, such as conscientiousness, resilience, motivation, and satisfaction, have been reported in other studies as critical factors related to professional practice and the quality of care provided.26–30 In another study, poor accountability was considered the most significant behavior related to unsafe practices. 6 Therefore, healthcare organizations can provide satisfaction and prevent professional misconduct by improving existing conditions and strengthening motivations.
Regarding beliefs, in line with the present study, in a meta-analysis, nurses had low empathy and a negative attitude toward patients who self-harmed. 32
While the female nurse population is, generally and in studied environments, higher than male nurses, according to the data in this study, professional misconduct was more frequent in male nurses. In line with the present study, missed nursing care and counterproductive work behaviors were reported to be high among male staff in other studies.33,34 However, in another study, no difference was reported between gender and unprofessional behaviors. 18 Similarly, in a study, 87% of nurses considered religious practices effective in their moral decision-making. 35 Background problems, including family, physical, mental, economic, and addiction problems, were influential factors in the occurrence of professional misconduct. Few studies were found in this regard due to nurses' challenging work environment and conditions; therefore, it is recommended to monitor nurses' health to prevent misconduct periodically.
Although identifying and modifying inequality in providing health services to patients is one of the characteristics of patient advocacy in nursing, 36 in this study, some patient-related conditions, including the clinical condition or patient’s/companion’s personal characteristics, were identified as the source of professional misconduct.
Consistent with the present study, patients’ aggressiveness and refusal/demand to receive care was among the critical factors in missed nursing care. 17 Organizations can help reduce misconduct by informing patients of their rights, surveying them about the quality of services received, particularly after discharge, and ultimately applying their opinions to the personnel reward and punishment system.
In this study, age was introduced as one of the patients’ characteristics that could be the source of professional misconduct. The patient’s age is a characteristic that leads nurses even to provide futile care. 37 A study reported the age discrimination experience in healthcare centers in 30% of the elderly and 47% of the students. 38 In another study, the prioritization of medical care and treatment based on the patient’s age was reported. 39 Teaching ethics to nursing students and nurses can help create a positive attitude toward old age.
Regarding the patient’s clinical condition, in line with the present study, ethical issues related to the end-of-life stage were the most frequent subjects in a review. 40 In this study, the nature of the disease emerged as one of the underlying factors of professional misconduct. In another study, nurses’ fixed mentalities were influential in their care for patients with mental disorders. 41 In another study conducted on COVID-19, nurses felt less responsible in responding to patients’ urgent needs, and as a result, patients did not receive optimal care. 42
In this study, some factors influencing professional misconduct by nurses were related to the procedure. The procedural conditions refer to measures that may be more challenging to implement and require a large amount of time, precision, and closer monitoring. The difficulty or impossibility of proving some types of misconduct is one of the crucial factors influencing it and even its discovery and management. This factor might be more noticeable in some contexts with less technological progress. No study was found in this regard.
In this study, organizational factors were also identified as significant factors affecting professional misconduct. Insufficient nurse staffing is a crucial challenge for healthcare systems around the world 43 and a chronic challenge in Iran. 44 Rationed nursing care is associated with the lack of resources. 17 Studies show a direct relationship between insufficient workforce and missed nursing care.31,45,46 In addition, the patient-to-nurse ratio is an important factor in job dissatisfaction, quality of care, and patient safety. 47 Inadequate human resources do not allow nurses to provide optimal care, often leading to ethical dilemmas such as eliminating or rationing care. 40 In a cross-sectional study, the high workload was identified as the most significant organizational factor related to unsafe practice. 6 In addition to the condition of nurse staffing, the recruitment process is another organizational factor in the occurrence or prevention of professional misconduct. In the literature review, no evidence was found to support or oppose it.
The equipment condition was one of the factors influencing the misconduct. In a study, the most critical factor influencing missed nursing care in Iran was the unavailability of medicines needed for patients. 48 Improvement of human resources and provision of sufficient resources is suggested in order to improve the quality of nursing care. 49 The organization can take beneficial measures to prevent misconduct by providing, managing, and optimizing resources.
Managing misconduct was also another critical and influential organizational factor. One of the effective factors in improving nurses’ professional ethics is the appropriate support system and effective encouragement and punishment system. 50 According to studies, injustice in the workplace affects the employees’ commitment to the organization, their profession, and performance.51,52 Organizational justice and unethical behavior by nurses are correlated. 53 In the studies conducted in Iran and Egypt, organizational justice perceived by nurses was reported to be lower than average, which was associated with deviance in the work environment.54,55 Considering the effect of organizational justice on the quality of care provided to patients, nursing managers can help maintain and create a healthy and supportive work environment for nurses and improve care quality by planning to reduce discrimination and promote organizational justice.
Supervision is a significant issue in professional misconduct by nurses. Lack of regular staff evaluation has been mentioned as one of the factors of missed nursing care. 17 There is a relationship between abusive supervision and counterproductive work behavior.56,57 Clinical evaluation through the appropriate assignment of nursing officials and precise and sufficient supervision by vigilant, specialized, and proficient supervisors with sufficient clinical experience and at different times of the day and night can reduce the extent of misconduct, particularly in novice nurses. Although 24 h monitoring of all procedures and nurses is impossible, installing cameras while maintaining the patient’s privacy might be helpful.
Another underlying factor of professional misconduct in this study was bureaucracy. One of the challenges of documentation in nursing is the shortage of time and increased patient admission. 58 In line with the present study, increasing bureaucracy has been mentioned as one of the factors of rationed nursing care. 17 One of the crucial issues in reducing the workload is to alter the report writing process from narration to a checklist.
The ward type is also one of the influential factors in professional misconduct by nurses. The conditions of different wards in different hospitals vary. These differences cause the type and extent of misconduct to be dissimilar. It is worth noting that no study was found regarding the higher occurrence of misconduct in a specific ward.
Limitation
Some participants had doubts about the possible disclosure of their names and institutional information in the study, which was resolved by assuring them about the anonymity and confidentiality of the data. Similar to other qualitative studies, this study is not generalizable, and it is suggested to conduct similar studies with more diverse samples.
Conclusion
The present study revealed the factors influencing professional misconduct by nurses from their point of view using conventional content analysis. The results showed that professional misconduct by nurses was influenced by numerous human, procedural, and organizational factors. Considering that professional misconduct by nurses is influenced by various factors, including nurses’ professional characteristics, nurses’ and patients’ personality traits, patients’ clinical conditions, procedural conditions, the possibility of proving misconduct, the recruitment process, conditions of resources, managing misconduct, bureaucracy, and ward characteristics, failure to monitor and pay attention to these factors identified due to the lack of studies in this field, can have severe consequences on the quality of patient care and safety. Therefore, managers and planners should develop interventions to prevent and modify factors contributing to misconduct and strengthen factors that prevent it in order to ensure quality and safe care for patients.
Footnotes
Acknowledgments
This study is part of a doctoral dissertation in nursing. The research team hereby appreciates the nurses participating in this study and the School of Nursing and Midwifery of Tehran University of Medical Sciences.
Author contributions
Study conception and design: ShV, NDN, and AGh
Data collection: AGh
Data analysis and interpretation: AGh, NDN,LS, ANSh, and ShV
Drafted the article: AGh, NDN,LS, ANSh, and ShV
Critical revision of the article: NDN,LS, ANSh, and ShV
Approved the version to be published: AGh, NDN,LS, ANSh, and ShV
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.