
Abstract
Abstract
Introduction: Maternal and child health (MCH) benefit schemes were introduced to increase institutional deliveries, to reduce out of pocket expenditure, to provide quality care and nutrition to mother and baby and thereby reduce maternal mortality rate and infant mortality rate.
Objective: To assess the awareness and estimate the uptake of benefits regarding various MCH benefit schemes among study participants.
Methodology: A cross-sectional study was conducted at district hospital, Mangaluru, Karnataka, India, among 250 antenatal women and postnatal mothers. They were interviewed using a semi-structured–validated questionnaire. Data were analysed using Statistical Package for Social Science version 11.5.
Result: Awareness for scheme varied, ranging from 94 per cent for Integrated Child Development Service and 0.8 per cent for Rashtriya Bal Swasthya Karyakram. Major source of information being accredited social health activist (40.41%), most of the study participants had a favourable opinion regarding the benefits of MCH schemes. Maximum uptake was seen for Janani Shishu Suraksha Karyakram (100%); however, none of them availed Prasoothi Araike.
Conclusion: Our study showed that the awareness and uptake for different MCH-related schemes varied. Most of the study participants had a favourable opinion about the benefits of MCH schemes. Since awareness for some schemes were low, efforts should be made to increase awareness regarding all schemes by displaying the information. Uptake can be increased by proper channelising the resources.
Keywords
Introduction
In developing countries like India, maternal and infant mortality is a problem of concern in public health (Datta & Datta, 2013, pp. 33–35; Guin, Sahu, Khare, & Kavishwar, 2012; Manjula, Ravish, & Ranganath, 2016). Sustainable development goals (SDGs) introduced in 2016 aim at reducing global maternal mortality ratio (MMR) to less than 70 per 100,000 live births and to end preventable deaths of newborn and children aged less than 5 years by 2030. It also targets to achieve universal access to sexual and reproductive healthcare services, including for family planning, information and education and the integration of reproductive health into national strategies and programmes (United Nations, 2015).
According to Sample Registration System (SRS) 2017, MMR in India is 174/lakh live births (Government of India [GOI], 2017). According to National Family Health Survey (NFHS-4), infant mortality rate (IMR) in India and Karnataka is 41/1,000 live births and 28/1,000 live births, respectively, and institutional birth rate was 78.9 per cent (GOI, 2015a; Government of Karnataka, 2015). There are 30 million conceptions every year in India, resulting in 27 million births. Only around 50 per cent of deliveries are conducted by trained personnel, which includes doctor (35%). Rest of the deliveries are assisted by trained birth attendants (37%), and even by friends or relatives (16%) (Johnson et al., 2015).
Most of the maternal mortalities are due to pregnancy-related complications such as haemorrhage, infection, pregnancy-induced hypertension and unsafe deliveries (Goyal, Singh, & Munday, 2014). These can be prevented to a great extent by institutional deliveries, skilled attendants and quality care to antenatal women (ANC) and postnatal mothers (PNC) in public health facilities which also helps in reducing their out of pocket expenditure (OOPE) (Goyal et al., 2014; Randive, Sebastian, De Costa, & Lindholm, 2014; Rose et al., 2007).
MMR and IMR reflects the efficiency of healthcare system and socio-economic affluence of the country (Deshpande, Gadappa, Pagare, Dhaduti, & Andurkar, 2016, Guin et al., 2012). So, the Government of India has made efforts to reduce the high MMR and IMR by promoting institutional deliveries under National Rural Health Mission (NRHM). The number of institutional deliveries has increased from seven lakhs (2005–2006) to more than a crore (2010–2011) after the implementation of maternal and child health (MCH) schemes like Janani Suraksha Yojana (JSY) since April 2005. Following this, many other schemes such as Janani Shishu Suraksha Karyakram (JSSK), Prasoothi Araike, Madilu Kit, Thayi Bhagya Scheme, Anganwadi nutrition supplementation and 108 ambulance service were introduced (Johnson et al., 2015).
This study aims to find out the awareness and uptake of all MCH benefit schemes in coastal South India.
Materials and Methods
A cross-sectional study was carried out among the ANC and PNC attending District Maternity and Child Healthcare Hospital, Mangaluru, Karnataka, India, in the year 2017. Approval from Institutional Ethics Committee was taken, permission was obtained from District Medical Officer and Resident Medical Officer prior to the commencement of study.
Participants were explained the nature and purpose of study in local language and were assured full confidentiality of the information provided by them. Written informed consent was taken from all consenting participants.
Sample size was calculated based on a study done by Johnson et al. (2015), the awareness level was 18.6 per cent (p). By using the formula n = (Zα)2pq/d2, with absolute precision (d) of 5 per cent, n was calculated to be 227, with 95 per cent confidence interval, power of 80 per cent and α-error of 5 per cent. Assuming 10 per cent non-response rate, 250 people were approached. Non-probability convenience sampling was followed to approach ANC and PNC attending outpatient department (OPD) and inpatient department (IPD) on a daily basis. A semi-structured and validated questionnaire was used to interview the participants; questionnaire was developed based on literature review and was content validated. It comprised of following sections: socio-demographic characteristics, obstetric details, awareness, source of information, perception and uptake of various MCH schemes. Socio-demographic characteristics included were age, religion, social group, place and status of residence, education, occupation and socio-economic status was assessed using updated BG Prasad socio-economic classification for 2016 (Khairnar, Wadgave, & Shimpi, 2016).
If participants could tell the name and key benefits under each scheme, they were considered to be aware of MCH schemes. Perception regarding the various MCH benefit schemes was assessed using a 5-point Likert scale, where strongly agree was scored as 5, agree as 4, neutral as 3, disagree as 2 and strongly disagree as 1. Uptake of various MCH benefit schemes was assessed based on the eligibility, registration among the eligible participants and uptake among the registered participants.
Having a Thayi card was one of the eligibility criteria for some schemes such as JSY, Madilu Kit, Prasoothi Araike. Thayi card is a document recording the details of MCH-related services and contains ANC and PNC details of mother and basic information of the newborn, which is given at the time of registration of the pregnancy.
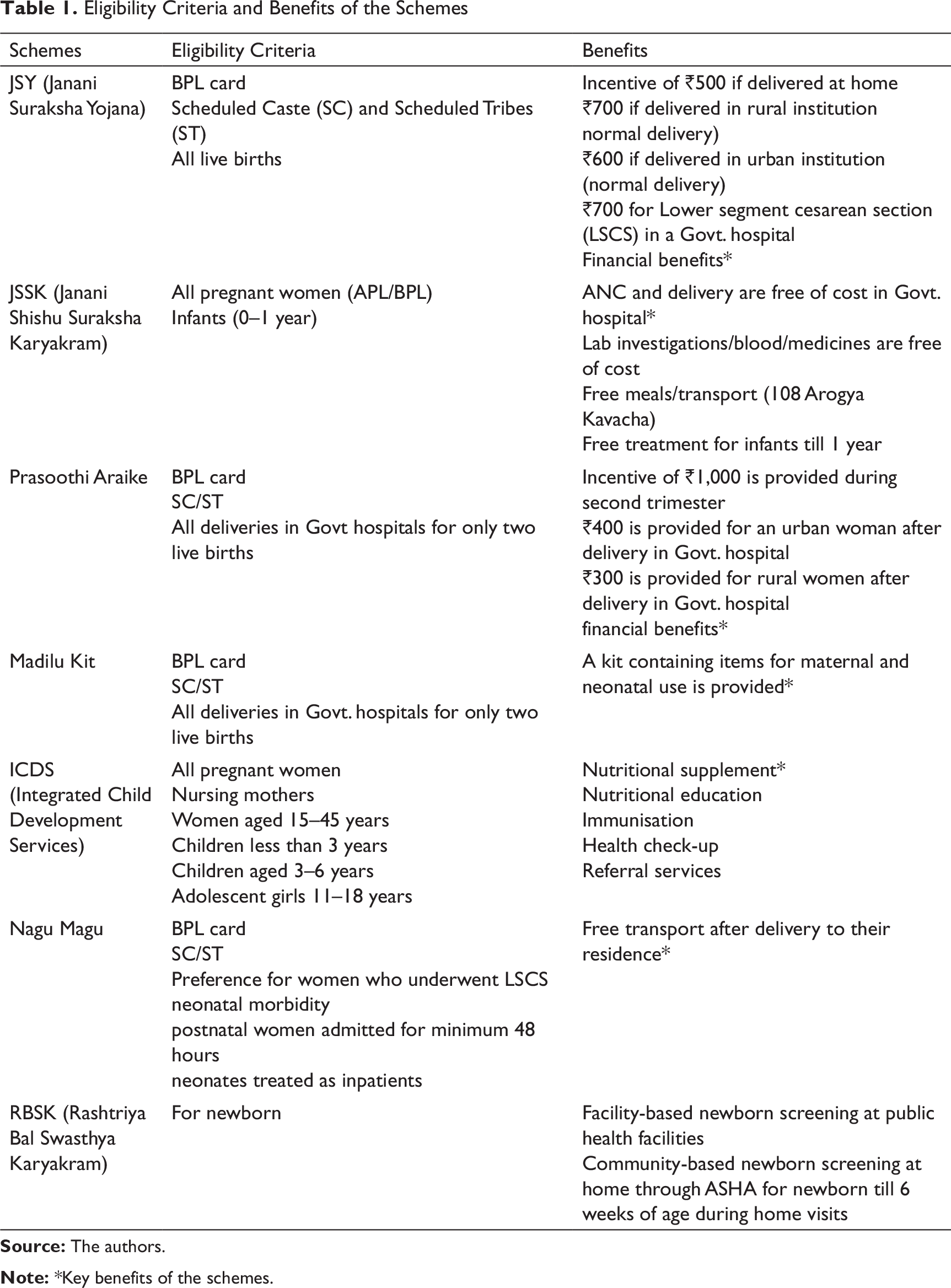
Details of each scheme and the key benefits are available in Table 1 (Government of Karnataka, 2016; Park, 2015).
Statistics and Analysis of the Data
Data were entered and analysed in Statistical Package for Social Science (SPSS) version 11.5. Categorical data were summarised using percentages. Perception was summarised using median and interquartile range (IQR).
Results
Eligibility Criteria and Benefits of the Schemes
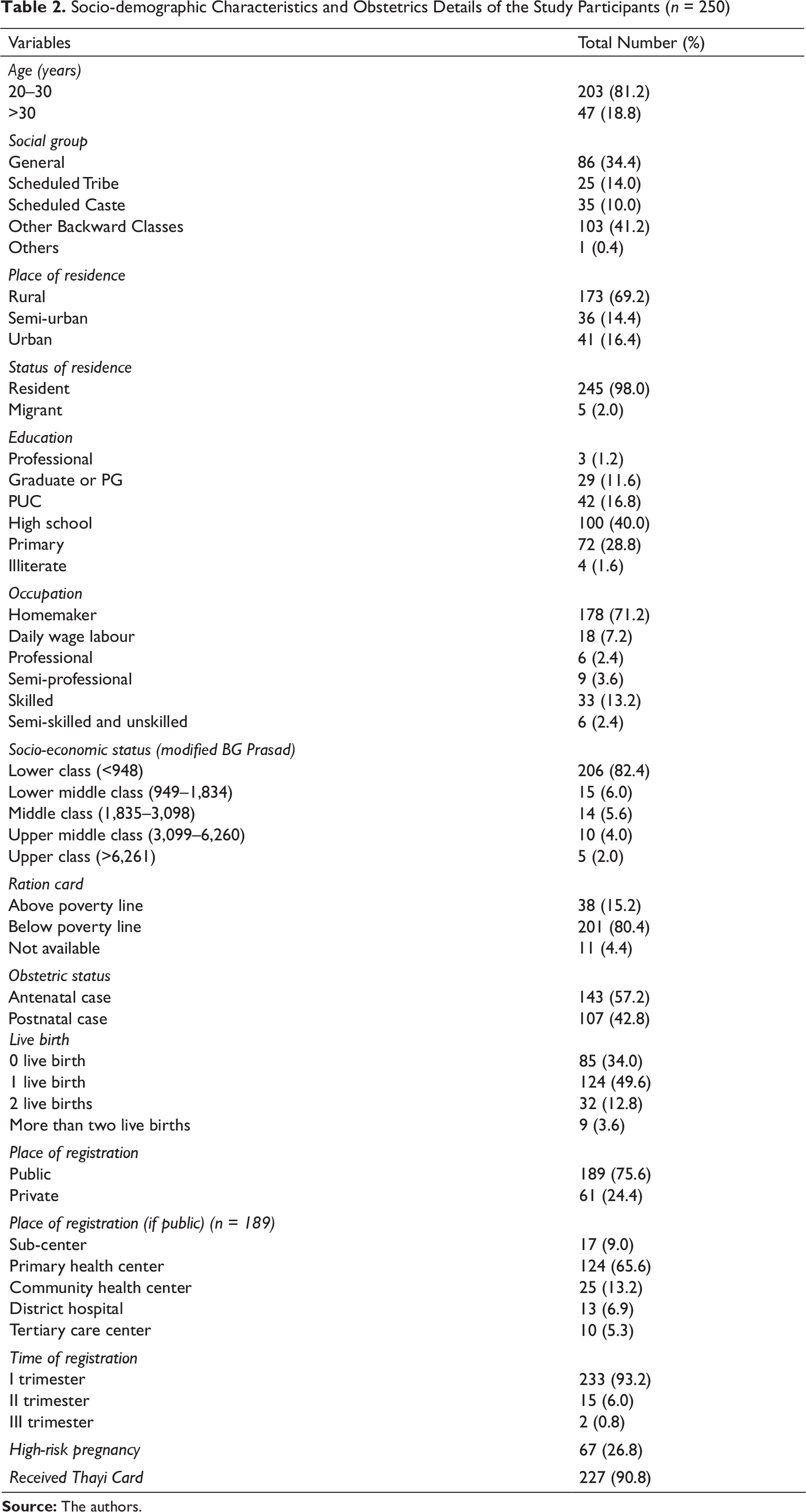
Socio-demographic Characteristics and Obstetrics Details of the Study Participants (n = 250)
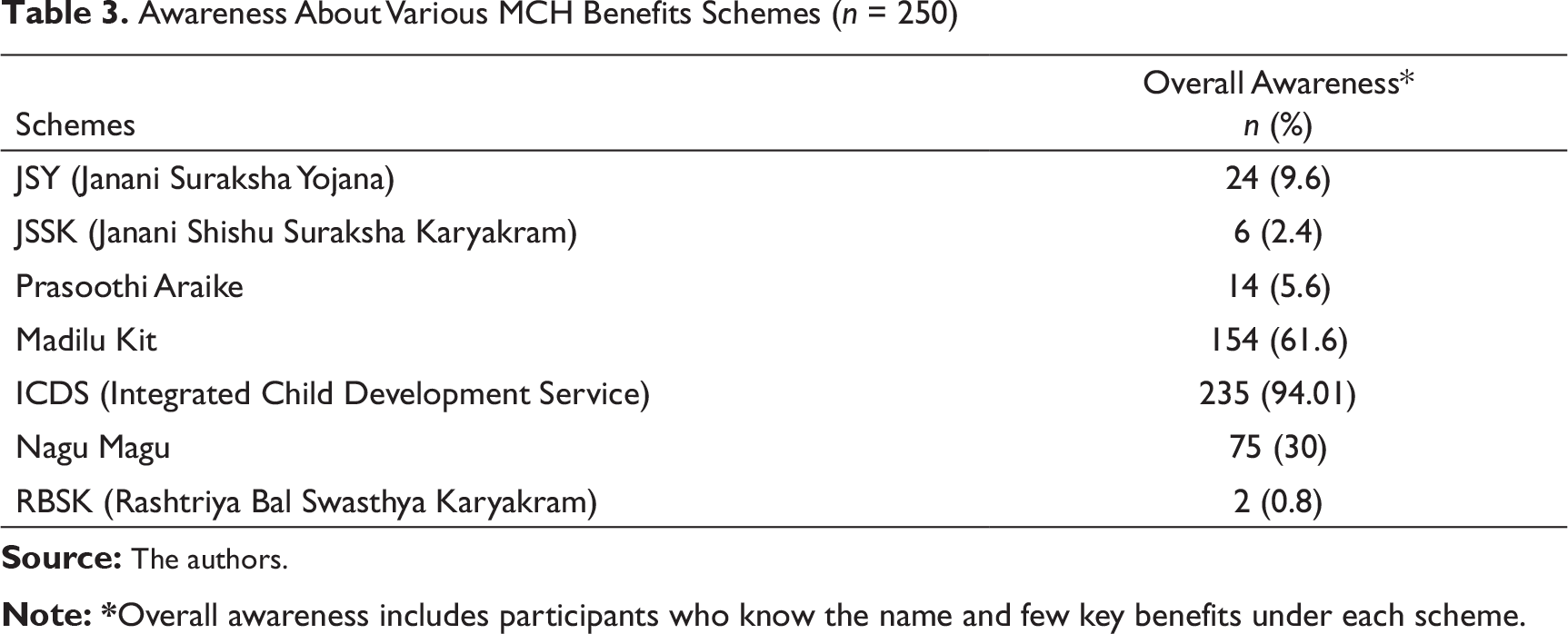
Awareness About Various MCH Benefits Schemes (n = 250)
The obstetric details of the study participants are depicted in Table 2. Out of the 250 study participants, 57.2 per cent were ANC. Most of the participants had one live birth (49.6%). Registration of pregnancy was 100 per cent and most of the participants registered in government sector (75.6%), primary health centres being the most common place of registration (65.6%). A great number of women were registered during the first trimester of pregnancy (93.2%), and majority of them had a Thayi card (90.8%). A total of 26.8 per cent of the study subjects were high-risk pregnancy, gestational diabetes mellitus being the most common risk (34.3%).
For each of the schemes, majority of the participants were aware of the name of the schemes but not the key benefits. Hence, the overall awareness for each scheme was low (Table 3).
Overall awareness of the participants ranged from 0.8 per cent for Rashtriya Bal Swasthya Karyakram (RBSK) to 94.01 per cent for Integrated Child Development Services (ICDS). A great number of the study participants were aware of the name (97.2%) as well as the benefits of ICDS accounting to an overall awareness of 94.01 per cent. One-third of the study participants were aware of the name of JSY (32.4%), but fewer knew the benefits amounting to an overall awareness of 9.6 per cent. Very small fraction of the study participants was aware of the name (7.2%) and benefits of RBSK, with an overall awareness of 0.8 per cent.
The source of information for the study participants who were aware of the names of the schemes varied as shown in Table 4. Accredited Social Health Activist (ASHA) was the major source of information for all the schemes. Even though Internet/social media is a major source to access information, none of them reported it as a source of information.
Source of Information for Various MCH Benefit Schemes #
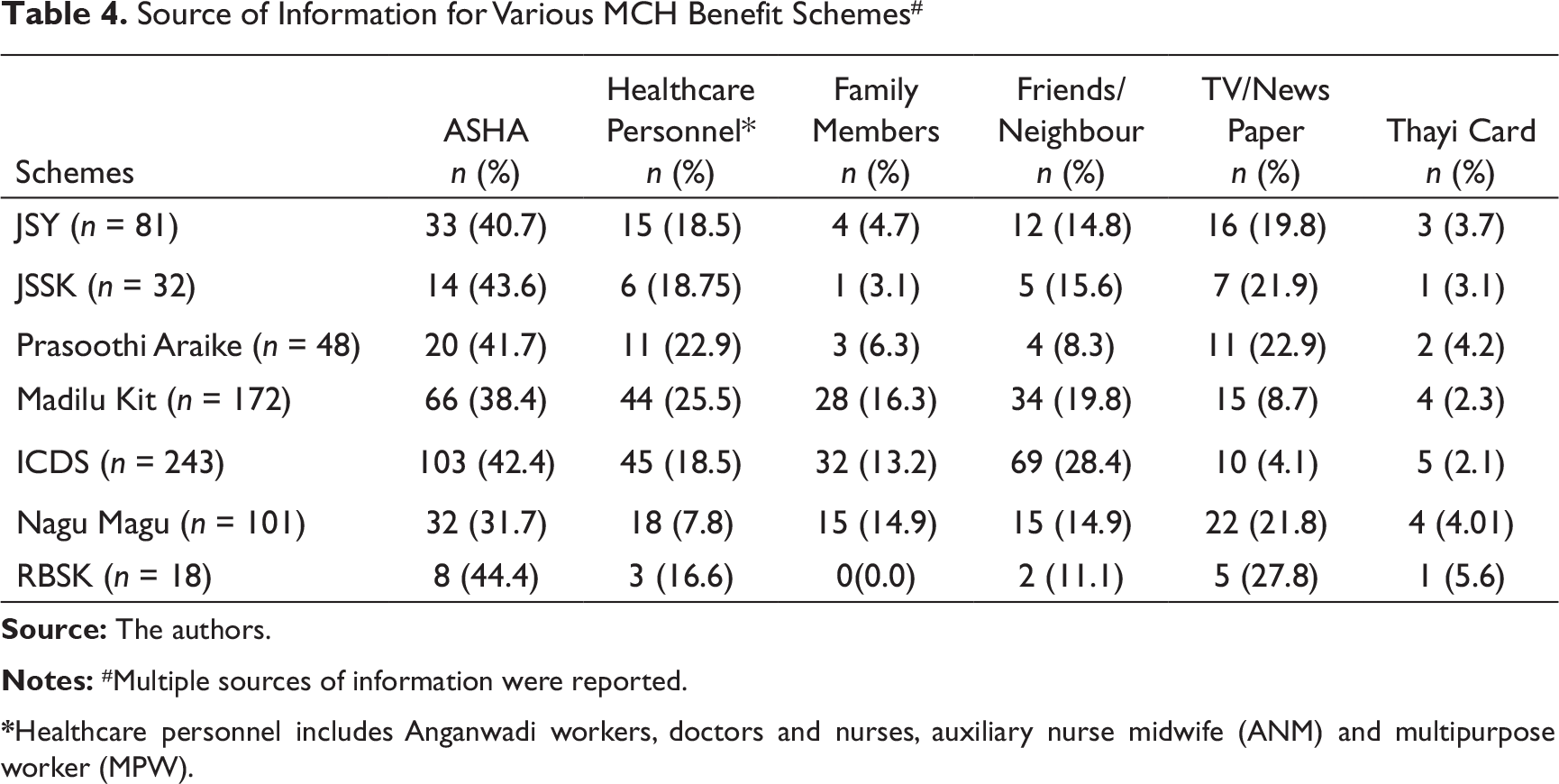
*Healthcare personnel includes Anganwadi workers, doctors and nurses, auxiliary nurse midwife (ANM) and multipurpose worker (MPW).
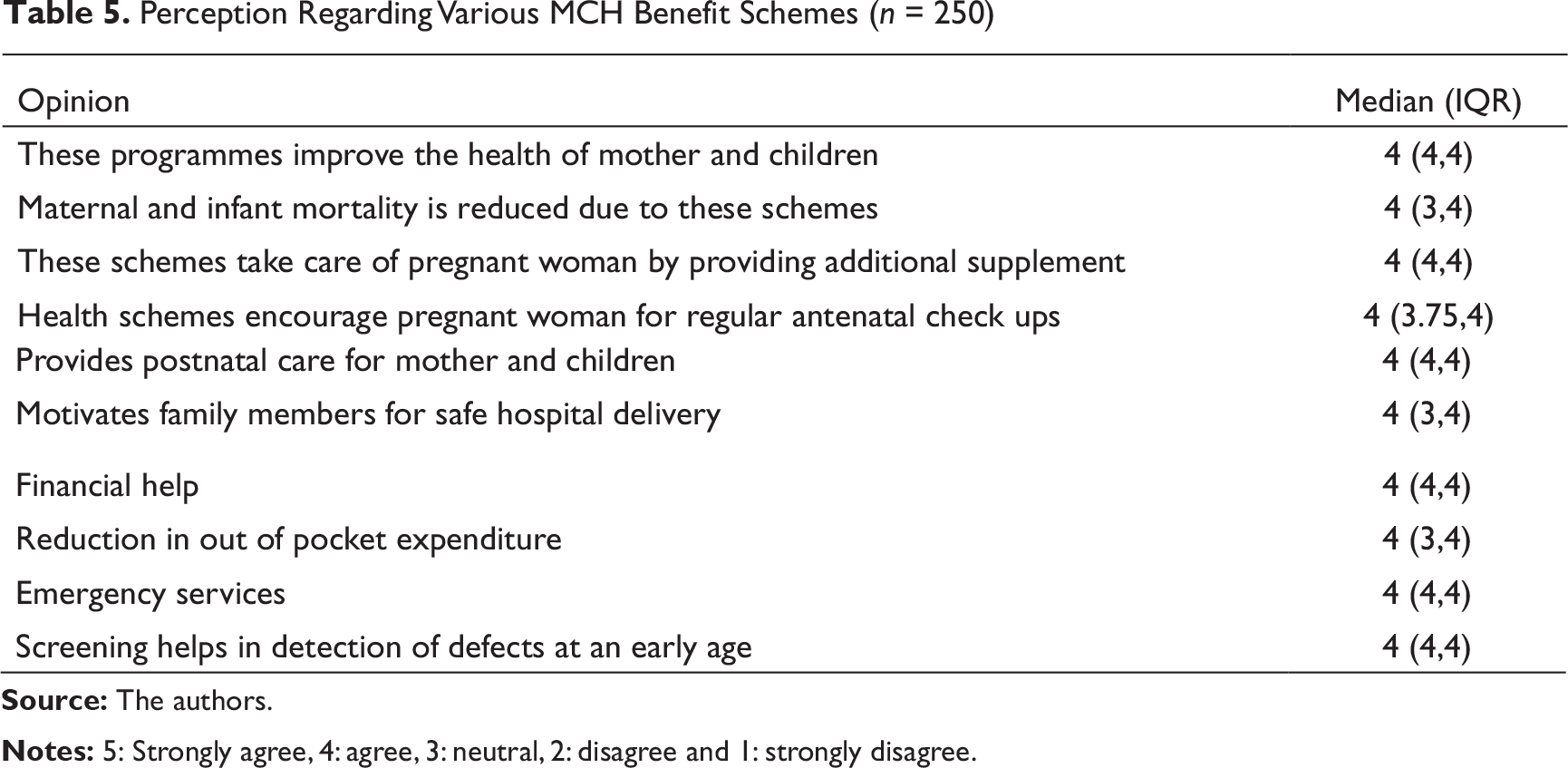
Perception Regarding Various MCH Benefit Schemes (n = 250)
Uptake of Various MCH Benefit Schemes Among the Study Participants
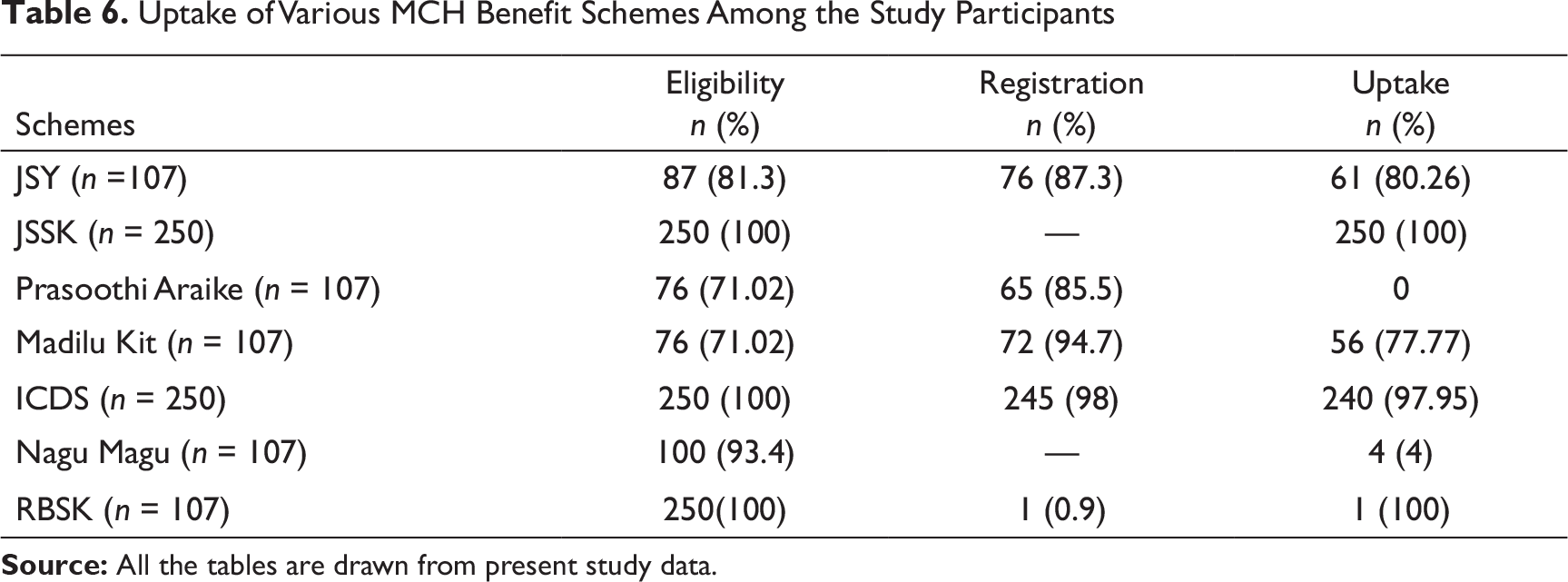
Table 6 shows the eligibility, registration and uptake of various MCH benefit schemes. All the study participants were eligible and all had taken up the benefits (100%) of JSSK. Majority of the study subjects availed the benefits of ICDS (97.95%). Out of the 107 PNC, none of them received the benefits under Prasoothi Araike, thus being the least uptake.
Discussion
Both the state and central governments have made efforts to reduce MMR and IMR by initiating various MCH schemes. Their successful implementation and utilisation is possible only when the beneficiaries are aware and have positive attitude towards the schemes.
We conducted the study to assess the awareness, perception and uptake of various available MCH schemes in one of the district hospitals in coastal Karnataka among ANC and PNC.
We found that most of the women belonged to age group of 20–30 years, permanent residents, from rural area, belonging to OBC, studied up to high school and above, homemaker and held BPL card.
Our study showed that overall awareness varied, ranging from 2.4 per cent (JSSK) to 94.01 per cent (ICDS). According to study conducted by Johnson et al. (2015), the awareness ranged from 0 per cent (JSSK) to 83.6 per cent (ICDS). A limited number of studies have been conducted to assess the awareness of all MCH benefit schemes. Majority focused on JSY and JSSK. A study conducted by Uttekar et al. (2007) showed the awareness of JSY among antenatal women of Varanasi to be 26 per cent, whereas it was 79 per cent in a study conducted by Sharma, Srivastava, Vyas, Kishore, and Semwal (2012) in Dehradun and 18.6 per cent in a study conducted in Bangalore by Johnson et al. (2012). A study conducted by Suman Chatterjee et al. (2015) on good awareness for JSSK was reported among 31.25 per cent. However, awareness of JSY in our study was 9.6 per cent and JSSK was 2.4 per cent. Significant number of participants were aware of the names of the schemes but did not know the key benefits, and few knew about the benefits but were not aware of the name of the schemes under which it was given, due to which the overall awareness was found to be low.
It is evident from above data that there is no uniformity in awareness regarding all MCH schemes anywhere in India. This could be attributed to the fact that the popularity of one scheme is more than the other in the way they are implemented. ICDS launched in the year 1975 is a community-based programme with an Anganwadi centre within the community, being a good old popular programme among the general population might have led to increased awareness for ICDS, whereas RBSK is only applicable in case of the enlisted issues; hence, its awareness was least among the general population (GOI 2015b; Park 2015).
However, there is a need to increase the awareness of all MCH-related schemes, which will empower the beneficiaries to utilise them effectively. Mangaluru is one of the cities with very high literacy rate of 91.4 per cent among females (GOI, 2011). Therefore, it will be comparatively easy to increase the awareness among them, with a little effort from the government.
Our study showed that ASHA was the main source of information (40.41%), followed by healthcare personnel (19.79%), and friends and neighbours (16.12%). TV/newspapers were also reported to be one of the sources of information. Whereas in a study conducted by Johnson et al. (2012), in Bangalore, health personnel (20.93%) followed by friends (18.47%) and family (7.3%) were the most common sources; in contrast, none of the women reported that radio/TV/newspaper had contributed as the source of information. In a study conducted by Uttekar et al. (2007), in Rajasthan, it was observed that ANMs were main source of information (71%), followed by ASHA (24.2%). Though Internet/social media is being widely used in this era, their contribution as a source of information was low.
Awareness can be improved by making use of Internet/social media, encouraging the beneficiaries to share the information with others. Also, the information regarding all the schemes with equal emphasis on each scheme can be given to the community during their Anganwadi visits, registration of pregnancy and antenatal check-up and during the home visit by peripheral health workers.
Most of the mothers in our study had a favourable opinion regarding the benefits of the MCH benefit schemes, which is consistent with the study done by Chandavari et al. (2013). Our study population agreed on the following: MCH schemes help them reduced their financial burden, provide benefits during emergency, provide additional supplements and motivate safe hospital delivery. The perception plays a major role in decision-making. This could also explain a better uptake of services in our study population in spite of low awareness.
In the study setting, the eligibility for availing certain schemes was to possess a Thayi card and the BPL card; however, ICDS and JSSK was given to all. Our study showed that uptake was maximum for JSSK (100%); since the study was conducted in a tertiary care hospital, all the women had availed the benefits. It was followed by ICDS (97.9%). Rest of the schemes were applicable to postnatal women. Out of the 107 postnatal women, uptake of JSY was 80.26 per cent, whereas it was 66.6 per cent in a study conducted by Julakatti, and Ade (2016) and only 25.5 per cent mothers received cash benefits under JSY according to a study conducted by Kumar, Bachloo, Bharadwaj, and Mukherjee (2016) in Haryana. According to a study conducted by Murthy, Siddalingappa, and Mishra (2016) in Mysore, 65.5 per cent of mothers received the benefits from JSY, 58.5 per cent from Prasoothi Araike and 61.5 per cent mothers had received Madilu kit. However in our study, uptake of Madilu kit was 77.7 per cent.
In a study to assess implementation status of JSSK for free referral transport services conducted by Goyal et al. (2014) in Maharashtra, 65.83 per cent pregnant women reported to have utilised transport services from hospital to home. Nagu Magu ambulance was introduced in Karnataka to provide drop-back facility for postnatal mothers and newborn from government health facilities to home. Though considerable number of participants were aware of Nagu Magu scheme (30%), the uptake was low (4%). Majority of participants were not willing to take their newborn babies back home in an ambulance due to social stigma. Few participants who were willing could not utilise it since the service was available only in certain days in a week. However, none of them availed Prasoothi Araike as the scheme is currently not implemented due to insufficient funds, thus being the least uptake.
Conclusion
Our study showed that the awareness and uptake for different MCH-related schemes varied. Most common scheme, which the participants were both aware and had availed the service, was ICDS, and least common was Prasoothi Araike. Most common source of information was ASHA worker, followed by friends and neighbours. Most of the study participants had a favourable opinion about the benefits of MCH schemes. There should be display of Information Education and Communication (IEC) materials in MCH hospital to increase the awareness regarding various available MCH schemes and self-help groups, and mass media and SMS may be utilised.
Compliance with Ethical Requirement
Informed Consent: Taken
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.