
Abstract
Majority of people in low- and middle-income countries with mental illness do not receive healthcare, leading to chronicity, suffering and increased costs of care. This study estimated the out-of-pocket expenditure (OOPE), catastrophic health expenditure (CHE), and poverty impact due to mental illness in India. Data was acquired from the 76th round data of the National Sample Survey (NSS) on the theme ‘Persons with Disabilities in India Survey’, July–December 2018. Data of 6,679 persons who reported mental illness during the survey was included for analysis. OOPE, CHE, poverty impact and state differentials of healthcare expenditure on mental illness were analysed using standard methods. In total, 18.1% of the household’s monthly consumption expenditure was spent on healthcare on mental illness. About 59.5% and 32.5% of the households were exposed to CHE based on 10% and 20% thresholds, respectively. About 20.7% of the households were forced to become poor from non-poor due to treatment care expenditure on mental illness. Our study suggests the critical need to accelerate on various measures for early diagnosis and management of mental health issues along with financial risk protection for reducing financial impact of healthcare expenditure on mental illness among households in India.
Key Messages
In total, 18.1% of household’s monthly consumption expenditure among 5,935 persons surveyed as part of National Sample Survey 76th Round on ‘Persons with Disabilities in India Survey’, 2018 was spent on healthcare on mental illness in India.
At 10% and 20% thresholds, 59.5% and 32.5% of the households were exposed to catastrophic health expenditure for treatment related to mental illness.
About 20% of the households became poor from being non-poor initially due to treatment expenditure on mental illness.
There is a critical need to provide financial risk protection to reduce financial impact of healthcare expenditure on mental illness among households in India.
Introduction
Mental illness has been overlooked, undermined and tabooed for a long in both developed and developing countries. Mental illness encompasses a spectrum of disorders that are typically characterised by some combination of abnormal thoughts, emotions, behaviour and relationships with others, and includes schizophrenia and other psychotic disorders, mood disorders including depressive disorders and bipolar mood disorders, substance use disorders, people with intellectual impairments with behavioural problems, neuropsychiatric conditions like seizure disorders, dementia, other organic mental disorders and developmental disorders (World Health Organization [WHO], 2015). Although mental illness is more commonly recognised in adults, studies indicate that the onset of the initial signs may occur in childhood or during adolescence (Jones et al., 1994; Kessler et al., 2007). Fortunately, most of the mental illnesses can be treated and managed to help the affected person lead a fruitful and productive life. Despite the availability of treatment, stigma and superstitions around mental illnesses prevent the sufferers from seeking timely care (Sangeeta & Mathew, 2017). In developing countries like India, the situation is even more worrying as people with mental illnesses also have problems in everyday life, especially with jobs and marriages where prejudice and contempt are very high (Baldwin & Marcus, 2011; Corrigan & Watson, 2002; Sharma et al., 2015; Trani et al., 2015). Studies have revealed that people with mental illness face a lack of acceptance and inclusiveness even among the educated strata of society (Bingham & O’Brien, 2018; Wang & Lai, 2008).
Globally, as per 2016 estimates, the disease burden for mental illness (or mental disorders) accounts for 32.4% of years lived with disability (YLD), and 13% of disability-adjusted life-years (DALYs) (Vigo et al., 2016). In low-and middle-income countries (LMICs), more than 11.1% of the total disease burden is due to mental health disorders, yet they receive less than 1% of many of these countries’ health budgets (Patel, 2007). In India, depressive disorders contribute to 7.1% of total YLDs, and 2.5% of total YLDs due to anxiety disorders (WHO, 2017).
The majority of people in LMICs with mental illness do not receive healthcare, leading to chronicity, suffering and increased costs of care (Patel, 2007). The stigma is so deep-rooted that despite treatment, many people with mental illnesses are not considered ‘suitable’ or responsible enough for a task, job or relationship. People with mental illness often suffer financial setbacks pushing them further away from seeking treatment for their problems. People with severe mental illness are found to be more likely to several physical disorders such as/or risk of comorbid conditions such as hypertension, heart diseases, diabetes, respiratory diseases and nutritional disorders (Coxon et al., 2020; De Hert et al., 2011). Additionally, mental illness is also a risk factor for other health problems, such as contribution of alcohol use or any other substance to road traffic accidents or liver disease (Patel, 2007). This poses additional financial burden on households with persons suffering from mental illness.
This study aimed to estimate the impact of out-of-pocket expenditure (OOPE) on catastrophic health expenditure (CHE), and poverty impact due to mental illness in India. To the best of our knowledge, there has been no study conducted towards analysing the financial burden of mental illnesses on Indian households. The present study, aims to highlight the burden of mental illness and the gaps in seeking care for mental health issues in India, thus highlighting the need in formulating and strengthening financial risk protection policies affected by mental illness in India.
Data and Methodology
Data Sources and Sample Size
The current study uses the 76th round data of the National Sample Survey (NSS) on the theme ‘Persons with Disabilities in India Survey’ which was conducted during July–December 2018 (National Statistical Office [NSO], 2018). The NSS is a nationally representative population-based survey organisation that collects data on several domains, like employment status, morbidity, healthcare utilisation, household consumer expenditure, housing conditions, disabilities, etc. The NSS is a national representative population-based survey organisation and findings of NSS surveys are generally used by policymakers and researchers. The NSS 76th round covered 1,18,152 households and 576,569 individuals. The present study covers a total of 6,679 individuals who reported mental illness during the survey.
Research Design and Geographical Coverage
NSS 76th round survey used Census 2011 population with suitable growth rates for a sampling frame. At the national level, rural villages were divided into a number of sub-units (SU) of more or less equal population and the number of SUs formed in a village was determined a priori. SUs were formed in urban sector also, similar to that adopted in rural areas except that SUs were formed on the basis of households in the Urban Frame Survey (UFS) instead of population. Each UFS block with a number of households more than or equal to 200 was divided further into a number of SUs, and those with households less than 200, the entire UFS block was considered as one First Stage Unit (FSU). In the remaining UFS blocks, the SUs was considered as FSUs. A stratified two stage sampling design has been adopted for the NSS 76th round survey. In the first stage villages/urban blocks (FSU) were chosen by Probability Proportional to Size with Replacement (PPSWR). The ultimate stage units (USUs) were both households in both rural and urban areas. In the second stage of sampling, a total 20 households from each of the selected village/urban wards were selected by Simple Random Sampling Without Replacement scheme in both rural and urban areas. The survey covered all states and union territories of India (NSO, 2018).
Definition of Mental Illness
The NSS 76th round defined mental illness as
a substantial disorder of thinking, mood, perception, orientation or memory that grossly impairs judgment, behaviour, capacity to recognise reality or ability to meet the ordinary demands of life, but does not include retardation which is a condition of arrested or incomplete development of mind of a person, especially characterised by sub normality of intelligence. (NSO, 2018)
The NSS 76th round survey asked the following three questions to access the mental illness among individuals during the survey period:
Whether having unnecessary and excessive worry and anxiety, repetitive behaviour/thoughts, changes of mood or mood swings, talking/laughing to self, staring in space? Whether having unusual experiences of hearing voices, seeing visions, strange smell or sensation or strange taste? Whether having unusual behaviour or difficulty in social interactions and adaptability?
Measuring Out-of-Pocket Expenditure (OOPE) for Healthcare
The NSS 76th Round survey captured medical expenditure (surgery, equipment, hospitalisation, etc.) and non-medical expenditure (transport, lodging, food, etc.) for infrequent expenditure during the last 365 days from date of survey, and usual monthly expenditure (excluding those covered infrequent expenditure during the last 365 days) (NSO, 2018). We calculated yearly OOPE, monthly OOPE and average monthly total OOPE in monthly using the following formulas

where YME = yearly medical expenditure, YNME = yearly non-medical expenditure

where MME = monthly medical expenditure, MNME = monthly non-medical expenditure
Where YME = yearly medical expenditure, YNME = yearly non-medical expenditure, MME = monthly medical expenditure, MNME = monthly non-medical expenditure
Burden of Income Loss Due to Mental Illness
We have examined the OOPE burden as a percentage of OOPE on the total household consumption expenditure as used in several previous studies (Mitra et al., 2009; Sahoo & Madheswaran, 2014).

Households Monthly Consumption Expenditure (HMCE)
This study used monthly household consumption expenditure as a proxy variable for household income which has been used in numerous earlier studies (Joe & Rajpal, 2018; Kastor & Mohanty, 2018; Sangar et al., 2019). This is a preferred measure since it is less prone to disparity and bears fewer chances of being under reported or over reported when related to income (Kastor & Mohanty, 2018). Based on the information in the NSSO 76th round survey, this study considered the monthly consumer expenditure by households as below (Government of India, 2018):
where A = usual consumer expenditure in a month for household purposes out of purchase, B = imputed value of usual consumption in a month from homegrown stock, C = imputed value of usual consumption in a month from wages in kind, free collection, gifts, etc., and D = expenditure on purchase of household durables during the last 365 days.
Measuring Catastrophic Health Expenditure (CHE)
This study defines CHE as a situation where health expenditure exceeds α% threshold of households’ income (Kwesiga et al., 2015). In the published literature, there is no consensus on the threshold of CHE (Aregbeshola & Khan, 2018; O’Donnell et al., 2008). Furthermore, studies have used CHE if health expenditure is exceeding the 40% threshold of household’s on total non-food consumption expenditure or health expenditure exceeds 10% threshold of household’s on total consumption expenditure (Berki, 1986; Kumar et al., 2015; Russell, 2004; Somkotra & Lagrada, 2009; Van Doorslaer et al., 2007; Wagstaff & van Doorslaer, 2003; Xu et al., 2007). The present study measured CHE by two approaches as described below (Kumar et al., 2015; Wagstaff & van Doorslaer, 2003).
First approach


If OOPE exceeds 10% and 20% threshold of a household’s total consumption expenditure (HCE).
Second approach

where α is the average household consumption expenditure per person and β is the average household consumption expenditure for two members of the household (Joe & Rajpal, 2018).
Measuring Poverty Impact Due to Healthcare OOPE on Mental Illness
For measuring the poverty impact of OOPE on households, this study used the poverty head count ratio (PHCR) and poverty gap indices. For measuring the poverty line, this study used per capita household monthly expenditure at INR 972 in rural areas and INR 1,407 in urban areas as per recommendation by the Rangarajan committee based on 2012 data (Raveendran, 2016) which described below

The PHCR is a percentage of households who falls below the poverty line due to OOPE (Kumar et al., 2015; Somkotra & Lagrada, 2009; Van Doorslaer et al., 2007).

The percentage shortfall from the poverty line of those households that have become poor due to OOPE is counted using poverty gap, and the poverty gap ratio defines the percentage shortfall from the poverty line of households that have become poor due to OOPE as a proportion of all the households in the population (Kumar et al., 2015; Van Doorslaer et al., 2007; Wagstaff & van Doorslaer, 2003).

Data Analysis
Descriptive statistics, bivariate analyses and multivariate models were used in the analyses. In the first part of the analysis, descriptive analysis was carried out to describe the background characteristics of persons who were reported mental illness. In the second step, bivariate analyses were carried out to access the burden of income loss due to healthcare expenditure on mental illness, CHE and poverty impact on households by selected socioeconomics characteristics using predictor variables such as age, sex, education, economic status, relation to the head of the household, place of residence and type of mental illness. These variables were chosen based on previous studies and data availability in the dataset (Government of India, 2018; Ringel & Sturm, 2001). In the third step of the analysis, binary logistic regression analysis was carried out to observed the effect of selected socioeconomics characteristics on CHE and poverty impact. In order to take into account, the survey design (i.e., sampling weights with clustering and strata), while estimating bivariate and multivariable statistics, the Survey Data Reference (SVY) command was used in STATA 13.1 (StataCorp. 2013). All expenditures are reported in Indian Rupees (₹).
Results
Socioeconomic and Demographic Characteristics of Respondents
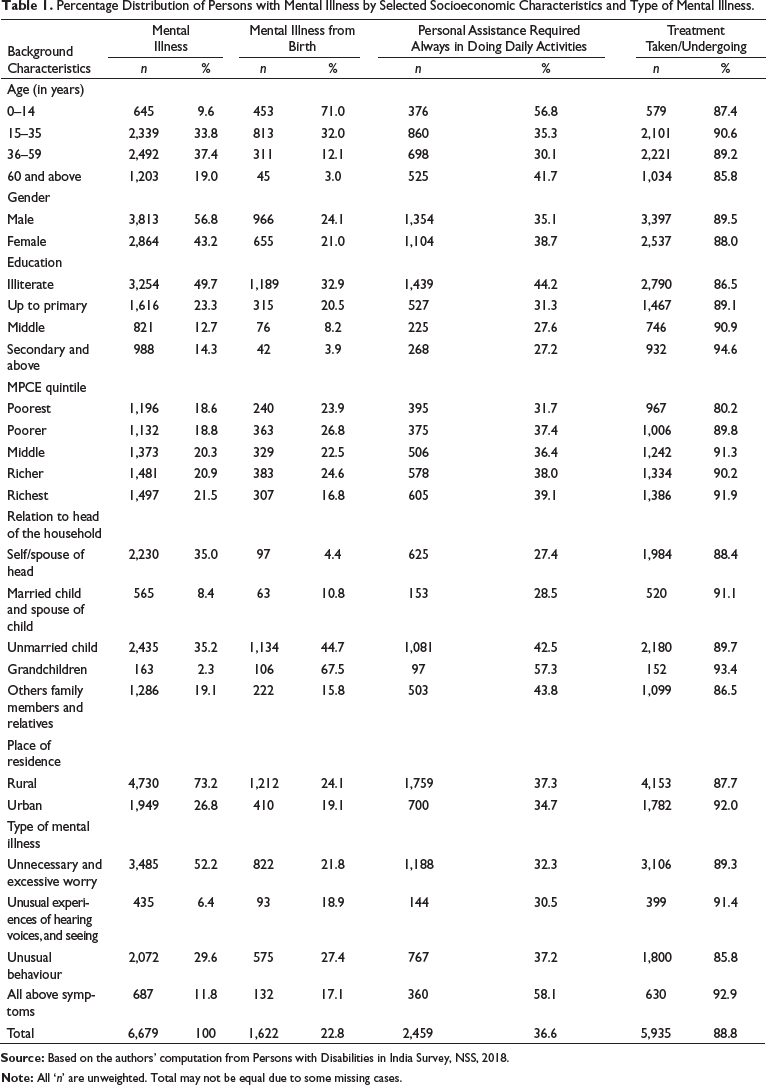
Table 1 shows the selected socioeconomic and demographic characteristics of those persons who reported any types of mental illness during the survey period. Higher percentage (71.2%) of persons identified in the survey belonged to working age group 19–59 years, among them 56.8% were male and almost half 49.7% were illiterate. More than half, 52.2%, persons reported that they felt unnecessary and excessive worry, while 29.6% reported unusual behaviour. About 36.6% required personal assistance for all their daily activities (Table 1).
Percentage Distribution of Persons with Mental Illness by Selected Socioeconomic Characteristics and Type of Mental Illness.
Burden of Income Loss Due to Mental Illness
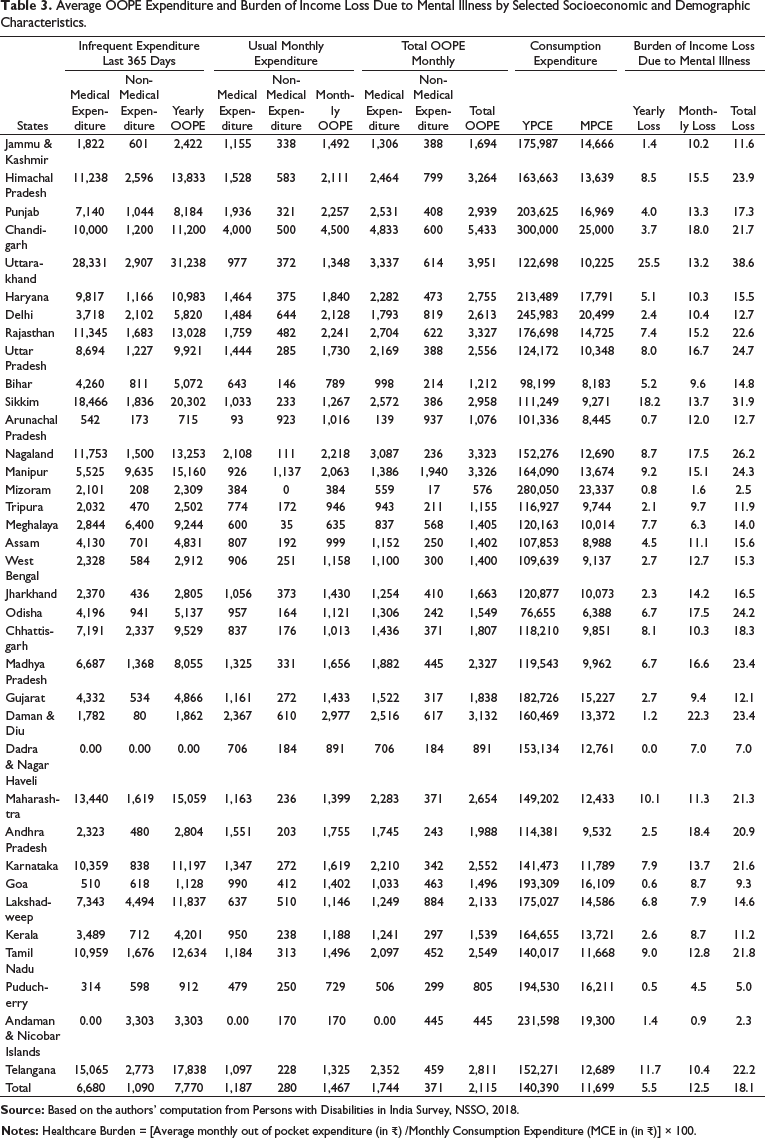
The average yearly and monthly OOPE and proportion of OOPE on healthcare due to mental illness on the total consumption expenditure of households is reported in Table 2. Age group 60 years and above age group reported the highest OOPE on mental illness in the last 365 days across all age groups. The richest households reported around nine times the OOPE expenditure compared to the poorest household. However, the burden of income loss due to mental illness remained almost consistent across all income quintiles. Overall, 18.1% of the household’s monthly consumption expenditure was spent on healthcare due to mental illness of member in the household. Finding showed that states like Daman and Diu (19.4%), Himachal Pradesh (18.0%), Sikkim (17.4%), Lakshadweep (14.6%), Maharashtra (13.7%), Telangana (13.3%), Punjab (12.7%), Uttarakhand (12.5%) reported higher healthcare burden than the national average for India (10.4%). On the other hand, Mizoram (0.5%), Andaman and Nicobar Islands (1.2%), Puducherry (1.7%), Dadra and Nagar Haveli (2.0%), Arunachal Pradesh (3.0%) and Nagaland (3.5%) reported lower healthcare burden (Table 3).
Average OOPE Expenditure (in ₹) and Burden of Income Loss Due to Mental Illness by Selected Socioeconomic and Demographic Characteristics.

Average OOPE Expenditure and Burden of Income Loss Due to Mental Illness by Selected Socioeconomic and Demographic Characteristics.
Exposure to Catastrophic Health Expenditure
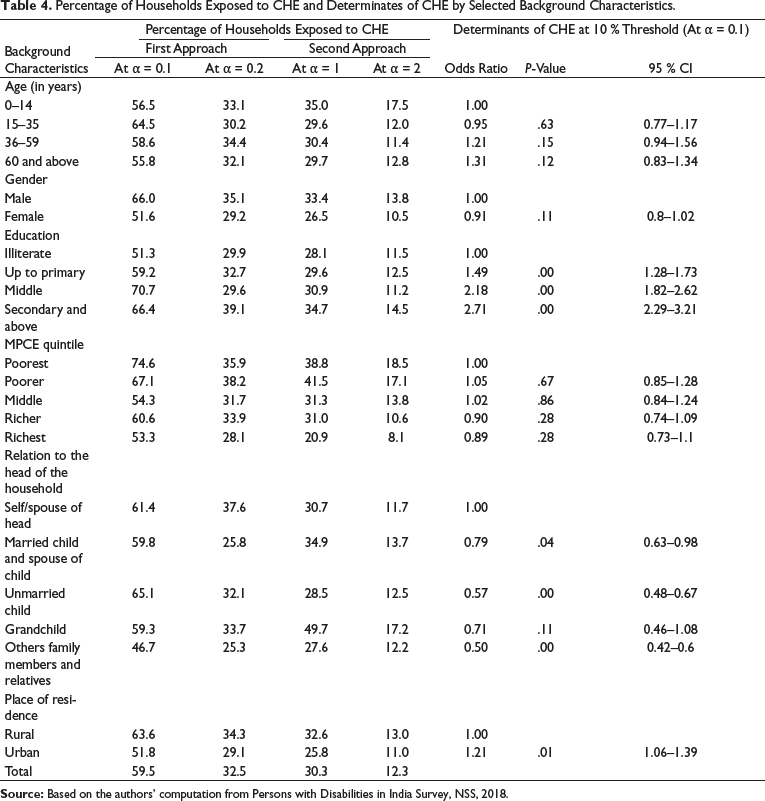
Table 4 provides the analysis of households who faced the CHE due to healthcare expenditure on mental illness using two approaches, first if OOPE exceeded 10% and 20% of the total household’s consumption expenditure and second when the average OOPE on healthcare exceeded per capita household consumption expenditure (PHCE) of one and two household members (Table 4). About 59.5%, and 32.4% of the households forced to CHE due to treatment care of mental illness based on 10% and 20% thresholds respectively while 30.3% of the household’s healthcare expenditure exceeded PHCE of one household member, and in 12.3% households of two household members due to treatment care expenditure on mental illness. Odds of pushed households to CHE were significantly associated with the education of persons and being located in an urban area for households with person(s) with mental illness (Table 4).
Percentage of Households Exposed to CHE and Determinates of CHE by Selected Background Characteristics.
Poverty Impact Due to Healthcare Expenditure on Mental Illness
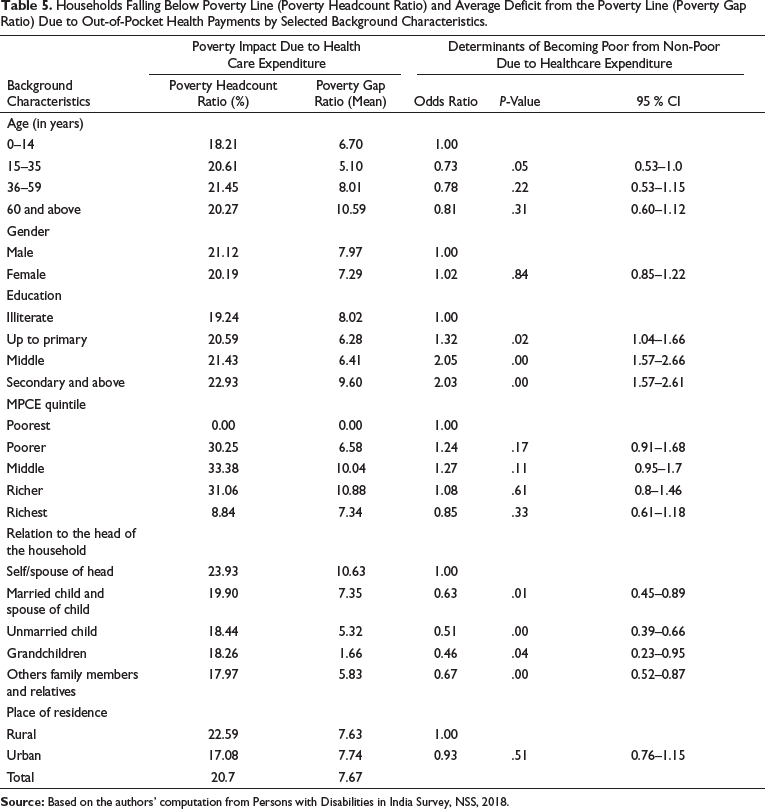
Table 5 describes the households falling below the poverty line (PHCR) and average deficit from the poverty line (poverty gap ratio) due to OOPE health payments for the treatment of mental illness. About 20.7% of the households fall below the poverty line due to treatment care expenditure for mental illness. The percentage of households falling below the poverty line was higher among rural residents than urban residents. About 22.5% of rural households, were pushed from being non-poor initially to below poor, due to treatment cost of mental illness compared to 17% in patients belonging to urban households. Average percentage shortfall in income from the poverty line due to mental illness treatment care expenditure was 7.6%. Results indicate that age, education and relation to the head of the household were found to be statistically significant predictors of household falling below poverty line due to healthcare expenditure towards mental illness.
Households Falling Below Poverty Line (Poverty Headcount Ratio) and Average Deficit from the Poverty Line (Poverty Gap Ratio) Due to Out-of-Pocket Health Payments by Selected Background Characteristics.
State-Wise Variations in Prevalence, OOPE, CHE and Poverty Impact Due to Mental Illness
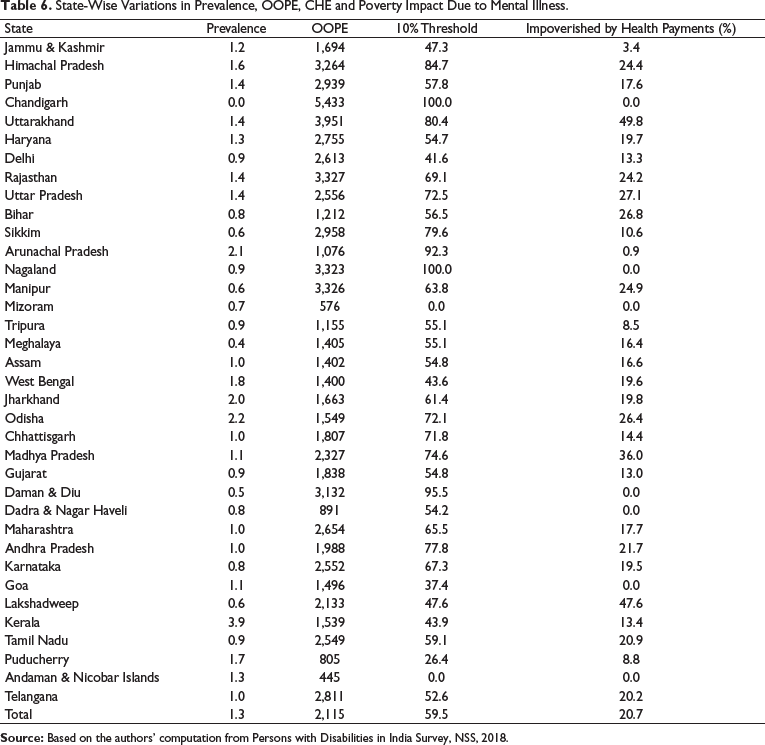
This study also compares the prevalence of mental illness, OOPE, CHE and PHCR by the states of India (Table 6). The prevalence of mental illness per 1,000 was higher in Tripura, Manipur, followed by Manipur, Haryana, Maharashtra and Madhya Pradesh while the OOPE was higher in Chhattisgarh, followed by Himachal Pradesh, Daman and Diu, Lakshadweep and Punjab. The percentage of households pushed to CHE due to high healthcare expenditure was much higher in Daman and Diu, Himachal Pradesh, Chandigarh, Lakshadweep, Sikkim, Punjab and Andhra Pradesh while the percentage of households who become the poor from non-poor was higher in Lakshadweep, Himachal Pradesh, Manipur, Uttarakhand and Haryana.
State-Wise Variations in Prevalence, OOPE, CHE and Poverty Impact Due to Mental Illness.
Discussion
In the present article, we examined the OOPE, CHE and OOPE, and poverty impact due to healthcare expenditure on mental illness in India. Based on the authors’ knowledge, this is the first study that discusses about the household’s economic burden due to healthcare OOPE on mental illness in India using a national representative survey. In this article, we have defined monthly OOPE as a total of medical expenditure and non-medical expenditure and healthcare burden is defined as a share of OOPE on the total households consumption expenditure which has been used in many previous studies study (Mitra et al., 2009; Ringel & Sturm, 2001; Sahoo & Madheswaran, 2014). The following are the salient findings of our study.
Our study reveals that a higher proportion of the people with mental illness is seen in the economically productive age group (19–55 years). Reports from India have suggested that the mental illness rate is high among productive age groups and is the largest contributor to economic loss in India (Isalkar, 2015). Among non-communicable diseases, mental health is expected to account for 20% of economic loss (estimated at $6.2 trillion) from 2012–2030. In LMICs 40%–50% of mental healthcare costs are borne out of pocket, and the higher prevalence among the productive age group (19–55 years) in our study imply the disability effects of mental illness limiting the ability of persons to search for and sustain productive employment (Patel, 2007).
Overall, 18.1% of the household’s monthly consumption expenditure was spent on treatment care on mental illness and varies across socioeconomic groups. Burden of OOPE was higher in urban and more literate patients compared to rural and illiterate patients, respectively. The results reveal that 59.5%, and 32.4% of the households experienced CHE due OOPE for mental illness based on 10% and 20% thresholds respectively while 30.3% and 12.3% of the households had catastrophic impact based on the modified approach of average per capita and average two capita monthly consumption expenditure respectively. This approach is new and has been highlighted in a previous study (Joe & Rajpal, 2018). Our findings are consistent with the incidence of CHE among households in other developing countries (Hailemichael et al., 2019).
Our results revealed that mental illnesses push around 20% of the households below the poverty line and the extent of financial trauma may vary with different socio-economic parameters. Previous studies have also shown a vicious cycle in which mental health pushes towards poverty while poverty itself may increase the vulnerability towards mental illnesses (Lund et al., 2010; Sriram, 2018). Although people who had the education of or above secondary level were more likely to get poorer due to mental health issues than less educated people, mental illnesses may also affect a person from seeking education as supported by previous studies (Sriram, 2018; Trani et al., 2015).
Strengths and Limitations of the Study
The strength of the present study is that results of this study can be generalised subsequently as they were derived from the current countrywide representative cross-sectional NSS data which was well designed, covering all the states of India and more particularly the survey was based on the theme of persons living with disability in India. Second, this study used standard methods from previous studies to capture the households’ financial burden due to healthcare expenditure on mental illness and strictly followed all the standardised steps calculating the dependent and independent variables for analysis. While this study has several strengths, there are some limitations as well. First, recall bias is a major limitation of expenditure data reported by households on healthcare. Second, we cannot make any causal inferences as our study is based on the cross-sectional survey study design. Third, due to the study design limitations, we could not calculate indirect costs due to unemployment, reduced educational attainment, expenses for social support, costs associated with chronic disability, homelessness, crime, suicide, homicide, caregiver burden, family caregiver’s time, other medical complications of mental illness, early mortality, substance use and other unquantifiable costs such as emotional burden on family (Isalkar, 2015). Future research on mental illness in India should aim to focus on estimation on mental illness’s indirect costs, as these are higher than direct costs (Isalkar, 2015).
Conclusion
India is currently facing a serious mental health crisis, with mental illness constituting one-sixth of all health-related disorders (WHO, 2017). There have been rising cases of mental issues in India, particularly depression, anxiety, bipolar disorders and schizophrenia, and suicide being a leading cause of deaths among young people—reference. The National Mental Health Policy 2014 and the Mental Healthcare Act, 2017 has proposed several steps to combat mental illnesses through promoting awareness, ending the stigma associated and provision of good quality and affordable care for mental illnesses in the country (Government of India, 2017; Gururaj et al., 2016; MOHFW, 2014). Our article suggests that there is a critical need to accelerate on ground various measures for the early diagnosis and management of mental health issues in order to reduce OOPE, CHE and poverty impact due to healthcare expenditure on mental illness among households in India.
Footnotes
Acknowledgement
An earlier version of this article was presented at 41st annual conference of the Indian Association for the Study of Population from 28 to 30 November 2020, and this article got the best poster award. The authors are grateful to session chairpersons and participants for comments and constructive suggestions facilitating improvement in the article.
Author contribution
JY and DJ conceived the idea for the study and developed the analysis plan. JY led the analysis and organised the first draft of the manuscript. JY and DJ conducted data interpretation and manuscript writing. JY, GRM, DJ, CV and RS read and approved the preliminary manuscript. All authors approved the final version of the manuscript.
Data Availability Statement
The present article is based on NSS 76th round survey data, which is freely available to individuals at
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
The present study used the data from the recent NSS 76th round survey. First, the NSS obtained the ethical consent from the review committee of the NSS before the survey. Second, during the survey, a usual written consent had been taken by the respondent once they are agreed to take part in the study. Therefore, no ethical approval is required separately for the present study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.