
Abstract
The changing nature of technology has influenced the physical activity behaviour of working adults in tropical-built environments. Existing physical activity interventions show a lack of diversity in delivery strategies and limited local context community assimilation measures. This study aims to provide a perspective on the interventions implemented to promote physical activity in urban and rural neighbourhoods in tropical regions. Three analytical themes were synthesised from 29 screened qualitative and quantitative literature: the social context, the environmental factors and the mechanisms to promote physical activity in the built environment. The findings recognise the importance of spatial heterogeneity in physical activity promotion at midstream and downstream intervention levels in a tropical built environment. A multifaceted intervention model for positive physical activity behaviour change (MIPA) consisting of built environment variables, micro-climate conscious design, health awareness and self-efficacy factors according to the tropical built environments context is proposed.
Keywords
Introduction
In this study, physical activity refers to walking or cycling as a mode of transportation to and from an individual’s place of work. Earlier reviews of physical activity suggest that it is the key to combating metabolic syndrome and can be based on complex interactions between individual, environmental and socio-cultural factors (Dinu et al., 2019; Nunan et al., 2013; Rawlings et al., 2019; Saunders et al., 2013). Reports have shown that sedentary office workers comprise the majority of obese individuals worldwide due to the lack of physical activity during work and non-working hours (Addo et al., 2015; Cheng, 2016; Heinen & Darling, 2009; MalayMail, 2016; Mohamad Nor, 2018). In an alarming report, 73% of all recorded deaths were caused by non-communicable diseases (NCDs) that are evidenced to be preventable by changing one’s physical activity behaviour (Institute for Public Health (IPH), 2015; The Economist, 2017). The understanding of obesogenic features of the tropical built environment by identifying distinct types of neighbourhoods may offer solutions to the growing trend of physical inactivity in this region. That is why built environment design decision-makers need to be aware of the direct and indirect impacts that their decisions have on longstanding health and societal welfare, given that they are primarily determined by environmental factors (Fitzpatrick et al., 2018; Lee et al., 2019).
This article aims to discuss through thematic synthesis (a) constraints and facilitators for physical activity implemented in tropical built environments, and (b) the available interventions designed to reduce the effects of obesogenic environments through physical activity. The discussion focuses on the impact of the changing nature of technology that has influenced the physical activity behaviours of working-age adults in monsoon-affected built environments. In contrast to Europe, North America and other mid-latitude climates, tropical temperatures do not change much throughout the year. The seasonal cycle in tropical continents is marked by an oscillation between dry (December until February in South Asia and sub-Saharan Africa) and wet (June–September in South Asia and December–February in Southeast Asia) periods. The region affected by the monsoon stretches from the South China Sea to the Indian Ocean and includes the northern end of Australia. In recognising the role of the built environment as a health determinant, this study also discusses intervention strategies designed to reduce the effects of NCDs through the facilitation of physical activity behaviour adopted from public health policies.
Methodology
Search Strategy
Our search includes four databases (Science Direct, PubMed, ProQuest and Google Scholar) and is made in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. Literature available beyond 31 July 2020 is not considered in this review. Keywords used are physical activity, tropical environment, NCD prevention, thermal transient condition perceptions, obesogenic environment and walkability. We include sources with samples consisting of working-age adults (18–60 years old) with minimal physical activity in their daily routine from both quantitative and qualitative studies. In terms of methodology, sources that focus only on data modelling and climate chamber experiments were not included. Studies that focused only on sedentary time, the nutrition perspective of physical activity and the obesogenic effects were excluded. All included sources are published in peer-reviewed English journals.
Data Synthesis
Search activities were managed using Endnote X9 software. The thematic synthesis aims to determine to what extent interventions in the current tropical built environment address the factors that predominantly influence sedentary workers’ participation in physical activity. By using NVivo 11, the data was organised into three stages, such as line-by-line coding, descriptive themes coding and analytical theme coding.
Results and Discussion
Figure 1 shows the literature screening flow adopted from PRISMA. A total of 1,374 titles and abstracts were identified following duplication removal. Subsequently, 1,126 records were screened and deemed to be irrelevant to this search based on their article type, title and abstract. A total of 248 full texts were screened implying 219 excluded records; reasons for exclusion are stated in Figure 1. Records were sorted according to quantitative and qualitative studies. The outcome of the previous screening was discussed to clarify the interpretation of inclusion criteria. The 29 studies included studies were further divided into 23 quantitative and 6 qualitative or mixed-method studies.
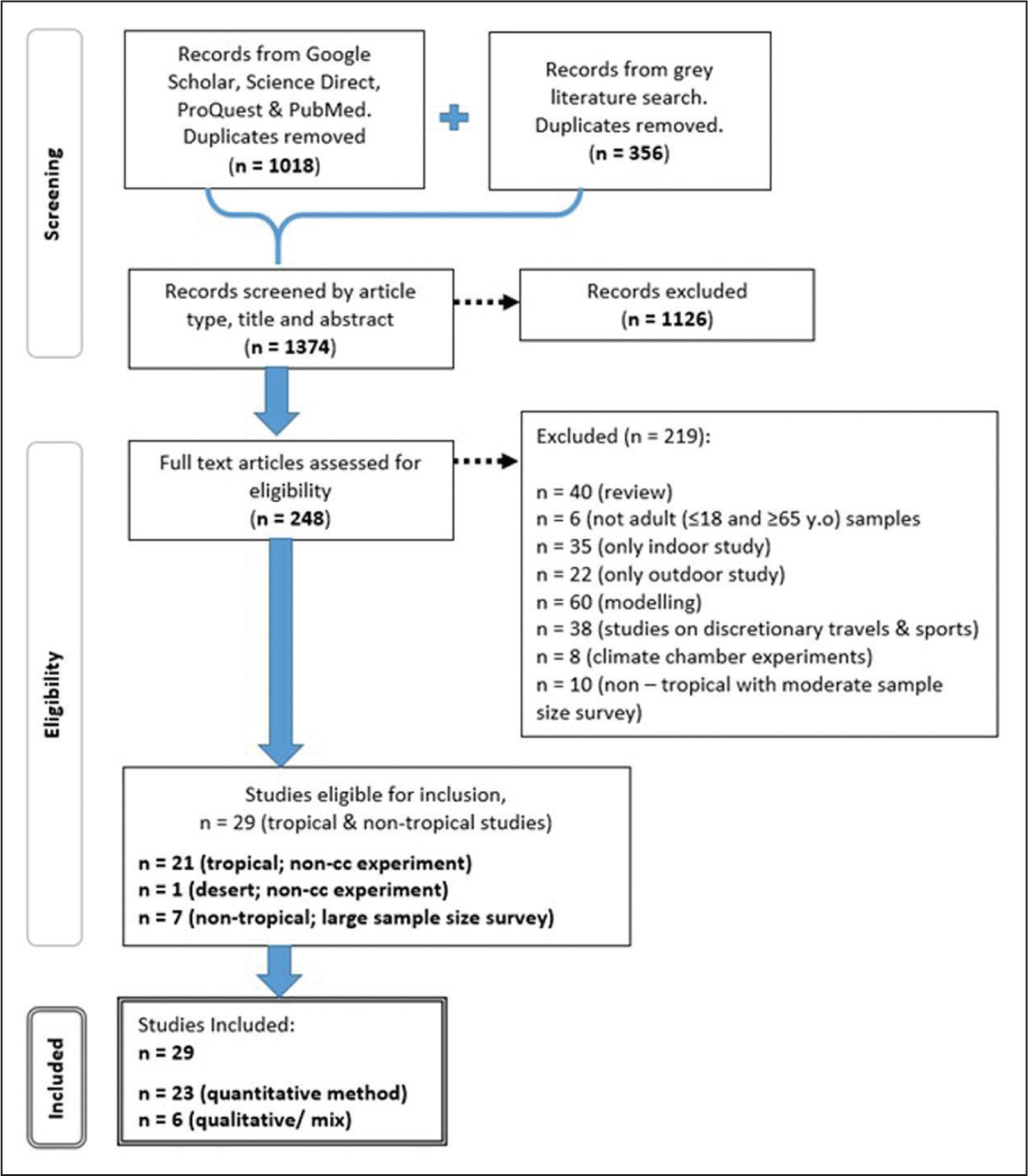
These studies were published between 2003 and 2020; 24 were published between 2013 and 2019 (Table 1). Twenty-three studies examine perceptions and behaviours of adults in tropical climate countries while the remaining six studies were performed in non-tropical built environments. These six studies were considered exceptional due to their contribution to reporting physical activity participation and NCD prevention strategies in various environments with very large sample sizes of 4,000 or more. Fifteen of the sources have predominantly female samples, four sources have predominantly male samples, and 10 do not disclose their sample gender.
Data Extraction (n = 29).

* See Table 2 in the description for the intervention group ID.
** Intervention levels: downstream intervention (DI); midstream intervention (MI); and upstream intervention (UI).
The interventions from the studies are derived based on the authors’ recommendations on subjects such as promoting physical activity, as well as their critical view of the current policies adopted in tropical cities by the definition of public health intervention levels given by McKinlay (1998). The number of studies on downstream, midstream and upstream intervention levels was 6, 9 and 14, respectively.
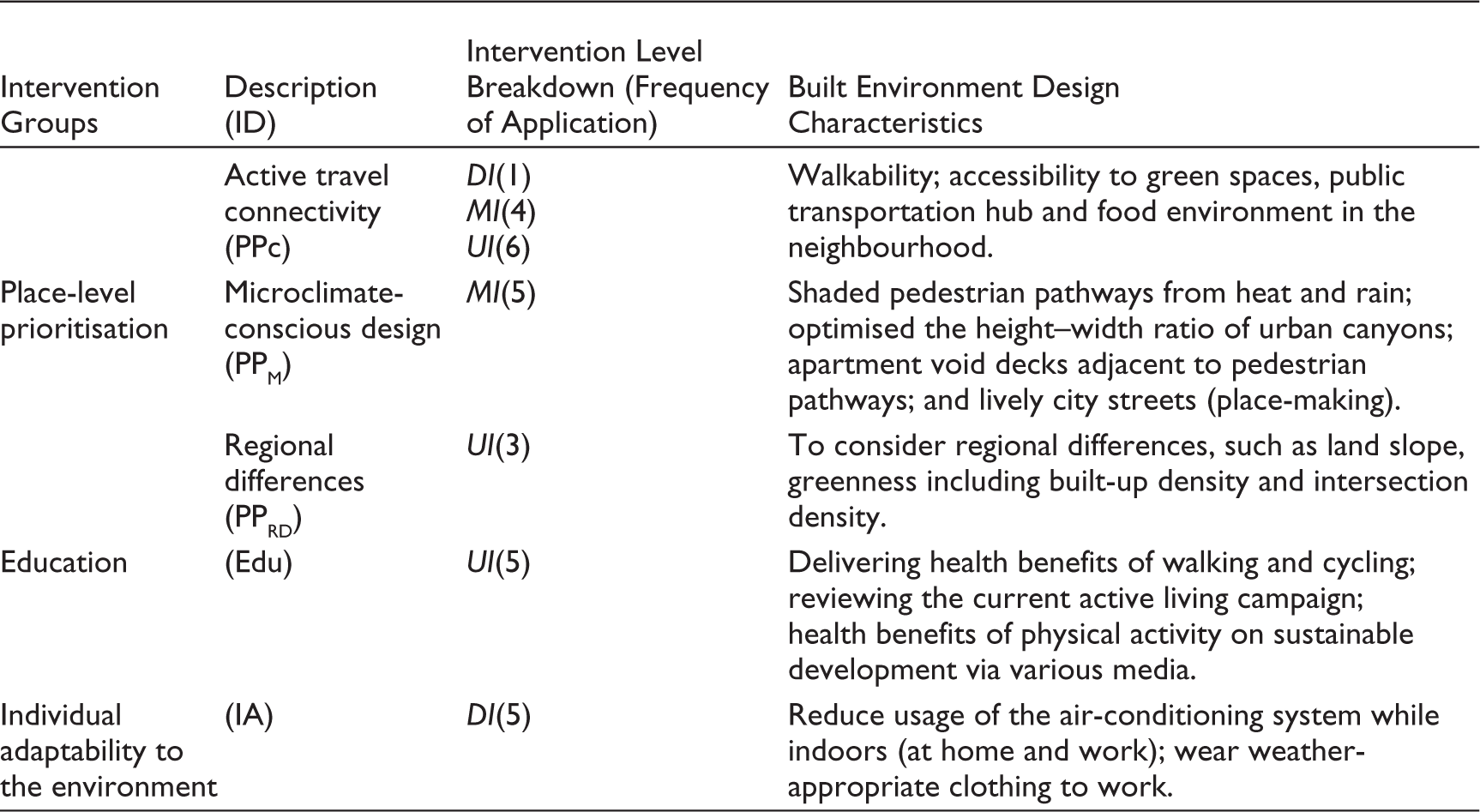
Table 2 shows the five groups of interventions from the included studies. The majority of the interventions reviewed emphasised place-level prioritisation (i.e., PPC and PPRD), which suggest the importance of recognising spatial heterogeneities as physical activity triggers, especially at the midstream and upstream levels. Meanwhile, interventions that observed the inhabitants’ sentiment toward the micro-environment and culture may be executed at midstream (i.e., PPM) and downstream (i.e., IA) levels. Encouragement of physical activity behaviour through education (i.e., Edu) is commonly seen as an upstream-level intervention and delivered via various media.
Five Groups of Interventions (n = 29).
Thematic Synthesis
A total of 494 free codes from eight descriptive themes were identified. The content of relevant nodes was streamlined by reorganising and omitting overlapping codes. Three analytical themes were synthesised into theme 1: social context, theme 2: environmental factors and theme 3: mechanisms to promote physical activity in the built environment. The implications for future research are discussed within each theme. Figure 2 shows the NVivo 11 text cloud which illustrates the 50 most frequent words used in each theme. The three most frequent words identified in themes 1, 2 and 3 are walking–health–income; temperature–outdoor–spaces; and health–urban–public, respectively. The word frequency is per their size.

Theme 1: The Social Context
Socio-Demography
Socio-economic conditions observed in developing tropical countries are directly associated with income, education level and neighbourhood aesthetic consciousness. Wealthier neighbourhoods are more likely to have proper road construction for private car use, access to well-maintained parks and pathways for walking and cycling for leisure rather than as a mode of transportation (Adlakha et al., 2016; Karuppannan & Sivam, 2013; Le Gouais et al., 2020; Wan Omar et al., 2013). However, higher-income residents have a lower likelihood of being physically active than their poorer counterparts. This is related to the former having busy lifestyles, thus reducing their time spent on physical activity. In contrast, the lack of advanced infrastructure available to the latter demographic group has made their daily activities more physically demanding (Cheah & Poh, 2014). In addition, with a low level of education, the poor communities have a limited understanding of health and only view physical activity as a necessity rather than leisure (Adlakha et al., 2016; Le Gouais et al., 2020). Rother (2020) pointed out that the act of self-efficacy is impeded by the social, economic and political environments that often go beyond a person’s means (e.g., excessive cost of bicycles, lack of dedicated bicycle lanes, and high rates of bicycle theft given their economic value).
Community Culture
The low participation rates in physical activity among the inhabitants of tropical cities have been determined to be associated with community attitudes and poor public health goal enforcement. For instance, poor air quality in Jamaica encouraged workers to use their private vehicles for their commute to work (Le Gouais et al., 2020). In Malaysia, physical activity is seen to have illness prevention measures but with varying levels of participation among its three major races (i.e., the Malays, Chinese and Indians). Compliance with the Health Belief Model (Champion & Skinner, 2008) was found to increase among the respondents when they perceived greater susceptibility to diseases associated with physical inactivity, a greater awareness of the benefits of walking, a higher self-efficacy and greater exposure to positive cues for action (Wan Omar et al., 2013).
Observation of participation in physical activity in most South Asian and Southeast Asian populations also showed lower female rather than male involvement. It is customary for women, specifically working mothers with small children, to perform caregiving and other domestic activities; thus, they have limited time for physical activity (Cheah & Poh, 2014; McKay, 2015). In another study, the female respondents were found to be more likely to use facilities within their neighbourhood like green spaces and apartment void decks that are located closer to their homes compared to their male counterparts (de Keijzer, 2019). Attempts to encourage both genders to participate in physical activities can be seen in the development of gender-inclusive outdoor facilities, particularly in wealthier neighbourhoods (Adlakha et al., 2016; Richards et al., 2020; Sarkar et al., 2018).
Interpersonal Constraints
The authors identified that despite the high level of health awareness as a result of physical activity, many inhabitants in tropical-built environments were reluctant to engage in regular walking because of interpersonal constraints. These include a lack of free time, weather, safety, laziness, crime, unsafe traffic, stray dogs and having a disability or health condition, as the most common among the female respondents. Watching television, playing video games, reading and socialising were preferred instead (Adlakha et al., 2016; Wan Omar et al., 2013). In another study, urban stressors such as noise were seen to reduce one’s long-term greenspace exposure (de Keijzer, 2019).
This theme focuses on the psycho-social aspects of physical activity in association with the environmental characteristics of the neighbourhoods under review. The attributes found in highly walkable neighbourhoods, such as more residential structures, more mixed land use and greater street connectivity, which are complemented by aesthetic attributes, are in line with demographics (Duncan & Mummery, 2005; Owen et al., 2004; Saelens et al., 2003) except for studies of higher-income neighbourhoods. However, the coexistence of underweight and overweight people among the low-income communities in tropical cities stresses the importance of investing in family-friendly facilities, healthy food availability and public transportation accessibility, thereby pursuing the decentralisation of the poverty model (de Lima et al., 2017; Wang & Woo, 2017).
Implication: Theme 1
Focusing on social context should include detailed observations and interviews that capture day-to-day life, particularly in the low-income sub-group population. Therefore, identifying their health issues is critical as most of this population lacks access to public health facilities or is burdened with self-efficacy constraints. Moreover, longer periods of observation through ethnography studies of local communities not only provide behavioural data from the targeted population but also an understanding of the usage pattern of certain built environment features.
The authors acknowledge the connection between built environment variables, such as travel time (i.e., issues of traffic congestion), safety (i.e., crime rate) and health via environmental quality (i.e., air quality, heat stress and noise pollution) and the three types of daily physical activity commonly practised, such as commuting to work, running errands and participating in leisure activities. Shortcomings or difficulties related to any of these variables have been reported to influence people to drive their motor vehicles. The workplace neighbourhood is a good example that possesses all three built environment variables. The main attributes of living in workplace neighbourhoods, such as the ability to commute to work by walking and bicycling and the degree to which designated parking areas are available to workers, have been observed in planned cities, specifically Putrajaya in Malaysia (Hashim et al., 2017) and Singapore (Karuppannan & Sivam, 2013).
Theme 2: Environmental Factors
Micro-Climate Conscious Design
The design of indoor and outdoor spaces with interchangeable transient and stationary conditions elicit behavioural responses, as seen in inhabitants’ choices in time spent, clothing insulation and type of activity. The provision of shade and protection from direct solar radiation is essential to promote participation in physical activity (Karuppannan & Sivam, 2013; McKay, 2015; Vidyarini & Maeda, 2019). Willingness to cycle and walk for daily trips is strongly influenced by the midday heat of tropical warm-humid weather, the availability of trees or shaded pathways and whether heavy sweating can be avoided or not (Hashim et al., 2017; Vidyarini & Maeda, 2019; Wan Omar et al., 2013). Anthropometrical factors like body mass index (BMI) and gender also play a role in influencing a person’s tolerance of warm weather. Studies have shown that those with higher BMI were less tolerant of participation in physical activity in warm weather compared to those with lower BMI. The female respondents were also found to be less physically active in warm weather compared to their male counterparts (Dahlan & Kurmanbekova, 2019; de Keijzer, 2019; Loo et al., 2017).
People in tropical climate countries preferred thermally cooler and dryer living, commuting and working environments (Dahlan & Gital, 2016; Krüger et al., 2015; Le Gouais et al., 2020; Vidyarini & Maeda, 2019; Wan Omar et al., 2013). The use of air-conditioning systems has an effect on thermal sensation in the short term, which emphasises the relationship between micro-climatic conditions and the overall bodily thermal response. Behavioural changes such as an increase in perceived alertness and thermal satisfaction among office workers in the tropics were observed following large indoor–outdoor air temperature differences (Cheung et al., 2017; Vidyarini & Maeda, 2019).
With considerable outdoor street designs, such as covered pathways, rain shelters and covered street furniture, inhabitants are prepared to participate in physical activity but only within a reasonable distance (Ahmed, 2003). In Singapore, the use of an apartment void deck is preferred by residents over neighbourhood open spaces. This is because the former spaces are covered, equipped with facilities, thermally comfortable with cross ventilation, and well-lit, making them suitable for social activities and studying while being connected to main pedestrian pathways (Karuppannan & Sivam, 2013). Micro-climate-conscious designs are commonly complemented with comprehensive pedestrian networks located in mixed land-use development and within close distances of the inhabitants’ homes and workplaces, making them ideal for walking and cycling (Adlakha et al., 2016; Dahlan & Kurmanbekova, 2019; Hashim et al., 2017). Wider streets were interpreted as attractive, safe and inviting given that pedestrians were seen to stay longer in them and engage in more physical activity compared to narrower streets (Ahmed, 2003; Richards et al., 2020; Wijesundara & Wijekoon, 2017).
Obesogenic Environment
The rise in obesity is associated with activities that have to do with the outdoors, such as commuting for work and access to food stores, restaurants, sports facilities, health facilities and parks, all within the circulation buffer zone in the neighbourhood (Adlakha et al., 2016; Aizawa, 2019; Coffee et al., 2013; Loo et al., 2017; Matozinhos et al., 2015; McKay, 2015; Yu et al., 2017). Nevertheless, the role of health and disease prevention even in low- and middle-income countries has a concordant relationship with physical activity despite built environment characteristics, such as land slope, greenness, built-up and intersection density (Valson et al., 2019). Other authors (Arundhana, 2018; Dahly et al., 2013; Le Gouais et al., 2020; Matozinhos et al., 2015; Sarkar et al., 2018; Valson et al., 2019) have advised against a ‘one-size-fits-all’ method to mitigate the rising incidences of NCDs, thus calling for prioritisation of physical activity intervention based on local spatial heterogeneity.
The downstream interventions (i.e., reducing the use of air conditioning, wearing clothing appropriate for warm tropical weather, and controlling the air pollution level) mainly reflect people’s likelihood of participating in physical activity when exposed to pro-environmental conditions while at home and work (Dahlan & Gital, 2016; Dahlan & Kurmanbekova, 2019; Tan et al., 2020). In terms of environmental quality, physical activity is associated with practices that comply with sustainable development goals (SDGs) through a reduction in traffic congestion and the level of air pollution (Rother, 2020; Wan Omar et al., 2013). Some authors second the notion that the walkable neighbourhood also contributes as a stress relief mechanism and extended exposure to features may reduce common health ailments, such as hypertension (de Keijzer, 2019; Sarkar et al., 2018; Wan Omar et al., 2013).
Implication: Theme 2
The intervention reviewed in this theme mainly aims to understand the changes in people’s response to dynamic environmental factors that can lead to healthy physical activity behaviour. Assessment of the reciprocal and dynamic relationships between people and places has been done using qualitative and quantitative methods, thus leading to a variety of physical activity intervention types suitable for each measured population. People’s judgement and interpretations of the environment that lead to changes in physical activity patterns may take time. Currently, individual psycho-physical investigations show more objective and specific responses to micro-climatic and built environment characteristics. Moreover, an assessment of the individual’s interpretation of his environment (i.e., workplace, home and neighbourhood) can be translated into spatial mapping to identify the effectiveness of physical activity design intervention at the street level. Both the interpretation and psycho-physical responses of the people should be considered for physical activity participation, thus warranting a built environment design that is responsive to the micro-climate and socioeconomic status of the population.
Sedentary office-working adults in the tropics have shown similar health risk factors as their temperate-country counterparts. Uniform neutral operative temperatures in the workplace and a high-calorie diet contribute to low metabolism, thus leading to imbalances in energy expenditure. The authors emphasise that the spatial heterogeneity in high- and low-income communities causes a lack of localised influences on environmental determinants that are obesogenic and disparate in health information between both populations.
In terms of climate-cultural expectations, consideration of providing flexible working hours in tropical countries by having intermittent break periods, coupled with a low-temperature difference between the indoors and outdoors will reduce workers’ sedentary behaviour while indoors. There are many reviews on people’s behaviour towards their built environment (Angkurawaranon et al., 2014; Malambo et al., 2016; Saelens & Handy, 2008; Tucker & Gilliland, 2007), but little has been said about changing work flexibility in tropical countries, where the climate can be challenging to workers who are acclimatised to the air-conditioned indoor spaces of their workplace.
Theme 3: Mechanism to Promote Physical Activity in a Tropical Built Environment
Facilitating Behavioural Changes
The creation of mixed land-use developments and a continuous pedestrian network has promoted more utilitarian physical activity, albeit facilitating place-making processes (Hashim et al., 2017; Karuppannan & Sivam, 2013; Richards et al., 2020; Wijesundara & Wijekoon, 2017). The organisation of street interventions through activities and sensory attractions fuel the pedestrians’ enjoyment and also serves as a stress release mechanism after a hard day’s work (Alba & Williams, 2013). These measures are indicators of how to secure a work–life balance, such as adjustment to long working hours, creation of ample leisure and personal care time and a short commute time (OECD, 2011; The Economist, 2017).
Reports on upstream interventions in many cities in both developed and developing countries, including Ghent, Hamburg, Helsinki, Madrid, Bogota, Brussels, Chengdu, Hyderabad, Salaya, Putrajaya and Milan urge the public to reduce their private car and motorcycle trips through policies set by the health ministry, transportation ministry and local governments (Fraszczyk et al., 2019; Hashim et al., 2017; Thondoo et al., 2020). Despite resistance and a slow response from the public, the outbreak of COVID-19 has shown that an extreme reduction in motorised movement on the roads can become a reality (Thondoo et al., 2020).
Health Awareness Campaign
Health awareness in tropical countries currently emphasises two-way mitigation intervention strategies between NCD control and the need for adaptation to achieve SDGs through the increase in physical activity. As an example, healthcare providers have been seen as convincing leaders and models for physical activity campaigns in the built environment. Physicians with healthier personal habits are more likely to encourage patients to adopt similar habits related to sustainability, such as transportation choices, energy use and involvement in local policies affecting land use and community design (Cheah & Poh, 2014; Rother, 2020). Training health care providers alongside urban planners and related design professionals on sustainable and climate-sensitive NCD problem-solving solutions in a tropical built environment can potentially provide a more holistic built environment design (Rother, 2020). In recognising that the built environment affects health and climate change, emphasising the role of public health providers through their actions and leadership is consistent with the findings of Younger et al. (2008).
Implication: Theme 3
More creative and critical strategies in terms of self-reported status on health awareness and micro-environment adaptability through data collection are needed to educate the public on the health benefits of physical activity. Mechanisms to promote physical activity behaviours should be designed based on downstream-level data gathered through a mixture of climate-cultural monitoring and ethnographic interviews. Discrepancies in the feedback from inhabitants between built environments in tropical and temperate areas are anticipated and should be considered in future built environment health determinant policies.
Despite identifying education as one of the most commonly used upstream-level interventions in this region (Table 2), its effectiveness in determining physical activity participation is not widely reported. A knowledge-attitude-practices (KAP) survey administered to focus groups in the community allows an understanding of the tendencies (or indirect observable action), and observable action towards physical activity. KAP should be considered to complement the education intervention.
Multifaceted Interventions for Physical Activity in Tropical Built Environments
The multifaceted factors intervention model for physical activity behaviour change (MIPA) (Figure 3) is proposed as a tool to design potential interventions dedicated to the midstream and downstream levels. The model consists of four components: (a) the built environment variable which covers aspects such as safety, aesthetics and reasonable travel time factor; (b) environmental quality and micro-climate conscious design; (c) the health awareness level and (d) the self-efficacy factors. The compliance degree for the first and the third components is represented by the horizontal left (−) to right (+). Meanwhile, both the second and fourth components have ascending vertical compliance degrees; from (−) to (+). The likelihood of positive physical activity behaviour can only be represented via a diagonal flow from a double (−) corner to a double (+) corner. Flows to and from combined (+) and (−) corners are not applicable and should be neglected.

To illustrate the utility of the model, we considered the introduction of a new apartment with a void deck design. The proposed intervention is likely to involve a changing range of specific environmental variables, such as people’s awareness towards health benefits, connectivity of the void deck with home-to-work travels, pedestrian and cycling routes, and ample lighting. The variables in each component are instigated and may change based on evidence-based findings from the social interactions, for example, observations based on the changes like interactions between private motorcycle users who view the void deck as a convenient place to park their motorcycles, and pedestrians. The interventions leading to the double (+) corner of MIPA suggest good facilitators for physical activity implementation at the said apartment and at the same time educate the private motorcycle users to respect the pedestrian dedicated spaces.
To ensure up-to-date intervention strategies, variables in each component have to be generated through participatory sessions that involve multiple-discipline professional town planning stakeholders, policymakers and public health practitioners. The proposed interventions through the physical and social aspects within the MIPA model can either be executed in phases or simultaneously, as long as the said interventions comply with safety, work–life balance and local environmental quality standards, promote health awareness and facilitate self-efficacy.
Strengths and Limitations
This article limits its analysis to the working adult sub-group. Synthesis stratification from broader population sub-groups can be used to improve the specificity of findings. The structure of our analysis reflects only the frequency of the themes generated based on the aim and objective of the synthesis. Although newer relevant material may have been missed, our investigation seeks to identify the likelihood of a built environment design promoting physical activity based on current (the 2000s to 2020s) physical activity constraints, intervention delivery levels and mechanisms within the context of tropical cities. It is possible that relevant papers were missed because the search terms used were not specific to occupational intensity. Further investigation is needed to explore the impact of occupational intensity in tropical-built environments on workers’ decision-making concerning participation in physical activity.
Studies investigating either indoor or outdoor thermal comfort perceptions were excluded from this review as we only focused on transient thermal comfort perceptions in tropical built environments (i.e., moving from indoor to outdoor and vice versa). Nevertheless, understanding pedestrian outdoor thermal comfort experiences in other non-tropical micro-climates and dependence on climate-controlled building interiors may provide further insight into people’s walking behaviours, various thermo-regulatory and psycho-social reactions to changes in the built environment.
Conclusion
This study aims to discuss the current literature regarding participation in physical activities by working adults in tropical-built environments in response to their social context, climate-cultural expectations and awareness of health benefits. Twenty-nine studies were used to synthesise three interrelated themes. The majority of the authors emphasised the importance of physical activity, especially among the low-socioeconomic status community, which is also the predominant demographic group in the tropical region. Like others, we noted that few evaluative studies that articulate environmental changes, particularly in tropical built environments act to promote physical activity or call for greater consideration for place-level prioritisation, which we found to be a more promising intervention strategy than its ‘one-size-fits-all’ counterpart. In addition, we deduced that ‘place-level prioritisation’ through multifaceted factors encourages traits unique to the daily lives of the majority of people in tropical built environments. Our findings suggest that downstream and midstream delivery levels of intervention will most likely empower the public to participate in physical activity in their daily lives. The MIPA model describes a general relationship of causal pathways which can be applied to a range of environmental interventions, particularly to the tropical built environment. It is simple enough to be used by town planning-related experts, public health policymakers and researchers in conceptualising future physical activity interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.