
Abstract
Introduction:
Attention-deficit/hyperactivity disorder (ADHD) is a prevalent neurodevelopmental condition in children and adolescents, yet randomized controlled trial evidence supporting pharmacological treatment in Chinese populations remains limited. This study evaluated the efficacy and safety of clonidine hydrochloride extended-release tablets (CLON-XR) as monotherapies for ADHD among Chinese children and adolescents.
Materials and Methods:
In this 6-week, multicenter, randomized, double-blind, placebo-controlled phase 3 trial, 75 patients aged 6–17 years with ADHD were assigned (2:1) to receive once-daily CLON-XR (target dosage 0.2 mg/day) or placebo. The primary endpoint was the change from baseline to week 5 in the Swanson, Nolan, and Pelham Version-IV (SNAP-IV) total score. Secondary endpoints included SNAP-IV subscales, Clinical Global Impression—Severity (CGI-S) and Improvement (CGI-I) scores, and safety assessments.
Results:
Compared with placebo, CLON-XR significantly improved the primary endpoint (least squares mean change in the SNAP-IV total score: −17.5 vs. −10.3; p = 0.0039). Significant improvements were also observed in the SNAP-IV inattention and hyperactivity/impulsivity subscales, CGI-S, and CGI-I (all p < 0.05). The incidence of treatment-emergent adverse events (TEAEs) in the CLON-XR group was comparable with that in the placebo group; the TEAEs were mild, and the dropout rate was low (5.3%). No serious adverse events or clinically significant vital sign abnormalities were reported.
Conclusions:
CLON-XR was efficacious and well tolerated in Chinese children and adolescents with ADHD, supporting its potential as a nonstimulant treatment option in this population. These findings provide evidence for ADHD management in China and suggest that further investigations in longer-term and real-world settings are needed.
Keywords
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common chronic neurodevelopmental disorder characterized primarily by attention deficit and/or hyperactivity impulses disproportionate to the level of development (Committee on Quality Improvement, Subcommittee on Attention-Deficit/Hyperactivity Disorder, 2000).
The prevalence of ADHD in Chinese children is 6.4% (Li et al., 2022), with cases predominantly distributed between the ages of 4 and 17 years. However, owing to a lack of timely diagnosis and intervention, the disorder persists into adulthood for approximately 65% of these children, resulting in far-reaching negative effects on the individuals, their families, and society (Polanczyk et al., 2015; Wang et al., 2017).
The pathophysiology of ADHD is strongly linked to prefrontal cortex (PFC) dysfunction. Specifically, dysregulation of PFC-related neurotransmitter systems—with particular emphasis on catecholamines—is a well-established mechanism (Xing et al., 2016). The PFC function exhibits an inverted U-shaped dose-response relationship with catecholamine levels: both deficient and excessive dopamine or norepinephrine (NE) signaling can impair cognitive control and emotional regulation. Accordingly, optimizing catecholaminergic activity in the PFC represents a principal mechanism through which pharmacotherapies exert their therapeutic effects in ADHD (Arnsten and Rubia, 2012).
ADHD therapeutics include pharmacotherapy, behavioral therapy, and a combination of both. Early and effective treatment has been reported to lead to a better prognosis. Central stimulants and non-stimulants have demonstrated efficacy and are approved by the American Food and Drug Administration (FDA) for the treatment of ADHD in American adolescents (Childress and Berry, 2012). However, 20%–30% of children with ADHD do not experience adequate symptom relief and are affected by adverse side effects. Therefore, non-stimulant medications are often recommended as alternatives (Connor et al., 2000; Pozzi M et al., 2020). These agents primarily include selective NE reuptake inhibitors and α2-adrenergic receptor agonists.
Clonidine is an α2-adrenergic receptor agonist that may improve the core symptoms of ADHD by enhancing prefrontal cortical function (Sharma and Couture, 2014). Although the immediate-release formulation of clonidine showed some efficacy in the treatment of ADHD, its requirement for multiple daily doses results in marked fluctuations in plasma concentration, which may increase the risk of adverse effects such as sedation and hypotension (Connor et al., 1999). In addition, immediate-release clonidine is not approved by the FDA for the treatment of ADHD, which limits its clinical application. In contrast, extended-release formulations approximate steady drug release and reduce peak–trough concentration variability, thereby effectively minimizing adverse reactions and improving medication adherence. In 2010, the U.S. FDA approved clonidine extended-release tablets for the treatment of ADHD, and this formulation has been recommended in several international guidelines for managing ADHD and its comorbidities (Barbaresi et al., 2020; Wolraich et al., 2019; Zheng and Liu, 2015).
Available evidence indicates that clonidine, either as a monotherapy or in combination, shows good efficacy and safety in children and adolescents with ADHD (Cannon et al., 2009; Hazell and Stuart, 2003; Hunt et al., 1985; Jain et al., 2011). However, these studies were primarily conducted in European and American populations, with relatively scarce data in Asian populations. Furthermore, CYP2D6, the primary metabolizing enzyme of clonidine, is characterized by well-established East–West genetic polymorphisms (Byeon et al., 2018; Li et al., 2019), which could theoretically influence its metabolic rate and drug exposure. Although previous bioequivalence studies have shown that clonidine extended-release tablets approved in China have overall pharmacokinetic profiles similar to those of the extended-release U.S. reference product Kapvay (Xiamen LP Pharmaceutical Co., Ltd., in-house data), the actual impact of genetic differences in CYP2D6 on clinical outcomes still needs to be verified in a Chinese population.
This study aims to report the main results of a phase III clinical trial of clonidine extended-release tablets in Chinese children and adolescents with ADHD, providing local evidence to support its clinical application.
Materials and Methods
Patient population
Patients (aged 6–17 years) were diagnosed with ADHD by a specialist psychiatrist according to the criteria set forth in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), with intelligence quotient estimated to be ≥70 on the Wechsler Abbreviated Scale of Intelligence, a total score ≥26 on the Swanson, Nolan, and Pelham Version-IV (SNAP-IV) scale (National Medical Products Administration of China, 2021), and the ability to swallow tablets. Patients with comorbid tic disorders or oppositional defiant disorder were also eligible, as these are common comorbidities of ADHD.
Patients were excluded if they had (1) a current diagnosis or history of a psychiatric disorder that required psychotropic medication or may interfere with assessment of clonidine efficacy and safety, such as autism spectrum disorder, anxiety disorders, mood disorders, or other neurodevelopmental conditions necessitating psychotropic treatment; (2) a history of conduct disorders, syncopal episodes, or seizures; (3) current or past drug abuse; (4) a history of clonidine intolerance; or (5) used any investigational drug within 30 days of the study initiation or had a positive drug test result. Patients were also excluded if they had clinically significant abnormalities in vital signs, physical examination, clinical laboratory tests, or electrocardiogram (ECG) readings, based on the normal reference ranges defined in Diagnostics. Females of childbearing age who were pregnant were also excluded.
The study protocol, amendments, and informed consent forms were approved by central and local institutional review boards before study initiation. Prior to the initiation of any study procedure, written informed consent was obtained from the parent(s) or legal guardian(s) of each patient. In addition, patient assent was obtained in a tiered manner based on age and cognitive capacity: for patients deemed by the investigator to be capable of understanding the study and providing autonomous assent, the investigator explained the study content in an age-appropriate manner and obtained written informed assent; for patients under 8 years of age or those considered incapable of providing assent, age-appropriate explanations were provided, and verbal assent was obtained.
Study design
This 6-week, parallel-group, randomized, double-blind, placebo-controlled study was conducted at seven centers in China from December 2019 to October 2020. The study began with a screening period to determine eligibility, followed by baseline assessments and a 2-week washout period, during which all current ADHD medications were discontinued. Patients who completed the screening and washout periods were assigned to the next available randomization number and randomly allocated in a 2:1 ratio to receive clonidine hydrochloride extended-release tablets (CLON-XR) (Xiamen LP Pharmaceutical Co., Ltd.) or placebo. Matching clonidine and placebo tablets were provided at each clinic visit (weeks 1, 3, 5, and 6)according to the randomization schedule. Compliance was evaluated by tablet count at each visit. The 6-week double-blind treatment period included a 1-week dose escalation period, a 4-week stabilization period, and a 1-week dose tapering period for discontinuation. The target dosage was 0.2 mg/day, which was maintained for 4 weeks; thus, patients received 0.1 mg tablets at bedtime during week 1, with an equal split dosage of 0.1 mg tablets being given in the morning and at bedtime during weeks 2–5 and 0.1 mg tablets at bedtime during week 6. All randomized patients who received at least one dose of the study medication were included in the safety analysis set. The primary efficacy analysis was based on the intent-to-treat (ITT) principle. The ITT population was defined as all randomized patients who received at least one dose of the study medication and had at least one post-baseline assessment record for the primary efficacy measure (SNAP-IV total score). For patients who discontinued the study early, their last observation was carried forward (LOCF) to week 5 for the primary endpoint analysis. Safety and efficacy outcomes were assessed at each clinic visit, and a final safety assessment was conducted 1 to 2 weeks after cessation of the study medication.
The study was registered with the China Drug Trials Registry under the National Medical Products Administration’s Center for Drug Evaluation (http://www.chinadrugtrials.org.cn: CTR20191871). The trials were conducted in accordance with the International Council on Harmonization of Good Clinical Practice guidelines and the ethical principles of the Declaration of Helsinki. This was a double-blind trial in which patients, investigators, and study staff remained blinded to treatment assignment throughout the study. An independent statistician generated the randomization schedule using SAS software and maintained the blinding code. Randomization was stratified by study center, and sealed emergency envelopes indicating treatment assignment (CLON-XR or placebo) were prepared for each randomization number and stored at each site. These envelopes were to be opened only in case of medical emergencies or serious adverse events (SAEs) requiring unblinding for clinical management. The blind was maintained until database lock. Study medications were packaged identically to ensure blinding.
Study assessments
Primary efficacy measure (SNAP-IV)
The primary efficacy measure was the change in the SNAP-IV total score from baseline to week 5. The SNAP-IV, a 26-item scale, consists of Inattention (Items 1–9), Hyperactivity/Impulsivity (Items 10–18), and Oppositionality (Items 19–26) (Swanson et al., 2001). The 26 items of the SNAP-IV are rated on a four-point Likert scale (0 = not at all, 1 = just a little, 2 = quite a bit, 3 = very much). This study utilized the simplified Chinese version of the SNAP-IV-Parent, which has been shown to have good validity and reliability and has been widely applied in clinical trials to assess the efficacy of medications for children with ADHD (Zhou et al., 2013). SNAP-IV assessments were completed by investigators based on semi-structured interviews with parents and direct clinical observation during clinic visits. This structured approach integrated multisource information to ensure a comprehensive and consistent evaluation of ADHD symptoms across all participants and study sites.
Secondary efficacy measures
The Clinical Global Impression (CGI) is a validated, standardized clinical assessment tool comprising two subscales: the Clinical Global Impression of Severity (CGI-S) and the Clinical Global Impression of Improvement (CGI-I). The CGI-S and CGI-I are also widely used tools in clinical psychiatric assessment (Busner and Targum, 2007; Hall et al., 2020; Kollins et al., 2011). On the basis of a review of the literature and considering real-world clinical application, the secondary outcome measures included improvements in scores from baseline to week 5 on SNAP-IV hyperactivity/impulsivity and inattention subscales and the CGI-S and CGI-I. The CGI-S is rated on a seven-point scale (from 1 = normal, not at all ill, to 7 = among the most extremely ill), and the CGI-I is rated on a seven-point scale (from 1 = very much improved to 7 = very much worse) (Guy, 1976). Treatment responders were defined as patients with a CGI-I score of 1 (very much improved) or 2 (much improved) at week 5. The SNAP-IV, CGI-S, and CGI-I were completed by the investigator.
Safety measures
Safety assessments included adverse events (AEs), vital signs, ECGs, and clinical laboratory tests. Throughout the study, any untoward medical occurrence was recorded as an AE. Treatment-emergent adverse events (TEAEs) were defined as AEs that occurred following the initiation of the study drug or placebo. All AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA) version 23.1.
At each visit, adverse events were actively solicited using non-leading questions and systematically documented. The following details were recorded for each event: the reported term and corresponding MedDRA preferred term; dates of onset and resolution; duration; severity (graded as mild, moderate, or severe); relationship to the study drug (assessed on a five-point scale: definitely, probably, possibly, probably not, or definitely not related); interventions taken; impact on study drug administration; outcome; and classification as a SAE.
Patients were required to attend the research site for six to seven scheduled visits. At each visit, vital signs (body temperature, blood pressure, and heart rate) were monitored, concomitant medications were documented, and AEs were recorded. Laboratory tests—including complete blood count, blood chemistry, and urinalysis—were performed at screening and at the end of the treatment period. During the treatment phase, 12-lead ECGs were obtained at all visits except Visit 4. For female patients who had reached menarche, urine pregnancy tests were conducted at Visits 1, 2, and 6. All patients, whether they completed the study or withdrew prematurely, returned for a follow-up visit 1 to 2 weeks after treatment discontinuation, during which time concomitant medications and AEs were again documented.
Statistical analyses
Statistical analysis was performed using SAS version 9.4. All predefined primary statistical efficacy analyses were conducted in the ITT population, defined as all randomized subjects who took at least 1 dose of study medication with at least 1 postrandomization assessment of the primary efficacy variable available for analysis. The sample size was calculated on the basis of data from the pivotal trial of Kapvay (Jain et al., 2011), in which the mean changes from baseline in the ADHD-RS-IV total score were −15.6 points (SD = 12.96) for the active treatment group and −7.5 points (SD = 9.41) for the placebo group. Assuming similar efficacy and variability in the present study, a mean improvement in the SNAP-IV total score of −15.5 points (SD = 13) for the CLON-XR group and −8.0 points (SD = 9.5) for the placebo group was adopted. With a two-sided α of 0.05, 90% power, a 2:1 randomization, and an estimated 10% dropout rate, a total of 75 patients (50 in the CLON-XR group and 25 in the placebo group) were required to detect a statistically significant difference.
Improvement from baseline to week 5 in the SNAP-IV total score in the CLON-XR group versus the placebo group was analyzed using analysis of covariance with terms for the baseline SNAP-IV score, study site, and treatment group. A LOCF method was used to account for patients who discontinued the study before week 5. Analyses of secondary end points were similar to those of the primary efficacy variables. Effect size was calculated on the basis of the observed mean differences between the groups and the observed SDs using the unbiased version of Hedges’ g. Safety data (i.e., TEAEs, vital signs, and ECGs) were collected from the defined safety population (i.e., all patients who received at least 1 dose of study medication or placebo) and were presented as descriptive statistics.
Results
Patient disposition
Of the 83 patients screened, 75 were randomized and received treatment (placebo, n = 24; CLON-XR, n = 51; Fig. 1). All the placebo-treated patients (100%) completed the study, and in 92.2% of the patients were in the CLON-XR group. Discontinuations due to adverse events and withdrawals occurred in 3.9% of patients in the CLON-XR group.
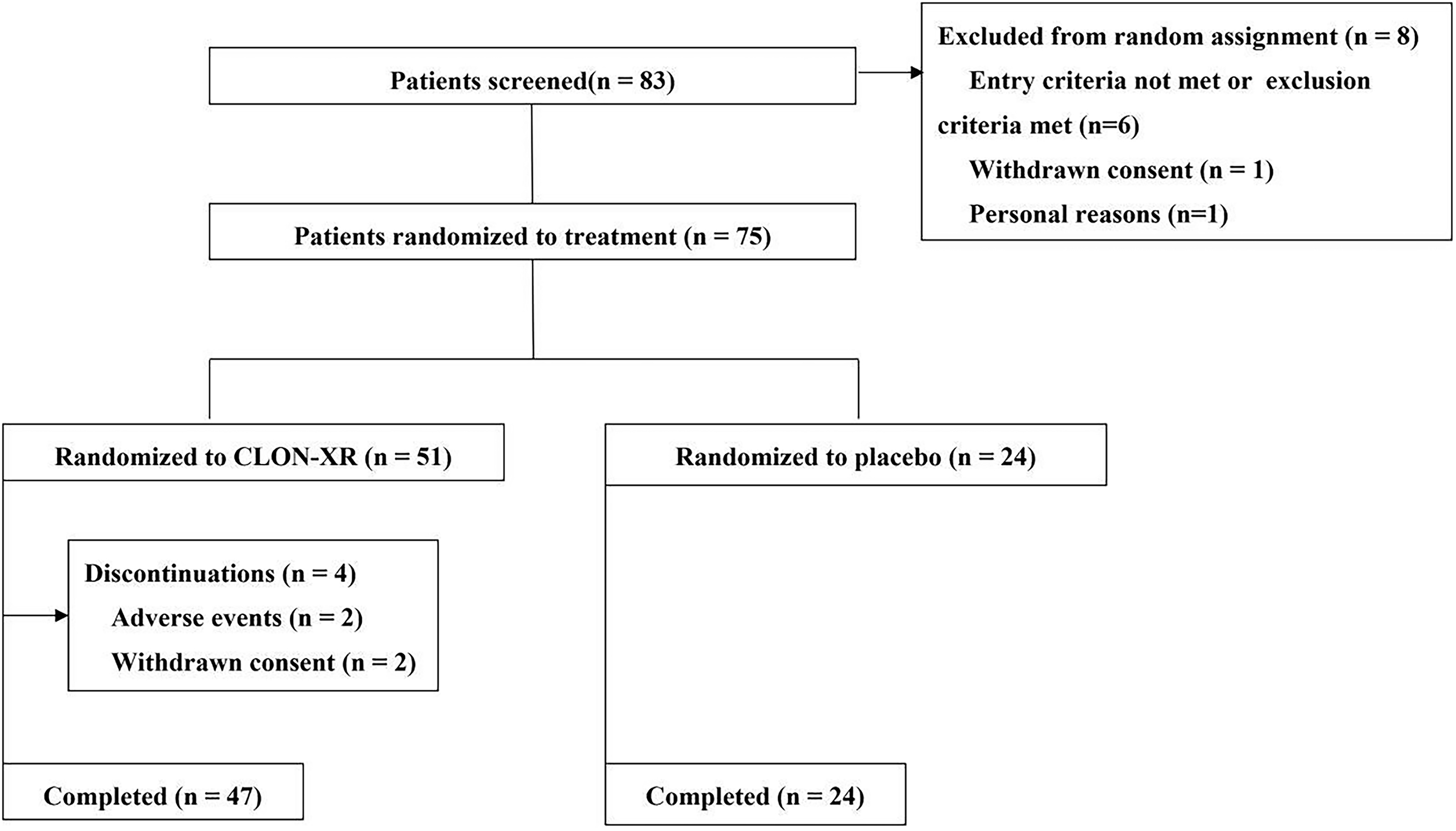
Patient disposition. Note: CLON-XR = clonidine hydrochloride extended-release tablets.
The demographic and baseline characteristics were comparable between the groups (Table 1). The mean age (SD) of patients at baseline was 9.0 (1.95) years for CLON-XR and 8.7 (1.83) years for placebo, with fewer patients in the 12- to 17-year age group. The distribution of ages was not significantly different between the CLON-XR group and the placebo group. The majority of the enrolled patients were boys (85.3%), which is consistent with the epidemiology of ADHD. The CLON-XR and placebo groups were comparable in terms of weight, full-scale intelligence quotient, and SNAP-IV total score.
Patient Demographics and Characteristics (ITT Population)

FIQ, full-scale intelligence quotient; ITT, intent to treat; SD, standard deviation.
Efficacy
Primary efficacy measure (SNAP-IV)
The mean reduction from baseline to week 5 in the SNAP-IV total score was significantly greater with CLON-XR (−17.5) than with placebo (−10.3; p = 0.0039), with an effect size of −0.69 (95% Cl: −1.16 to −0.23, Table 2). Repeated measures analysis revealed that the change in the SNAP-IV total score at week 5 in the CLON-XR group was significantly greater than that in the placebo group (p < 0.0001).
Improvement in the SNAP-IV Total Scores from Baseline to Week 5 (ITT Population)
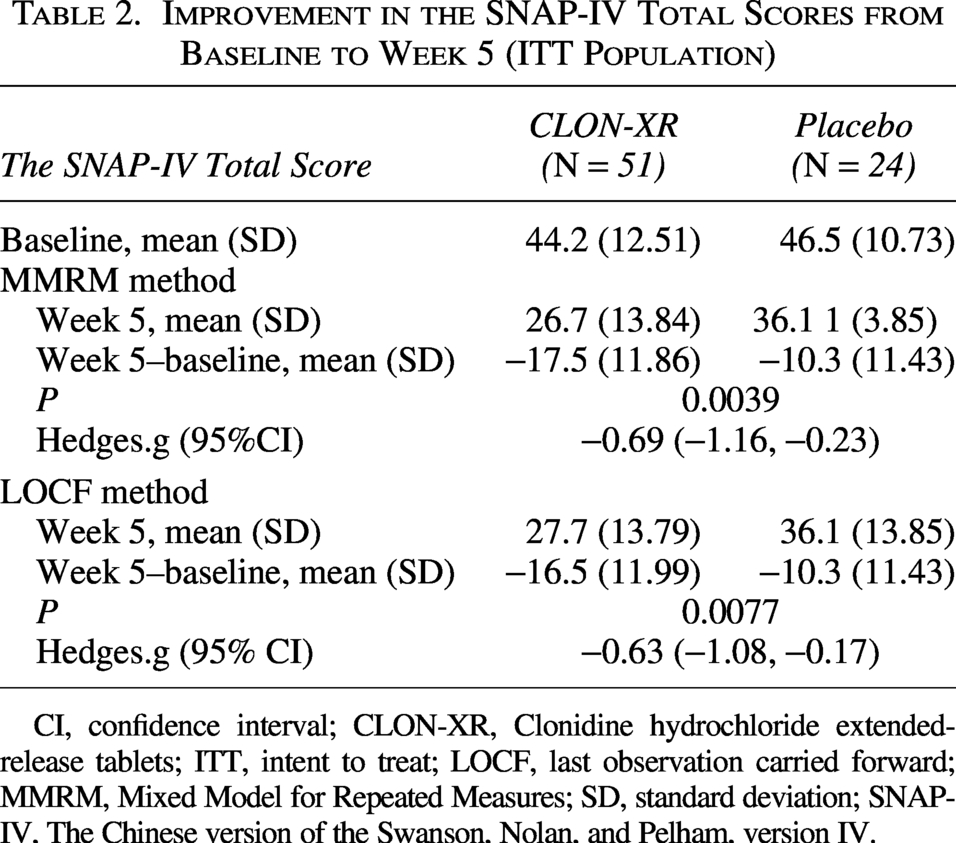
CI, confidence interval; CLON-XR, Clonidine hydrochloride extended-release tablets; ITT, intent to treat; LOCF, last observation carried forward; MMRM, Mixed Model for Repeated Measures; SD, standard deviation; SNAP-IV, The Chinese version of the Swanson, Nolan, and Pelham, version IV.
Between-group differences in the reduction in the SNAP-IV total score emerged by week 1 and were sustained throughout treatment (Fig. 2), and symptoms of patients with ADHD were almost eliminated after 3 weeks of medication. The mean change in the SNAP-IV total score of the CLON-XR group versus that of the placebo group was −8.8 versus −4.9 from baseline to week 1, −15.6 versus −9.6 from baseline to week 3, and −17.1 versus −11.3 from baseline to week 6, respectively.

SNAP-IV total scores over 5 weeks of treatment. Note: Patients in the CLON-XR group had a more significant reduction in symptoms compared with those in the placebo group over the whole treatment period. CLON-XR = clonidine hydrochloride extended-release tablets; SNAP-IV, Swanson, Nolan, and Pelham, version IV; a p < 0.05.
Secondary efficacy measures
Reductions in scores on the inattention and hyperactivity subscales of the SNAP-IV, CGI-I, and CGI-S were also significantly greater in the CLON-XR group than in the placebo group from baseline to week 5 (Table 3). The mean change in the SNAP-IV inattention subscale score from baseline to week 5 was −6.5 for the CLON-XR group and −4.7 for the placebo group (p = 0.0275). The mean changes from baseline to week 5 in the SNAP-IV hyperactivity/impulsivity subscale score were −6.8 in the CLON-XR group and −3.1 in the placebo group (p = 0.0006).
Improvement in Secondary Efficacy Measures from Baseline to Week 5 (ITT Population)
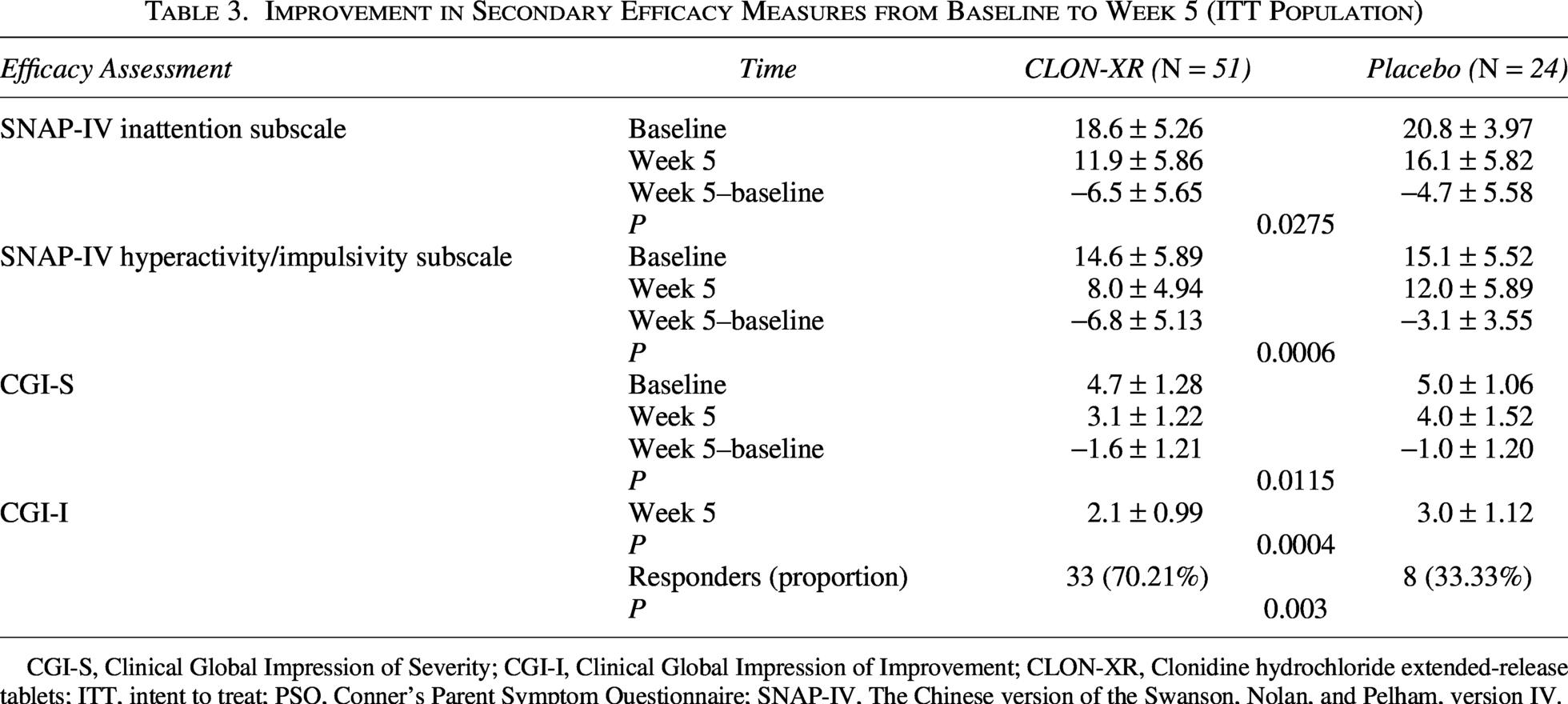
CGI-S, Clinical Global Impression of Severity; CGI-I, Clinical Global Impression of Improvement; CLON-XR, Clonidine hydrochloride extended-release tablets; ITT, intent to treat; PSQ, Conner’s Parent Symptom Questionnaire; SNAP-IV, The Chinese version of the Swanson, Nolan, and Pelham, version IV.
The mean change in the CGI-S score from baseline to week 5 was −1.6 for the CLON-XR group and −1.0 for the placebo group. The decrease in the CLON-XR group was significantly greater than that in the placebo group (p = 0.0115). At week 5, the CGI-I score was 2.1 in the CLON-XR group and 3.0 in the placebo group, and the difference was statistically significant (p = 0.0004). In accordance with the CGI scale grading criteria defined in the Methods section, approximately 70.21% of patients who received CLON-XR were classified as responders and were rated as minimally, much, or very much improved, whereas in the placebo group, only 33.33% were classified as responders (p = 0.003).
Because ADHD is more common among younger boys, we further performed analyses in different age and gender groups. When age was incorporated into the primary efficacy analysis, there was a statistically significant difference between the CLON-XR group and the placebo group in the 6- to 12-year-old age group (p = 0.0037; Fig. 3). When gender was incorporated into the primary efficacy analysis, a statistically significant difference was observed in the male group (p = 0.0065; Fig. 3).
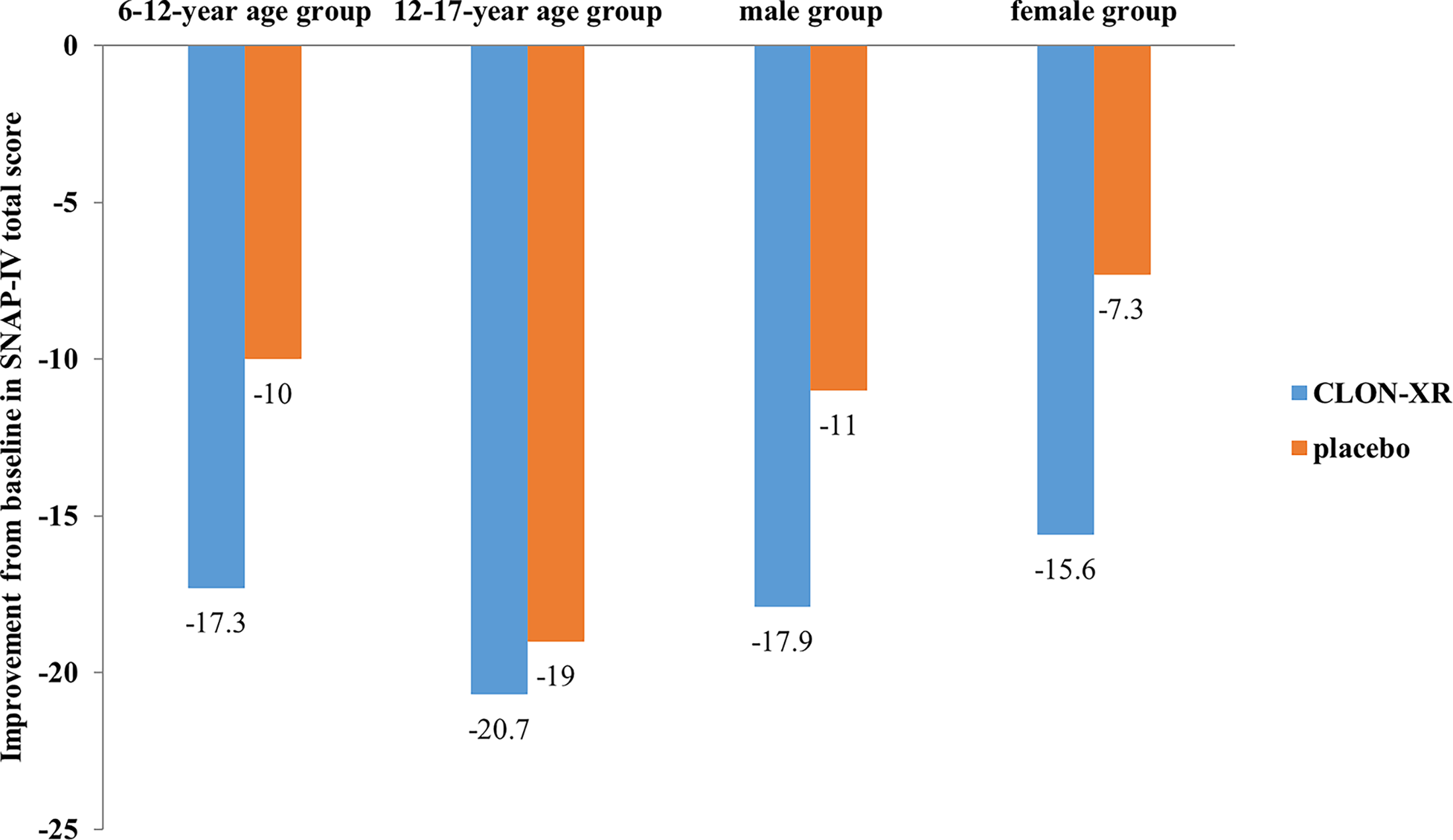
Improvement from baseline to week 5 on SNAP-IV total score by age and gender. Note: Improvement was significantly greater in the CLON-XR group versus placebo group in the 6- to 12-year-old age group and male group. CLON-XR = clonidine hydrochloride extended-release tablets; SNAP-IV, Swanson, Nolan, and Pelham, version IV.
Safety
In this study, the patient dropout rate was low (5.3%), and medication compliance was good. The compliance rates of all 75 randomly enrolled patients from baseline to week 5 and during the whole study period were 94.05% and 95.77%, respectively. In the CLON-XR group, the compliance rates from baseline to week 5 and during the whole study period were 93.18% and 94.70%, respectively (Table 4). Compliance was slightly higher in the placebo group than in the CLON-XR group.
Patient Compliance at Week 5 and in the Whole Study Period

CLON-XR, Clonidine hydrochloride extended-release tablets; SD, standard deviation.
TEAEs of ≥5% in CLON-XR Group and ≥2-Fold More Frequent Than in Placebo (Safety Population)
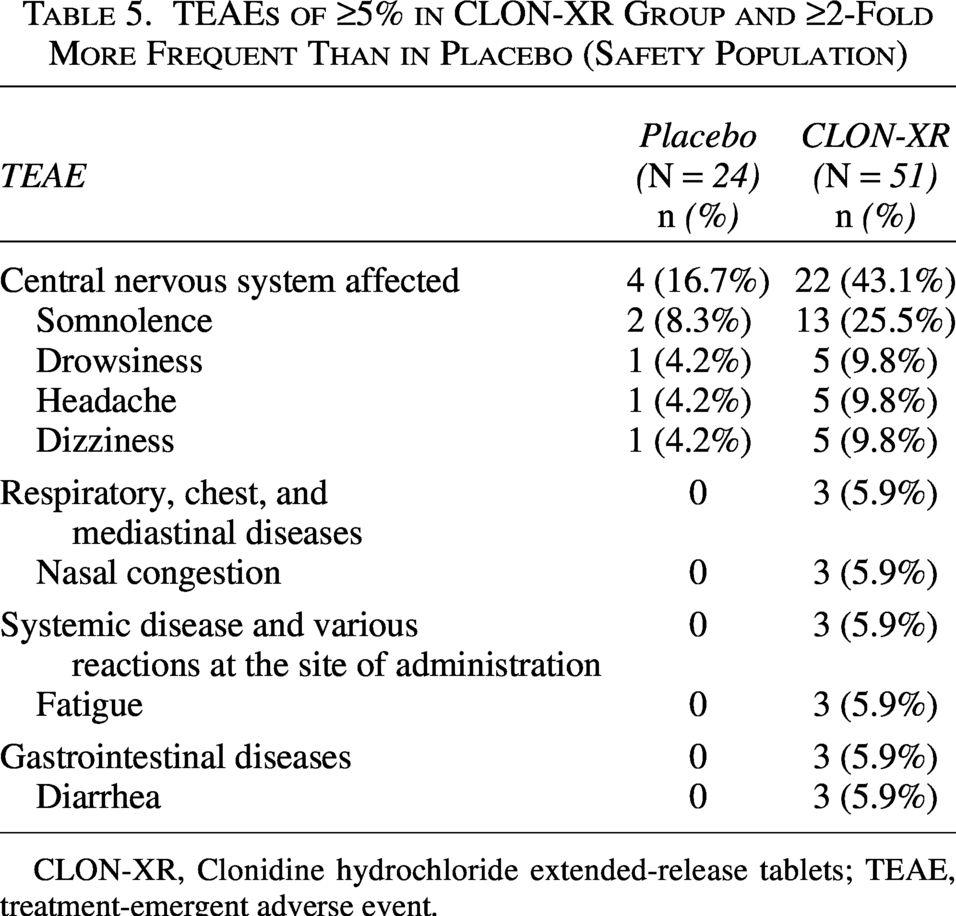
CLON-XR, Clonidine hydrochloride extended-release tablets; TEAE, treatment-emergent adverse event.
Overall, 74.5% and 70.8% of patients who received CLON-XR or placebo, respectively, reported a TEAE. Treatment-related TEAEs were reported by 7 patients receiving placebo (29.2%) and 24 patients receiving CLON-XR (47.1%). The most common TEAEs with an incidence of ≥5% are listed in Table 5. The most common TEAEs in the CLON-XR group were as follows: somnolence (n = 13, 25.5%), drowsiness (n = 5, 9.8%), headache (n = 5, 9.8%), and dizziness (n = 5, 9.8%). Most TEAEs were mild or moderate. No deaths or serious TEAEs occurred during the study. TEAEs that led to discontinuation occurred in 2.7% of patients, and the researchers determined that those TEAEs were not drug related. No clinically meaningful changes were observed in vital signs, laboratory parameters, ECGs, or physical examinations.
Discussion
This study is the first report of results from a randomized, double-blind, placebo-controlled trial assessing the safety and efficacy of CLON-XR in Chinese children and adolescents with ADHD. ADHD is a common neurodevelopmental disorder characterized by inattention, hyperactivity, and impulsive behavior (American Psychiatric Association, 2013), which often persists into adulthood and impairs learning, social functioning, and daily life.
At present, there are few types of drugs on the market for the treatment of ADHD in China, and although stimulants are the most commonly prescribed medications, their use is limited in some patients with ADHD because of safety considerations (including appetite suppression, sleep disorders, and inhibition of growth and development), potential addiction, no or poor response in some patients, and inadequate dosages prescribed by clinicians (Becker et al., 2016; Clemow and Walker, 2014; Deng et al., 2021). Nonstimulant atomoxetine is available; however, approximately 40% of patients continue to experience clinically significant symptoms despite treatment (Da Silva et al., 2023; Guo et al., 2024).
The efficacy of nonstimulant medications such as the α2-adrenergic agonists clonidine and guanfacine has been demonstrated in patients with ADHD (Cortese et al., 2021). Clonidine is an α2 adrenergic receptor agonist that reduces sympathetic outflow and presynaptic α2 receptors, decreasing NE release and thereby mitigating hyperactivity, impulsivity, and inattention (Isaac, 1981; Kawaura et al., 2014; Philbin et al., 2010).
However, immediate-release formulations of clonidine, including somnolence and sedation, have untoward effects (Daviss et al., 2008; Spiller et al., 2013). Furthermore, clonidine IR often requires frequent administration, which further complicates its use. Extended-release formulations of clonidine (i.e., CLON-XR) have been developed to overcome the AEs associated with the fluctuating pharmacokinetics of immediate-release formulations (Clemow and Walker, 2014). CLON-XR is a stable matrix tablet formulation that, following oral administration, releases clonidine gradually over a 12-hour period, thus permitting once- or twice-daily administration (Croxtall, 2011). The results of the present study demonstrated that the nonaddictive CLON-XR significantly improved ADHD symptoms and had a good safety profile, potentially serving as a new treatment option for Chinese children and adolescents with ADHD.
In studies, the observed gender differences in prevalence may stem from sociocultural factors, such as the encouragement of boys to participate in sports and related activities, while girls are often steered toward quieter pursuits. As a result, ADHD in boys tends to be more readily recognized by parents and teachers, leading to a higher detection rate of the disorder.
Efficacy
This trial was a phase III multicenter clinical trial assessing the efficacy and safety of CLON-XR in the treatment of ADHD. The effectiveness results revealed that compared with the placebo group, the CLON-XR group had significantly lower scores for the primary and secondary efficacy indicators, namely, the SNAP-IV total score, the SNAP-IV inattention and hyperactivity/impulsivity subscale score, and the CGI score, indicating that 0.2 mg/day CLON-XR can significantly improve the core symptoms (including attention deficit and hyperactivity/impulsivity) and overall function in patients with ADHD. Notably, this study revealed that the SNAP-IV total scores in the CLON-XR group were significantly lower than those in the placebo group as early as the first week of treatment, and this advantage was consistently maintained across all subsequent visits. This pattern aligns with the early onset of efficacy previously reported for extended-release clonidine by Jain et al. (2011). The results of the present study further confirm that the efficacy of extended-release clonidine in treating ADHD in patients aged 6–17 years is consistent with findings from previous studies (Cannon et al., 2009; Hazell and Stuart, 2003; Hunt et al., 1985; Jain et al., 2011).
In addition, clonidine is recommended as a first-line treatment for patients with ADHD with comorbid tic disorders, and studies have shown that clonidine significantly improves tic symptoms and is effective at relieving tic symptoms in patients with ADHD (Barbaresi et al., 2020; Joo and Kim, 2018). Patients with ADHD often suffer from sleep problems, and clonidine has been shown to help improve sleep quality in patients with ADHD by stimulating the γ-aminobutyric acid system and inhibiting the release and transport of NE. This effect has been validated in children with ADHD or other neurodevelopmental disorders (Angriman et al., 2015; Jang et al., 2022; Lewis et al., 2023; Naguy, 2016).
Safety and tolerability
CLON-XR was well tolerated in the study subjects, with most TEAEs being mild to moderate and no severe adverse events. Like immediate-release clonidine (Daviss et al., 2008) and guanfacine (Biederman et al., 2008), somnolence was the most common TEAE. No clinically meaningful changes were observed in vital signs or ECGs. High medication adherence (95.77%) and a low dropout rate (5.3%) further support the favorable safety profile of CLON-XR in children with ADHD and adolescents in China.
Clonidine has demonstrated efficacy and safety in ADHD across multiple studies (Cannon et al., 2009; Hazell and Stuart, 2003; Hunt et al., 1985; Jain et al., 2011; Luan et al., 2017; Ming et al., 2011). Given that ADHD requires long-term management and that poor adherence—largely driven by adverse effects (63%) or insufficient efficacy (15.5%) (Minrong et al., 2014)—negatively impacts outcomes, the favorable safety and efficacy profile of CLON-XR supports its potential as a long-term treatment option.
Limitations of this study that may affect the ability to generalize these findings include the relatively small sample size and the study design of forced dose escalation. The design did not allow clinicians to adjust the dose according to a patient’s weight or age; thus, the results may overestimate the safety concerns associated with CLON-XR in clinical practice. An additional potential limitation is that the distinct side-effect profile of CLON-XR, notably somnolence, might have introduced a risk of inadvertent unblinding among some participants or investigators. Future trials may consider incorporating objective biomarkers or placebo-controlled run-in designs to further mitigate this concern, and long-term trials are warranted to validate the efficacy of CLON-XR.
Conclusions
The clonidine hydrochloride extended-release tablets were generally well tolerated and significantly improved ADHD symptoms in this study population. This work supports the potential clinical use of clonidine in the treatment of ADHD children and adolescents with ADHD China and highlights the need for further research and validation.
Clinical Significance
This study provides direct evidence supporting the clinical use of CLON-XR in Chinese patients aged 6–17 years with ADHD. The results position CLON-XR as a recommended, effective, and well-tolerated non-stimulant option within the treatment spectrum for ADHD in China.
Authors’ Contributions
Q.Y.: Conception and design of the study; enrolled patients; participated in data acquisition, analysis, interpretation, and presentation; writing the original draft; drafting the article; and revising the intellectual content. K.X.Y., G.F., C.W.X., W.W.G., L.Y.P., D.L.J., and L.H.F.: enrolled patients and participated in data acquisition, analysis, interpretation, and presentation; drafted the article; and revising the intellectual content. D.Y.S.: Writing—review and editing.
Footnotes
Acknowledgments
The authors thank the investigators and their clinical staff as well as the many patients who generously agreed to participate in this clinical trial. The authors would also like to thank the clinical operations staff for their excellent trial implementation and support.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.