
Abstract
Objective
Recent research on psychosocial interventions addressing the well-being of women with HIV/AIDS has brought new options for practitioners. This study critically reviews the treatment features, methodological quality, and efficacy of these interventions.
Methods
A comprehensive search between 2000 and 2011 identified 19 studies employing 10 different interventions.
Results
In all, 11 studies were methodologically strong and 12 reported interventions superior to other treatments. Among those with positive results, Cohen’s effect sizes ranged from small (d = 0.33) to large (d = 1.50) across well-being outcomes. The Cognitive Behavioral Stress Management/Expressive Supportive and Structural Ecosystems Therapies ranked as probably efficacious. The Teaching, Raising and Communicating with Kids and the Maternal HIV Self-Care Symptom Management programs were ranked as promising treatments.
In the United States, among the estimated 1.1 million persons living with HIV by the end of 2010, 280,000 (24%) were women (The Henry Kaiser Family Foundation, 2013). For the first time since 2008, new HIV infections among women decreased significantly by the end of 2010 (The Henry Kaiser Family Foundation, 2013). However, minority women, particularly Black women, continued to be disproportionately affected. Black and Hispanic/Latina women accounted for 64% and 15% of new infections, while representing only 13% and 16%, respectively, of the U.S. female population (The Henry Kaiser Family Foundation, 2013). HIV incident rates were 20 and 4 times higher for Black and Hispanic/ Latina women, respectively, when compared to the rate of White women (Kates, Hoff, Levine, Carbaugh, & Gutierrez, 2013). In 2009, HIV disease was the fourth leading cause of death among Black women aged 25–44 (Kates et al., 2013).
Approximately 76% of new HIV infections in women occur between the ages of 13 and 44, the childbearing years (Murphy, Marelich, Dello-Stritto, Swendeman, & Witkin, 2002). Family responsibilities may hinder or reinforce the effective management of their illness (Kates et al., 2013), and children dependent on their parents in HIV-affected families are especially vulnerable (Schuster et al., 2000). Thus, in addition to facing the challenges of living with a stigmatizing chronic illness, HIV-infected mothers must meet the demands of childrearing, plan for an uncertain future, and buffer the negative impact that the disease has on their families (Murphy et al., 2002; Murphy, Greenwell, Moutappa, Brecht, & Schuster, 2006).
Highly active antiretroviral therapies (HAARTs) have slowed the progression of HIV symptoms. The benefits of a prolonged life and improved health for HIV-infected women come with stringent adherence to complex antiretroviral medication regimens and daily life challenges in coping with this chronic illness (Bova, 2000). Some women may develop symptoms not only from the illness itself but also from medications, and opportunistic infections, which diminish physical functioning, add psychological distress and create psychosocial problems in parenting, mobilization of social support, and daily self-care activities that need attention (Hudson, Lee, & Portillo, 2003; Murphy, Roberts, & Herbeck, 2011; Silver, Bauman, Camacho, & Hudis, 2003).
Most HIV-infected women live in poverty, depend on public assistance, and are the sole caregivers for their children (Murphy et al., 2002). Some women may omit or postpone caring for their HIV disease because they must attend to other basic competing needs related to subsistence, caregiving responsibilities, and relationship problems (Moore, 2011).
In the early years of the AIDS epidemic, the development of HIV-related preventive or other interventions for women was mostly considered in the context of preventing mother-to-child or sexual partner transmission of the virus (Bova, 2000). Psychosocial care interventions for HIV-infected women only emerged in the mid-1990s, when practitioners focused on issues uniquely related to women living with HIV/AIDS, including environmental and societal macrostructural factors. These factors included delayed diagnosis, poor access to care, and antiretroviral medication, competing priorities related to the woman’s caregiver role and social location, HIV-related stigma, drug use, poverty, intimate partner violence, lack of social support, low educational attainment, and psychological distress (Bova, 2000; Watkins-Hayes, Pittman-Gay, & Beaman, 2012).
In the last decade, gender-specific interventions have been developed or tailored to address the multidimensional psychosocial needs of this population, at different stages of the disease trajectory (Abramowitz & Greene, 2005). However, the few rigorous reviews found in the literature have focused on preventive interventions for women at risk of contracting HIV rather than treatment or care interventions for women who are already living with HIV/AIDS (Crepaz et al., 2009; Lichtenstein & Malow, 2010). The primary aim of this study is to examine the efficacy of HIV/AIDS psychosocial care interventions for women. To guide both practice and research, this critical review seeks to answer the following questions: (a) What are the most effective psychosocial interventions for women living with HIV/AIDS? (b) What is the level of evidentiary support for each intervention? (c) What are the methodological features and rigor for each study? (d) What are the treatment characteristics of the interventions?
Method
This article synthesizes the empirical literature and examines the methodological quality, treatment characteristics, and efficacy of gender-specific empirical interventions that address the well-being and psychosocial needs of women diagnosed with HIV/AIDS. The search was limited to reporting findings from quantitative studies published in peer-reviewed journals over the past decade in the United States and which tested psychosocial interventions for HIV-infected women. The last decade has witnessed the proliferation of psychosocial care interventions for women living with HIV/AIDS, making this field sufficiently developed to warrant an examination of only quantitative studies. Specifically, studies were included if they (a) were published between 2000 and 2011; (b) were conducted in the United States; (c) included quantitative (e.g., experimental trials, pilot studies, quasi-experimental) or mixed-method designs (quantitative/qualitative) with the quantitative portion reported in this review; (d) reported psychosocial outcomes; and (e) included adults (>18 years of age).
Search Methods
The following databases were searched: Social Service Abstracts, Sociological Abstracts, Medline, PubMed, PsycInfo, CINAHL Plus, Scopus, Campbell Collaboration Library, and the Cochrane Library of Systematic Reviews. Manual searches of the reference section of the identified studies were also utilized to identify additional pertinent interventions. Key words employed in this search using Boolean logic with “and”, “not” or “or” included: HIV/AIDS, HIV infection, HIV, AIDS, women, mother*, female*, intervention*, treatment*, psychotherapy*, and therap*.
After duplicate citation removal, the search yielded 35 studies, 19 of which met criteria for inclusion. These 19 studies published between 2003 and 2011 within 10 journals composed the final sample for this review.
Review Criteria: Descriptive and Critical
Treatment and methodological variables were extracted and organized to present a descriptive analysis for each study in this review. Treatment variables included in this analysis comprised the following: setting, sample characteristics, theoretical framework and goals of the treatment, intervention format, recruitment/retention incentives, and a description of the clinician delivering the treatment. Methodological characteristics included study type, research design, primary and secondary measures utilized, attrition rates, statistical analyses used, and study quality rating.
To derive the study quality rating, each intervention was evaluated using the Quality of Evidence Score (QES) rating system developed by Becker and Curry (2008). This scale integrates 14 methodological study quality attributes from three different sources: 6 items from the Consolidating Standards of Reporting Trials current version (Moher, Jones, & Lepage, 2001), 4 attributes from the Methodological Quality Rating Scale (Miller et al., 1995), and 4 design variables that reflect recent advances in clinical intervention research. Becker and Curry (2008) modified some extracted items (e.g., enumerate dropouts/attrition) increasing its sensitivity to discriminate between methodologically weak and strong studies (i.e., inclusion of drop outs in the statistical analysis). Ratings of the 14 individual attributes were added to calculate total QES for each study, yielding a possible range from 0 to 15. In addition, each study was classified as either methodologically weak (QES below the median) or methodologically strong (QES equal or above the median).
Treatment Effects and Efficacy
There were several benchmarks used for determining treatment effects and efficacy. First, for studies with treatment and comparison groups design, the effect size was calculated as the difference between the intervention group’s mean posttest score and the comparison group’s mean posttest score divided by the pooled standard deviation (Cohen, 1988). Second, this calculation was repeated for each follow-up measure for those studies assessing effects of the intervention against the comparison group across time. The magnitude of the effect size was interpreted using Cohen’s (1988) classification: small (.20), medium (.50), and large (.80).
To determine the overall efficacy of the interventions, two methods were used. The first was based on the standards set by Chambless and Hollon (1998), and Chambless et al. (1998) for identifying “efficacious” and “possibly efficacious” treatments. These criteria require the following study characteristics:
Comparison with a no-treatment control group, alternative treatment group, or placebo in a randomized control trial, controlled single case experiment, or equivalent time-sample design, and in which the tested treatment is statistically significantly superior to no treatment, placebo, or alternative treatments, or in which the tested treatment is equivalent to a treatment already established in efficacy, and power is sufficient to detect moderate differences.
These studies must have been conducted with a treatment manual or its logical equivalent; a population treated for specific problems, for whom inclusion criteria have been delineated in a reliable and valid manner; reliable and valid outcome assessment measures, at minimum tapping the problems targeted for change; and appropriate data analysis.
For a designation of efficacious, the superiority of the expressive–supportive therapy (EST) must have been shown in at least two independent research settings (sample size of three or more at each site in the case of single case experiments). If there is conflicting evidence, the preponderance of the well-controlled data must support the EST’s efficacy.
For a designation of possibly efficacious, one study suffices in the absence of conflicting evidence.
Relatively new areas of intervention study may not reach the high standards for efficacious or possibly efficacious, and thus a category was added. In their critical review of interventions in another relatively unexplored area (group treatments for adolescent alcohol and drug abuse), Engle and Macgowan (2009) created another category called “some indication of positive outcomes.” This category comprised Chambless and Hollon’s second and fourth criteria mentioned earlier but includes single-group designs in which pretest to posttest and/or follow-up assessments indicated a statistically significant benefit but that did not outperform (or was not tested against) a comparison condition.
A second method identified superior treatments by cross-referencing methodologically strong studies (i.e., high QES scores) with a classification of their intervention effects. Specifically, QES study results were “dichotomously coded as having positive [P] or neutral/negative results [N/N], with indication of superior immediate outcomes relative to a comparison condition considered as positive findings in support of an intervention” (Becker & Curry, pp. 534–535).
Results
This section reviews the treatment and methodological quality of the studies and evaluates the efficacy of the treatments.
Treatment Features
The 19 studies, shown in Table 1, tested 10 different interventions in 3 treatment modalities: 5 group interventions (n = 10), 1 family therapy approach (n = 5), and 4 individual interventions (n = 4). The 5 group interventions are Cognitive Behavioral Stress Management (CBSM; Antoni et al., 2008)/Cognitive Behavioral Stress Management/Expressive Supportive Therapy (CBSM+; Jones et al., 2003, 2007, 2010; LaPerriere et al., 2005; Lechner et al., 2003), Positive Life Skills Workshop Project (PLS; Bova, Burwick, & Quiñones, 2008), Enhanced Sexual Health Intervention (ESHI; Wyatt et al., 2004), Protect and Respect program (Teti et al., 2010), and peer-based symptom management intervention using the Peer-based Intervention for Symptom Management (PRISM-HIV; Webel, 2010).
Interventions for HIV-Infected Women: Treatment Variables.

Note. AA = African American; ACASI = audio computer-assisted self-interview; ACS = Adherence coordination services; As = Asian American; B= Black; BDI = Beck’s depression index; beh = behavioral; Car = Caribbean American; Cau = Caucasian; CBSM/CBSM+ = Cognitive–Behavioral Stress Management/Expressive Supportive Therapy; CDC = Centers for Disease Control and Prevention; CM= case manager; Comm = community; CSA= childhood sexual abuse; ctrl = control; DDT = Directly Delivered Therapy; depre = depression; DoM = Discovery of Meaning Writing intervention; dx = diagnosis; edu= educational; ESHI = Enhanced Sexual Health intervention; exp = experience; fam = family; fem = female; F/T = full time; fx = functioning; GLI = group level intervention; gp(s) = group(s); HAART = highly active antiretroviral treatment; HG = Health group; HCP = Health care providers; hr = hour; HS = high school; Hs = Hispanic-American; Ht = Haitian-American; hv = home visit; hx = history; ind = individual; jrnal = journal; Lat = Latina; M = mean; med = medication; mgmt = management; MH = mental health; min(s) = minute(s); Mix = mixed racial/ethnic; mo(s) = month(s); MPH = Master’s in Public Health; MSC-HIV = Maternal HIV Self-care symptom management intervention; MSW = master’s level social worker; mtg = meeting; NA = Native American; N/A = not applicable; NR = not reported; O = other race/ethnicity; PA = public assistance; pc= phone call; PCA= Person-Centered Approach therapy; PLS= Positive Life Skills; P & R = Protect and Respect project; PRISM-HIV = Peer-based intervention for symptom management; P/T = part time; SA = substance abuse; SES = socio-economic status; SET= Structural Ecosystems therapy; SoA = South American; SOC= Standard of Care; TRACK = Teaching, raising and communicating with kids program tx = treatment; VL = viral load; W = White; wk(ly) = week(ly); WLH/A = woman living with HIV/AIDS.
The Structural Ecosystems Therapy (SET), the only family intervention included in this review, was used in 5 of the 19 studies (Feaster, Brincks et al., 2010; Feaster, Burns, et al., 2010; Feaster, Mitrani, et al., 2010; Mitrani, McCabe, Robinson, Weiss-Laxer, & Feaster, 2010; Szapocznik et al., 2004). SET aimed to reduce psychological distress, increase family support, improve medication adherence, prevent substance abuse relapse in HIV-infected women, and provide benefits for those women in this population who care for children.
The four individual interventions included Teaching, Raising, and Communicating with Kids program (TRACK; Murphy, Armistead, Marelich, Payne, & Herbeck, 2011), HIV Maternal Self-care Symptom Management (Miles et al., 2003), Discovery of Meaning program (DoM; Westling, Garcia, & Mann, 2007), and Directly Delivered Therapy (DDT; Visnegarwala et al., 2006). Four separate studies test each of the interventions in this category. The first two interventions, guided by family systems, self-efficacy, or cognitive reframing treatment change theories, targeted specific concerns among populations of HIV-infected mothers. The DoM intervention utilized a positive psychology construct (i.e., discovery of meaning in response to illness) as theoretical guide. Treatment delivered in the family home or the community often addressed some of the multiple environmental factors impacting HIV-infected women’s well-being behaviors, such as barriers in accessing care and HIV-related issues of privacy and confidentiality, disclosure, and stigma. In contrast, treatments delivered in clinic- or office-based settings may complicate access to treatment for some women, while offering others privacy away from home or the neighborhood, and additional support from peers or professionals.
A range of theoretical models were used, either alone or in combination, including ecosystemic, cognitive–behavioral, social learning, peer health education, gender/power, stress appraisal coping, stages of change, risk reduction, and stress-related growth. For example, SET and TRACK targeted changes in the woman’s contextual environment and her different relationships in this milieu (Murphy, Armistead, et al., 2011; Szapocznik et al., 2004). In contrast, CBSM+, PLS, and MSC-HIV aimed to improve well-being outcomes by delivering knowledge on coping skills and facilitating practice and generalization of newly acquired skills (Bova et al., 2008; Jones et al., 2003; Miles et al., 2003). The use of well-established theories in the development of these interventions represented strength across the reviewed studies, regardless of which theory is acknowledged with greater prominence. Family intervention treated women or mothers living with HIV/AIDS; while group treatments, especially in the early stages of intervention development, treated women who met Centers for Disease Control and Prevention guidelines for case-defined AIDS.
The studies included diverse outcomes, and some targeted more than one including (a) reducing levels of distress; (b) improving antiretroviral medication adherence; and (c) increasing the social support among HIV-infected women. For example, SET aimed to reduce psychological distress by decreasing family hassles and mobilizing the family as a supportive resource to buffer the effects of the stressors (Szapocznik et al., 2004). Furthermore, operational definitions and measurements of HIV-infected women’s distress varied across studies and interventions. For example, distress can be measured as parenting stress, HIV-related stress (i.e., stigma and failing physical health), family hassles, emotional distress (i.e., depression and anxiety), traumatic life events, quality of life, and family environment. Consequently, different instruments were used to measure psychosocial distress, which adds difficulty to the task of comparing well-being outcomes between studies. The Parenting Stress Index, the Brief Symptom Inventory, and the Quality of Life Scale were some of the instruments utilized by more than one researcher for this purpose (Lechner et al., 2003; Murphy, Armistead, et al., 2011; Szapocznik et al., 2004). In addition, some of the self-reported measures used in the studies were originally developed among White, middle-class population, which questions their validity when applied to the racial and ethnically diverse population of HIV-infected women. For example, Miles et al. (2003) employed the Medical Outcomes Survey-HIV, a tool not designed to measure the health of low-income African American mothers with HIV.
Several of the reviewed interventions tested their efficacy on improving health outcomes, such as medication adherence (PLS, SET, CBSM+, and DDT), HIV-related risk reduction behaviors (P&R and ESHI), or symptom management (MSC-HIV and PRISM-HIV). Finally, 6 of the 10 interventions analyzed in this review (PLS, SET, Department of Correction; CBSM/CBSM+, MSC-HIV, and DDT) established objectives or formulated hypotheses related to social support. The concept of social support appeared more difficult to conceptualize and measure than the distress construct. Intervention studies on HIV-infected women considered social support a resource for coping with this chronic illness and improving this population’s well-being.
A variety of professionals and paraprofessionals delivered the program including nurses, social workers, psychologists, peer educators/reach out workers, and other master’s degree level psychotherapists or health educators (Table 1). Eight (42%) studies identified the interventionist by gender and/or race/ethnicity to match the female participants as a desirable feature, and 12 (63%) reported details on the interventionist’s competence, such as credentials, training, years of experience, or discipline, which may facilitate the replicability of the studies. The four interventions fully or partially facilitated by peers (P&R, PRISM-HIV, ESHI, and DDT) utilized community natives whose shared demographic characteristics and life experiences with the patients may facilitate linkages of the women to health services (Kenya, Chida, Symes, & Shor-Posner, 2011).
Methodological Features
Eight studies used experimental designs, including one in a mixed-methods study, and 11 were quasi-experimental studies (Table 2). Of the 11 quasi-experimental studies, 9 had pretest–posttest, nonequivalent control group designs, 1 included historical comparisons, and 1 used a pretest–posttest single group design. The median QES across studies was 8, with a range from 4 to 14. Eleven (58%) studies were methodologically strong (QES ≥ 8; Antoni et al., 2008; Feaster, Brincks et al., 2010; Feaster, Burns et al., 2010; Feaster, Mitrani et al., 2010; Jones et al., 2003; Miles et al., 2003; Mitrani et al., 2010; Murphy, Armistead, et al., 2011; Szapocznik et al., 2004; Teti et al., 2010; Webel, 2010) and eight (42%) utilized weaker methodological designs (QES < 8; Bova et al., 2008; Jones et al., 2007, 2010; LaPerriere et al., 2005; Lechner et al., 2003; Visnegarwala et al., 2006; Westling et al., 2007; Wyatt et al., 2004).
Interventions for HIV-Infected Women: Methodological Variables and Quality of Evidence (Becker & Curry, 2008).
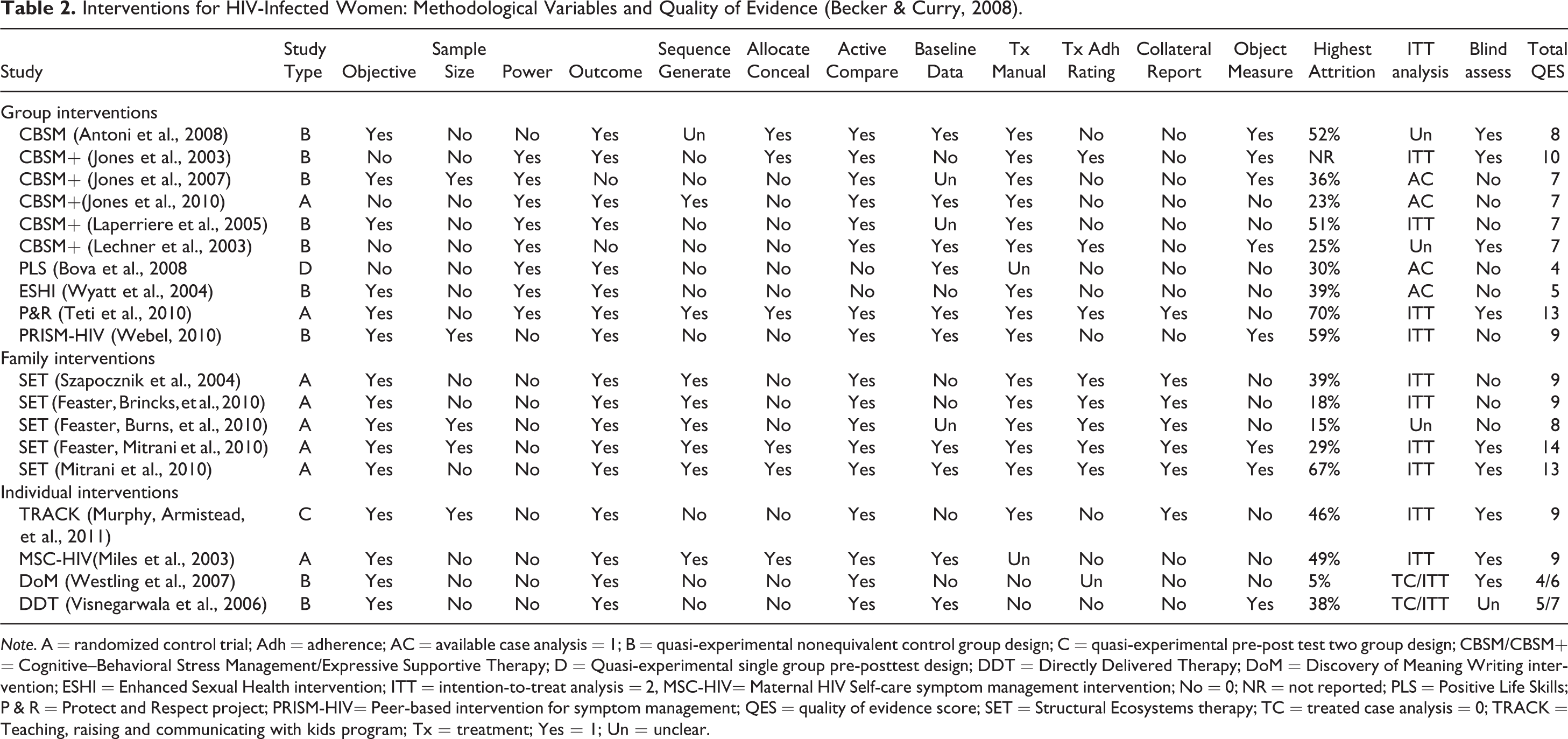
Note. A = randomized control trial; Adh = adherence; AC = available case analysis = 1; B = quasi-experimental nonequivalent control group design; C = quasi-experimental pre-post test two group design; CBSM/CBSM+ = Cognitive–Behavioral Stress Management/Expressive Supportive Therapy; D = Quasi-experimental single group pre-posttest design; DDT = Directly Delivered Therapy; DoM = Discovery of Meaning Writing intervention; ESHI = Enhanced Sexual Health intervention; ITT = intention-to-treat analysis = 2, MSC-HIV= Maternal HIV Self-care symptom management intervention; No = 0; NR = not reported; PLS = Positive Life Skills; P & R = Protect and Respect project; PRISM-HIV= Peer-based intervention for symptom management; QES = quality of evidence score; SET = Structural Ecosystems therapy; TC = treated case analysis = 0; TRACK = Teaching, raising and communicating with kids program; Tx = treatment; Yes = 1; Un = unclear.
The methodologically strong studies, several of which tested SET, consistently used the following attributes: report of study objectives, use of an active comparison group, explicit primary outcomes, manualized treatment, intention-to-treat (ITT) analyses, and inclusion of detailed baseline data (demographic and clinical attributes). In contrast, the methodologically weak studies testing CBSM/CBSM+, TRACK, and MSC-HIV lacked the following design features: low retention and attrition rates, a priori power/sample size determination, clear randomization procedures, treatment allocation concealment, blind assessment, standardized treatment protocols, treatment adherence rating, collateral reports, objective and culturally sensitive measures, and consistent use of ITT analyses.
Seven studies testing the CBSM (Antoni el al., 2008; LaPerriere et al., 2005), P&R (Teti et al., 2010), PRISM-HIV (Webel, 2010), SET (Mitrani et al., 2010), the MSC-HIV (Miles et al., 2003), and TRACK (Murphy, Armistead, et al, 2011) interventions reported research attrition rates over 40% related to the completion of follow-up measures. Of the 19 studies testing the CBSM+, SET, PRISM-HIV, P&R, and DoM treatments, 13 offered monetary (US$40 to US$330) and/or other incentives (e.g., transportation, meals) for the completion of data collection during study visits.
Efficacy of Treatments
Three separate criteria guided the critical assessment of the efficacy of the reviewed interventions: (a) evidence of treatment superiority in two or more methodologically stronger studies (Becker & Curry, 2008); (b) analysis of computable effect sizes; and (c) examination of the extent to which each intervention met the criteria for level of empirical support developed by Chambless and collaborators (Chambless et al., 1998; Chambless & Hollon, 1998), with the modifications by Engle and Macgowan (2009).
Evidence of treatment superiority
Of the 10 reviewed interventions, only CBSM/CBSM+ and SET were replicated in separate studies; therefore, comparison between total number of studies with positive results only applies to these 2 interventions. Evidence of treatment superiority as defined by Becker and Curry (2008) could not be analyzed for the other eight interventions. Of the six studies evaluating CBSM/CBSM+, two were methodologically strong (Antoni et al., 2008, QES = 8; Jones et al., 2003, QES = 10), and only one of these found positive results. Antoni et al. (2008) found superior outcomes compared to another active treatment condition, a reduced dosage of CBSM. The other two CBSM+ studies with positive well-being outcomes (Jones et al., 2007; LaPerriere et al., 2005) were weak in methodological quality (QES = 7; Table 3).
Evidence of Effect Sizes.
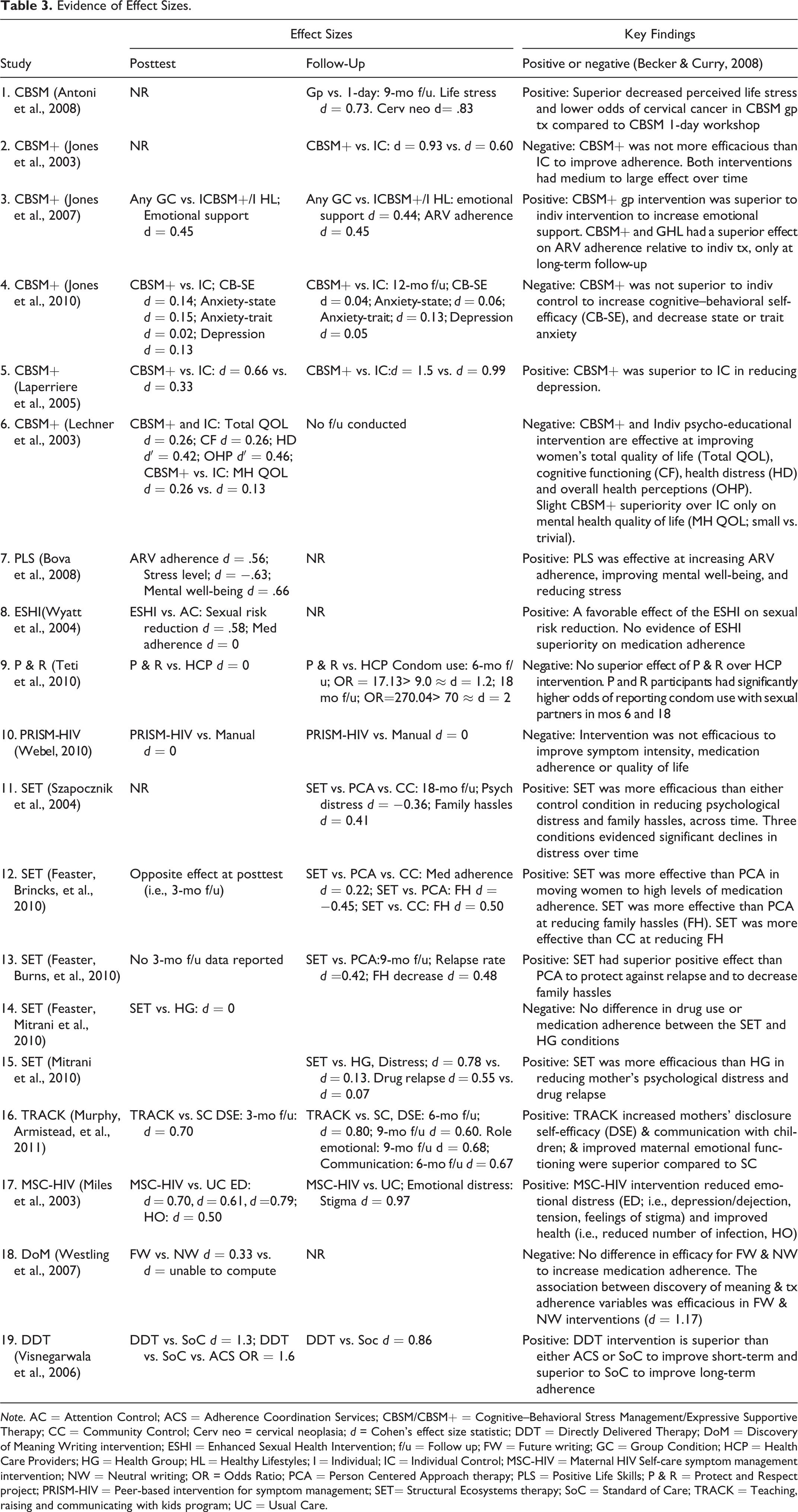
Note. AC = Attention Control; ACS = Adherence Coordination Services; CBSM/CBSM+ = Cognitive–Behavioral Stress Management/Expressive Supportive Therapy; CC = Community Control; Cerv neo = cervical neoplasia; d = Cohen's effect size statistic; DDT = Directly Delivered Therapy; DoM = Discovery of Meaning Writing intervention; ESHI = Enhanced Sexual Health Intervention; f/u = Follow up; FW = Future writing; GC = Group Condition; HCP = Health Care Providers; HG = Health Group; HL = Healthy Lifestyles; I = Individual; IC = Individual Control; MSC-HIV = Maternal HIV Self-care symptom management intervention; NW = Neutral writing; OR = Odds Ratio; PCA = Person Centered Approach therapy; PLS = Positive Life Skills; P & R = Protect and Respect project; PRISM-HIV = Peer-based intervention for symptom management; SET= Structural Ecosystems therapy; SoC = Standard of Care; TRACK = Teaching, raising and communicating with kids program; UC = Usual Care.
SET efficacy was evaluated in five studies; all five used methodological strong designs (Median QES = 9, QES ranged from 8 to 14), and four yielded positive results (Table 3). Feaster, Brincks et al. (2010), Feaster, Burns et al. (2010), Mitrani, McCabe, Robinson, Weiss-Laxer, and Feaster (2010), and Szapocznik et al. (2004) found favorable evidence for SET, whereas one study found no efficacy differences between SET and a health group condition (Feaster, Mitrani et al., 2010).
Of the four individual interventions evaluated in four separate studies, TRACK and MSC-HIV were tested in methodological strong designs and evidenced superior efficacy for their respective individual interventions compared to usual and standard care (Miles et al., 2003; Murphy, Armistead, et al., 2011; Table 3). The authors also report on the theory-based mechanisms for treatment change.
Analysis of effect sizes
Of the 19 studies in this review, 8 report posttest findings, 15 report follow-up findings, and 9 report findings at both data points (Table 3). Medium to large effect sizes were observed for several group intervention studies, including CBSM/CBSM+, at both posttest and 12 months or less follow-up points. In contrast to the only family intervention in this review, SET demonstrated small to medium effect sizes, only at long-term follow-up assessments (i.e., up to 18 months; Table 3). This comparison suggests that both intervention modalities have sleeper effects, justifying the use of extended follow-up points in the study designs. Alternatively, the larger effect size combined with the shorter follow-up assessments observed in CBSM/CBSM+ could be interpreted as a disadvantage over more modest effects for SET’s longer follow-up data points. Moreover, the contrast between treatment and comparison intervention effect size is more drastic for SET (medium vs. trivial) than CBSM/CBSM+ (medium vs. small).
MSC-HIV and TRACK evidenced superior medium to large effect sizes in posttest and 6- and 9-month follow-up assessments, respectively, compared to standard/usual care, on well-being outcomes for the population of HIV-infected mothers.
Level of empirical support
None of the 10 interventions reviewed met Chambless and collaborators’ (Chambless et al., 1998; Chambless & Hollon, 1998) criteria for well-established treatments because none were replicated in at least two independent research teams, as required in Criterion 3 (Table 4). CBSM+ and SET met criteria for possible efficacious treatments. CBSM+ outperformed a comparison condition on the following well-being outcomes for HIV-infected women: (a) increasing emotional support posttest and 6-month follow-up; (b) improving medication adherence only at 6-month follow-up; and (c) reducing depression at posttest and 12-month follow-up. SET outperformed a comparison condition in reducing psychological stress and family hassles, only at the 18-month follow-up, and protecting against relapse only at the 9-month follow-up.
Level of Empirical Support Using Evaluation Criteria Developed by Chambless et al. (1998) and Chambless and Hollon (1998).
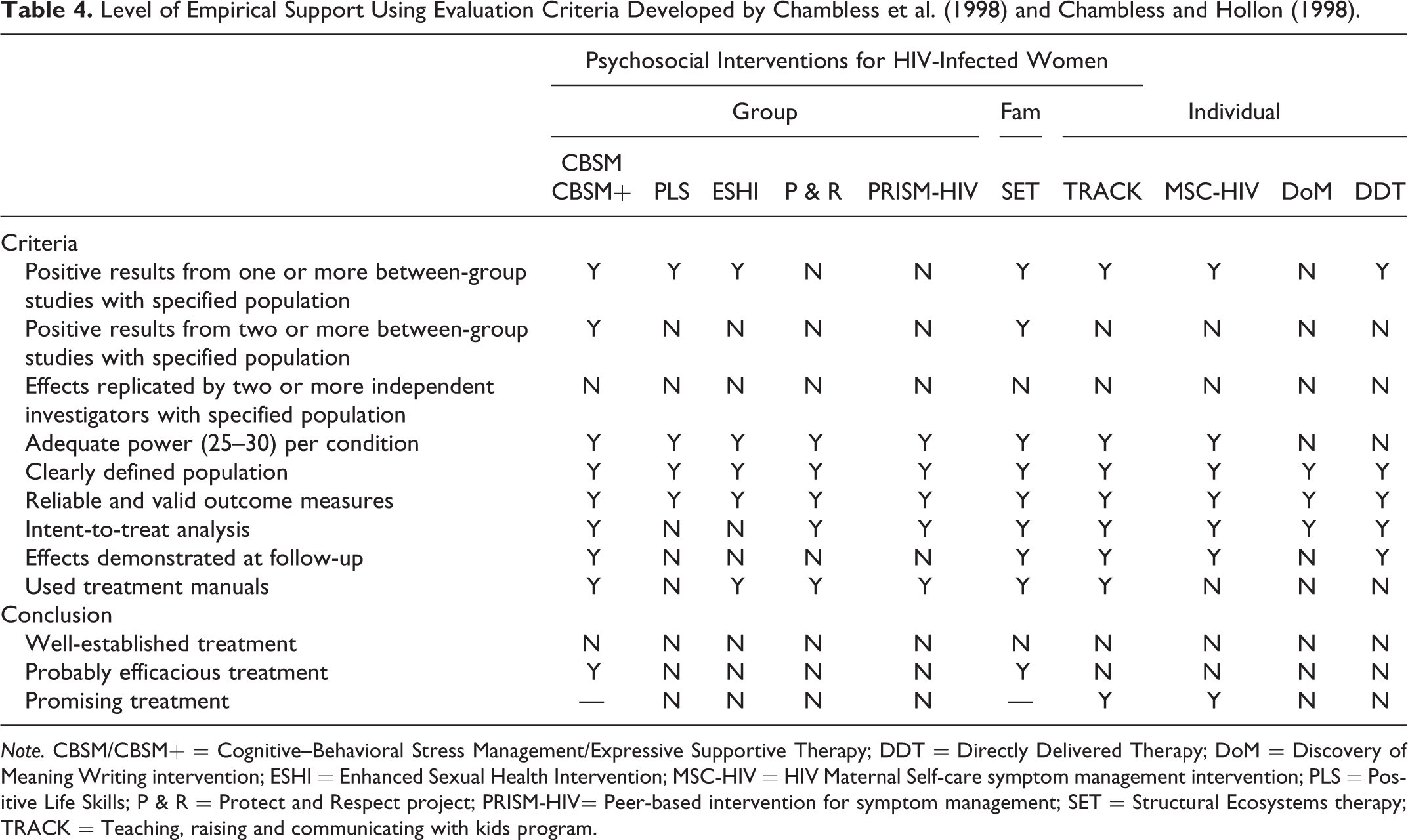
Note. CBSM/CBSM+ = Cognitive–Behavioral Stress Management/Expressive Supportive Therapy; DDT = Directly Delivered Therapy; DoM = Discovery of Meaning Writing intervention; ESHI = Enhanced Sexual Health Intervention; MSC-HIV = HIV Maternal Self-care symptom management intervention; PLS = Positive Life Skills; P & R = Protect and Respect project; PRISM-HIV= Peer-based intervention for symptom management; SET = Structural Ecosystems therapy; TRACK = Teaching, raising and communicating with kids program.
TRACK and MSC-HIV (Miles et al., 2003; Murphy, Armistead, et al., 2011) surpassed criteria for Engle and Macgowan’s (2009) “some indication of positive outcomes” rating, as they outperformed comparison conditions utilizing a pretest–posttest nonequivalent control group and a randomized control trial design, respectively. TRACK outperformed a comparison condition in promoting higher number of maternal HIV-status disclosure to children at 3-month follow-up, increasing disclosure self-efficacy at 6- and 9-month follow-up, improving maternal emotional functioning at 9-month follow-up, and increasing communication with children at 6-month follow-up. MSC-HIV also showed significant results and superior effect to reduce emotional distress and improve health among HIV-infected women, thereby providing some indication of positive outcomes. However, they failed to meet Chambless and collaborators’ (Chambless et al., 1998; Chambless & Hollon, 1998) criteria for “probably efficacious” because these interventions have not been replicated yet.
In summary, CBSM/CBSM+ and SET met Chambless and collaborators criteria for probably efficacious, and TRACK and MSC-HIV were classified as promising interventions, exceeding Engle and Macgowan’s rating of “some indication of positive outcomes.”
Discussion and Applications to Social Work
The results should be considered in view of several limitations. The criteria to select studies reporting on specific well-being outcomes for women with HIV/AIDS limit the generalization of the results to all subgroups of HIV-infected women. The inclusion of only some specific well-being outcomes, perhaps those researched more often, may have omitted studies reporting on alternative outcomes not considered in this review. The use of a broad definition of well-being outcome may preclude a more refined comparison of the interventions included in this review. In addition, the exclusion of studies published before 2000, during the initial and the pre-HAART era of the AIDS epidemic, introduces bias against interventions that address the psychosocial needs of HIV-infected women with late stages of HIV disease (i.e., AIDS). Similarly, the exclusion of studies conducted outside the United States precludes generalization of results beyond the United States.
This review employed multiple strategies to assess the methodological quality and the efficacy of treatment of psychosocial care interventions for women living with HIV/AIDS. When considered all together, the multiple criteria employed in this review clearly identified the top four interventions (SET, CBSM/CBSM+, TRACK, and MSC-HIV) and other mixed findings. The majority of the reviewed studies shared methodological strengths and/or reported positive results favorable to the intervention of interest. However, the wide efficacy rating assessed in the studies showing positive results for some of the different well-being outcomes among diverse groups of HIV-infected women may lack in clinical relevance (Lechner et al. 2003). Moreover, interventions tested in methodologically weak studies demonstrated medium effect sizes on certain well-being outcomes (PLS; Bova et al., 2008). This finding illustrates Becker and Curry’s (2008) conclusion that “higher levels of methodological quality were not necessarily associated with stronger evidence in support of an intervention” (p. 539). Remarkably, two interventions lacking efficacy superiority at posttest related to specific well-being outcomes (P & R, Teti et al., 2010; CBSM+, Jones et al., 2003) reported medium to large long-term effect sizes on these outcomes among HIV-infected women in both treatment and comparison conditions.
Compared to psychosocial intervention studies for women with HIV/AIDS done in the mid- to late 1990s, the focus of intervention research emerging in the following decade shifted from helping women with AIDS prepare and cope with death, to helping women with HIV/AIDS adapt and cope effectively with this chronic illness (Watkins-Hayes et al., 2012). This shift reflects the extended life expectancy and improved health status that highly antiretroviral medication affords HIV-infected women nowadays. Encouragingly, intervention studies for this population seem to keep up with recent trends in the evolution of HIV disease epidemiology and biomedical technology. This trend integrates established individual and family interventions with typical HIV care and further adapts intervention models to the specific circumstances or problems of subgroups of women living with HIV/AIDS (e.g., cultural affiliation, mother–child dyads, drug users; Feaster, Mitrani, et al., 2010; Mitrani et al., 2010; Wyatt et al., 2004).
SET and CBSM/CBSM+, the two interventions assessed as probably efficacious in this review (Chambless et al., 1998; Chambless & Hollon, 1998), utilize the strongest experimental designs to test theory-grounded hypotheses and efficacy against active and/or passive comparison conditions. Notably, SET studies score higher in methodological quality and treatment superiority compared to CBSM/CBSM+ studies. The implementation of both interventions is costly and lengthy because they employ highly trained professionals, carefully developed treatment manuals and they assess for effects at multiple follow-up points. They both tend to outperform active comparison group conditions in the long-term follow-up; however, the comparison treatment conditions were also efficacious across time (Jones et al., 2003; Lechner et al., 2003; Szapocznik et al., 2004). Not surprisingly, the rigorous testing of two or more treatment conditions over extended follow-up points creates attrition challenges for these interventions.
The studies using SET and CBSM/CBSM+ interventions identified change mechanisms and treatment factors that may explain either the effects reported by these interventions or some undesirable treatment effects for specific subgroups of participants. For example, Feaster, Mitrani et al. (2010) found that improved CD4 T cell and drug use relapse protection were mechanisms of change behind indicators of well-being outcomes for this population. Jones et al. (2003) observed that high-adherent women in CBSM+ and individual comparison conditions decreased their level of medication adherence. The effective treatment components of these interventions should be further evaluated in translational or implementation research designs and disseminated among community agencies working with this population (Miles et al., 2003; Mitrani et al., 2010).
TRACK and MSC-HIV, the two promising interventions in this review, address well-being outcomes for the emerging population of HIV-affected mother and child dyads. Compared to the group (CBSM+) and family (SET) interventions, individual interventions are less lengthy and their implementation in real-world settings could be less costly and time intensive, in terms of interventionist training and treatment adherence protocols. On the other hand, TRACK (46%) and MSC-HIV (49%) treatment studies also reported problematic high attrition rates in the follow-up measures of the research design.
Social work practitioners should only select interventions with the highest efficacy to address the comprehensive priority needs of diverse subgroups of HIV-infected women. They may select the most appropriate intervention from those best reviewed and assess its applicability to specific subgroups of this population. The challenges to accomplish this task abound, from engaging and maintaining the neediest HIV-infected drug using women in care, to providing innovative long-term interventions for newly diagnosed mothers and their uninfected infants. Social workers are well trained to tackle some of these challenges by delivering selected interventions in the client’s home or community environments.
Group-based CBSM/CBSM+ and family-based SET interventions were probably efficacious for reducing psychological distress (e.g., life stress, depression, family hassles, or parenting stress), improving self-efficacy in coping skills, medication adherence, and protecting against substance abuse relapse. Social workers could match effective treatment components from CBSM+ or SET and the most prominently barriers to well-being observed in the cohort of women for whom they are planning the group or family intervention. For example, practitioners could employ specific CBSM+ modules designed to reduce depression and assess the efficacy of the intervention in accomplishing this goal. This practice may potentiate the effectiveness of CBSM+ for this cohort and reduce the dropout rate of group participants. If properly designed, such application could simultaneously contribute evidence to the efficacy of CBSM+ and evaluate its effectiveness in a real-world setting.
The two individual interventions TRACK and MSC-HIV hold promise in reducing emotional distress (e.g., depression, tension feelings of stigma) among mothers with HIV/AIDS, improving health, and helping mothers disclose their HIV status to their children. Practitioners could incorporate the findings of this critical review in working with HIV-infected mothers and effectively address these mothers’ multiple and unique psychosocial needs. For example, practitioners could use all or some components of the MSC-HIV intervention to improve the physical health reported by mothers diagnosed with HIV during pregnancy. Given the potential trauma of HIV diagnosis, the lack of knowledge on HIV disease, and the inexperience in coping with this disease of these mothers, they may experience high emotional distress and practice poor self-care. These psychosocial needs may match the aims of the MSC-HIV program.
High research attrition rates reported in the top four interventions identified in this review challenge future evaluations of these treatments. Rather than strict replication, future research could utilize an enhanced translational or implementation research design to maximize retention and properly evaluate the long-term efficacy of CBSM/CBSM+, SET, TRACK, and MSC-HIV. Such design would evaluate treatment effectiveness in real-world community settings, uncover creative strategies to retain HIV-infected women in research studies, and perhaps synthesize knowledge between researchers and practitioners (Antoni et al. 2008, Bhattacharyya, Reeves, & Zwarenstein, 2009)
Future translational or implementation research designs should also elucidate which combination of treatment model and modality is most useful for which subgroup of HIV-infected women (e.g., newly diagnosed, with AIDS, substance abusers, mothers). Social work researchers are well positioned to take on the challenges of translational or implementation research to further assess which interventions should be used in which practice context for which problem faced by women living with HIV/AIDS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The first author received financial and professional development support as a McKnight Doctoral Fellow from the Florida Education Fund.