
Abstract
Objectives:
This research article aims to measure the effects of group therapy on institutionalized elderly in terms of reducing depression and improving psychosocial functioning.
Methods:
Thirty elderly nursing home residents were recruited, and 16 of them elected to receive group treatment for depression and 14 declined treatment. The Multidimensional Observation Scale for Elderly Subjects and the Geriatric Depression Scale were given to both groups when group work began and again when it ended.
Results:
Clients who received group treatment experienced reductions in depression and their psychosocial functioning improved.
Conclusion:
Group work intervention was followed by reductions in the depression levels and improvements in their psychosocial functions among institutionalized elderly clients.
As it is the case in many countries all over the world, the demographic structure of Turkey has been rapidly changing. As fertility rates are falling and longevity is increasing, the share of the elderly (65+) within the population is constantly increasing. Moreover, along with technological developments, economic and social development is producing a longer life span (Karataş, 1988). As of 2014, the elderly in Turkey constituted 7.7% of the population which almost equals 6 million people and this percentage is projected to reach 20.8% by 2050 (TUIK, 2014). Since old age is a phase where physiological and mental changes are at their peak (Pekcan, 2000), this can bring about some challenges regarding the adaptation process of elderly to growing old (Emiroğlu, 1995). With old age, people may experience status loss, financial difficulties, loneliness and isolation, difficulties in adaptation to social life, increases in chronic diseases, and decline in physical abilities. On the other hand, decreasing number of children and fertility rates, mobility, urbanization, and increasing female labor force participation are decreasing kin resources in terms of caring for the elderly. As a result, the need and demand for formal and institutionalized care facilities are increasing in Turkey as well as around the world. The objective of nursing homes is to provide elderly people with a healthy environment and to help meet their social and psychological needs. Nursing homes in Turkey admit socioeconomically disadvantaged people over 60 years who are able to continue their daily living activities, those who do not need medical long-term care, and who are not severely disabled or mentally ill (MFSP, 2014). Even though these older patients do not have severe health problems and limited communication with their family, isolation and difficulty in adaptation to the new environment can be mentally and emotionally challenging (Özer, 2004). For this reason, depression and impairments in psychosocial functioning are common among the institutionalized elderly.
Geriatric Depression
Depression is a pervasive psychiatric disorder that emerges due to various reasons, and geriatric depression is one type that occurs among elderly (65+). According to the Fact Sheet published by World Health Organization (2013), depression effects 7% of the elderly and this percentage may vary according to the context and country. In Turkey, the prevalence of geriatric depression is much higher. According to a study conducted in Istanbul, 17% of the elderly were diagnosed as depressed, and depression rates are even higher among the illiterate and aged 75–79 (Kulaksizoglu et al., 2005). Another prevalence study conducted in Trabzon, Turkey, also showed that 13.6% of the elderly had depression symptoms (Kavakcı, Bilici, Çam, & Ülgen, 2011). According to a study that investigated risk factors for depression, depression rates were higher among women, divorcees, people living alone, and among those having no social security (Nahcıvan & Demirezen, 2005). Given the rise in the share of elderly in the population all around the world and in Turkey, the percentage of depressed older adults is expected to increase.
Diagnosis and treatment of geriatric depression is crucial because along with other physical and cognitive declines, untreated depression can severely decrease the quality of life. Research shows that depression immensely decreases the quality of life among older people (Akyol, Durmus, Dogan, & Canturk, 2010; Hasche, Morrow-Howell, & Proctor, 2010; Reynolds, Haley, & Kozlenko, 2008). In order to increase the quality of life among elderly persons, treatment of depression is essential. However, since depression symptoms can vary according to age-groups, different diagnostic and treatment procedures may be relevant and useful with older persons. For instance, sleeping disorders and decreasing sexual activity can be a sign of depression for young adults, whereas these symptoms may not indicate depression for the elderly. Moreover, some symptoms of depression overlap with dementia and may lead to misdiagnosis of the patient. For this reason, accurate diagnosis of depression is crucial for appropriate treatment.
Geriatric depression has many treatments such as psychopharmacological therapies, electroconvulsive therapy, individual and group psychotherapy, and psychosocial interventions. Even though medical intervention may be effective, selected psychotherapies are also effective in treating geriatric depression. Moreover, group therapies can further create a synergy among group members and be more effective compared to individual therapies. These group therapies entail different kinds of interventions such as cognitive and remotivation therapies, reminiscence and grief therapy, physical exercise activities and preventive health behavior, managing medical conditions and social skill development, relaxation and imagery, pleasurable events, and positive social praise.
Psychosocial Functioning
Psychosocial functioning is a multidimensional concept that encompasses different aspects of functioning such as intellectual, social and cognitive functioning, psychosocial aptitude, and measurement of physical needs (Hill, Thorn, Bowling, & Morrison, 2012). There are five areas of psychosocial functioning that are identified: Self-help: This area of functioning assesses the ability of the elderly to look after his or her own physical care needs, and if more physical nursing care is required. Disorientation: This type of functioning assesses disorientation and confusion experienced by the elderly in relation to people, recent events, and past memories. Depression: This area of functioning explores an exhibition of signs for personal distress and unhappiness. Irritability: This area of functioning assesses cooperative and abusive behaviors of elderly toward staff and other residents of the institution. Withdrawal: This area of functioning looks at the level of interest the resident takes in people, events, and activities.
Group Therapy Models
Along with the quality of life, psychosocial well-being of the institutionalized elderly is crucial and interventions to enhance their psychosocial well-being therapeutic interventions are essential. Life review therapy, reminiscence therapy, or memoir sharing are some intervention models that are used to empower and improve the psychosocial well-being of the elderly (Peck, 2001; Tufan, 2007). As Turan (1985) indicates, elderly people may enjoy reliving the past. Despite the occasional interruption of regretful feelings, reminiscing the past often brings gratification and mental satisfaction to the elderly while making it easier to live with the current facts. Social cognition and cognitive appraisal are useful concepts to understand the life review process and subjective well-being. In later phases of the life course, the schemata that an individual uses for appraisal are challenged and changed by various losses that come with age. These schemata can be activated through the creation of narratives and reminiscing about the past, which brings personal reconciliation and enables working through changes. All these processes can improve the subjective well-being of seniors (Peck, 2001). Reminiscence therapy can also help with improving emotional well-being and their socialization skills and processes (Siviş & Demir, 2007). A group study conducted with elderly persons has shown that group work improved their spontaneity, creativity, and empathy, giving way for better interpersonal communication, problem-solving, and self-expression (Oğuzhanoğlu & Özdel, 2005). In this respect, it can be argued that reminiscence therapy can decrease depression levels and enhance psychosocial functioning through enabling elderly to continue their social interaction, making them hold onto life, delaying memory loss and other age-related mental deficiencies, promoting intergenerational solidarity, and revealing interesting cultural and historical information (Turan, 1985).
Method
Research Objective
The objective of this research is to find out how group work intervention affects the depression levels and psychosocial functioning of elderly nursing home residents. It was hypothesized that psychosocial functioning and depression scores of the elderly in the treatment group will positively increase following group work and that similar improvements will not be observed among members of an untreated control group.
Research Design, Sample, and Site
We used a quasi-experimental pretest–posttest no-treatment control group study. Purposive sampling was used to recruit participants (Chao et al., 2006; Nachar, 2008). This study conducted at the Süleyman Demirel Nursing and Rehabilitation Centre, a state 240-bed elderly home in Ankara, Turkey, supported by the General Directorate of Disabled and Aged Services of Ministry of Family and Social Policies. The elderly home has two wards. One is for elderly people who are healthy and second one is for elderly people who need special care and rehabilitation. Fifty-nine beds are for healthy patients and 191 beds for patients who need special medical care. Elderly people who lived in the special care and rehabilitations ward were excluded from this project. When we conducted the study, 5 of the 59 beds were empty, 11 elderly people were away with their families or at holiday, and 5 of them were hospitalized. Because of that only 43 elderly people were potentially enrollable in this study. Ultimately, 30 elderly people participated after being informed about the content, objectives, and the project. In addition, staff members and other personnel were informed about the study.
In the scope of the project, two groups were formed. The first group consisted of 15 elderly nursing home residents who received group therapy and the second group of 15 did not receive group therapy. The study is diagrammed in Figure 1. The independent variable (treatment) of the study is the group work that has been applied to the elderly.
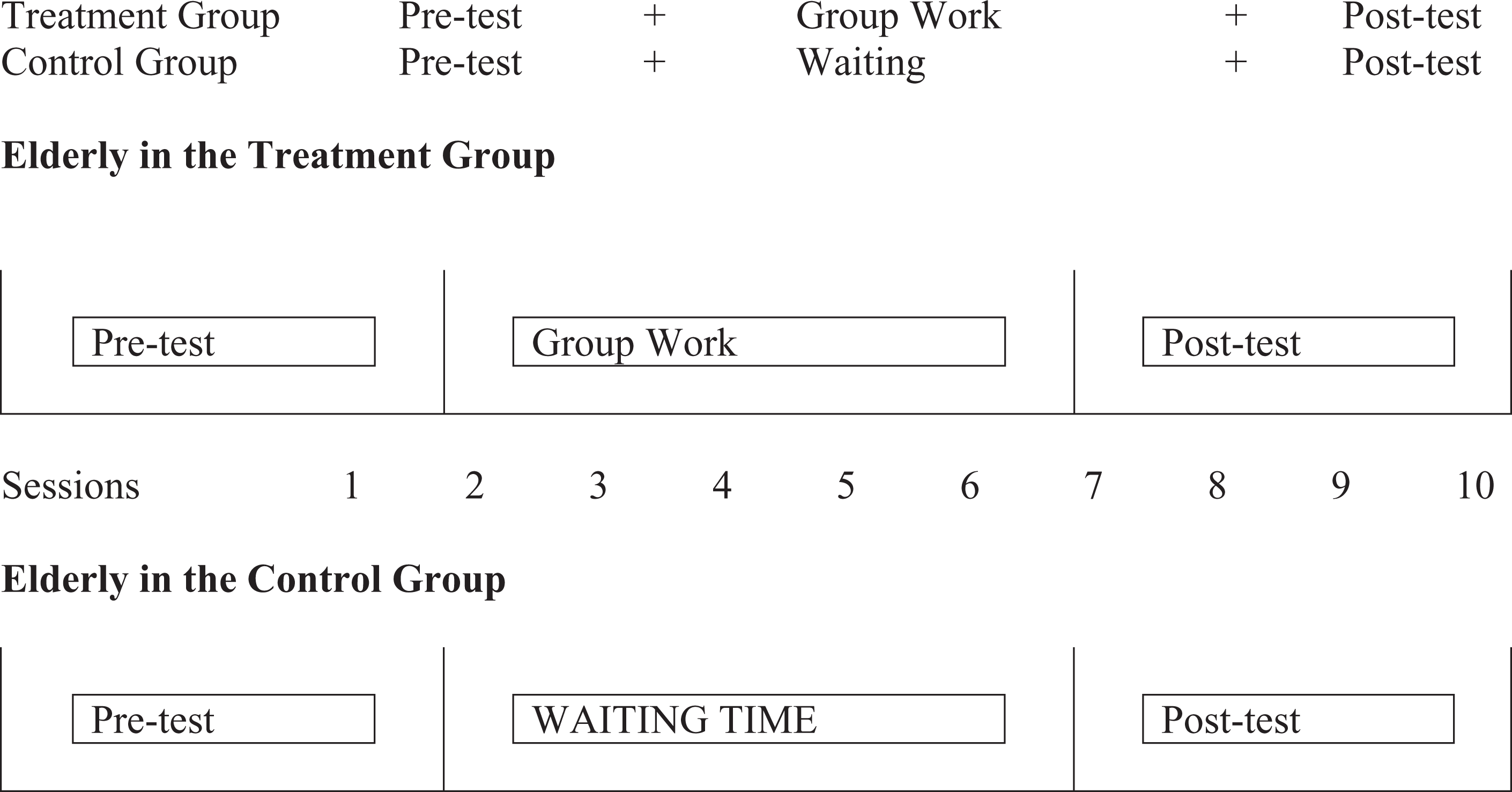
Group work process.
Outcome Measures
Three instruments were used to evaluate the effects of reminiscence group work on elderly people nursing home residents: (1) a demographic questionnaire, (2) a psychosocial functioning scale, and (3) a depression inventory.
A Turkish version of the Multidimensional Observation Scale for Elderly Subjects (MOSES) was used to measure the participants’ psychosocial functioning level. The MOSES was developed by Helmes, Csapo, and Short (1985) to measure the psychosocial functioning of institutionalized elderly and the scale’s reliability and validity study in a Turkish context has been examined (Soygür, 2000; Soygür, Aydemir, Güzelarslan, & Akturk, 1998). The MOSES is composed of 40 items that can be completed by the caregiver in 10–15 min. However, observation of the patient by the caregiver is required for a certain period of time, generally 1 week. The scale provides five separate scores (8 items for each), and each of these scores deals with a different area of functioning. The higher the score for the rating area, the more problematic is the type of functioning. These five areas of functioning are as follows: (a) Self-Help (Items 1–8): The less able the resident is to look after his or her own physical care needs, and therefore the more physical nursing care required by the resident, (b) Disoriented Behavior or Disorientation (Items 9–16): The more disoriented and confused the resident’s behavior is in relation to people, recent events, and past memories, the higher the score is, (c) Depressed/Anxious Mood or Depression (Items 17–24): The more the resident exhibits signs of personal distress and unhappiness, the higher the score is, (d) Irritable Behavior or Irritability (Items 25–32): The less cooperative and more abusive the resident is with the staff and other residents, the higher the score is, and (e) Withdrawn Behavior or Withdrawal (Items 33–40): The less interest the resident takes in people, events, and activities, the higher the score is.
A Turkish version of the Geriatric Depression Scale—Short Form (GDS-S) was used to measure the participants’ depression level (Ertan & Eker, 2000). As indicated before, depression is characterized by a sense of hopelessness, lack of interest in life, sadness, self-criticism, self-blame, slow thinking, poor concentration, and appetite and sleep disturbances (Chao et al., 2006). The GDS-S consists of 15 items chosen from the GDS-Long Form. These 15 items were chosen for the shorter version because these items showed high correlation with depressive symptoms in former validation studies (Sheikh & Yesavage, 1986). Clients can usually complete the GDS-S in 5–7 min. There have been many studies that were conducted to test the validity and reliability of the GDS (D’Ath, Katona, Mullan, Evans, & Katona, 1994; Fuentes & Aranda, 2012; Husaini et al., 2004; Marwijk et al., 1995; Parmelee, Lawton, & Katz, 1989). The validity of the scale has also been translated into many languages including Turkish and the validity of the scale has been demonstrated in the country-specific context (Kohli, Banerjee, & Verma, 1991; Lieh et al., 1995; Niino, Imaizumi, & Kawakami, 1991).
Identifying Group Members
After the application of the GDS-S and Multidimensional Evaluation Scale by the institution’s nurse, the results were evaluated and the elderly were selected accordingly. The participants in the treatment group were elders who were able to share their stories with others. Criteria for potential participants for inclusion in the treatment group were being over 60 years of age, without serious psychiatric illnesses, possessing normal communication ability, being without physical discomfort or pain caused by disease or severely damaged sensory function (e.g., loss of vision or hearing), and being volunteering to participate in group therapy. Before the sessions, meetings were held with the selected elderly and they were informed about the objectives, content, time, duration, place, participants, and the anonymity of the group sessions. After these meetings, the treatment and control groups were formed. While forming these groups, MOSES and GDS-S pretest scores were taken as a measure of pretreatment functioning, along with information regarding the client’s personal demographics. These data are presented in Table 1.
SocioDemographic Features of Elderly (Education Level and Age).
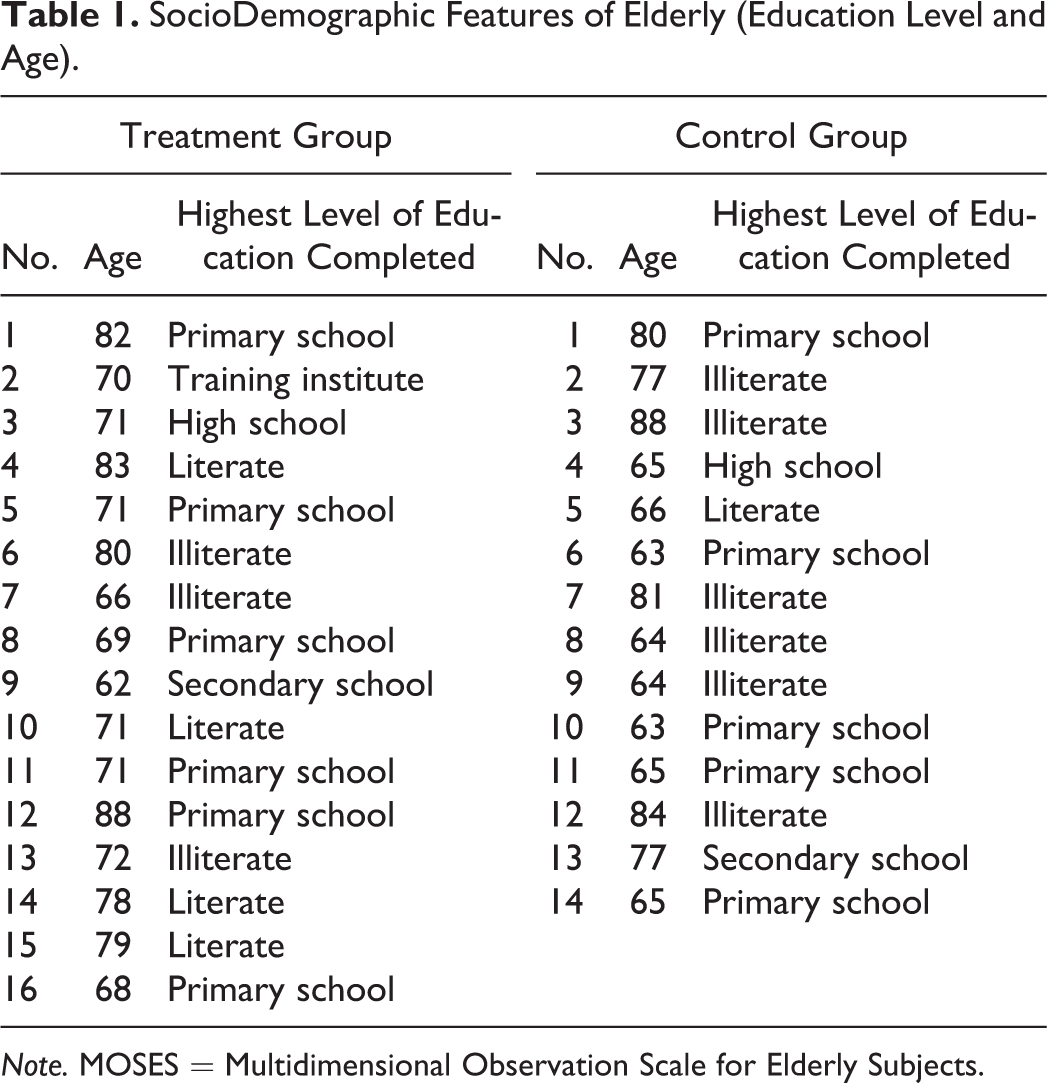
Note. MOSES = Multidimensional Observation Scale for Elderly Subjects.
Group Work Procedure
Group work was conducted by the second author (G.Ş.-K.) of this study who is a specialist in clinical social work. Approximately 1 week before we started to the study, all participants in the treatment and control groups individually took the pretest measure. Immediately following the 10-week group work sessions, all participants individually took the posttest measures. The “reminiscing” group work was carried out in the library and training room of nursing home between the dates January 14, 2008, and March 17, 2008. Initially, the room was arranged in a circular way with armrest chairs but since the participants were not very comfortable with these chairs, they were replaced by sofas. Some participants used wheelchairs. The group work lasted approximately for 3 months and the sessions took place every Monday between 14.00 and 15.30. All treatment group members were reminded of group work activity during morning visit. Before each session, the participants were provided with some snacks and beverages which gave them some free time to socialize, warm up, and relax before the sessions.
An essential element of the group work is memory sharing and reminiscences of the memories as a tool for therapeutic intervention. We conducted 10 sessions. As indicated by Chao et al. (2006), each group activity centered on a topic carefully designed to avoid threatening or irritating participants.
At the beginning of each session, the participants were encouraged to read poems or sing songs to create a relaxed environment. These ice-breaking practices were accompanied by snacks, tea, and coffee. And in order to encourage interaction between the participants and initiate the conversations, the participants were asked to draw a name of a participant from a bucket and either poses a question on the week’s topic or introduces that person and comment on that person. Here is how each session was arranged: Week 1—In the first session, the participants were asked to introduce themselves and indicate their expectations from the group work sessions. Once more, the group leader informed the participants about the content, purpose, and duration of the study. The participants slowly started to talk about their childhood memories in this session. Week 2—In the second session, two new participants were introduced and every participant continued to share their childhood memories. The participants were asked to bring their old photo albums for the next session. Week 3—At the beginning of this session, the participants played a memory game by trying to identify the missing objects in a tray in order to emphasize the relationship between memory, memoirs, and souvenirs. After that, old photo albums brought by the participants were distributed across the group and the members shared their memories through these photographs. Week 4—In this session, the participants were encouraged to share their positive memoirs related to their work lives in the past. In order to remind each other’s name and personal history, the participants were asked to introduce each other before the session started. Week 5—In this session, the participants were asked to share their “first” moments, such as starting primary school, having a child, getting married, receiving a letter, and so on. The group leader focused on shy participants to encourage them for more participation and support. Week 6—In this session, the participants were asked to describe their happiest moments in the past and where would they want to live again. The participants were directed to talk about their happy moments, as they had a tendency to talk about unsolved problems. Week 7—In this session, the participants were encouraged to help each other and appreciate the happiness that helping each other brings. In this session, the participants were blindfolded and given objects to identify. In the identification process, the other participants gave clues and helped the blindfolded participant. Week 8—In the eighth session, the participants stated their favorite places and cities, their favorite activities, and their favorite people to spend time with. Week 9—In this section, the group leader tried to push the participants to scrutinize the meaning of happiness through sharing happy moments in their lives and create a common identity. They were asked to describe the happiest moments in their lives. The participants were also informed about the final session that was coming up. Week 10—During the last session, the group leader asked for feedback from the participants about the group therapy.
Ethical Considerations
This research was conducted after obtaining the voluntary consent of the research participants. They had a full understanding of the objective, process, and potential dangers and benefits of this research. Also, we informed the participant that they will receive no payment for taking part in this study. All information gathered from the participants were considered confidential.
Results
Pre- and posttest data for the clients in the treatment and no-treatment conditions were analyzed using a 2 (time periods) × 2 (groups, treatment vs. no-treatment) analysis of variance (ANOVA). As seen in Table 2, the average GDS-S scores of the 16 elderly people who accepted to participate in the group work was 12.44 (SD = 3.72) where the average score for the 14 elderly people who did not participate was 10.57 (SD = 4.60). These two means did not significantly differ. Posttest the average GDS-S score of the 16 older people who participated in the group application is 10.81 (SD = 2.86) where the average of the 14 who did not is 11.07 (SD = 3.05). ANOVA results depicted in Table 3 show that the only statistically significant posttreatment difference occurred in the “Withdrawn” subscale of the MOSES, which declined in the treatment group and became elevated in the nontreatment group. Multiple comparison analyses on MOSES scores are displayed in Table 4 and favor the patients who received group therapy on the variables of Disoriented, Irritable, and Withdrawn.
MOSES and GDS-S Scores Before and After Group Work.
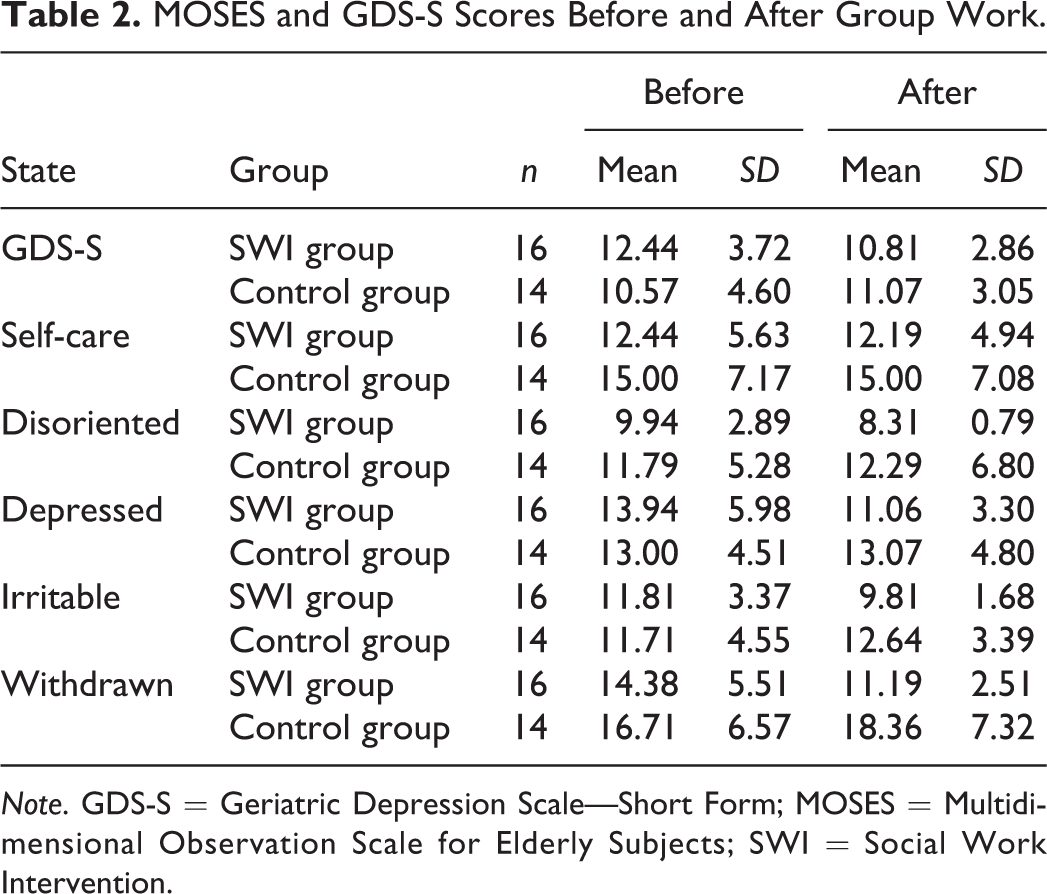
Note. GDS-S = Geriatric Depression Scale—Short Form; MOSES = Multidimensional Observation Scale for Elderly Subjects; SWI = Social Work Intervention.
ANOVA for Comparing MOSES and GDS-S Scores.
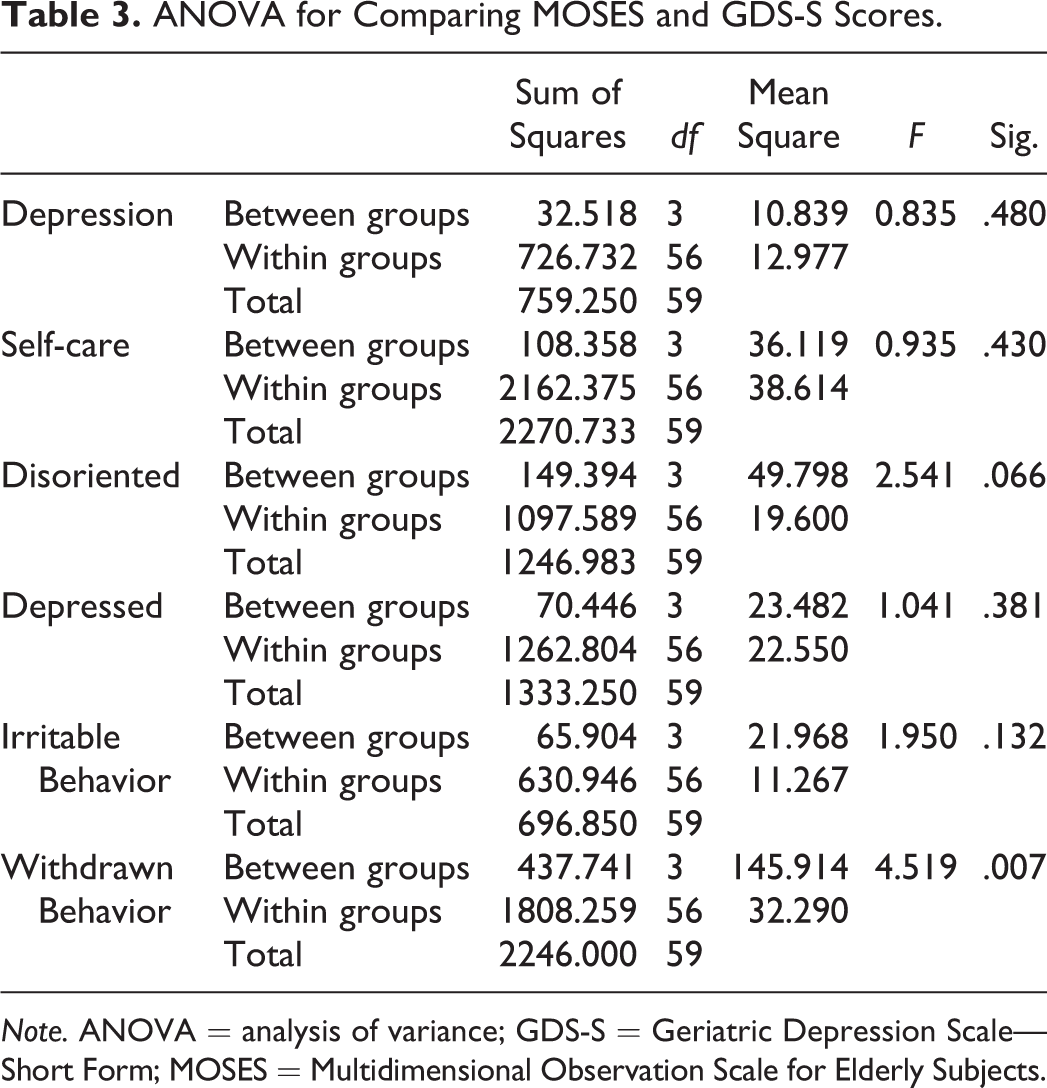
Note. ANOVA = analysis of variance; GDS-S = Geriatric Depression Scale—Short Form; MOSES = Multidimensional Observation Scale for Elderly Subjects.
Multiple Comparisons in MOSES and GDS-S Scores.
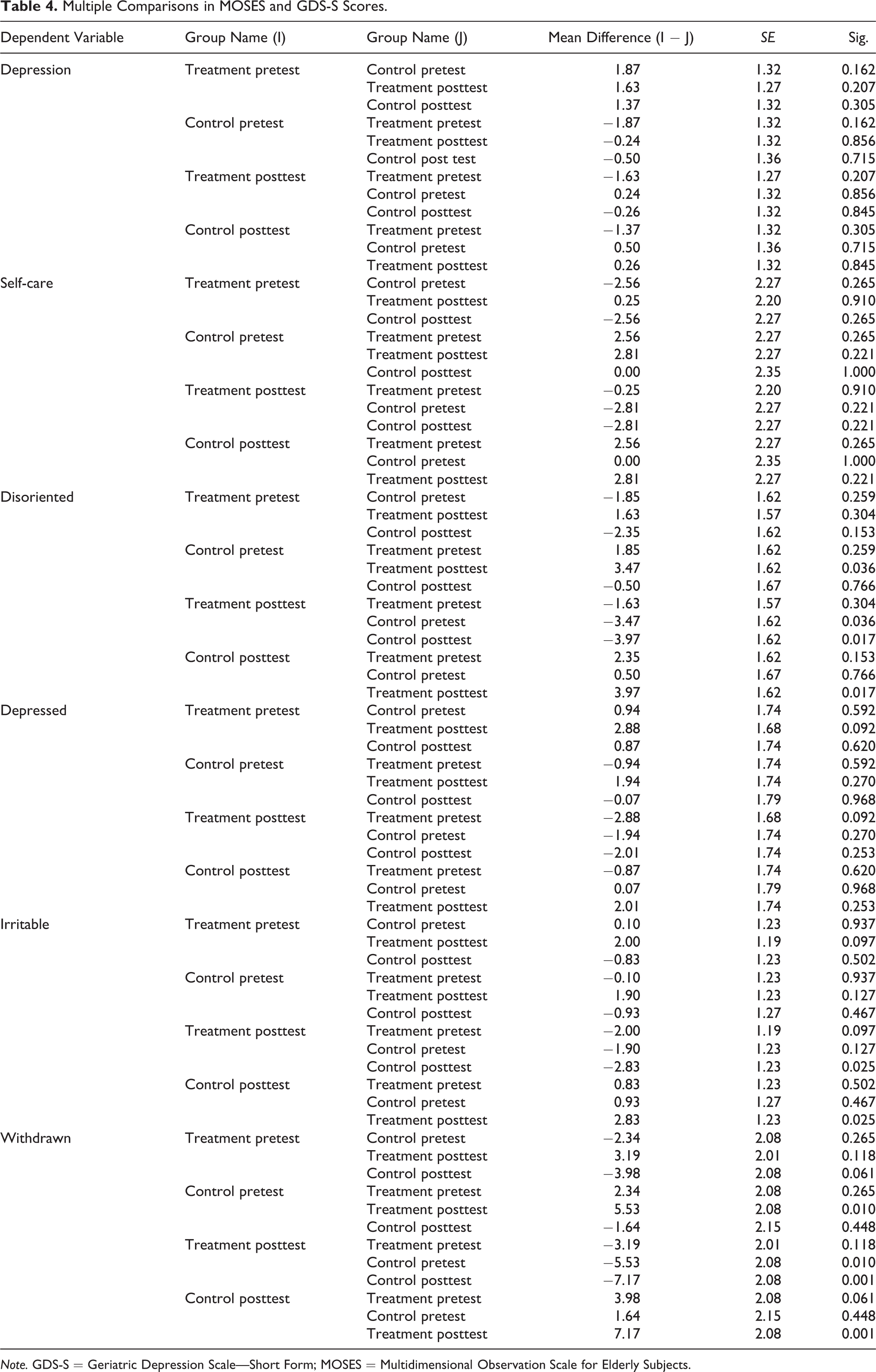
Note. GDS-S = Geriatric Depression Scale—Short Form; MOSES = Multidimensional Observation Scale for Elderly Subjects.
The Difference After Group Work
Table 3 shows the differences between treatment group and control group. The ANOVA analysis shows that the differences between the withdrawn behaviors were statistically significant at p < .05 level. However, differences between the other behavior types (self-care, depression, disorientation, self-help, and irritable behavior) were not statistically significant.
In addition to the ANOVA analysis, Fisher’s least significant difference (LSD) test (Meier, 2006) was employed. Table 4 shows an LSD analysis and compares each post- and pretests of the control and treatment groups according to each behavior category. According to the analysis, the difference between control pretest and treatment posttest is significant for disoriented behavior at p < .05 level. The positive relationship shows that control group mean scores were higher than the treatment group. On the other hand, the difference between control posttest and treatment posttest for the disoriented behavior was statistically significant at p < .05 level. The positive sign of the mean confirms that the scores of control group posttests were higher compared to the treatment posttest. In short, this result shows that the group work therapy was useful in reducing disoriented behavior among participant elderly.
Discussion and Application to Social Work
In this work, we intended to evaluate the possible effects of group therapy on a sample of elderly nursing home residents. In addition to the statistical analysis, behavioral changes like improvement in self-expression and increase in the joy of living are observed in the treatment group. The participants of the treatment group were observed to support each other with emotional sharing and giving and exchanging advice on getting through tough situations. Also, giving meaning to life became more consolidated with the help of sharing memoirs and reminiscence therapy. Empathy with other participants who had been experiencing similar situations formed a connection between each other and made them reconsider and realize what happened in their own lives. This also enhanced the communicative, expressive, and assistive skills of the participants of the group work. Moreover, group work was seemingly effective for developing relationships, sustaining friendships, gaining a more constructive self-perception, and gratifying senses. All of these outcomes support the therapeutic factors that Yalom describes (1995). According to Yalom (1995), there are 11 therapeutic factors that are “the actual mechanisms effecting change in the patients” (p. 1). For instance, the group work conducted in the scope of the project promoted cohesion and gave the participants a sense of belonging to a group. Moreover, not feeling alone in the experiencing of the problems (universality), helping and supporting others (altruism), encouragement for recovery (instillation of hope), providing support and assistance (guidance), interpersonal learning, and developing social skills were among the therapeutic benefits of the group work that was conducted with the elderly.
As far as the benefits of the group therapy from a preventive social work point of view are concerned, it can be argued that the group work has provided the participants with secondary prevention and tertiary prevention. The objective of the secondary prevention is to aim for early diagnosis and treatment (Mant, 2004; McWhinney & Freeman, 2009). In our study, we used GDS-S for early diagnosis and intervened with group work, which helped to treat the older participants and reduce their depression levels. Similarly, the group work helped by serving as a tertiary preventive intervention, which aims to prevent the further development or deterioration of the disease (Sheafor & Horesji, 2003). The elderly participants, who already had high levels of depression according to the GDS-S scores, stopped developing further depression. On the other hand, the control group, who did not receive any treatment, turned out to have higher GDS-S scores, which is a sign of increasing depression.
Regarding the benefits of group work that are described above, the therapeutic power of the group should be transferred to other areas of social work. For instance, previous research in Turkey shows that working with earthquake victims, the disabled, and the detained children showed that their depression levels and psychosocial well-being have improved (Baykara-Acar & Acar, 2001; Duyan, 1997; Duyan & Gökçearslan, 2004; Duyan & Sahin-Kara, 2010). Since the usage of group therapy has been very limited in the Turkish context, the usage of the group work therapy should be expanded to other fields of social work.
To conclude, we found that group work was followed by improved depression and social functioning among treated nursing home clients, compared to clients who did not receive group work. We believe that continuing with group work is crucial, as is with individual therapies. MOSES and GDS-S scales are also useful for measuring the change after the group work is conducted. In this study, we only used reminiscence therapy; however, other types of group work should also be expanded and used in the treatment of depression and decreased psychosocial functionality. As the number of nursing homes and care homes is very much likely to increase in the future due to demographic and structural changes, mental health of the institutionalized elderly will be at stake. For this reason, the need for individual and group therapies will also increase. Considering the cost of individual therapy, group work therapies will be more cost- and resource efficient. In this respect, studies on group therapies should also be expanded.
Footnotes
Acknowledgement
The authors would like to acknowledge with appreciation the helpful and co-operated way of conducting data analysis of ANOVA of the current manuscript by Dr. Hasan Atak, Faculty of Education, Kırıkkale University, Kırıkkale, Turkey.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.