
Abstract
Background
Hippotherapy uses horse movement to promote physical and psychosocial rehabilitation and may benefit children with cerebral palsy (CP). Standardised instruments such as the Activity Scale for Kids-Performance (ASK©), the Gross Motor Function Classification System (GMFCS) and the Gross Motor Function Measure (GMFM) are needed to quantify effects on motor function.
Objectives
To systematically review the effects of hippotherapy on gross motor skills in children with CP. Although autism spectrum disorder (ASD) was included in the search strategy, no eligible ASD studies were identified.
Methods
Following PRISMA guidelines, six databases (PubMed, EMBASE, Web of Science, SCOPUS, Cochrane and SciELO) were searched for English, Portuguese or Spanish studies employing ASK©, GMFCS or GMFM. Two reviewers independently screened records, extracted data and assessed risk of bias.
Results
Twenty-five studies (602 participants, mean age 7.1 years, 3–14) met inclusion criteria; all involved CP, none ASD. Interventions lasted 8–24 weeks (1–3 sessions/week). Two ASK© studies showed significant motor gains (Hedges g = 0.48–0.62). GMFM was used in 22 studies; 20 reported clinically relevant improvements, particularly in dimensions D (standing) and E (walking, running, jumping). The sole GMFCS study reported no change in classification. Methodological quality was moderate, limited by small samples and lack of blinding.
Conclusion
Hippotherapy improves gross motor function in CP, best demonstrated with GMFM. Evidence for ASD is absent, highlighting a research gap. Broader application of ASK© and GMFCS is still needed to better define benefits across neurodevelopmental disorders.
Keywords
Introduction
Hippotherapy, a treatment strategy that places the participant astride a walking horse, capitalizes on the animal's gentle yet constantly shifting three-dimensional gait. Every stride transmits rhythmic pelvic displacements, vestibular cues and tactile feedback that mirror the sensory flow of typical human walking (Guindos-Sanchez et al., 2020; Plotas et al., 2024). The rider must respond in real time, recruiting deep-trunk and postural musculature, refining equilibrium reactions and continuously updating proprioceptive maps (Sterba et al., 2002), all while immersed in an intrinsically motivating environment that differs markedly from conventional gym-based therapy. Because the activity is engaging, task-oriented and socially rich, it sustains the practice intensity thought to drive neuroplastic change (Silkwood-Sherer & McGibbon, 2022; Whalen & Case-Smith, 2012). These attributes align closely with the unmet needs of children with cerebral palsy (CP) (Noritz et al., 2022), who often demonstrate a higher energy cost of walking (McGibbon et al., 1998). CP is the leading cause of long-term motor disability in childhood, affecting about 2–3 per 1 000 live births worldwide (McIntyre et al., 2022). The disorder results from a non-progressive insult to the developing brain and manifests as enduring limitations in muscle tone, coordination and selective motor control. Despite evidence-based conventional physiotherapy, many children plateau below their age-expected gross-motor milestones, prompting interest in adjuncts that enhance neuroplastic drive and motivation. Although its etiology spans prenatal vascular events and infections, perinatal hypoxia and postnatal encephalitis or trauma, functional abilities depend chiefly on lesion topography and the consequent network disruption within corticospinal, basal-ganglia and cerebellar circuits (Novak et al., 2025). Clinically, spastic CP predominates, followed by dyskinetic and ataxic forms; each phenotype imposes distinct challenges to gross-motor development, balance and energy efficiency. Standard physiotherapy, constraint-induced movement training and technology-assisted interventions have advanced outcomes (Jackman et al., 2022), yet functional plateaus and motivational fatigue remain common (Novak et al., 2020). Interventions that concurrently drive neuroplasticity, challenge postural control and sustain engagement are therefore highly sought, explaining the steady uptake of hippotherapy across pediatric neuro-rehabilitation clinics (Potvin-Belanger et al., 2022). Despite growing clinical use, practice guidelines remain equivocal because meta-analysed effect estimates vary widely - from small, near-trivial gains (GMFM total SMD of 0.19; 95% CI 0.02–0.36) in a 17-trial review (Qin et al., 2024) to improvements (GMFM-66 SMD of 0.81; 95% CI 0.47–1.15) (Peia et al., 2023), with earlier balance-focused work showing odds ratios as high as 25.4 (Zadnikar & Kastrin, 2011). These discrepancies reflect differences in study quality, outcome choice and dosing. Early narrative reviews pooled hippotherapy with broader “equine-assisted programs”, while later systematic reviews merged CP cohorts with other neurodevelopmental conditions such as autism spectrum disorder (ASD) (du Plessis et al., 2023; Tseng et al., 2013). This methodological heterogeneity dilutes signals specific to CP and hampers evidence-based service planning. Outcome selection adds another layer of uncertainty. Many primary studies report surrogate measures (e.g., pelvic tilt angles, surface electromyography timing) that are difficult to translate into day-to-day function (Sharma et al., 2023). In contrast, three instruments capture clinically meaningful change across paediatric motor disability: the Gross Motor Function Measure (GMFM), the Gross Motor Function Classification System (GMFCS) and the Activity Scale for Kids (ASK©). The GMFM (both 88- and 66-item versions) quantifies performance across lying-rolling, sitting, crawling-kneeling, standing and walking-running-jumping domains; GMFCS offers a five-level snapshot of ambulatory capacity and assistive-device needs; ASK© reflects the child's own report of participation in everyday tasks. All three map onto the International Classification of Functioning and have established minimal clinically important differences (Storm et al., 2020). Yet only a fraction of hippotherapy studies prioritize these gold-standard metrics, and previous reviews rarely stratify results by instrument (Plotas et al., 2024). Consequently, uncertainty persists not only about whether hippotherapy is helpful, but about how much improvement a therapist or family might realistically expect when progress is scored with tools that guide everyday decision-making. The present systematic review was designed to close that gap. We synthesized evidence from controlled studies in which hippotherapy was delivered as an active intervention for children and adolescents with CP and outcomes were measured with GMFM, GMFCS or ASK©. ASD was included in the a-priori search because equine-based programs are frequently recommended for children on the spectrum; however, no eligible ASD trials met our criteria, highlighting a separate evidence gap. By isolating standardized outcome data within a homogeneous diagnostic group, this review aims to provide a clear, clinically interpretable estimate of hippotherapy's effect on gross-motor function and to inform future work on optimal dosage (Jackman et al., 2022), cost-effectiveness (Alito et al., 2023) and long-term retention of gains (Mutoh et al., 2019).
Materials and Methods
A systematic review of the benefits of hippotherapy on the motor development of children with cerebral palsy and autism spectrum disorder was conducted using the ASK©, GMFCS and/or GMFM scales, following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). This review was registered in PROSPERO under the ID CRD420251135488.
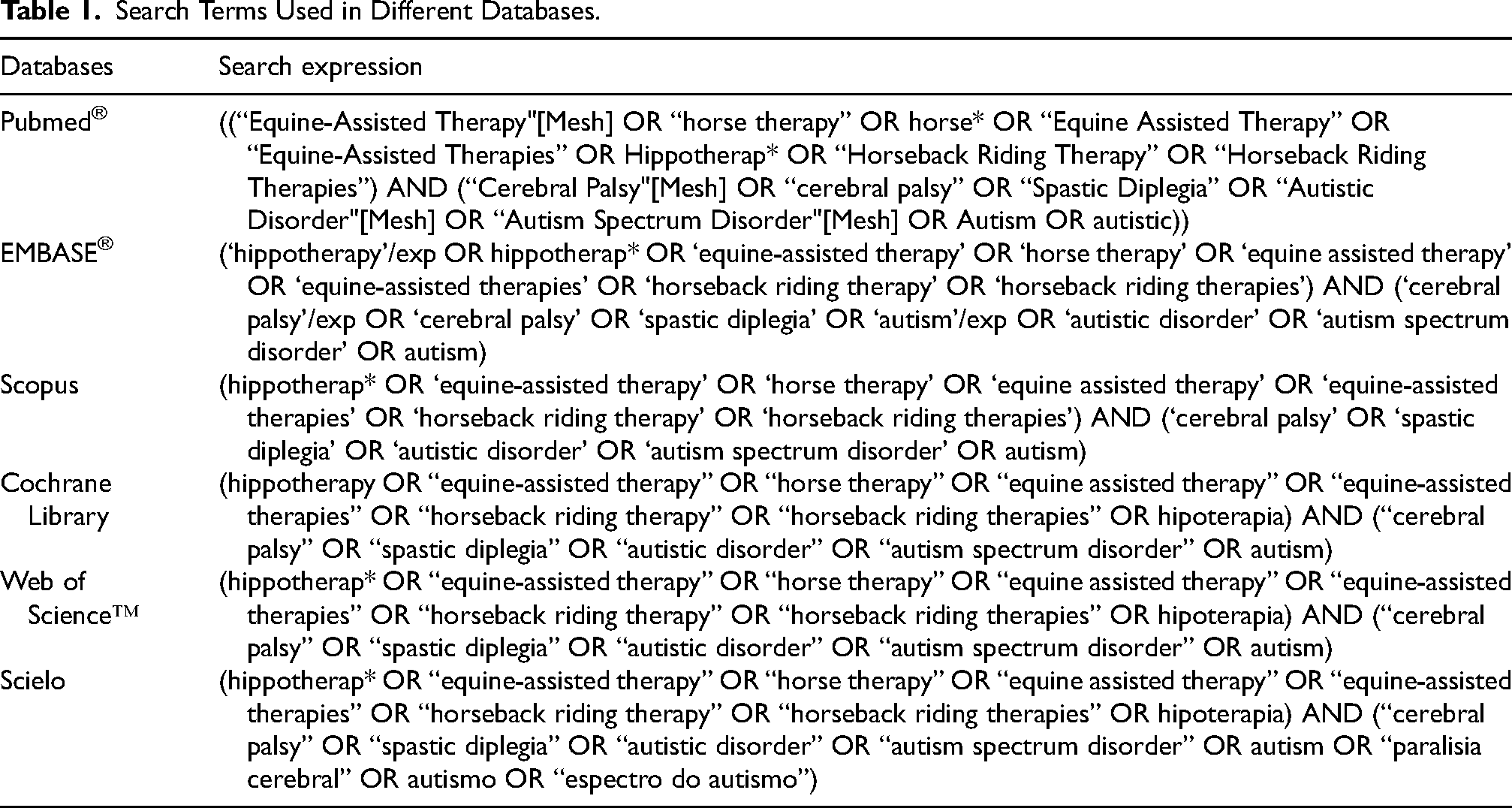
The search was conducted in the following databases: PubMed®, EMBASE®, Web of Science™, SCOPUS, Cochrane Library and Scielo. For the PubMed® and EMBASE® databases, combinations of controlled terms (MeSH terms - “Equine-assisted Therapy”, “Cerebral Palsy”, “Autistic Disorder” and “Autism Spectrum Disorder” and EMTREE terms - ‘hippotherapy’, ‘cerebral palsy’ and ‘autism’) together with non-controlled terms related to hippotherapy, cerebral palsy and autism were used to increase the sensitivity and specificity of the search. The search terms are described in Table 1.
Search Terms Used in Different Databases.
Selection Methods
To minimize selection bias, two reviewers (IB and JIS) independently screened titles and abstracts in Rayyan, a web-based systematic review tool (Ouzzani et al., 2016). Studies had to meet all of the following inclusion criteria:
Population: children or adolescents (6 months to 18 years) of either sex diagnosed with cerebral palsy or autism who received hippotherapy with live horses; Outcomes: motor performance assessed with the GMFCS, GMFM and/or ASK© scales; Language: article written in English, Portuguese or Spanish; Study design: randomized controlled trial, experimental or quasi-experimental study, cohort, case–control or cross-sectional study.
Exclusion criteria were the use of hippotherapy simulators instead of live horses, motor outcomes measured only with instruments other than GMFCS, GMFM or ASK©, publications in languages other than the three specified, and study types such as case reports, narrative reviews or editorials. Disagreements in screening were resolved by consensus, with a third author acting as referee where necessary. Full-text articles that passed the first screening were re-evaluated by the same reviewers using the same eligibility criteria. Finally, the reference lists of all included studies were scanned to identify further suitable publications.
Data Extraction
Data were extracted into a pre-formatted Microsoft® Excel spreadsheet (version 2311; Build 16.0.17029.20108). Data collected included information on authors, year of publication, country, study design, number of participants, age, sex, type of cerebral palsy, duration of hippotherapy program, motor-performance scores before and after hippotherapy, together with the reported pre- vs post comparisons. For nominal variables, absolute and relative frequencies were collected where available. Where available, nominal variables were recorded as absolute and relative frequencies. For continuous variables, we preferably recorded the mean ± standard deviation; if these were not provided, the median and interquartile range were recorded instead. When none of these summary statistics were provided, we transcribed the data exactly as they were presented in the publication.
Risk of Bias Assessment
Risk of bias assessment was performed independently by two reviewers (JIS and JCL) and conflicts were resolved by consensus. The RoB2 tool was used for randomized control trials, while the 12-item National Institute of Health (NIH) quality assessment tool for before–after studies was used for studies with no control group and ROBINS-I-v2 for non-randomized studies. These validated tools intend to identify potential risk of bias in different domains, such as patient randomization, study design and outcome assessment.
Results
Selection and Characteristics of the Studies
The search strategy in the databases yielded a total of 1019 articles for this systematic review, of which 507 were identified as duplicates by automatic and manual methods. When evaluating the titles and abstracts, 466 articles were excluded because they did not meet the eligibility criteria. A total of 39 studies were read in full (the full text was not available for 7 publications), and 16 were excluded. The exclusions were based on the following criteria: 11 studies did not include the scales selected for this systematic review, 2 studies did not use hippotherapy as a therapeutic method, 1 study focused on other pathologies and did not include cerebral palsy and autism, and 2 studies were written in languages that did not meet the inclusion criteria. Figure 1 shows the flowchart for article selection according to PRISMA recommendations. A total of 13 studies were selected through citation analysis, of which 11 studies were excluded after reading the full text. The exclusions were based on the following criteria: 8 studies did not include the selected scales, and 2 studies were review articles. The characteristics of the included studies are summarized in Tables 2, 3 and 4. A total of 602 children/adolescents with cerebral palsy participated in the 25 included studies (Alemdaroglu et al., 2016; Ali & Awad, 2022; Angsupaisal et al., 2015; Casady & Nichols-Larsen, 2004; Champagne et al., 2017; Chang et al., 2012; Cherng et al., 2004; Davis et al., 2009; Deutz et al., 2018; Hensangvilai et al., 2011; Jang et al., 2016; Kwon et al., 2011; Kwon et al., 2015; Lerma-Castaño et al., 2017; McGibbon et al., 1998; McGibbon et al., 2009; Mutoh et al., 2019; Mutoh et al., 2018; Park et al., 2014; Silkwood-Sherer et al., 2012; Silkwood-Sherer & McGibbon, 2022; Starling et al., 2019; Sterba et al., 2002; Temcharoensuk et al., 2015; Vidal Prieto et al., 2021), of whom 452 received hippotherapy treatment and 150 formed a control group. A total of 329 male children aged 1 to 18 years were included. The most common form of cerebral palsy was spastic (483 participants in total), followed by dyskinetic (5 participants) and ataxic (3 participants). It should be noted that no studies were found that included children/adolescents with autism spectrum disorders. Most of the included studies were conducted in the United States (6 studies) and South Korea (5 studies), with participants from Brazil, Japan, Saudi Arabia, Colombia, Thailand, Germany, Turkey, Taiwan, Canada, the Netherlands, and Australia.
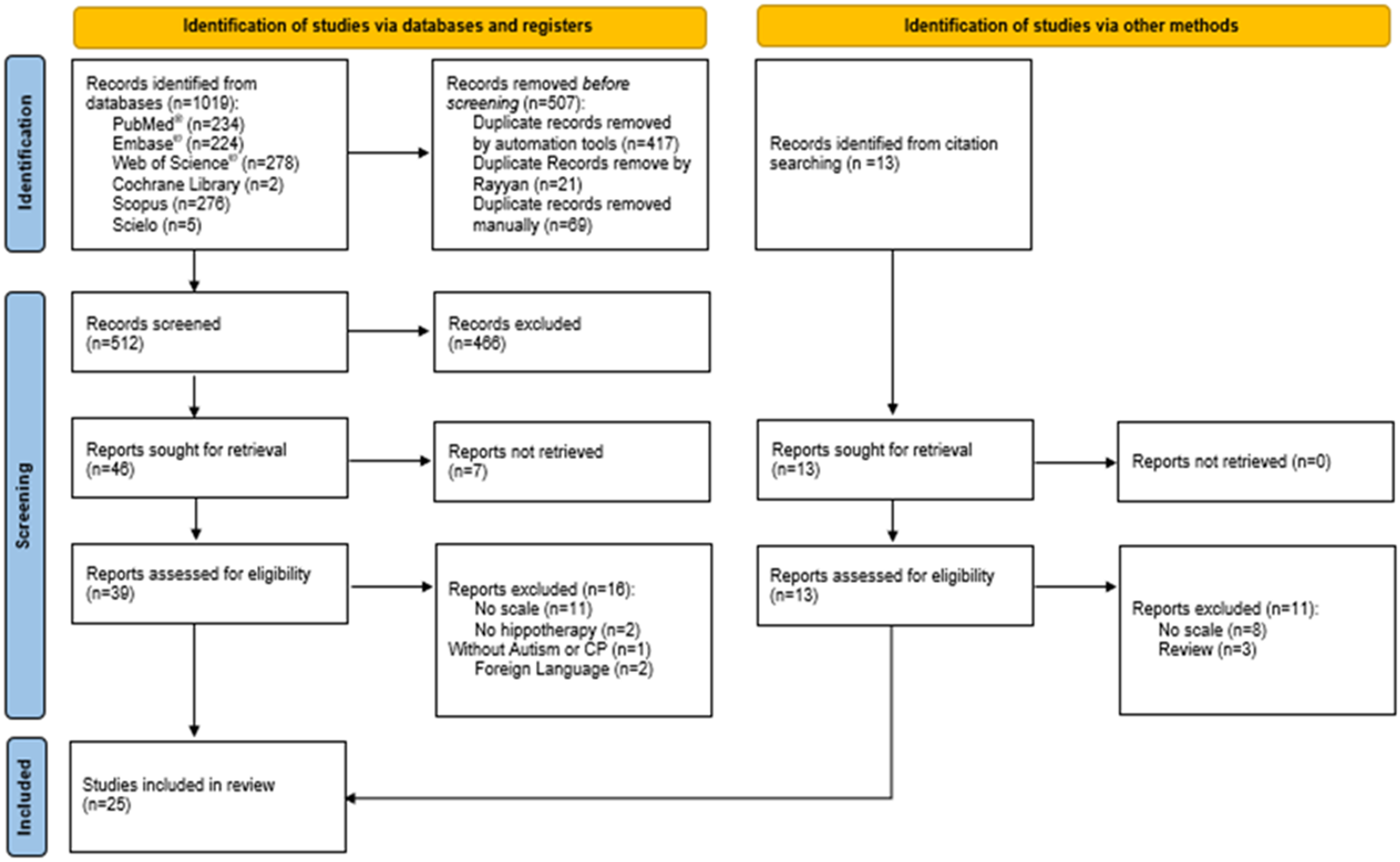
Flowchart of Research and Study Selection for the Systematic Review According to the PRISMA Guidelines.
Summary of the Characteristics of the Included Studies Using the Activity Scale for Kids©.

ASK: Activity Scale for Kids; CP: cerebral palsy; Ctr: control; Hpt: hippotherapy; IQR: interquartile range; NR: not reported; RCT: randomized clinical trial; SD: standard deviation.
USA: United States of America.
Summary of the Characteristics of Studies Using the Gross Motor Function Measure Scale.
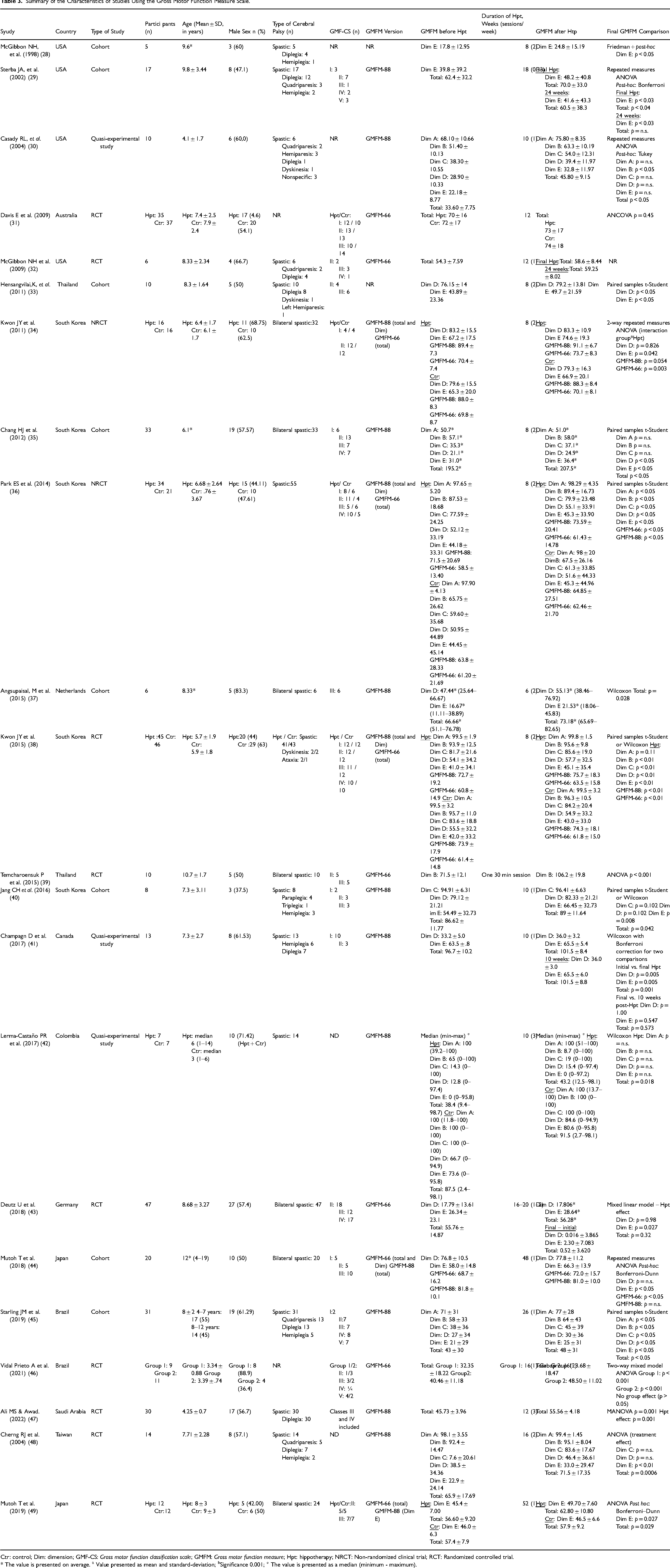
Ctr: control; Dim: dimension; GMF-CS: Gross motor function classification scale; GMFM: Gross motor function measure; Hpt: hippotherapy; NRCT: Non-randomized clinical trial; RCT: Randomized controlled trial.
* The value is presented on average. a Value presented as mean and standard-deviation; bSignificance 0.001; ° The value is presented as a median (minimum - maximum).
Summary of the Characteristics of the Studies Using the Gross Motor Function Classification Scale.

Ctr: control; GMF-CS: Gross motor function classification scale; Hpt: hippotherapy; NRCT: Non-randomized clinical trial.
§ Only results related to hippotherapy were reported, while the rest were related to simulator
Hippotherapy
Each hippotherapy session lasted on average between 30 and 45 min, with the exception of two articles in which the required session duration was 60 min (Angsupaisal et al., 2015; Sterba et al., 2002). The frequency of sessions varied from once to twice a week, with the number of weeks required in each study ranging from 2 to 52 weeks for each article. In the different studies, each hippotherapy session was accompanied by a physiotherapist or an occupational therapist in addition to the horse handler (80% of the studies). The sessions were usually conducted individually, although in 4 studies they took place in a group setting (Angsupaisal et al., 2015; Davis et al., 2009; Kwon et al., 2011; Kwon et al., 2015). Regarding the methodology of the individual sessions, they were conducted with a horse with a specific temperament, and it was common to use a therapy pad and lunging roll (63% of studies) (Ali & Awad, 2022; Angsupaisal et al., 2015; Champagne et al., 2017; Cherng et al., 2004; Hensangvilai et al., 2011; Jang et al., 2016; Kwon et al., 2011; Mutoh et al., 2018; Park et al., 2014; Silkwood-Sherer & McGibbon, 2022; Sterba et al., 2002; Vidal Prieto et al., 2021), in an indoor arena (8 studies) (Chang et al., 2012; Davis et al., 2009; Kwon et al., 2015; Lerma-Castaño et al., 2017; Mutoh et al., 2018; Park et al., 2014; Sterba et al., 2002; Temcharoensuk et al., 2015) or outdoors (4 studies) (Casady & Nichols-Larsen, 2004; Champagne et al., 2017; Mutoh et al., 2018; Vidal Prieto et al., 2021).
Motor Evaluation Using the Activity Scale for Kids (ASK)©
Two articles assessing global motor function using the ASK© scale were identified. These studies included 18 participants, 13 of whom underwent hippotherapy. In both studies, statistically significant improvements were found between pre- and post-hippotherapy assessments using this scale. It is worth noting that in one of the studies, this improvement was maintained 12 weeks after completion of the hippotherapy sessions (Table 2).
Motor Assessment Using the Gross Motor Function Measure (GMFM) Scale
Twenty-two articles used the GMFM to assess global motor function. Of the included participants, 29.22% were categorized as level II (walking with limitations) on the GMFCS, which corresponds to the most common level as shown in Table 3. Looking at the available versions of this scale, 13 studies (59.1%) used the GMFM-88 as the primary assessment tool, 7 studies (31.8%) used the GMFM-66 as the main scale and 2 studies (9.1%) did not specify the version of the scale used. It should be noted that 4 studies described the total score using both scales and one publication assessed dimension E using a different version of the scale than the one reported in their total score. A total of 19 articles described the GMFM total score, of which 14 studies used the GMFM-88 version and 9 used the GMFM-66 version. Only two articles (Davis et al., 2009; Vidal Prieto et al., 2021) showed no improvements in global motor function in children with cerebral palsy after a period of hippotherapy, although they found a slight increase in the GMFM-88 total score. One of these studies suggests that significant improvements could be achieved if the frequency of sessions was twice a week instead of once a week (Vidal Prieto et al., 2021). In the dimension-specific description, dimension E (walking, running and jumping) was the most frequently assessed. It was reported in 17 studies, of which 13 (76.5%) showed statistically significant improvements in this dimension. Dimension D (standing) was assessed in 14 publications, of which 6 (42.9%) showed a benefit of hippotherapy in improving this dimension. Dimension A (lying and rolling) was analyzed in 7 studies (all using the GMFM-88 version), of which 2 (28.57%) showed statistically significant improvements with hippotherapy. Dimension B (sitting) was described in 8 of the included studies. It was assessed with the GMFM-88 in 7 studies (87.5%), with 4 studies showing a benefit of hippotherapy in this dimension. The study that used the GMFM-66 also showed statistically significant improvements between the pre- and post-Hippotherapy assessments. Finally, dimension C (crawling and kneeling) is reported in 8 studies that used the GMFM-88 as an assessment measure. Of these, 3 studies (37.5%) showed statistically significant improvements when hippotherapy was performed. Children/adolescents categorized as levels I-III on the GMFCS were more likely to have better outcomes after hippotherapy sessions. One of the articles shows that a child who was initially categorized as level III according to the GMFCS was downgraded to level II after the sessions as he was able to walk independently without assistance (Casady & Nichols-Larsen, 2004). It is worth noting that 3 studies evaluated the effect of hippotherapy several weeks after the end of the sessions to assess the maintenance of the effects in the medium to long term. Of these studies, two reported that the effects of hippotherapy were maintained in the long term.
Motor Assessment Using the Gross Motor Function Classification Scale (GMFCS)
Only Alemdaroğlu et al. (Alemdaroglu et al., 2016) used GMFCS to assess whether hippotherapy is a good therapeutic tool for children/adolescents with cerebral palsy. This study included 16 participants, most of whom were male (56%). After five weeks of hippotherapy, no changes were noted in the level at which they were categorized at the beginning of the study, as shown in Table 4.
Risk of Bias Assessment
RoB-2 tool was used to assess risk of bias in 10 randomized controlled trials. The overall risk of bias was low for 4 studies, two showed some concerns (namely due to the randomization process and the measurement of outcome) and 4 showed a high overall risk (due to the measurement of outcome and missing outcome data). ROBINS-I-v2 scale was applied for 3 studies: one showed an overall moderate risk of bias, due to the selection of participants, and one showed a high risk of bias, due to missing data.The remaining 11 studies were assessed using the NIH quality assessment tool. The number of positive answers ranged from 4 to 11, with 8 studies scoring 8 or more points. Questions 1, 7 and 10 had positive answers for all studies. A detailed description of the application of RoB-2, ROBINS-I-v2 and NIH tools is available in supplementary tables 1, 2 and 3, respectively.
Discussion
Principal Findings
This review identified 25 studies that evaluated hippotherapy in children and adolescents with cerebral palsy using at least one of three motor-function instruments - ASK©, GMFCS, or GMFM. Although Portuguese-language versions of the ASK©, GMFCS, and GMFM-66 (European and Brazilian Portuguese) have already been translated and psychometrically validated (Almeida et al., 2016; de Oliveira et al., 2023; Hiratuka et al., 2010; Paixão et al., 2016), published reports showing how these tools are being used in Portuguese clinical or research settings are still scarce, and a Portuguese validation of the full GMFM-88 remains unavailable. Only two studies (Silkwood-Sherer et al., 2012; Silkwood-Sherer & McGibbon, 2022) employed the ASK©, and both reported significant pre-to-post gains, supporting hippotherapy as a promising intervention for motor-function development. Most of the included studies were based on the GMFM, but they differed in the version analyzed. The GMFM-66 was derived from the GMFM-88 by removing 22 items with low internal consistency - 13 from Dimension A, five from Dimension B and four from Dimension C; Dimensions D and E remained unchanged (Russell et al., 2010). Of the four studies that calculated total scores with both versions (Kwon et al., 2011; Kwon et al., 2015; Mutoh et al., 2018; Park et al., 2014) all found a significant improvement with the GMFM-66, while only two found a change with the GMFM-88. These results emphasize the greater sensitivity and reliability of the GMFM-66 in detecting hippotherapy-induced motor progress.
Clinical Significance
Most authors have focused on dimensions D (standing) and E (walking, running, jumping) of the GMFM because the baseline values in these tasks are typically the most impaired and therefore offer the greatest opportunity for improvement. Improvements in these dimensions have a direct impact on everyday activities such as transferring, walking around and playing, so even modest changes in scores can be clinically significant. For some authors, hippotherapy has shown positive results in improving global motor function. McGibbon et al. found evidence of this improvement up to 12 weeks after the end of sessions (McGibbon et al., 2009), as did Casady RL et al., and Cherng et al., who reported that the results were maintained after completion of hippotherapy (Casady & Nichols-Larsen, 2004; Cherng et al., 2004). One study (Champagne et al., 2017) shows that there are no differences in the D, E and total score dimensions 10 weeks after hippotherapy compared to when the hippotherapy sessions ended, suggesting that the improvements are maintained in the long term. Two studies (Starling et al., 2019; Sterba et al., 2002) describe that part of their sample had previously undergone hippotherapy sessions and showed significant improvements.
How Much Change is “Clinically Important”?
Across all studies, gains of ≈2–4 GMFM points/percentage points are typical, significantly exceeding published MCID thresholds and suggesting that the statistical improvements reflect real, functionally relevant changes.
Methodological Considerations
The heterogeneity between the studies was determined both by the previous experience of the participants and by the “dose” of the intervention In several studies, children who had already participated in hippotherapy programs were not examined, so baseline motor skills may have already been increased, which limited any measurable change during the study period.
Limitations
One of the limitations of this systematic review was the lack of articles related to ASD, although hippotherapy is a therapeutic approach chosen by families. No articles were found that used the ASK©, GMFCS and GMFM scales to assess global motor function in these children/adolescents with autism. Another limitation of the search was that for this systematic review, only two studies were found that assessed the global motor function of children/adolescents with CP using the ASK© scale, a scale that assesses different aspects of motor functionality and consequently their independence and quality of life. We must also emphasize the heterogeneity of the study design in the included studies. The small samples and the lack of control groups in more than 60% of the studies precluded meta-analysis and increased the risk of bias. Finally, by limiting our analysis to studies that reported GMFM-66/88, GMFCS, or ASK©, we maximized clinical interpretability but necessarily excluded studies that used biomechanical surrogate scales or parent-reported scales. As a result, our pooled estimates reflect only the subset of evidence based on standardized gross motor metrics and may underestimate the full extent of the effect of hippotherapy. In addition, the restriction reduces the sample size and precludes meta-analysis for GMFCS and ASK©. Readers should therefore consider our conclusions to be very specific to gross motor outcomes and not a comprehensive assessment of all potential benefits.
Future Directions
Future studies need to move beyond small, single-center case series to rigorously designed, pre-registered, multicenter, randomized controlled trials that use concealed allocation and are sufficiently powerful to detect effects in all GMFCS subgroups. Agreement on a core outcome set - GMFM-66 (with an optional trunk-control add-on), ASK©, and a fatigue or participation scale - will make the results comparable and clinically meaningful. Studies should also incorporate dose–response issues into their design by directly comparing sessions longer than 45 min with shorter sessions and programs lasting eight weeks or longer with shortened courses to determine the minimum effective dose. Since there is no controlled data yet for children on the autism spectrum, applying the same protocol to this population would fill an important evidence gap. Finally, follow-up periods of at least six months are needed to determine whether the gains in gross motor skills achieved through hippotherapy translate into lasting improvements in daily functioning.
Conclusion
This systematic review synthesized the most recent controlled evidence on hippotherapy for children and adolescents with cerebral palsy using only standardised outcome measures (GMFM-66/88, GMFCS and ASK©. Pooled data indicate a mean GMFM-66 increase of about 4 raw points (≈ 0.64 SMD), exceeding the MCID by a factor of three to five and corresponding, for a child at GMFCS Level II, to progress from limited community ambulation to independent 10-metre walking. A practice implementation is one 45-min hippotherapy session weekly for at least eight consecutive weeks, ideally initiated once progress with conventional physiotherapy plateaus. These findings are specific to improvements quantified with GMFM-66/88, GMFCS and ASK© and should not be generalized to outcomes assessed with other instruments. Methodologically, the heterogeneity of the study design and the incomplete reporting of concomitant therapies limit certainty. This emphasises the need for preregistered, adequately driven studies that include long-term follow-up and cost analyses. Nevertheless, taken together, these findings support the inclusion of hippotherapy as an evidence-based adjunct to conventional pediatric neurorehabilitation programs aimed at improving gross motor autonomy in children with CP.
Supplemental Material
sj-docx-1-nre-10.1177_10538135251387278 - Supplemental material for Hippotherapy Improves Gross Motor Function in Children with Cerebral Palsy: Evidence from a Systematic Review
Supplemental material, sj-docx-1-nre-10.1177_10538135251387278 for Hippotherapy Improves Gross Motor Function in Children with Cerebral Palsy: Evidence from a Systematic Review by Inês Bernardino, Daniel Filipe Borges, João Casalta-Lopes and Joana Isabel Soares in NeuroRehabilitation
Footnotes
Author Contributions
IB: Conceptualization, data curation, formal analysis, interpretation of data, writing original draft. DFB: Formal analysis, interpretation of data, writing review and editing. JCL: Conceptualization, formal analysis, interpretation of data, writing original draft. JIS: Conceptualization, data curation, formal analysis, interpretation of data, writing review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.