
Abstract
A family counseling intervention grounded in systemic family therapy was conducted in a Title I school-based setting with (N = 48) kindergarten through sixth-grade student-clients and their primary caregivers. Families’ perception of family communication and satisfaction on the Family Adaptability and Cohesion Evaluation Scale-IV was investigated to determine changes in the percentile score at three benchmarks. A repeated measure analysis of variance indicated a statistically significant difference over time in caregivers’ perception of family communication and satisfaction after 5 and 10 weeks. There was no difference in relationship to gender. School-based family counseling programs can contribute to improved family communication and satisfaction. School-based counselors can partner with institutions of higher education to provide free and accessible counseling for students and families in the greatest need.
Keywords
Mental health challenges are problematic for youth and families in the United States and may create obstacles to school success. Approximately 20% of children have had a diagnosable mental health disorder at some time period in their lives and only one in the five of those children receives the necessary and appropriate services for treatment (Capp, 2015; Kaffenberger & Seligman, 2007; Merikangas et al., 2010). When mental health concerns are not addressed during childhood, they may negatively influence future academic achievement and social–emotional problems throughout adulthood (i.e., depression, anxiety; Beaudoin, 2016). Children with mental health concerns are more likely to be suspended and expelled for behavioral problems and tend to have a higher number of absences from school than their school counterparts without the same challenges (Stagman & Cooper, 2010).
Environmental stressors may impact families living in low-income communities contributing to substantial disparities in childhood and overall well-being and mental health (Macklem, 2014; Stagman & Cooper, 2010; Williams & Greenleaf, 2012). Children from low socioeconomic status (SES) families often encounter multiple barriers when trying to access mental health services (Gamble & Lambros, 2014). Barriers for low SES families utilizing professional mental health treatment for their children may include (a) the lack of insurance or financial means to pay for services, (b) existing language barriers, (c) limited transportation, and (d) stigmas and misconceptions surrounding mental illness (Gambles & Lambros, 2014). Children may react to unmet mental health needs through internalizing (e.g., depression, anxiety, withdrawal) and externalizing behaviors (attention seeking, hyperactivity, aggression) within the school and home environments (Axelrod et al., 2009; Ballard et al., 2014). Therefore, it is imperative that families and school communities work together to identify and treat children’s mental health issues to promote prosocial behavior, academic performance, and emotional well-being (Beaudoin, 2016). Mental health services within schools can be one way to strengthen the partnership between families and schools (Anakwenze & Zuberi, 2013; DiCocco, 1986). Mental health professionals placed in the school setting may bridge communication and foster collaboration between administrators, teachers, and guardians when implementing mental health treatment for a child (Blount, 2012; Cooper-Haber & Haber, 2015; DiCocco, 1986; Ofordile, 2009; Terry, 2002). Additionally, providing counseling within the schools may raise awareness among school staff and families concerning early mental health concerns warning signs before symptoms are exacerbated (Capp, 2015; Cefai & Cavioni, 2015; Salerno, 2016).
Literature Review
Family factors such as family SES and dysfunctional family factors (e.g., lack of family cohesion, family conflict, rigid family parenting styles, home environment instability) can contribute to children’s academic performance and learning which can be predictors of lower levels of academic success for children (Crespi & McNamara, 2015; Oxford & Lee, 2011). The consequences of not addressing childhood mental illness have implications in other societal systems. There has been a rise in juvenile offending, and youth involved with the Department of Juvenile Justice have a higher rate of mental health issues (Scholt & Van der Ploeg, 2015; Vincent et al., 2008). Children in vulnerable populations, including low SES, are frequently exposed to multiple traumatic events throughout their childhood, such as abuse, neglect, and secondary adversities that derive from distress (Osofsky et al., 2015). Furthermore, children from families living below or at the poverty line may lack parental involvement and support for learning pursuits due to families’ own educational background or limited resources (Oxford & Lee, 2011). Transgenerational education patterns are established over multiple generations within a family. These patterns may lead to decreased school–family bonding or may lead to a deficiency in school relationships that may inhibit academic success as measured by achievement. In one study of third-grade students, conducted by Dubow et al. (2009), guardians’ level of education was found to predict similar education levels and occupational prestige for their children. Moreover, children’s self-efficacy and potential are affected by these complex factors that are beyond their control (Crespi & McNamara, 2015).
School-Based Mental Health Counseling Services (SBMHCS)
SBMHCS are defined as any program, intervention, or strategy applied in a school setting that was specifically designed to influence students’ emotional, behavioral, or social functioning (Rones & Hoagwood, 2000). SBMHCS have been shown to be effective in benefiting children, families, and the school community in a variety of ways including engagement and attendance (Anakwenze & Zuberi, 2013). In school settings, children and their families are more engaged in counseling services and exhibit increased cooperation with treatment interventions made by school-based mental health professionals compared with counseling settings in outside agencies (Mince, 2000; Perfect & Morris, 2011; Solomon et al., 2016). A research synthesis of 23 studies investigating the effectiveness of mental health services delivered in school-based settings found that adolescents were 21 times more likely to utilize school-based mental health services compared to community health centers (Bains & Diallo, 2016). SBMHCS attendance rates are higher than outside community health centers, as they are typically free and are offered in the school, which helps to mitigate barriers to receiving services (Blackman et al., 2016). Ultimately, without SBMHCS, vulnerable children may not otherwise receive the help they need. If a healthy family–school bond is already established, stigmas related to seeking mental health counseling in families from low-income communities may be minimized (Anakwenze & Zuberi, 2013).
Montañez et al. (2015) examined the effectiveness of SBMHCS to treat children living in poverty in New York City. A comprehensive school-based mental health promotion and prevention program indicated that students from ethnic minority backgrounds made strides in social performance, attendance, and standardized test scores. Lambros and colleagues (2016) found students with a dual diagnosis of intellectual disabilities and a co-occurring mental health disorder who participated in a school-based intensive outpatient program had a reduction in the number of school suspensions and absences. Students in their study also displayed positive changes in behavior per caregiver report. Overall, the literature supports the notion that SBMHCS helps improve child suspension rates, academic performance, internalizing behavior, and externalizing behavior (Ballard et al., 2014; Bernstein et al., 2005; Kayler & Sherman, 2009; Liber et al., 2013).
However, there are some research synthesis and meta-analytic studies that provide conflicting evidence of SBMHCS. A meta-analytic review of 23 studies between 1985 and 2009 investigated the impacts and outcomes of SBMHCS on low SES urban youth and concluded the evidence for program and service effectiveness was limited (Farahmand et al., 2011). Noted limitations of the studies in the review included (a) small sample sizes, (b) lack of information to support the developmental appropriateness of the SBMHCS interventions, and (c) minimal follow-up measures to further evaluate provided interventions. Conversely, Salerno (2016) conducted a systematic literature review of 15 studies relevant to the effectiveness of universal mental health awareness interventions in K–12 schools and suggested that improved knowledge and attitudes of mental health awareness can be enhanced by SBMHCS. Nevertheless, the review cautioned that the results are not generalizable because most of the studies’ research designs were not rigorous enough to claim cause–effect relationships.
Systemic Family Therapy (SFT)
SFT is a theoretical orientation and family systems approach that conceptualizes human behavior and mental health challenges through the lens of the social systems in which the client or the family is situated (Retzlaff et al., 2013). SFT is a paradigm shift from client’s individualized perspective to a systems perspective (Ray, 2016). Incorporating the entire family system allows room for understanding all components of a client. Assisting an individual with their functioning in isolation of family connections, relationships, and intergenerational elements is a secondary pursuit in SFT (Goldenberg et al., 2017). SFT primarily focuses on the organization of the family system and communication patterns, reciprocal interactions, and connections with larger ecological systems (e.g., school, work, cultural memberships, and community support) and any other micro- or macrosystems (Goldenberg et al., 2017).
The SFT framework and family-based interventions address the whole family system including all subsystems (parent–parent, parent–child, sibling–sibling, and nuclear family–extended family). Furthermore, SFT approaches may be well suited to target changes in school-aged children’s overall mental health outcomes (Goldenberg et al., 2017; Lorås, 2018; Riedinger et al., 2017; Ungar, 2015). Regardless of the treatment setting, SFT practice has shown to help reduce negative outcomes associated with child abuse and neglect (Carr, 2009, 2014). Many internalizing behaviors which may lead to mood disorders, somatic illness, and eating disorders, and externalizing behaviors which may lead to conducts disorders, substance abuse, and attention deficit hyperactivity disorders are manifestations of childhood abuse and neglect (Carr, 2009, 2014; Cottrell & Boston, 2002; Sydow et al., 2013).
School-based family counseling (SBFC) is family counseling that takes place in the school setting. Gerrard (2008) conducted a review of the literature across mental health professions dating back from the 1920s and reported that the major benefits experienced by students receiving SBFC included (a) improved academic functioning, (b) reduced problematic emotional and behavioral symptoms, (c) decreased incidences of classroom disruption affecting other students, (d) improved prosocial behaviors in the home, (e) strengthened relationships between schools and families served by SBFC, and (f) promotion of cost-effective access to counseling services. Stormshak et al. (2011) conducted a controlled experimental design with a random sample of 593 adolescents and their families from three Title I middle schools occurring over a span of 3 years. Stormshak et al.’s (2011) findings demonstrated that family-centered interventions lowered students’ incidences of antisocial behaviors as well as substance abuse throughout the middle school years. Such findings suggest the union between the SFT approach and the school setting can positively impact children, families, peers, school staff, and teachers.
The majority of research done on SBMHCS has focused on individualized treatment for youth, without incorporating the family system (Cooper-Haber & Haber, 2015; Green, 2015). A future direction for expanding the reach of SBMHCS would be to incorporate a family systems approach in the counseling process within the schools. Using a family systems approach, while incorporating mental health professionals, teachers, and administrators may lead to a decrease in student dropout risk factors (e.g., poor attendance, low-grade achievement, suspension, and conduct issues; Blount, 2012; Boutelle, 2010; Ofordile, 2009; Powell, 2011; Stagman & Cooper, 2010).
The effectiveness of family counseling to target child mental health issues has been established in nonschool settings and contexts (Carr, 2009). However, the lack of research regarding SBFC may be due to a lack of training in the family systems approach and working in a school setting (Mince, 2000). Martin (2013) surveyed a random sample of 657 members of the American School Counseling Association and found (a) school counselors did not feel adequately prepared and competent to use a family systems perspective, (b) school counselors thought family systems practice was less important in the school setting, and (c) family systems practice was used less frequently in the school systems. The importance of utilizing a family systems approach to mental health counseling with children in school settings may mitigate school personnel’s misconceptions of problems originating from within the child alone without consideration of the family system and the notion of the child being “bad” (Powell, 2011).
Elementary school students from low SES families experience higher rates of mental health concerns, which left untreated may persist into adulthood (Solomon et al., 2016; U.S. Department of Health and Human Services, 2001). Limited transportation, stigma associated with mental health, lack of finances, and restricted number of services are some of the possible barriers to children living at low SES levels receiving psychological services (Gamble & Lambros, 2014). SBFC services are a good option to help mediate some of the known barriers of families and children accessing mental health resources (Powers et al., 2013). Although family systems approaches have been shown to be effective with children in vulnerable populations, there is a lack of research and focus on SBFC.
Thus, the purpose of this investigation is to examine the effectiveness of SBFC intervention with children from three Title I elementary schools on family communication and family satisfaction and caregivers’ perspectives of the intervention. The research questions for the investigation are as follows:
Method
A mixed-methods convergent designed study was conducted to investigate an SBFC intervention with children from three Title I elementary schools.
Context of the Study
Through an established school-based partnership between an institution of higher education and a school district, an SBFC program was conducted during a 30-week period. The elementary school student-clients were recruited from the current student body of three Title I elementary schools in the southeastern United States. The percentage of students receiving free and reduced lunch at the three elementary schools was (a) School 1, 95%; (b) School 2, 87%; and (c) School 3, 92%. The gender of the students at the three elementary schools (N = 2,247) is equally divided (females = 1,101 [49%] and males = 1,146 [51%]). The students at the three elementary school identified with the following ethnic/racial groups: Black/African American (n = 1,057, 47%), Hispanic (n = 639, 28%), White (n = 491, 22%), Multiracial (n = 110, 5%), Asian (n = 22, <1%), Indian (n = 5, <1%), and Hawaiian or Other Pacific Islander (n = 5, <1%). Geographically, all three schools were located in suburban areas within 5 miles of each other.
Procedures
Recruitment of the elementary school student-clients was facilitated through school personnel (e.g., administrators, teachers, family liaisons, and school counselors) using convenience sampling. Specifically, school counselors contacted the clinical coordinator with the names of potential student-clients. The clinical coordinator then contacted the parents or guardians to inform them about the no cost, SBFC services, and confirm interest. A clinical coordinator recruited student-clients by attending parent events at the schools and passing out recruitment brochures to interested families. Finally, parents or guardians contacted a research team member if they were interested in having their child and family receive mental health services and participate in the research investigation.
Parents or guardians and their children participated in a prescreening interview that provided details about the counseling services and assisted in completing initial paperwork (e.g., Parent/Guardian Informed Consent for Research, Client Information, and Consent for Counseling Services). In addition, sample screening was employed to ensure that the SBFCI provided was appropriate to meet the needs of the elementary school students and their families. For instance, research team members confirmed that (a) the student-clients/families were willing to participate in the counseling services provided after school hours, (b) transportation would be provided from school after each scheduled session, and (c) scheduled sessions would be attended on a regular basis. The SBFCI was available after school hours for 3 hr 1 day per week at each school. The SBFCI was provided for 30 weeks of the academic school year. Additionally, efforts were made to ensure that student-clients’ presenting concerns would be appropriately addressed by novice counselors under the direct supervision of experienced clinical supervisors.
Participants’ data were collected at three time points—baseline, after five sessions, and after 10 sessions—to investigate change. Prior to the recruitment of participants, approval was granted from the university’s institutional review board and the participating school district to conduct the study.
Participants
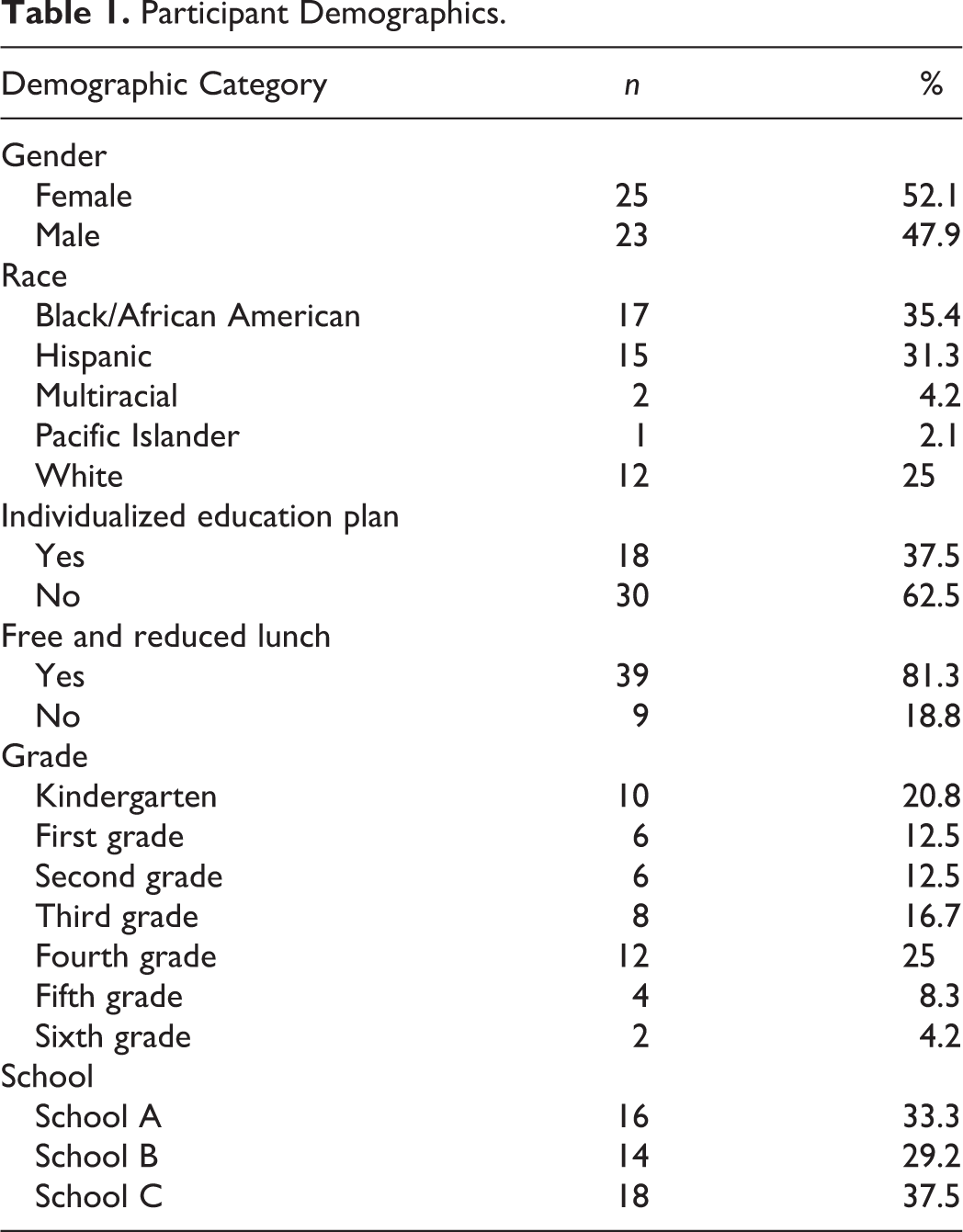
A total of 48 kindergarten through sixth-grade student-clients completed more than five counseling sessions within the SBFCI with complete data collection (see Table 1). The mean age of the student-client was 7.64 years old (SD = 1.905, range = 4–11). Participants were almost evenly split on gender, with 52.1% identifying as female (n = 25) and 47.9% identifying as male (n = 23). The majority of participants belonged to an ethnic/racial minority, with only 25% (n = 12) identifying as White, 35.4% identifying as African American (n = 17), and 31.3% identifying as Hispanic (n = 15). Almost 38% of participants had an individualized education plan (n = 18), and 81.3% qualify for free or reduced lunch (n = 39).
Participant Demographics.
Systemic Theory as the School-Based Family Counseling Intervention
All student-clients received treatment from counselors who were trained in systemic theory. Rather than applying a theoretical orientation and techniques typically focused on individualized treatment, counselors used SFT to guide the SBFCI that sought to benefit the student participants and their families. Counselors collaborated with family members toward creating healthier emotional relationships, effective communication patterns, clear boundaries, and problem-solving as the primary objective of treatment, in addition to ameliorating the presenting problem of the child and their accompanying symptoms (Kaslow et al., 2012). The counselor initiated treatment by assessing the child, family members, and teachers, essentially mapping the ecosystem of the child and family before designing steps of the treatment plan with the family (Goldenberg et al., 2017). For example, each counselor used a genogram as an initial assessment technique to obtain a graphic representation of the nuclear and extended family on both sides over three generations, which allowed counselors to investigate the origin of the family’s and child’s presenting problem.
Counselors used SFT traditions to hypothesize the question of which dysfunctional mechanisms kept families from changing (homeostasis) when it was necessary (Cottrell & Boston, 2002). The counselors assisted the family in gaining insight into the origins of their problems through establishing circular causality. Instead of attributing certain problems to an identified family member, or a linear chain of events with a cause-and-effect relationship to problems, families were able to recognize the multiple relational transactions and environmental conditions that modulate and perpetuate members’ characteristics and behaviors (Flaskas, 2010). The counselors were advised to take a nonpathologizing approach and view of the family while structuring the therapeutic process in such a way in which blaming is minimized, transparency is encouraged, and appreciation is expressed among members in and out of session (Lorås, 2018). Furthermore, counselors taught parents and guardians cognitive and behavioral skills, such as managing negative interactions and affecting regulation strategies applicable to themselves and their children (Kaslow et al., 2012). Families were able to learn a balance of establishing both firmness and flexibility around rules and family roles in order to reach a better level of family functioning (Goldenberg et al., 2017).
Supervision
Clinical supervision was provided to counselors to ensure the welfare of the clients and to promote treatment fidelity to SFT counseling. Each supervisor was trained in SFT and family counseling. Clinical supervision included live supervision, group supervision, and triadic supervision. Prior to each counseling session, counselors participated in group supervision at one of the school sites. This supervision provided counselors the opportunity to discuss their clients, learn SFT techniques, and receive feedback on their approach from their peers and supervisor. Additionally, supervisors provided live supervision through bud-in-ear technology while counselors were providing services to ensure client safety with immediate feedback. Finally, counselors received triadic supervision off-site where they were able to process their clinical work and discuss treatment goals related to SFT. Through supervision, counselors received formative and summative feedback to facilitate their clinical growth working with families that aligned with SFT.
Instrument
FACES-IV is a self-report assessment to measure family cohesion and family flexibility. The 42-item assessment is meant to measure the effectiveness of family therapy (Olson, 2011). There are six subscales within the instrument, two of which were considered in this investigation, the Family Communication and Family Satisfaction. Scoring is completed using an Excel spreadsheet. Parents’ responses are recorded, and scores are automatically calculated for subscales. For this study, the percentile scores for each of the subscales under review were considered at three time points: precounseling and after 5 and 10 counseling sessions.
Feedback Form
A feedback form was deployed after Sessions 5 and 10 asking caregivers to share any other thoughts about their child and the SBFC sessions. The form consisted of one question: Please indicate anything else that you would like to share or clarify about your child and the SBFC sessions that were not addressed in the FACES-IV instrument that you just completed. It was determined from prior years of conducting school-based family interventions that some caregivers preferred to provide more information than a scale allowed.
Data Analysis
To analyze the percentile scores obtained from the FACES-IV data (e.g., Family Satisfaction and Family Communication), a repeated measure analysis of variance (ANOVA) was conducted to determine the mean change in scores from preintervention to two time points during therapy (5 and 10 sessions). Data were cleaned and limited to those who had participated in family therapy sessions and had three scores on both subscales. Next, data were screened for outliers and one participant was removed as they had more scores than session visits. Other statistical analyses included a paired sample t test of the Family Satisfaction and Communication after the Session 5 and Session 10 benchmarks.
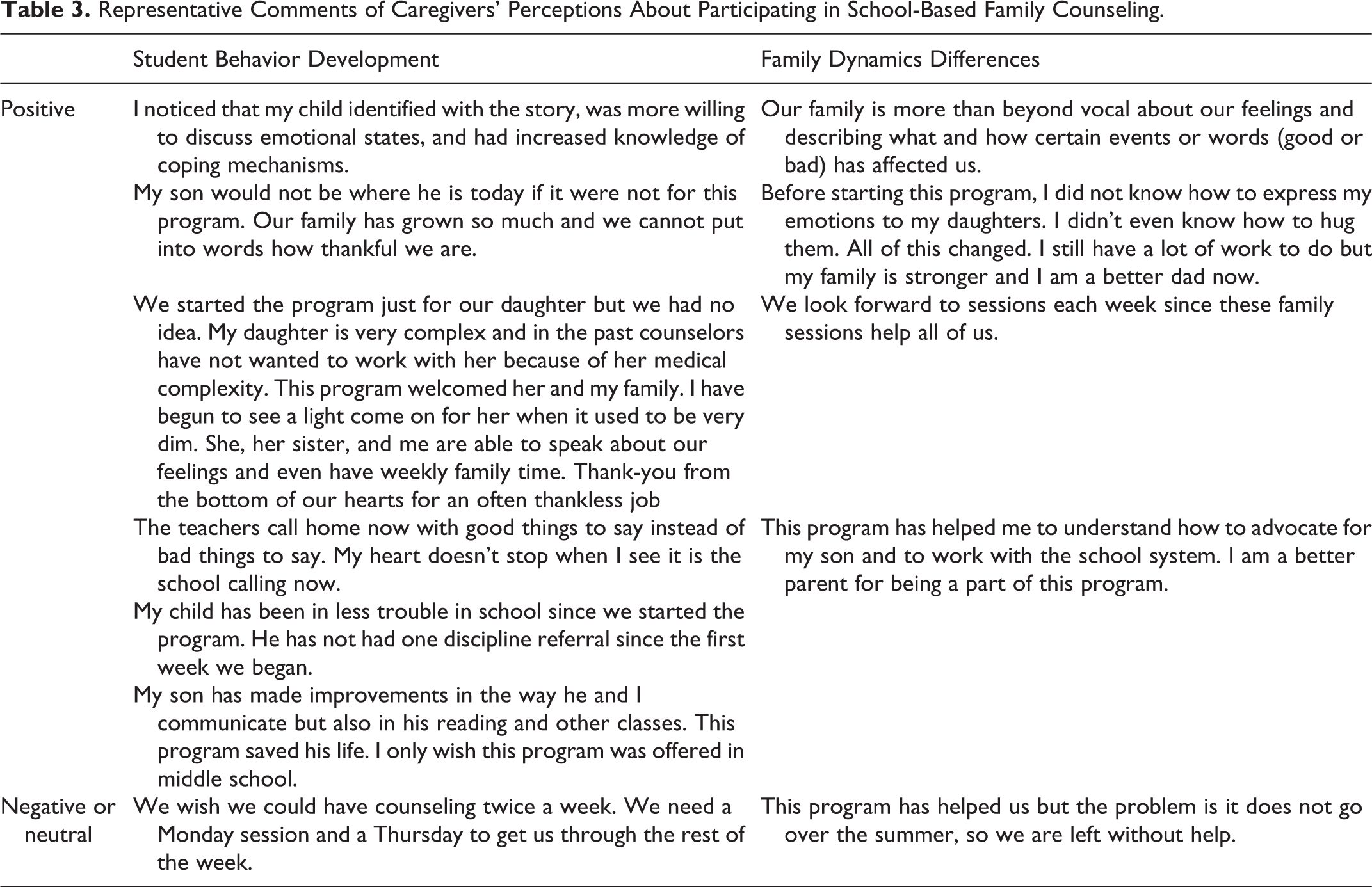
To analyze the open-ended questions on the feedback form, all results were read by two of the authors. Potential codes were jointly determined based on the initial readings and the meaning patterns observed. Two overarching themes emerged: (a) student behavior development and (b) family dynamics differences. These themes were further categorized into positive/advantages, strengths/negative, and challenges/limitations. Next, the researchers coded all comments into these themes and subcategories. To eliminate researcher bias, the comments were coded independently and then converged to establish consensus. In the rare instance where there was divergence, the coders discussed the rationale for their coding and consensus was met.
Results
Paired Sample t Test for Family Satisfaction and Communication.

A repeated measure ANOVA was conducted to evaluate the mean increase of the construct family satisfaction over time. There was a main effect for time, Wilks’s λ = .49, F(2, 28) = 28.96, p < .001,
To answer Research Question 2 about caregivers’ perceptions of school-based family therapy as it specifically relates to their child and family, caregivers’ comments from an open-ended question were coded and categorized. Of the possible 48 families represented, the program received 22 responses to the open-ended question. Eighty-six percent of the comments were rated as positive. The other 14% were neutral comments or negative. Sixty-eight percent of the comments related to student behavior development and the other 32% were related to family dynamic differences. These unsolicited comments were coded into two themes: student behavior development and family dynamic differences (Table 3).
Representative Comments of Caregivers’ Perceptions About Participating in School-Based Family Counseling.
Discussion
Limited research has investigated the effectiveness of SBFCI with children and families. In this mixed-methods convergent study, an SBFC intervention was conducted with children from three Title I elementary schools. Participants were asked to rate aspects of family communication and satisfaction utilizing the FACES-IV. To contextualize the quantitative results, caregiver perceptions were collected at the same time.
The findings indicated a statistically significant difference in caregivers’ ratings on the FACES-IV of family satisfaction and family communication, indicating that their family communication as well as their satisfaction with each other improved over time. These results are similar to other studies conducted in schools (Cooper-Haber & Sanchez, 2013). When family counseling occurs and is continual and all parties are committed, there can be improved communication and family satisfaction. Gerrard and Soriano (2013) noted school-based family counseling was a culturally responsive modality for family counseling. Similarly, in this study, at three Title I schools inclusive of underserved and underrepresented populations, school-based counseling correlated with improved family communication and satisfaction. Caregivers in this study confirmed that family counseling was a needed support for their families (Gerrard & Soriano, 2018) and that students’ school and home behavior improved as the families participated in counseling. Further, our results indicate school-based counseling was an important contributor to family cohesion, parental involvement, and school engagement for diverse youth and played a key role in academic success (Stormshak et al., 2010).
The school environment can be an important context for family counseling as counselors in this study were viewed as an extension of the school system. By virtue of the counseling taking place at school, families felt supported by the school because the family therapist established a safe space in a familiar setting. Furthermore, when families feel supported by the school, the school–family bond is strengthened, which may lead to better academic gains for children (Cooper-Haber & Sanchez, 2013). School-based family therapists can provide needed support for their clients since navigating family, school, and community systems is a crucial component of family and school success.
Caregivers’ perceptions of school-based family therapy provided evidence of student’s behavior development and family dynamic differences. Caregivers attributed the student’s academic and personal behavioral improvements to participating in SBFC partnership. The way a family system functions influences the child’s well-being including their internalizing and externalizing behaviors (Scholte & Van der Ploeg, 2015). When family discord decreases and positive functioning increases, the likelihood of the child’s success in and out of school becomes greater. Caregivers and students attributed improvements to having tools for communication and problem-solving. Other researchers have noted the importance of the partnership between school-based family therapists, caregivers, the family system, and academic performance (Soriano et al., 2013).
Limitations and Implications
The limitations of this study included the limited number of participants for all data points collected. The number of participants between the pretest and 10 visits decreased, perhaps due to attrition, survey fatigue, or caregivers not completing or returning forms as intended. The limited number of respondents limits the generalizability of the findings.
Implications for schools include seeking a partnership with a local university and their counselors-in-training programs to provide school-based family therapy at the school (Gerrard & Soriano, 2013; Soriano et al., 2013). Providing a program for youth in schools can reach students who may not otherwise access mental health services (Gamble & Lambros, 2014) and reduce social stigmatization (Solomon et al., 2016). District and school administrators can further support school-based, family counseling interventions by providing resources such as time and space for counseling sessions and supporting the inclusion of family-based counseling. With increased funding for mental health services in school districts and with a greater demand for mental health concerns in family systems (e.g., COVID-19, bullying, and school shootings), more trained school-based family counselors are needed. Counselor education programs should train their marriage and family students to work within the school context because these counselors would have the training and skill sets to understand and support multiple levels of individual, family, group, and community systems (Laundy, 2015). With the rise in the need for mental health services for children and the increase in juvenile offending, policies have focused on the functioning of the child and pretermitted to include the influence of the family system functioning on the child’s well-being (Scholte & Vander Ploeg, 2015). Furthermore, children’s social, emotional, and academic achievement could increase by creating policy changes that incorporate the family system. At the district and school level, administrators can support school-based, family counseling interventions by providing resources such as time and space for counseling sessions and incorporating family-based counseling into their response to intervention
In summary, the findings supported school-based family therapy for these students at Title I schools. School-based family counselors are well positioned to understand the complexities of school systems while connecting and supporting school counselors, teachers, administrators, social workers, and families to ensure school and family successes. The union of school-based mental health services and family therapy results in success for schools, children, and families. Future research could consider a larger sample size and include other student outcomes related to achievement, teacher ratings, and students’ perceptions of their counseling experiences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.