
Abstract
Anxiety has become ubiquitous in modern life, across countries. Cultural theories suggest that high uncertainty avoidance (UA) increases anxiety, while long-term orientation (LTO) decreases it. We question whether a high UA culture in a region attracts research and development (R&D) projects regarding anxiety management, compared to LTO. Furthermore, do these opposite dimensions moderate each other in attracting a pharmaceutical firm’s response? This article explores this link between the UA culture and the moderation effect of LTO. Using data on clinical trials related to anxiety management projects in 67 countries, we record 10,585 observations, capturing 4% of the global population of clinical trials on the subject. We find that the uncertainty avoidance index (UAI) shows a negative correlation with the intensity of the anxiety management project, while LTO has no significant correlation. The interaction between the two shows positive correlation. The results are found to be significant after controlling for confounding variables and robustness checks. This study makes three contributions. First, it highlights the link between culture and anxiety management projects through the clinical trial movement. Second, it contributes to cultural theory, suggesting that the UAI defines problems and LTO defines innovative solutions. It also highlights the differences and links between the UAI and LTO at the conceptual level. Thirdly, it offers general policy and practical implications.
Keywords
Introduction
Over the last 50 years, research in the fields of social sciences and humanities have suggested that national culture influences psychology, behavior, and environmental responses such as response to cultural consequences. In addition to other findings, national culture is perceived as a stable and useful tool to analyze uncertainty and anxiety (Minkov & Hofstede, 2014). Two cultural dimensions have attracted attention in entrepreneurship research and socio-economic development. One is the uncertainty avoidance index (UAI), and the other is long-term orientation (LTO). Existing literature on entrepreneurship shows that while a high UAI hampers the entrepreneurial activities in a country (Shane, 1993, p. 198), LTO increases the dimensions of entrepreneurial orientation (EO), namely, risk-taking, proactiveness, and innovativeness (Miller, 1983). Thus, both the UAI and LTO have different impacts on entrepreneurship theory and practice.
Furthermore, the implications of the UAI and LTO on socio-economic development differ. High uncertainty avoidance (UA) cultures show increased levels of anxiety, stress, and other mental health issues at the individual level, group level or society level (Hofstede, 2001); high LTO cultures show reduced anxiety because these cultures reflect control and discretion over the distal future (Bourdieu, 1963). The industry builds its assumptions and responds to the influence of national culture on society. For instance, national culture influences research and development (R&D) investment decisions (Lorca & de Andrés, 2019), determines the attention given to mental disorders (Heim et al., 2017; Hofmann et al., 2010), helps predict suicidal tendencies (Crowder & Kemmelmeier, 2017; Eshun, 1999), and dictates anxiety management activities (Cardemil, 2008; La Roche & Christopher, 2008). The extant literature reveals consistent support for culturally imprinted anxiety and decisions regarding its management (Hofmann et al., 2010). Thus, based on the fact that national culture predicts anxiety, researchers have developed technological solutions to manage anxiety in the population.
In this article, we investigate two questions overlooked by existing literature. First, does national culture attract the attention of the pharmaceutical sector to identify and locate clinical trial projects near high anxiety cultures based on high UAI? If so, how? Second, does the LTO culture influence the high UA culture and the location of clinical trial projects in the population? To answer these questions, we use empirical evidence to propose that the LTO culture moderates the effects of the UA culture on clinical trial projects for anxiety management. This proposition is built on two assumptions. First, the UA culture positively predicts anxiety (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014), but does not induce entrepreneurial risk-taking in the society of that country. Second, the high LTO culture induces risk-taking behavior, but is a reflection of anxiety in the population. Like R&D projects trail cancer diseases in some locations and diabetes diseases in others (Malik, 2019), anxiety attracts the attention of the pharmaceutical sector for clinical trials. The LTO complements the anxiety based on the risk-taking culture at that location. For instance, the LTO culture complements anxiety in the society in two alternative ways. On the one hand, it reduces anxiety based on increasing the control over the future. On the other hand, it increases risk-taking behavior in the society for entrepreneurship and new technology development, seeking new solutions to the anxiety problem. Since clinical trial experiments “travel” with human subjects (Malik, 2019), we trace this itinerary of clinical trials through the lenses of national culture and anxiety.
The combination of the national culture and the industry’s response to culturally imprinted anxiety (Hofmann et al., 2010) resolves a paradox. High UAI increases anxiety but decreases risk-taking for innovation; High LTO decreases anxiety, but increases risk-taking incentives and behavior for innovative technologies (Cardemil, 2008; La Roche & Christopher, 2008). Evidence shows that high UAI positively correlates with anxiety (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014), and it limits entrepreneurial orientation. Similarly, high LTO culture negatively correlates with anxiety, and it positively correlates with entrepreneurial orientation. Thus, it is essential to empirically analyze whether the interaction between UAI and LTO attracts or repels the introduction of clinical trials in a population (Cardemil, 2008; La Roche & Christopher, 2008). We attempt to fill this void in the literature.
This study suggests clinical trials as industrial decisions to solve the phenomenon of anxiety. Given the positive correlation between high UAI culture and clinical trials of anxiety management, we proceed to show the negative correlation between high LTO culture and the clinical trials of anxiety management. We then predict a moderation between opposite sides of the framework, as proposed below. Thus, we contribute to cultural moderation and contingencies in decision processes across levels and contexts.
The next section provides the theoretical framework. This is followed by the methodology in the third section, and a presentation of our results in the fourth section. The fifth section discusses the findings, as well as the implications and limitations of the study.
Framework
Culturally Imprinted Anxiety
Anxiety is a psychological state that is a manifestation of a person’s emotional response to a situation in the environment (Lazarus, 1993). The Encyclopaedia of Psychology (Kazdin, 2000) and the American Psychological Association (APA) define anxiety as “an emotion characterized by feelings of tension, worried thoughts and physical changes like increased blood pressure. People with anxiety disorders usually have recurring intrusive thoughts or concerns. They may avoid certain situations out of worry” (APA, 2019). They suggest the various causes of anxiety across cultures, highlighting the different visible and invisible societal implications, and the necessity to manage culturally imprinted anxiety.
National culture contributes to anxiety in subtle ways (Hofmann et al., 2010). While national culture has a direct influence on attitude and behavior, it has an indirect effect on genes and their response to the cultural environment (Reiss et al., 2013). An individual’s genes influence their responses to the environment internally, while a culturally imprinted situation, the inferred meaning, and planned responses influence genetic capabilities an external reaction to the situation. Both biological and sociological transitions play subtle roles in the interaction between genes and the social environment (Malik, 2019). One the one hand, the external environment (i.e., language, culture, religion, and other social situations) influences cognitive structure at the physical level over a prolonged period. On the other hand, a physical change impacts cognitive development at the conceptual and perceptual levels (APA, 2019). The interaction between genes and culture suggests that the concept of honesty triggers responses in different parts of the brain among the Chinese and American population in experimental studies (APA, 2019).
Over the decades, the link between national culture and anxiety has become evident (Ratner, 2000). In addition to the direct impact of national culture on anxiety, indirect examples also reflect the link between national culture and anxiety. For instance, national culture influences eating habits and socializing (Malik, 2019). Excessive eating can lead to obesity, which translates into anxiety. Similarly, excessive drinking leads to other psychological and mental hazards (Venuleo et al., 2015). While these cultural mechanisms play a significant role in the development of anxiety, their role in the expression and direction of anxiety varies based on the stigma attached to anxiety in a population (Heim et al., 2017). Since high anxiety brings about physical changes to mental development (APA, 2019), it results in an unhealthy outcome, leads to bad decisions, and accumulates harmful outcomes (Eshun, 1999). Thus, the extant literature has addressed the issue of anxiety as an emic (contextual) versus etic (universal) phenomenon.
However, the link between the national culture and anxiety has raised questions on how anxiety has developed across diverse cultural contexts. One explanation suggests that the conceptual logic and perceptual experience differ, and this gap between the two (concept and perceptions) induces anxiety (Whitson & Galinsky, 2008). The concept-perception gap is reflected in structural paths associated with symbols and memory, which represent reality and truth, respectively. These conceptual ideas have shared views on reality within a population and varies across cultures. In contrast, perceptual ideas reflect experience. This conflict between the conceptual history and perceptual situation create differences in meaning, leading to uncertainty and pressure—it translates into the anxiety and stress of the population (APA, 2019). Therefore, scholars of cross-cultural studies analyze the cultural perspective because it decodes the meaning of the experience in a situation.
Cross-cultural theories assume national culture as a stable, reliable, and concrete phenomenon associated with psychological issues (Hofstede & McCrae, 2014). Cross-cultural studies reflect on the differences in the interpretation of the situation, the development of uncertainty, and the management of pressure associated with uncertainty. Cultural research theories purport that national cultures vary on uncertainty avoidance, and high uncertainty avoidance leads to high anxiety. This means that high uncertainty avoidance cultures show high anxiety and stress. Empirical evidence supports these theories and links uncertainty avoidance to anxiety in the population. Heim et al. (2017) explain cultural variations and anxiety disorder among different regions. Similarly, cultural theories explain that similar situations of anxiety may attract different anxiety management responses in scale, due to cultural variations across regions (Cardemil, 2008; Crowder & Kemmelmeier, 2017; La Roche & Christopher, 2008). Thus, a high UAI culture gives cues to firms for anxiety management in that region.
Uncertainty Avoidance and Anxiety Management Projects
Cultural theories contend that UA creates anxiety, and pharmaceutical enterprises trace regions where such anxiety exists. The presence of a high UAI helps them trace the relevant regions for their clinical trial projects. The notion of uncertainty has a long history, and most authors in social sciences concur that uncertainty and anxiety provide cues about the society and its behavior. For instance, high anxiety regions attract management projects in response to the population’s behavior to uncertain situations. Natural disasters raise different anxiety levels across regions with cultural differences. Thus, there is consensus on the issue of uncertainty and anxiety. However, the confusion arises on account of the fact that the issues of uncertainty and risk are not the same (Hofstede, 2001).
Knight (1921) clarified uncertainty to differentiate it from risk. Uncertainty is about unknown and unstructured situations, which surprise actors in uncertain conditions. It is different from the unsurprising nature of the risk phenomenon as risk is about known thoughts and their structures. While uncertainty presents an unstructured situation, risk presents a structured situation. Hofstede and McCrae (2014) explain that unlike risk, UA is a psychological response to an ambiguous situation. Referring to Knightian uncertainty (Knight, 1921), we can differentiate and draw a link between the two. Risk has probabilities, uncertainty has no probabilities. As soon as we assign probabilities to uncertainty, it becomes risk (Hofstede & McCrae, 2014; Rossberger & Krause, 2014). Therefore, uncertainty reflects on anxiety, and risk might be a consequence of anxiety.
This idea of uncertainty supports the cross-cultural theory on the UAI dimension, which we translate as the anxiety index for the empirical analysis. Cross-culture research explains that UA correlates with the tolerance for ambiguities in response to an unstructured situation (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014). High UAI cultures reflect low tolerance for ambiguities and uncertainty, compared to low UAI cultures. This means that in contrast to low UAI cultures, high UAI cultures show high level of emotion, stress, and unease toward the situation at hand. Moreover, high anxiety induces an agitated attitude and aggressive behavior (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014). As a consequence, firms draw cues from the culture of that society to make entry decision in the concerned region for their clinical trial projects, to target the prevalence of anxiety in the population.
The culturally imprinted anxiety in regions with high UA cultures attracts firms and universities to develop new products, similar to the way certain diseases provide cues for firms to target them (Hofmann et al., 2010). Diseases such as cancer and diabetes emerge due to the habits of society, and partially from the genetic structure of society. The cultural dimension of society attracts the firm’s attention to engage in a clinical trial to target cancer or diabetes in the region (Malik, 2019). More recently, the COVID-19 (coronavirus disease) pandemic has specific cultural and regional links with respect to its causes and consequences. First, it traces its roots partially to cultural habits. Furthermore, we see that culture explains its management. While Asian countries used strict controlling measures; the United States of America (USA) used lenient controls on pandemic management. As a consequence of the pandemic, the pharmaceutical industry has shown increased dynamics.
In the early stages of the spread of COVID-19, the prices of stocks of pharmaceutical products and facemask-producing firms increased by their maximum limit in January 2020, after COVID-19 hit Wuhan. Approximately 6 months later, there are nearly 80 candidates for clinical trials globally, where the virus persists. Moreover, media houses share news and anecdotes regarding the anxiety prevalent among different cultures because of the lockdown measures in their regions. Since pharmaceutical firms and universities engage in anxiety management projects (i.e., clinical trials on anxiety management), we expect to see new itineraries of clinical trials in the world. Thus, we state our hypothesis based on assumptions regarding the UAI-specific driven clinical trial projects.
Long-Term Orientation and Anxiety Management Projects
Contrary to the UAI, which indicates increased anxiety and predicts itinerary of clinical trials that travel to the high anxiety UA regions, high LTO suggests a decrease in the anxiety followed by a decrease in the anxiety projects. The cultural theory explains that LTO refers to an increase or expansion in the time perspective of an individual in society, thereby enhancing perseverance (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014). The LTO perspective of society lengthens the experience of positive attitude on the timeline into the distal future. The LTO assumption primarily deals with the perceived control over the future, coping potential, and high expectations (Malik & Zhao, 2013). For instance, some cultures consider the future a destiny while other cultures consider it a measurement tool (Bourdieu, 1963). Those who consider it a destiny assume a low control over the future, and those who consider the future a tool of opportunity assume a high control over their futures (Bourdieu, 1963). Unlike the mechanical notion of time, the socially structural notion of time, its rhythm, and its pace differ among societies. Evidence shows that the experience of time matters in shaping anxiety disorders (Lengen et al., 2019), and the experience differs across cultures (Christie & Halpern, 1990). Therefore, the social time in socio-psychological contexts determines the contextual influence on the LTO throughout history.
Historically, Weber (1978) describes time in a social context, suggesting that time has different meanings across structures and cultures of societies (Weber, 1978). Similarly, Bourdieu (1963) addresses the social context of time by comparing the attitudes of a group in the past versus the future (Bourdieu, 1963). Recent scholars of cross-cultural studies show that reinforcing and enduring the past and future differ between societies who take control of time and those who surrender to the meaning and power of time (Whitson & Galinsky, 2008). In contemporary research on the intercultural differences of time (Hofstede & McCrae, 2014), scholars suggest the culturally imprinted meaning and value of time and decisions (Lengen et al., 2019). High LTO cultures take control of time, whereas low LTO cultures surrender to the force of time (Whitson & Galinsky, 2008). Furthermore, high LTO cultures tolerate contradictory logics while low LTO cultures repel the same (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014).
National scientists have acknowledged the cross-cultural values of time in recent understanding. The late physicist, Stephen Hawking (1988, p. 162) refers to the perception of time that has changed from a singular dimension to multiple dimensions. He explains that the variation in the conceptual and perceptual dimensions of time, and abandons the idea of universal time (Hawking, 1988). From a socio-cultural perspective, the notion of time signals complex societies, their long-term strategies, their interpretative stability, and the future value judgment for their forecasts (Bourdieu, 1963). In short, high LTO cultures show increased control and confidence, thereby showing reduced levels of anxiety of the population (Pagnini et al., 2016). At the same time, it results in risk-taking behavior in entrepreneurial activities. Low LTO cultures, on the other hand, increase anxiety in the population (McGoey, 2010), but lack the entrepreneurial spirit to induce clinical trials. In comparison to short-term orientation, since LTO influences interpretation, meaning, values, confidence, coping potential, and response, we predict the following hypothesis.
LTO Moderates UAI
LTO moderates the effects of UA on attracting clinical trials in the country. Multiple mechanisms link the moderating effects of LTO on the UAI. Firstly, uncertainty-avoidance differs from risk-avoidance, and they can move in opposite directions. For instance, a high UAI culture can take high risks in a critical decision. Hofstede 1 explains that drivers from high UA cultures prefer high-speed cars and tend to drive faster than those from low UA cultures. In so doing, they risk their lives, knowing that the speed might kill them. Further anxiety may result as a consequence of such risks. Similarly, high UA cultures tend to use alcohol with known risks. In other words, UA induces risk-taking in practice, which worsens the anxiety rather than resolves it.
Secondly, high UAI introduces the problem of anxiety in society, while LTO introduces EO to arrive at innovative solutions. High LTO cultures invest in future development, enabling conducive conditions for innovation. Clinical trial projects are expensive, lengthy, and conduct future-oriented activities in the industrial setting. This enduring investment, such as the stable supply of volunteers, consistent societal consent, technical support of partners, and cooperative structures of national institutions, are based on a high LTO culture. Thirdly, the EO induces risk-taking in the LTO (Miller, 1983), and, anxiety oriented risk-taking behavior reflects on the UAI. Both types of risk-taking behaviors have different roots and implications. Therefore, we conclude that high UAI generates problems, and high LTO generates solutions.
As a problem generating mechanism, the UAI increases clinical trial attention around the world (Malik, 2019). As noted earlier, the culturally imprinted anxiety directs us to the cultural location (Hofmann et al., 2010). Table 1 shows high UAI versus low LTO, or low UAI versus high LTO. Our focus is on high UAI and high LTO. Given that high UA culture increases the desire to reduce uncertainty in the country (Hofstede & McCrae, 2014; Minkov & Hofstede, 2014), and the LTO culture provides solutions through clinical trials on anxiety management (Lorca & de Andrés, 2019), then we hypothesize as follows.
Framework Topology.
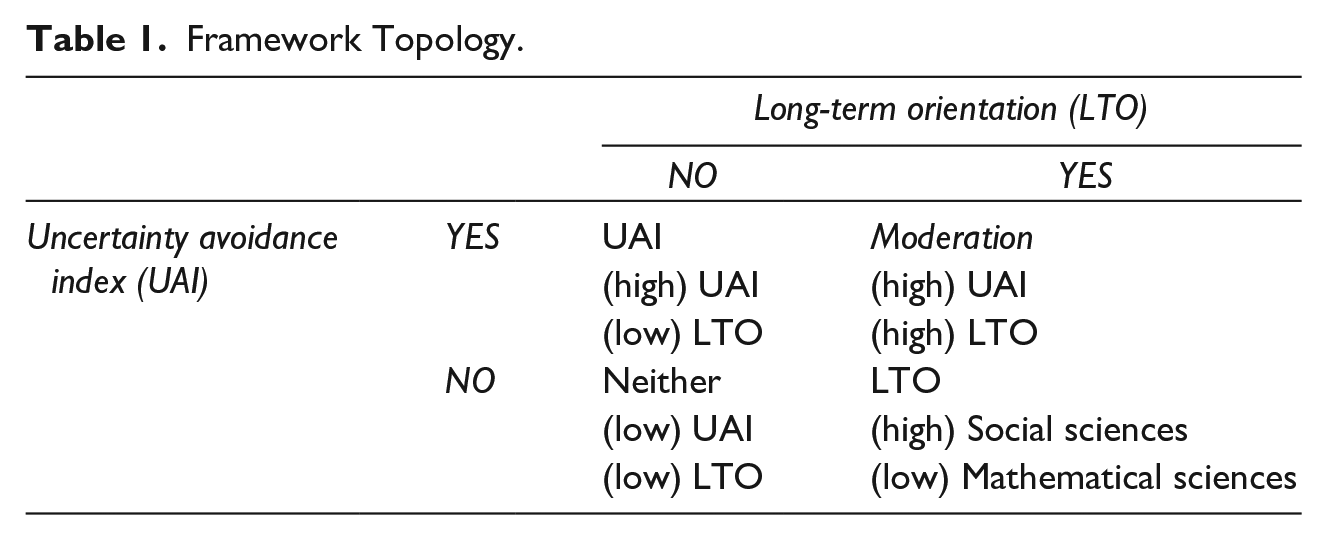
Table 1 shows four combinations of UAI and LTO. In this 2 × 2 matrix, the high UAI or high LTO alone is not sufficient. Instead, to meet the moderation condition, both need to be high to establish trails of clinical trials. The interactive position (high UAI and LTO) meets the necessary and sufficient conditions for analysis in this framework.
Figure 1 further elaborates this in the conceptual model. The left side shows multiple types of clinical trial sponsors. These sponsors include firms, universities, and foundations engaged in research and development activities internally or external via strategic alliances (Malik & Zhao, 2013). The right side shows a direct link between the UAI and anxiety clinical trials. The lower link shows the moderating roles of the LTO (interaction). The interaction between the two types of cultural measures shows a positive prediction, and thus the LTO is seen to have moderating effects on the UAI.

Conceptual model.
Methods
We see that culturally imprinted anxiety exists (Hofmann et al., 2010), attracting psychotherapy and drug therapy for anxiety management in the targeted population (Kazdin, 2000). Clinical trials in response to anxiety have emerged as a concerted solution to anxiety management (APA, 2019). The APA (2019) contends that “even though countless studies show that psychotherapy helps people living with depression and anxiety, drug therapy has become the most popular course of treatment over the past decade.” As a result, pharmaceutical firms engage in both types of therapies through clinical trial projects in the targeted population (Cardemil, 2008; Deaton & Cartwright, 2018; La Roche & Christopher, 2008). Hence, we combine clinical trials of both types of therapies into anxiety management projects of interest in the country, as a percentage of the clinical trial projects in that country.
In the anxiety management projects for new product development, multiple types of organizations engage to develop innovative technologies to solve anxiety and depression in the population. These organizations include universities, firms, hospitals, charities, and public agencies. Pharmaceutical firms dominate the industry, and universities often follow them in wholly owned or collaborative projects. Similarly, funding bodies vary from private financiers, to public financiers and global financiers. Among the public financiers, the federal governments, such as that of the USA, fund some projects more than others. In recent financing events, the Chinese government has allocated more than 10 billion dollars, Alibaba corporation has also allocated funding for R&D projects to target COVID-19, and the World Health Organization (WHO) has contributed in different ways to deal with this critical issue in the world. Foundations and charities are other sources of funding for targeted projects across regions, since they deal with several types of morbidities and solutions.
Anxiety management projects include two types of new product development. The first form of product development relates to psychotherapy of various forms of contents and deliveries. For instance, music therapy to manage anxiety is one set of technologies, and spirituality is another set of tools for the management of anxiety (Kogan et al., 2013). The second form of new product development refers to drug therapy as a commonly used technology across regions (Kazdin, 2000). Although psychotherapy has shown benefits that manage anxiety, the firm responds predominantly using drug therapy, and the response of clinical trial projects to the anxiety of the nation reflects drug therapy. Sometimes the two types of therapy are combined to deal with the population’s anxiety. Based on a clinical trial to treat anxiety using new product development across cultures, we used data from the National Institutes of Health (NIH) which maintains that all clinical trials are to be approved by the Food and Drug Administration (FDA) of the USA. 2
To gather the relevant data for our analysis, we first retrieved all clinical trial projects from the NIH’s database (from the 1990s to 2013). Appendix A shows the temporal patterns of core anxiety projects over the years, from 1999 to 2019. Because we gathered our data in 2013 and began the coding and analysis process after such time, our sample includes data before 2014 and the population of all anxiety projects. Appendix A shows the trends in subsequent years, showing a steep increase. Our analysis represents the sample before 2014 as the refined data on anxiety projects as a proportion of the total clinical trials at the national and organizational levels. The national-level projects of clinical trials capture the capacity and capability of the country as a whole, and the organizational level projects represent the firm’s capacity. Therefore, the proportion of anxiety in the total clinical trial projects helps establish the link between culturally imprinted anxiety and the firm’s response.
Appendix B shows anxiety as the central concept and its components as its parts. The sum of these constituents makes up 10,586 anxiety projects among the total population of clinical trials in the world which stood at 267,774 until 2013. Thus, the anxiety management clinical trial projects make up 4% of the entire population of the clinical trials. Some of the projects among this 4% of projects had a higher intensity compared to other projects. For instance, if the project with multiple terms on anxiety, it implies a higher level of anxiety management activity compared to a project with a signal reference to anxiety in the clinical trial activity. This means that the high-intensity projects reduced the proportion of non-anxiety projects, in contrast to the low-intensity projects that reduce the proportion of anxiety projects. Taking two assumptions from the earlier discussion which states that clinical trials shadow the subject of interest (Malik, 2019), and that the culturally imprinted anxiety provides cues to the industry (Hofmann et al., 2010), we linked anxiety projects to national cultures of the countries in the sample.
Appendix C shows the proportion of anxiety-related clinical trial projects across countries as a cultural representation. The USA hosts about 46% of the total R&D activity in global anxiety management clinical trial projects. The rest of the world has about 54% of the active projects on anxiety management clinical trials. After the US, France, the United Kingdom (UK), Canada, Israel, Spain, Germany, and China began their anxiety-related project development. We believe that two reasons explain these trends. First, the developed countries sponsor most clinical trial projects in the world because of their ability and willingness to engage in such ventures. Among them, the USA leads in capability and willingness. Second, these countries have engaged in military conflicts in the last decades, which has resulted in high anxiety related to the conflict and its implications on the society, for those who have returned and retired. Once again, the USA leads in this trend.
After linking projects to their countries and regions, we divided the financiers in our sample into universities, industries, public institutions, and federal governments. The institutional interaction among technological activities, firms, and public agencies make these technological projects possible (Nelson, 2005). These financiers differ in their share of anxiety management clinical trial projects. Similarly, the direct sponsoring of the core technology varies among different actors. Universities sponsor 68% of the sample, firms sponsor 26%, national institutes sponsor 21%, and federal governments 8%. These sponsors collaborate in some projects and compete in others, and they contribute various types of financial, intellectual, and social capital.
We then explored organization-specific projects, which act as a direct sponsor or co-sponsor of the clinical trial project. Appendix D shows the plotted map of these organizations. Although there are thousands of sponsors (varying in types and sizes), we selected the top 11.8% of 1,035 organizations to fit in the space of the chart. The x-axis shows the alphabetical position of the organization, and the y-axis shows the size of the sponsored project of this organization. Thus, the horizontal map shows similarities, and the vertical map shows differences in strength of the anxiety management projects.
Variables
Dependent variable: The dependent variable refers to the intensity of the anxiety management conditions in the clinical trial project. It measures the proportion of anxiety-based medical conditions in the clinical trial project. Appendix B shows the list of anxiety-based medical conditions in the sampled project. The APA (2019) includes these terms as different categories or levels of anxiety. Although the sample consists of all psychological issues associated with anxiety, stress and depression related clinical trials, and multiple other conditions such as causes, or correlates of anxiety conditions, enter the clinical trial project. For instance, cancer patients face anxiety differently because of cultural differences. Similarly, cultural differences reflect on alcoholism and eating disorders as responses to anxiety. Thus, we divided the count of anxiety conditions by the total conditions in the clinical trial to obtain the ratio (anxiety/sum), measuring the intensity of anxiety conditions in the project.
Independent Variables
○ Uncertainty avoidance (UAI)
○ Long-term orientation (LTO)
○ Interaction variable (UAI * LTO) shows the product of two main variables centered to their means.
The interaction effect of two continuous variables can occur in two forms, namely, exponential and antagonistic. The exponential interaction effect occurs when lines show similar direction but different steepness levels. Antagonistic interaction occurs when two lines cross each other. Figure 2 shows the antagonistic type of interaction effect. If the two lines were parallel, it would indicate that no interaction effect occurs between the two independent variables (UAI and LTO). If the two lines indicate different steepness, it would imply exponential interaction.

Anxiety projects versus UAI when LTO is 20, 40, and 60.
Three groups show distinct levels of LTO. The dotted line shows the group with 0 LTO. In this group, the UA culture shows declining attention to clinical trials. The middle group shows 50 levels of LTO. This middle line shows an increased attention to clinical trials. The highest group shows 100 LTO, which is an upwards trend. This group of countries increases the attention to clinical trials when they have a high anxiety and a high risk-taking attitude toward innovations.
Control Variables
Appendix E lists control variables, their definitions, rationales. The measures of these variables appear in the summary table in the results section. The preview of these variables in the appendix table reduces redundancies.
Analysis
Because our dependent variable is a count variable, we used two models: the ordinary less square (OLS) and Poisson. Both analyses produced similar results; therefore, we chose the OLS for the reporting of the findings for simplicity, clarity, efficiency, and brevity. The following expression shows the model.

The model shows Y as the outcome,
The interaction between continuous variables raises challenges in interpretation, thereby limiting the use of such interactions in social sciences (Cohen et al., 2002). Adding the main effect and interaction effects, the regression coefficients for X1 and X2 condition with each other. Since B1 is the effect of X1, and B2 of X2, if we consider the effects of either alone, then the effects of the other = 0. For instance, the UAI’s effect B1 occurred on Y, when LTO = 0, and LTO’s effect occurred on Y when UAI = 0. Thus, to know what the value of the UAI on Y, we need to keep the LTO’s effect X2 constant. In other words, it depends on the value of LTO. For the most reliable effects, we centered the two variables before developing their interaction variable (Cohen et al., 2002). We obtained this interaction variable in two steps by first estimating their means, and then subtracting the mean from the main variable. Centring the variables before interaction means that the intercept is the predicted Y score for an average subject or unit of analysis.
Furthermore, the analysis of the interaction effect requires the inclusion of the main effects and interaction effects, irrespective of the significance of the main effects (Cohen et al., 2002). The absence of the main effect complicates the results.
Robustness Test
To test the robustness, we first used the heteroscedasticity test and found f-statistics (8.09, p < .001) for 29 degrees of freedom. Second, we used weighted average methods, with multiple trials as the denominator [aw = 1/pdi^2, and pdi^.5], and we found that the f-statistics increased (9.30, p < .001). However, the significant p-value suggested heteroscedasticity, implying the need for other solutions. Third, existing literature on the issue guided us through two methods, namely the robust errors estimation method and the multilevel (mixed) method. The latter uses level 1 (organization) and level 2 (project). We compared four methods that is, the OLS, the sum of weights, robust errors, and multilevel (mixed) methods.
The robust standard errors estimation method produced unbiased standard errors of OLS coefficients under heteroscedasticity, while the multilevel model has fixed effects and random effects. The fixed-effects part acts as the standard regression coefficients. The random-effects model shows random intercepts (random coefficients), based on multiple levels of nested groups. Because of their nested levels, these multilevel models and fixed-effects models are used interchangeably in the literature. Hence, our results appear robust with respect to comparative models and assumptions used.
Results
Table 2 shows summary statistics. The higher ratio (anxiety/sum) of the dependent variable implies a high intensity of the anxiety project. The range shows 1 to 1 (50/50 proportion of anxiety project and non-anxiety project). The maximum in the range is 4 (1 being the condition of non-anxiety and 4 being anxiety). The summary shows the means and ranges of the remaining control variables. Appendix E defines and rationalizes these control variables to complement the summary table.
Descriptive Statistics.
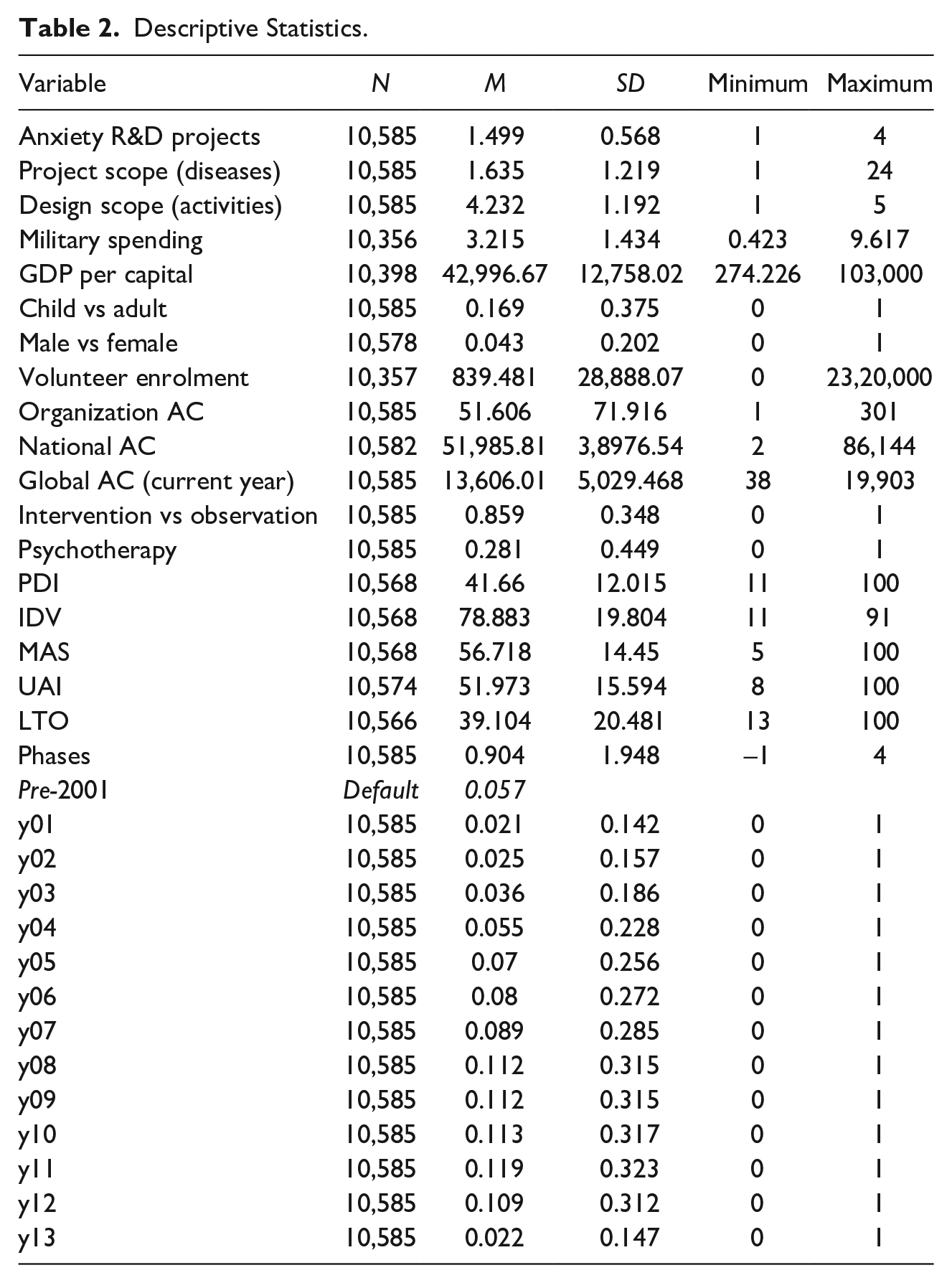
Table 3 shows inter-variable correlations. The correlations between independent variables serve two purposes, that is, it shows the expected direction of the correlation and the size of the correlation. The direction indicates preliminary support for the assumptions, and the effect size indicates multicollinearity. The correlation of the UAI and LTO are negative and significant, and their small effect sizes do not violate the collinearity assumption.
Inter-Variable Correlations.
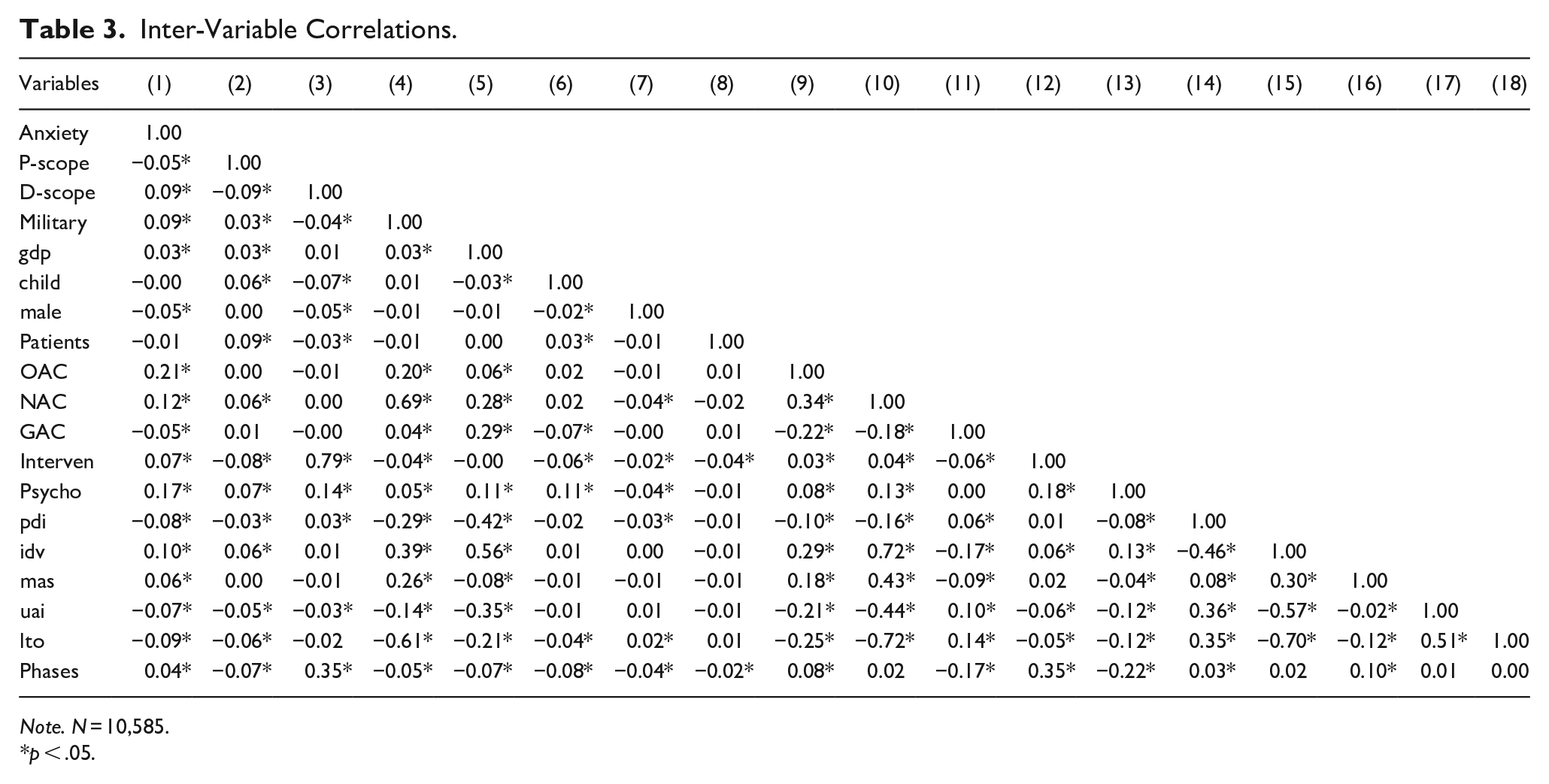
Note. N = 10,585.
p < .05.
Table 4 shows the variance inflation factor (VIF). The convention suggests that above the threshold of VIF = 10 raises issues of multicollinearity, and the accepted rule of thumb in social sciences is below that threshold. The highest VIF is 6.9, and the average is 2.4. To manage these values further, we centralized the focal variables such as the UAI and LTO to meet the rule of thumb assumption for the threshold values. Based on these variables and their VIF values, we conduct the regression analysis for the central proposition, that is the complementary relationship between high UAI and LTO moderation.
Variance Inflation Factor.

Table 5 shows the direct effects of the UAI and LTO on the entry of clinical trial projects into the country. M1 shows control variables excluding cultural variables. M2 introduces PDI (power distance index), IDV (individualism-collectivism index), and MAS (masculinity-femininity index) as control variables. The first two dimensions (PDI and IDV) show a positive correlation with anxiety-related clinical trials. However, the third controlled dimension (MAS) shows a negative correlation, before the main variables, UAI and LTO are entered in sequence. M3 introduces UAI into the regression, and the coefficient is negative and significant (0.0001, p < .001). M3 introduces LTO in the regression; the coefficient is not significant (p < .05). Therefore, at this point, the high UAI culture discourages anxiety projects, and LTO does not matter.
Regression Results of Direct Effects (Robust Error Estimation Method).
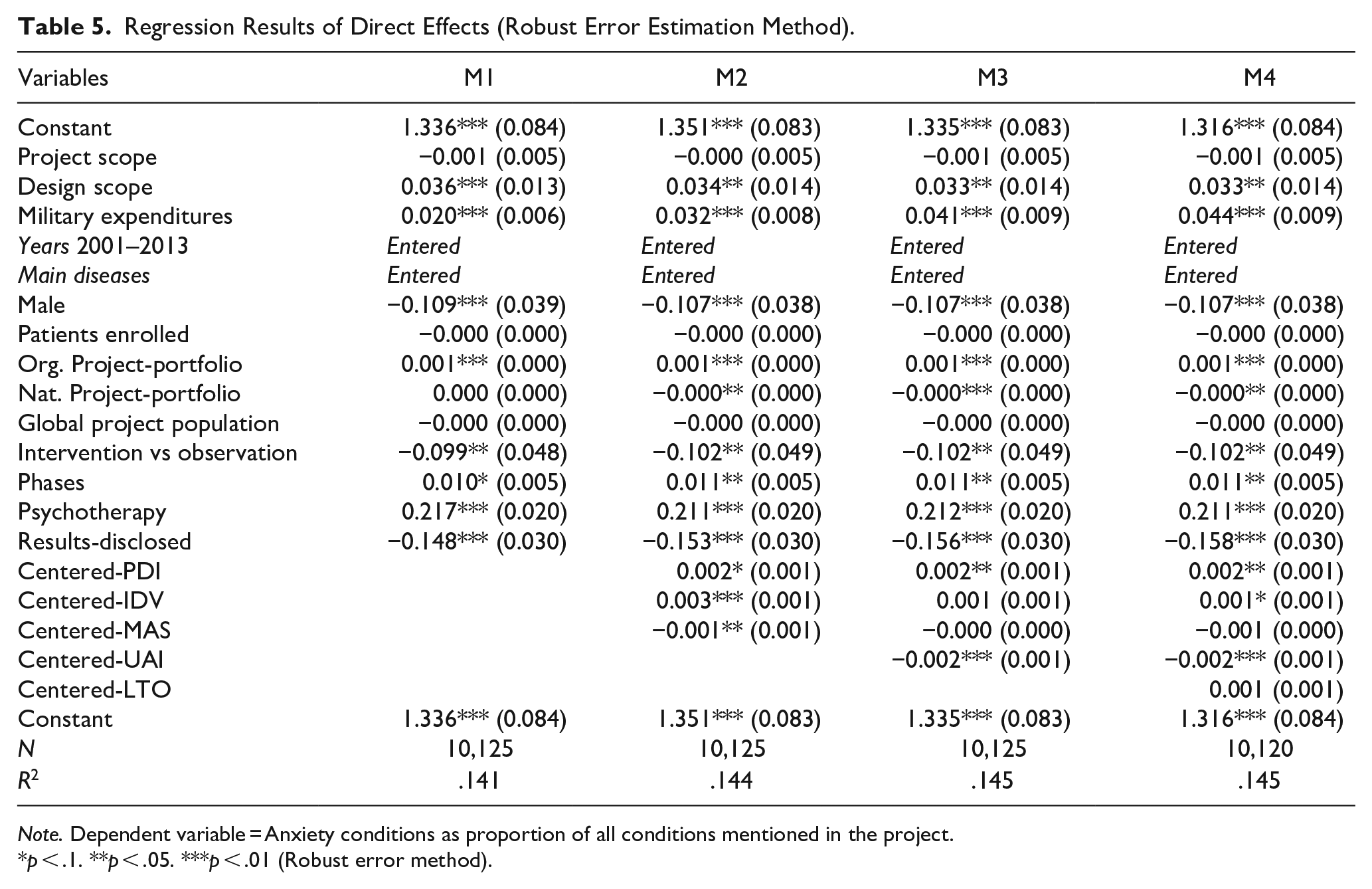
Note. Dependent variable = Anxiety conditions as proportion of all conditions mentioned in the project.
p < .1. **p < .05. ***p < .01 (Robust error method).
Table 6 shows the moderation (interaction effects) in four different techniques. M1 uses OLS (ordinary least squares) regression. The coefficient of interaction between the UAI and LTO is become positive and significant as we move from the direct effects to moderation effects. The net effects of the UAI are negative, and LTO is not significant. M2 shows the sum of the weighted method (aw = 1/PDI^2), and the moderation effect shows a result similar to that in M1. We use the robust errors method in M3, and show the results of the interaction in M1 and M2. Finally, we use a multilevel mode for fixed and random effects at the project and firm levels. The fixed-effect estimates show β0 = 1.43 and β1 = 0.0001. The random effect estimates at id (organization) indicates the variance-covariance matrix—the variance is −1.4001 with a standard error (0.0391). The results of the interaction match with the previous three models, deeming the analysis and results as robust.
Interaction Effect (UAI and LTO).

Note. Dependent variable = Anxiety conditions as proportion of all conditions mentioned in the project.
p < .1. **p < .05. ***p < .01.
Discussion
Anxiety and stress have become ubiquitous socio-psychological issues across countries and regions, attracting different explanations (causes) and management approaches (treatment). In the past, cognitive, behavioral, and neuroscience approaches explained the causes and management of anxiety; recent developments indicate the link between socio-cultural norms and mental issues (Brinkmann, 2016). They explain that culture affects and reflects genes, suggesting a moderation between both sides (Reiss et al., 2013). For instance, differences across cultures explain the varying degrees of suicides that can be attributed to the cultural pressures of maintaining honor and reputation in society (Crowder & Kemmelmeier, 2017). Similarly, empirical evidence-based therapy such as clinical trials (La Roche & Christopher, 2008) show that cultural differences influence the management of anxiety in society. These developments on cross-cultural studies clearly link national cultures and emotions through mechanisms of social activities and cultural concepts (Ratner, 2000). However, they do not explore whether national cultures, which link uncertainty avoidance and long-term orientation to anxiety, attract clinical trials from firms. In other words, does the clinical trial itinerary trails the person of interest?
In this article, we linked the proportion of clinical trials that target anxiety management as a proportion of the overall clinical trials in the country, to three measures of national culture, namely, UAI, LTO, and the interaction between them. Given that high UAI and LTO indicate different influences on the anxiety of the population (Hofstede & McCrae, 2014), we built our analysis on their moderation effects. Institutional theory supports the idea of co-moderation between national culture and policy, which implies that cultural structure influences action, and action produces new structures at the national level in the economy (North, 2005). Similarly, national culture and technological development affect and reflect each other in the same way that culture and psychology (anxiety) reflect each other (Dulin, 2011). This implies that national cultural dimensions moderate each other, just as genes and the environment moderate each other (Reiss et al., 2013). Uncertainty and anxiety correlate in the same path (APA, 2019). In this article, we propose that the UAI is positively correlated with clinical trial projects for anxiety management in the region, provided that the national culture also shows LTO.
The empirical evidence from the population of clinical trial projects on anxiety as a proportion of the total population from clinical trial projects in 67 countries supports that the high UAI and LTO co-moderate each other in attracting clinical trials for anxiety management. Prior literature explicitly or implicitly assert that clinical trial projects shadow the person of interest in the culture-specific population in the region (Cardemil, 2008; Deaton & Cartwright, 2018; La Roche & Christopher, 2008). A statistical analysis of 10,000 clinical trials reassert the moderation between the UAI and LTO in the anxiety projects, contributing to both cultural psychology and coevolution between institutions. We see that national culture is directly linked to the source and management of a medical problem. The causes and disclosure of the recent virus in China has roots in cultural practices, thereby presenting a clear link between the source and management of the issue. Furthermore, national culture explains why some R&D projects enter one location more than others (Cardemil, 2008; La Roche & Christopher, 2008). The co-moderation effect between the UAI cultures and LTO cultures combines two different logics (Heim et al., 2017). UA predicts national morbidities such as cancer and diabetes (Malik, 2019), while long-term orientation predicts the attitude toward those morbidities.
Multiple mechanisms which act as social processes lie between national culture and anxiety. Several studies have use these mechanisms to explain inter-institutional interaction between sectors and industries (Raybeck, 1998). First, reputation and honor exert pressure on individuals, resulting in the emotional response of anxiety and sometimes suicide (Crowder & Kemmelmeier, 2017). Second, cultural activities and concepts create contexts which produce emotions, leading to different implications (Lazarus, 1993). Third, evidence increasingly links social activities in the culture to mental disorder, suggesting that physical or cultural dimensions alone cannot explain the intricacies of anxiety and its management (Brinkmann, 2016). Last, the cultural implications extend beyond the prediction of anxiety and its management. For instance, national culture leads to the formulation of therapies for the treatment of disease (Ratner, 2000) and influences empirical treatments (La Roche & Christopher, 2008).
The current study considers that cultural anxiety acts as a cue that the firm draws from the population, to consider entering a region and deal with the management of anxiety. First, this study implies that the firm responds to high UA culture while engaging in anxiety management projects. Second, UA is the first cue that generates meaning for the firms, when the LTO exits to complement it. Regarding the first implication, our findings refute a group of studies which deny the role of socio-economic factors in anxiety development across cultures (Baskin, 1982). Instead, we find that socio-economic factors (such as GDP and military-related insecurity) show significant correlation with national anxiety projects. With respect to the second implication, our study complements prior studies that link culture to alcohol hazards (Venuleo et al., 2015), suicide risks (Eshun, 1999), and anxiety (Heim et al., 2017). In addition to linking national culture to anxiety management practices (Barber, 2011), we show some of the underlying causal mechanisms between culture and innovative projects for the anxiety management (Bukowski & Rudnicki, 2019).
Furthermore, the current empirical evidence combines two contradictory propositions in a specific context to draw theoretical and practical implications. Theoretically, it aligns with the prior literature, consistently supporting the direct and indirect roles of the UAI and LTO across contexts (Hofstede & McCrae, 2014). While a high UAI signals the existence and persistence of anxiety, increasing the need for entry of clinical trial projects in the market for the concerned population, the cultural propensity to tolerate long-term projects in the population of the region motivates these sponsors to make potential decisions to locate the clinical trial projects. It may be noted that a clinical trial takes 15 years on an average, has a high cost, and a low success rate. The regional LTO underpins the decision of the pharmaceutical firm and university to engage in anxiety management projects. Thus, the UAI and LTO co-moderate, complementing the contradictory logic wherein each of them alone meets the necessary condition, but not a sufficient condition.
At a practical level, national-level policy needs to develop the institutional infrastructure that can accommodate long-term strategies, tolerance to uncertainty, and lengthy projects. In order to make decisions for their clinical trial projects, firms and universities need to focus on the contradictory logic of the region rather than coherence between them. The public needs to understand that culture has both direct and indirect lasting impacts on their lives. Reminding themselves of their attitude and natural behavior to things may improve their lives, as opposed to the belief in destiny and faith. Thus, multiple stakeholders may benefit from the uncertainty of the direct effects and moderation of national cultural dimensions on anxiety and its management.
We list several limitations. First, this study focuses on cultural variables, but not on the situations. For instance, PTSD (post-traumatic stress disorder) in military conflicts reflects different behavioral responses. The USA handle the responses to conflict differently, compared to other developing countries engaged in similar situations, due to a difference in their political, economic, and technological capability. Second, the data limits the scope of the study scope to clinical trial projects registered with the NIH. Third, the situation-specific responses of society differ. For instance, when Singapore announced COVID-19 as an “orange-level” threat, rice from retail stores disappeared the next day, because people rushed to purchase and hoard for the future. This continued until the government introduced rules to prevent it. Our study does not capture such behavioral patterns in the culture. Fourth, the study introduced some general control variables such as types of sponsors, types of technologies, stages in the development and types of volunteers but left out many others. Last, the quantitative analysis supports a proposed link, but a qualitative understanding is required to rationalize the links between culturally imprinted anxiety and the firm’s response.
For future research, we draw the attention of scholars of national culture to three main points. First, the interaction of the UAI and LTO offers insights as a problem-solution context. While the UAI defines the problem of anxiety and stress, the LTO defines the solution. Clinical trials require continued investment, a stable supply of volunteers, consistent societal consent, technical support of partners, and cooperative structures. In contrast to a separate analysis of the UAI and LTO dimensions, we propose an interactive analysis. Second, the moderation hypothesis clarifies that uncertainty and risk confusion are not the same.
On the one hand, high UAI induces risk-taking. For example, drivers from high UAI cultures tend to take the risk on their lives by speed-driving the road. On the other hand, the LTO induces risk-taking in investments for discoveries and innovation. Like LTO, the EO argument in entrepreneurship builds on the risk-taking assumption (Miller, 1983). Both the risk-taking in driving and risk-taking in innovation decision precede the notion of uncertainty and response to the notion of uncertainty. This point alludes to multiple avenues for future research across contexts.
Third, the interaction between the UAI and LTO are relevant in the selection of therapy and the organizational selection for anxiety management. Two therapies are prevalent, namely, psychotherapy and drug therapy. Likewise, the moderation effect may apply to the incumbent versus emergent organizational selection of the solution across regions. Fourth, information disclosure in the field of clinical trial development in the present times of the pandemic is an issue for the global society. Future research may consider whether LTO moderates the disclosure of clinical trial results on the anxiety projects. In other words, based on the disclosure of clinical trial results in the times of COVID-19, further research can focus on whether the interaction between the UAI and LTO can predict differences in these results or not.
Footnotes
Appendix
Control Variables, Definitions, and Rationales.

| Variable | Definition | Measure | Rationale |
|---|---|---|---|
| Project scope | Medical conditions | Count | High scope confounds cultural effects |
| Design scope | Procedures | Count | Research design influence cultural effects |
| Military spending | % of GDP | Continuous | Conflicts correlates with anxiety (PTSD) |
| GDP per capita | GDP/population | Continuous | Developed economy influence anxiety |
| Child vs adult | Children participants | Dummy | Medical condition contingencies |
| Male vs female | Gender | Dummy | Gender conditions contingencies |
| Volunteer enrolment | Patients recruitment | Count | Potential recruitment influences entry decision |
| Organization AC | Firm’s experience | Count | Project-specific experience confounds culture |
| National AC | National sector | Count | Sector development confounds entry decision |
| Global AC (current year) | Global projects | Count | Global clinical trial influences local entries |
| Intervention vs observation | Treatment/safety | Dummy | Intervention vs observation differ |
| Psychotherapy | Vs drug therapy | Dummy | Psychotherapy-drug therapy reflect cultures |
| PDI | Power distance | 1–100 scale | Socio-economic distance influences UA/LTO |
| IDV | Individualism | = | Individualism confounds UA/LTO |
| MAS | Masculinity | = | Masculinity-femininity affect UA/LTO |
| Phases | Timeline | Order | Phase confound cultural effect across differently |
| Years dummies | 2001–2013 | Dummies | Events: NIH created, wars, and economic crisis |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.