
Abstract
In the current article, we comment on a recent article by Stoeber, Kobori, and Brown that provided evidence suggesting that a multidimensional approach to perfectionistic cognitions is superior to a unidimensional approach in predicting maladjustment. They also showed with their data from a university student sample that our Perfectionism Cognitions Inventory has multiple factors in contrast to our unidimensional approach. Our commentary focuses primarily on the issue of whether the Perfectionism Cognitions Inventory should be considered unidimensional versus multidimensional and outlines concerns about how perfectionism cognition factors should be used and interpreted. Although there are serious interpretive problems inherent in existing multidimensional measures of perfectionism cognitions, it is apparent that a cognitive approach is an important and viable supplement to the extensive focus on the trait multidimensional perfectionism that is currently in vogue. We conclude by discussing the potential clinical uses of cognitive assessments of perfectionism.
The perfectionism construct is complex. The field has been dominated over the past two decades by a focus on multidimensional perfectionism from a trait perspective, but other ways of conceptualizing and assessing perfectionism are equally relevant and are just as important when seeking to understand distressed people in clinical and counseling contexts. In 1998, we introduced another way of conceptualizing individual differences in perfectionism by focusing on a cognitive perspective. The Perfectionism Cognitions Inventory (PCI) was created to supplement the trait approach (see Flett, Hewitt, Blankstein, & Gray, 1998). This 25-item inventory assesses the frequency of automatic thoughts reflecting the need to be perfect and associated concerns about being imperfect. The thoughts assessed by this scale are believed to reflect the ideal self-schema described by Hewitt and Genest (1990). In essence, the PCI can be regarded as a measure of the frequency of perfectionistic rumination. This inventory was designed to assess perfectionistic states rather than perfectionistic traits. Existing empirical research suggests that the PCI predicts significant variance in psychological distress and burnout beyond the variance attributable to trait perfectionism (Flett et al., 1998; Hill & Appleton, 2011) and acts as a key mediator of trait perfectionism (e.g., Downey, Reinking, Gibson, Cloud, & Chang, 2014; Wimberly & Stasio, 2013). The PCI has been linked with a range of negative affective states, including feelings of defeat and entrapment (Sturman, 2011). Several intriguing findings have emerged from research using the PCI. Indeed, a recent experimental investigation yielded findings suggesting that some people who seem to have perfectionism that is adaptive may actually be quite vulnerable based on elevated PCI scores (Lo & Abbott, 2013).
The article by Stoeber, Kobori, and Brown (2014) on perfectionism and cognition from a multidimensional perspective is a welcome addition to the literature in that it advances our understanding of the cognitive component of the perfectionism construct. Their work has three unique aspects. First, they provided a clear illustration of how mutual suppression effects occur and why they need to be considered. Second, their article introduces evidence suggesting that the PCI is multidimensional rather than unidimensional when completed by a sample of more than 300 university students. Finally, they make the case that regardless of whether the measure being used is the PCI or the Multidimensional Perfectionism Cognitions Inventory (MPCI), more variance in adjustment scores is accounted for by considering a multidimensional assessment instead of taking a unidimensional approach.
Certain elements of their article merit further analysis. Our commentary focuses on issues related to the multidimensional assessment of perfectionism cognitions. We address four main questions: (a) Should the PCI be considered as multidimensional or unidimensional?; (b) What do the PCI factors identified by Stoeber et al. (2014) actually represent? Here we reexamine their interpretation of these factors; (c) Should the MPCI be seen as a suitable alternative to the PCI?; and (d) Is there clinical utility in treating the PCI as multidimensional?
The Multidimensionality of the PCI
As noted above, Stoeber et al. (2014) presented new evidence suggesting that the PCI is multidimensional and actually assesses three factors, labeled perfectionistic concerns, perfectionistic strivings, and perfectionistic demands. This determination was based on a series of procedures, including extensive analyses of eigenvalues. Although three factors were found, these factors were highly intercorrelated (rs ranging from .62 to .71). Their results suggesting three PCI factors contrast with our original focus on the PCI as unidimensional based on psychometric analyses that we have conducted with large samples of university students (Flett et al., 1998), clinical patients (Flett, Hewitt, Whelan, & Martin, 2008), and adolescents in high school (Flett et al., 2012). The obvious response to this new evidence reported by Stoeber et al. (2014) is that the multidimensionality of the PCI needs to be replicated with data from other samples, including clinical participants. But our position is that even if additional evidence confirms that the PCI does indeed have multiple factors, our initial conceptualization and associated statistical analyses reflected our emphasis on perfectionistic automatic thoughts from a unidimensional perspective. At the conceptual level, we were focused from the outset on perfectionistic automatic thoughts pertaining to the self. The self is the main referent even in the one PCI item that refers explicitly to social pressures (i.e., People expect me to be perfect). We left it to future research to develop a multidimensional measure, and we made this explicit recommendation in the general discussion section of the Flett et al. (1998) article. Unfortunately, this aspect of our discussion was not acknowledged by Stoeber, Kobori, and Tanno (2010) when they referred to the need for a multidimensional approach and concluded uncharitably that “the PCI, however, has an important limitation” (p. 17). We do not see the PCI as limited because our goal here was to expand the assessment and conceptualization of perfectionism by uniquely considering the cognitive and self aspects in accordance with the classification framework of individual difference variables advanced by Buss and Finn (1987).
Our initial psychometric analyses showed consistently that the PCI consists primarily of one large factor, and this fits with our conceptual perspective. We were particularly influenced by evidence that the mean interitem correlations for the PCI items fell in the range that suggested the presence of one factor according to criteria put forth by Briggs and Cheek (1986). They suggested that multiple factors exist when the mean interitem correlations are .20 or lower, but values for the PCI items were considerably higher.
Interpreting the Factors Found in the PCI
Unfortunately, because the PCI was not intended to be multidimensional, there are problems associated with the three PCI factors unearthed by Stoeber et al. (2014), both in terms of the items that comprise the factors and in terms of the interpretation of the factors. It is well known that there is a subjective aspect to conducting factor analyses and interpreting factors. As noted above, Stoeber et al. interpreted the three PCI factors they identified as representing perfectionistic concerns, perfectionistic strivings, and perfectionistic demands in accordance with the general distinction between adaptive striving versus a more dysfunctional concern with not being perfect (see Stoeber & Otto, 2006). The items that comprise the three PCI factors identified by Stoeber et al. (2014) in their new article are reproduced in Table 1 to facilitate our analysis of these factors. A total of 31 items are listed because 5 PCI items had complex loadings on more than one factor and 1 item (i.e., I am too much of a perfectionist) loaded significantly on all three factors.
Items Comprising the PCI Factors.
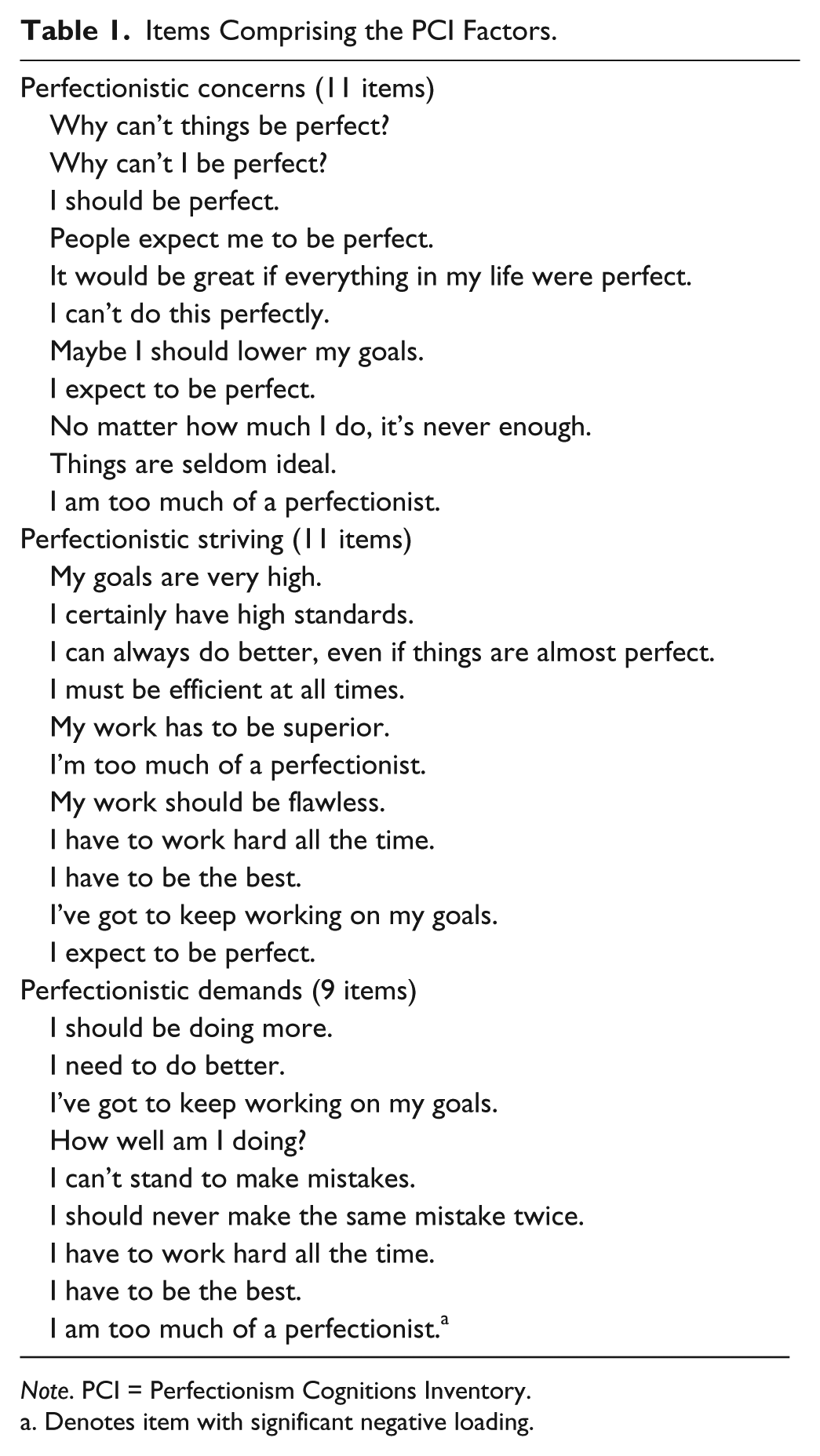
Note. PCI = Perfectionism Cognitions Inventory.
Denotes item with significant negative loading.
The first factor was labeled “perfectionistic concerns.” Stoeber et al. (2014) described this factor as assessing not only perfectionistic doubts but also the full range of concerns, including concern over mistakes, self-ideal discrepancies, and other people’s evaluations. This observation is not completely accurate because this first PCI factor has no items referring directly to concern over mistakes. Unfortunately, the labeling of this factor by Stoeber et al. failed to reflect what we regard as the core cognitive theme inherent in the PCI that is represented in this factor—ruminative thoughts that the self is not perfect but the self must be perfect. PCI items reflecting this theme include “I should be perfect,” I expect to be perfect,” and “Why can’t I be perfect?” Research and clinical assessments have reinforced our sense that dysfunctional perfectionism in the form of automatic thoughts is largely about issues involving the self and involves thoughts and images stemming from the fact that many people feel imperfect and have a core need to be flawless in all aspects of their lives. Accordingly, rather than reflecting perfectionistic concerns, we feel that this factor should be relabeled as “perfectionistic self-rumination.”
The second factor was deemed to be “perfectionistic striving.” This theme is clearly represented in most PCI items that loaded on this factor (e.g., I can always do better, even if things are almost perfect). However, as can be seen in Table 1, when all of the items in this factor are examined, it is apparent that this factor is quite complex; it includes a set of items that actually reflect introjected pressures and “shoulds” and “musts” in keeping with the irrational importance of needing to be perfect as emphasized by Albert Ellis (2002) (e.g., I must be efficient at all times. My work has to be superior. I have to be the best). This theme is important to acknowledge for two reasons. First, it suggests that perfectionistic striving at the level of automatic thoughts reflects a compulsion or internal pressure that is not simply a self-determined choice. These thoughts take on a very different meaning when experienced by the perfectionist who feels capable of striving and attaining perfection versus the perfectionist seen in a clinical context who is not functioning well but who still remains inflexible and is unable or unwilling to lower his or her standards or modify grandiose goals.
Second, several items found on the second PCI factor seem to reflect perfectionistic demands (e.g., My work has to be superior), and this is problematic because “perfectionistic demands” is the label that Stoeber et al. (2014) assigned to the third factor. Their third factor is also complex and does not seem well defined because certain items do not fit the label “perfectionistic demands.” Two items reflect a mistake rumination theme that is clinically important in its own right (e.g., I should never make the same mistake twice. I can’t stand to make mistakes). However, the chief limitation involving the perfectionistic demands factor is that this nine-item factor includes four items that also loaded on the second factor, so the distinction between the second and third factors is not as clear as would be optimally preferred. This third factor also seems to capture most of the more highly endorsed PCI items, and it is possible that this factor, at least to some extent, reflects a “frequency of thoughts” dimension.
These issues related to the labeling of the three PCI factors and their item content are significant ones and reflect the problems that arise when a measure that is designed to be unidimensional is treated as multidimensional. Clearly, the PCI is not an optimal way of measuring multiple automatic thought dimensions. This observation leads inevitably to the question of whether the MPCI should be used instead. This issue is now examined.
The MPCI as an Alternative to the PCI
The MPCI has three factors labeled as perfectionistic standards, pursuit of perfection, and concern over mistakes (Stoeber et al., 2010). It is important for potential users who are comparing the respective measures to realize that the MPCI and the PCI differ in several significant ways that go well beyond the fact that one measure was intended to be unidimensional whereas the other was multidimensional. Clearly, the measures are far from equivalent. For instance, in contrast to the PCI, the MPCI has item content on the perfectionistic standards factor that captures positive beliefs (e.g., It is to my own benefit to set high standards for myself. The higher the goal, the more challenging it is).
Another key difference is that the MPCI seems to lacks items that tap the central emphasis that the PCI has on ruminative thoughts about the self having to be perfect and thoughts about being imperfect. The relevance of these thoughts is clearly shown by the results displayed in Table 2 in the Stoeber et al. (2014) article. Here it can be seen that the PCI factor tapping perfectionistic concerns (or perfectionistic self-rumination, according to our interpretation) is actually the factor from among the various PCI and MPCI factors that has the strongest correlation with depressive symptoms.
We have not used the MPCI in our research because our main focus is on perfectionistic automatic thoughts. One apparent aspect of the MPCI that has not been noted thus far by anyone in this field is that on close inspection, it seems that several MPCI items among the 15 items are worded in ways that actually resemble dysfunctional attitudes in the Weissman and Beck (1978) tradition rather than the automatic thoughts that are spontaneously experienced and elicited in situational contexts. Here we are referring to the positively toned MPCI items listed above as well as other items involving attitude statements such as “There is meaning in doing something perfectly,” “I would feel worthless if I fail,” and “If I can’t do this well, it means I am below average.”
Regardless of whether the MPCI taps dysfunctional attitudes or automatic thoughts, there is no denying that the MPCI is predictive of distress, and this accords with the extensive literature on perfectionistic dysfunctional attitudes (see Brown & Beck, 2002). This brings us to one final concern about the MPCI. Three of the five items in the concern over mistakes subscale have contaminated content that overlaps with the types of items commonly found on depression inventories (e.g., I would feel worthless if I fail. I feel miserable if I make a mistake. I’ll blame myself if I make a mistake), so it is not surprising when this factor is associated with distress.
Accordingly, in light of these observations, we suggest that the PCI and MPCI should be regarded as complementary measures that are clearly not equivalent or redundant with each other. One or both measures should be used depending on the research question being examined. However, given the concerns outlined above, the ideal multidimensional measure of perfectionistic automatic thoughts remains to be developed.
The Clinical Utility of an MPCI
We conclude our commentary with some brief observations about the clinical usefulness of the PCI. Many years ago, B. F. Skinner (1980), in a different context, commented on contemporary research on mental measurement and factor analyses by posing the question, “But what do you do with factors after you get them?” (p. 72). Perhaps the most important question here is whether there is clinical utility in using the PCI as a multidimensional measure. At present, it is difficult to address this issue in a meaningful way since the existence of distinguishable PCI factors has yet to be established in a clinical sample. The measure is more clinically useful at present when treated as a unidimensional measure as intended due to the ease of scoring and the existence of clinical norms.
More generally, it should be evident to most readers that both the PCI and the MPCI have a variety of potential uses in clinical settings. Because the PCI was designed to tap ongoing thoughts and perfectionistic states, it is particularly well suited for use as outcome measure in cognitive-behavioral treatment studies where there is an explicit focus on reducing perfectionistic thoughts. Indeed, some researchers engaged in intervention research have already used the PCI in this manner, and it has been established that reductions in perfectionistic automatic thoughts following cognitive-behavioral therapy are associated significantly with reductions in anxiety, anxiety sensitivity, depressive symptoms, and negative automatic thoughts (Arpin-Cribbie, Irvine, & Ritvo, 2012). There is still merit in also including trait perfectionism measures, as was the case in the Arpin-Cribbie et al. study, to make certain that there are clinically significant changes in the trait components of perfectionism as well.
The PCI and the MPCI also have their uses at the individual case level. Clearly, it is important to establish whether someone who is suffering from perfectionism and associated forms of distress and dysfunction is experiencing thoughts such as “Why can’t I be perfect?” because this information is a key supplement to the information provided by trait measures. Perhaps this person is cognitively clinging to inflexible standards and is still feeling a need to be flawless. These same thoughts can pervade the therapy process and become incorporated into unrealistic recovery goals, so it is important to assess whether this is indeed the case. Select perfectionism cognition items such as “I should be perfect” and “I’m going to aim for the highest standards” could be administered and completed with respect to treatment goals as a way of facilitating discussion about the dangers of being absolutist and using all-or-none thinking when evaluating treatment progress.
The classic review of cognitive self-statement measures provided by Glass and Arnkoff (1997) underscored the importance of establishing the usefulness of these measures in clinical practice. One insightful suggestion they offered is to examine item responses individually and rank-order them in order of their importance for a given client. This seems like a viable procedure with the items from the PCI and the MPCI given the various themes represented in these measures.
In closing, we would like to conclude by noting that more than three decades ago, Glass and Merluzzi (1981) lamented that there is “a dearth of actual validity studies as researchers rush to develop new, creative methods to measure cognitive content” (p. 426). Accordingly, when viewed from this perspective, the article by Stoeber et al. (2014) is a clear contribution to the literature despite our significant concerns about the usefulness and the interpretation of the factors they identified within the PCI. We hope that this exchange will spark further interest in considering the cognitive aspects of perfectionism because key insights are bound to emerge by going beyond the trait approach and more deeply considering perfectionism from a cognitive perspective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.