
Abstract
The ecological–transactional model proposes that nested contexts interact to influence development. From this perspective, child maltreatment represents an individual-level risk factor posited to interact with numerous other nested contextual levels, such as the neighborhood environment, to affect development. The aim of this study was to investigate whether adolescents with maltreatment histories represent a vulnerable group for whom disadvantaged neighborhoods confer risk for substance use disorders. Participants were 411 adolescents (age 15–18; mean age = 16.24) from an investigation of the developmental sequelae of childhood maltreatment. Multiple-group structural equation models, controlling for family-level socioeconomic status, indicated that neighborhood disadvantage was associated with more marijuana-dependence symptoms among maltreated but not among non-maltreated adolescents. Moreover, among maltreated adolescents, those who experienced multiple subtypes of maltreatment were at greatest risk for problematic marijuana use in the context of neighborhood disadvantage. Interestingly, the direct effect of neighborhood disadvantage, but not the interaction with maltreatment, was related to adolescent alcohol-dependence symptoms. Results highlight the importance of considering multiple levels of influence when examining risk associated with child maltreatment.
Introduction
Child maltreatment is considered one of the most adverse and threatening experiences for children (Cicchetti & Lynch, 1995) and has been associated with varied negative developmental outcomes including emotion dysregulation, atypical neurobiological processes, disrupted interpersonal functioning, and psychopathology (see Cicchetti & Toth, 2015 for review). Moreover, child maltreatment represents a well-documented risk factor for problematic alcohol and drug use (e.g., Buckingham & Daniolos, 2013; Moran, Vuchinich, & Hall, 2004; Shin, Hong, & Hazen, 2010). For example, Huang and colleagues (2011) found that young adults with a history of childhood physical abuse were 37% more likely to use illicit drugs compared to those without abuse histories. Importantly, research also indicates that with each additional adverse childhood experience, such as physical and sexual abuse and neglect, the likelihood of early initiation of illicit drug use increases two- to fourfold (Dube et al., 2003), indicating cumulative risk associated with multiple childhood adversities results in heightened susceptibility to substance disorders. Childhood temperament, drinking motives, and externalizing symptomatology are among mechanisms identified to underlie this risk (Goldstein, Flett, & Wekerle, 2010; Oshri, Rogosch, Burnette, & Cicchetti, 2011). Although child maltreatment often co-occurs with additional environmental risk factors (i.e., parental substance use disorder [SUD], poverty, neighborhood crime, and domestic violence; Coulton, Corbin, Su, & Chow, 1995; Drake & Pandey, 1996; Dube et al., 2001; Manly, Oshri, Lynch, Herzog, & Wortel, 2013; McGuigan & Pratt, 2001), there is support for the unique direct effect of maltreatment on subsequent SUDs (Sartor, Agrawal, McCutcheon, Duncan, & Lynskey, 2008; Shin et al., 2010).
The ecological–transactional model proposes that nested contexts interact to influence development (e.g., Bronfenbrenner, 1977; Cicchetti & Lynch, 1993). From this perspective, child maltreatment represents an individual-level risk factor posited to interact with numerous other nested contextual levels, such as the neighborhood environment, to affect development. According to social disorganization theory (Sampson & Groves, 1989; Shaw & McKay, 1942), neighborhood characteristics such as low socioeconomic status (SES) and high residential mobility impede neighborhood collective socialization, which can contribute to a neighborhood context with greater exposure to deviancy and substance use and fewer adults willing or available to supervise neighborhood youths.
Research investigating neighborhood influences on youth adaptation has relied on both objective (i.e., U.S. census poverty indicators) and subjective (i.e., youth and/or parent report of neighborhood safety, drug availability, cohesion) measurements of disadvantage. In spite of these differences, there is evidence that children, adolescents, and adults living in disadvantageous neighborhoods have greater exposure to substances and more opportunities to use them (Crum, Lillie-Blanton, & Anthony, 1996; Storr, Chen, & Anthony, 2004). Previous research also indicates elevated levels of alcohol and drug use among individuals living in disadvantaged neighborhoods (e.g., Cerdá, Diez-Roux, Tchetgen, Gordon-Larsen, & Kiefe, 2010). For instance, Tucker, Pollard, de la Haye, Kennedy, and Green (2013) found that a higher neighborhood unemployment rate enhanced adolescent risk for marijuana use initiation. Moreover, Furr-Holden and colleagues (2011) demonstrated that young adults living in deteriorating neighborhoods were more likely to use marijuana than individuals living in more stable and less disadvantaged neighborhoods. There are notable exceptions, however (e.g., Allison et al., 1999; Mathur, Erickson, Stigler, Forster, & Finnegan, 2013), which may be due to the differing definitions of neighborhood disadvantage across studies and individual differences in susceptibility to neighborhood disadvantage risk (consistent with the ecological–transactional model).
A number of studies have demonstrated support for the ecological–transactional model with regard to the interplay of child maltreatment and the neighborhood context in shaping youth antisocial behavior. For example, Jaffee, Caspi, Moffitt, Polo-Tomás, and Taylor (2007) showed that neighborhood crime, social cohesion, and social control differentiated resilient and nonresilient maltreated children with regard to antisocial behavior. Moreover, Yonas and colleagues (2010) found neighborhood collective efficacy buffered the risk associated with childhood neglect, but not abuse, on youth aggressive behavior.
Taken together, prior research suggests that both child maltreatment and neighborhood disadvantage confer risk for the development of SUDs. Moreover, evidence has been shown that these two ecological levels may interact to affect youth antisocial behavior (Jaffee, Caspi, Moffitt, Polo-Tomás, & Taylor, 2007; Yonas et al., 2010). There is also emerging support for the notion that maltreated individuals may be especially vulnerable to SUDs in the context of disadvantageous neighborhoods. Specifically, among a sample of predominately African American adults, neighborhood disorganization predicted adult problem drinking only among individuals with self-reported high levels of child maltreatment (Keyes et al., 2012). However, whether maltreated children living in disadvantaged neighborhoods are at heightened risk for developing SUD in adolescence remains unknown. Additionally, whether experiencing multiple different subtypes of maltreatment represents a cumulative risk by which vulnerability to disadvantaged neighborhoods is enhanced has also yet to be examined.
The present study addresses these critical gaps in the literature in a number of important ways. First, we employ a sample of low-income at risk adolescents. Investigating etiological pathways to SUDs during adolescence is developmentally salient from a preventive intervention standpoint, given the well-documented negative consequences associated with substance problems during this period (e.g., Brown et al., 2008). Second, we utilize the Department of Human Services (DHS) records and the Maltreatment Classification System (MCS; Barnett, Manly, & Cicchetti, 1993) to document maltreatment histories, thus avoiding limitations associated with self-report and retrospective measurements of maltreatment. Third, we investigate the impact of the number of maltreatment subtypes experienced, which allows for a more nuanced understanding of cumulative risk associated with multiple different types of maltreatment. Finally, we use a multi-method measurement of neighborhood disadvantage, which incorporates U.S. census data, parent and adolescent reports of neighborhood safety, and adolescent reports of neighborhood drug availability. We hypothesize that maltreated adolescents, compared to non-maltreated adolescents, will be more susceptible to a disadvantaged neighborhood context. Relatedly, we also expect that the deleterious effect of neighborhood disadvantage on substance dependence will be strongest for adolescents who have experienced multiple subtypes of maltreatment.
Method
Participants
Participants for the current study were 411 adolescents (age 15–18; mean age = 16.24) from an investigation of the developmental sequelae of childhood maltreatment. The sample included both maltreated (n = 266) and non-maltreated adolescents (n = 141). Approximately half were male (57.3%), 55.8% African American, 27.8% Caucasian, 10.8% Hispanic, and 5.6% indicated another race/ethnicity. Maltreated and non-maltreated adolescents did not differ on age, t(405) = −1.81, gender, χ2(1) = .50, or race/ethnicity, χ2(3) = 4.84.
Parents provided informed consent for their adolescent’s participation and for complete access to any family records in the DHS. Maltreated children were identified prior to recruitment by a county DHS liaison based on the presence of documented records of child abuse and/or neglect reports. Comprehensive searches of DHS records were completed, and all maltreatment information was coded utilizing the MCS(Barnett et al., 1993). The MCS uses DHS records detailing investigations and findings involving maltreatment in identified families over time. The MCS codes all available information from DHS records, making independent determinations of maltreatment experiences. Based on operational criteria, the MCS designates all of the subtypes of maltreatment children have experienced (i.e., neglect, emotional maltreatment, physical abuse, and sexual abuse). Coding of the DHS records was conducted by trained research assistants, doctoral students, and clinical psychologists. Adequate reliability has been obtained (weighted ks = 0.86–0.98; Manly, 2005).
Number of maltreatment subtypes
In terms of the subtypes of maltreatment, neglect involves failure to provide for the child’s basic physical needs for adequate food, clothing, shelter, and medical treatment. Additionally, forms of this subtype include lack of supervision, moral–legal neglect, and education neglect (68.1% of maltreated children experienced neglect in this sample). Emotional maltreatment involves extreme thwarting of children’s basic emotional needs for psychological safety and security, acceptance and self-esteem, and age-appropriate autonomy. Examples of emotional maltreatment of increasing severity include belittling and ridiculing the child, extreme negativity and hostility, exposure to severe marital violence, abandoning the child, and suicidal or homicidal threats (51.4% of maltreated children experienced emotional maltreatment). Physical abuse involves the nonaccidental infliction of physical injury on the child (e.g., bruises, welts, burns, choking, broken bones). Injuries range from minor and temporary to permanently disfiguring (40.8% of maltreated children experienced physical abuse). Finally, sexual abuse involves attempted or actual sexual contact between the child and a family member or person caring for the child for purposes of that person’s sexual satisfaction or financial benefit. Events range from exposure to pornography or adult sexual activity, to sexual touching and fondling, to forced intercourse with the child (18.4% of maltreated children experienced sexual abuse). In the current sample, the majority of maltreated adolescents experienced multiple subtypes of maltreatment (M = 2.15 subtypes, SD = 1.0).
Because maltreated children are predominantly from low SES families (Fourth National Incidence Study of Child Abuse and Neglect; Sedlak et al., 2010), demographically comparable non-maltreated children were recruited from families receiving Aid to Families with Dependent Children. DHS record searches were completed for these families to verify the absence of any record of child maltreatment. Trained research assistants also interviewed mothers of children recruited for the non-maltreatment group to confirm a lack of DHS involvement and prior maltreatment experiences (Cicchetti, Toth, & Manly, 2003). In addition, families who received preventive services through DHS because of concerns over risk for maltreatment also were excluded from the non-maltreated comparison group.
Participants and their parent were interviewed individually in private interview rooms by trained research assistants who were unaware of the participant’s maltreatment status and research hypotheses. The participants and their parent completed a range of assessments, including self-report measures and interviews regarding the adolescent’s behavioral functioning and substance use.
Measures
Neighborhood disadvantage
Neighborhood safety was assessed with both parent and adolescent reports of 15 items from the Neighborhood Environment for Children Rating Scale (Coulton, Korbin, & Su, 1999). Participants reported on the frequency of each item in their neighborhood using a scale of (1) rarely to (10) frequently. Items included “unemployed adults loitering,” “gang activity,” and “vacant, abandoned, or boarded up buildings.” Mean scores were calculated such that high scores indicated the lack of neighborhood safety (see Table 1 for descriptive statistics). Reliabilities (αs) ranged from .94 to .95.
Descriptive Statistics.
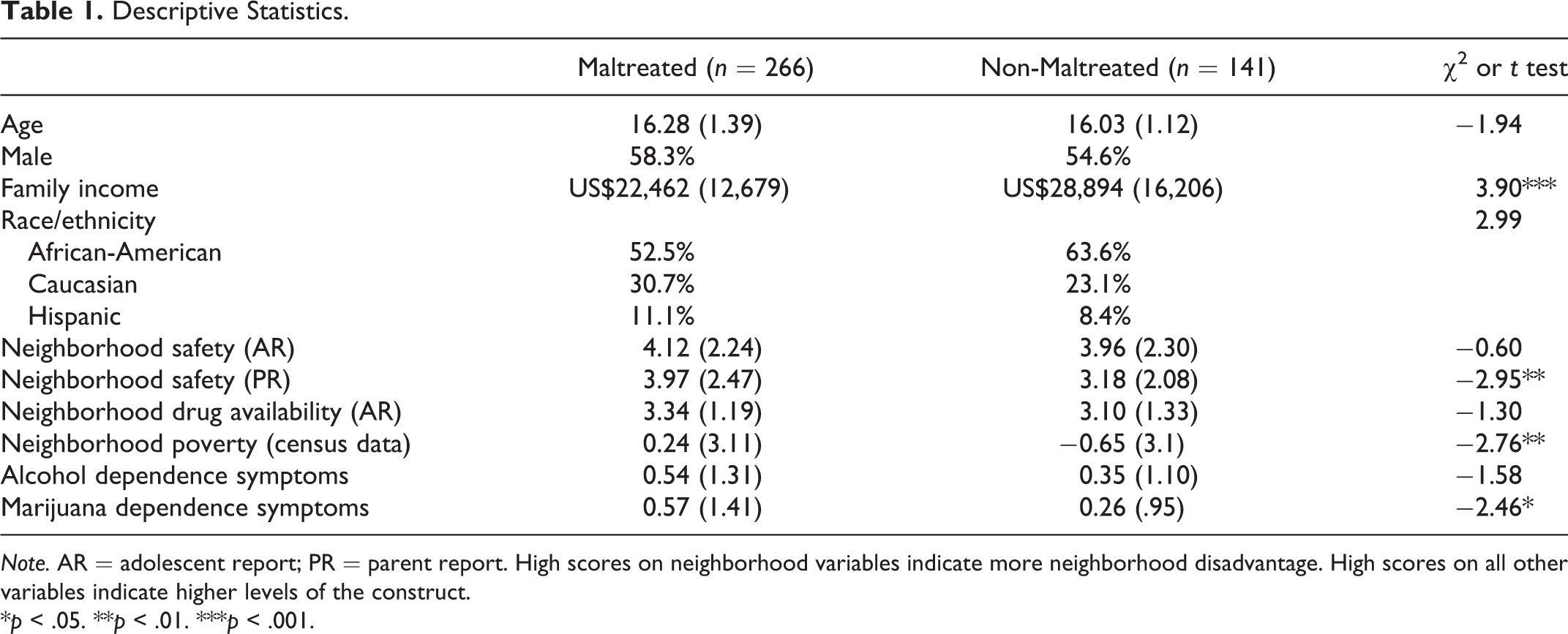
Note. AR = adolescent report; PR = parent report. High scores on neighborhood variables indicate more neighborhood disadvantage. High scores on all other variables indicate higher levels of the construct.
*p < .05. **p < .01. ***p < .001.
Neighborhood drug availability was measured using adolescent report of 3 items written by project staff. Adolescents indicated their agreement with each statement on a scale of (1) strongly disagree to (5) strongly agree. Items included “Marijuana would be easy to find in my neighborhood” and “Lots of drugs are sold in my neighborhood.” A mean score was computed such that high scores indicated more neighborhood drug availability (see Table 1 for descriptive statistics). Reliability (α) was .87.
Neighborhood poverty was measured using 2000 U.S. census data. Following Trim and Chassin (2008) and Mathur, Erickson, Stigler, Forster, and Finnegan (2013), principle components analysis was used to derive a composite of neighborhood poverty. The following census track-level variables were included: (1) median household income, (2) percentage of residents living in the same household for the past 5 years, (3) percentage of owner occupied units, (4) percentage of female headed households with children under 18 and below the poverty line, and (5) percentage of unemployment rate. These indices were chosen, given their use in prior studies of neighborhood disadvantage (e.g., Allison et al., 1999; Mathur et al., 2013; Tucker, Pollard, de la Haye, Kennedy, & Green, 2013). Scores were coded such that high scores indicated greater neighborhood poverty. Z scores were computed for the five census track variables and a sum was calculated. See Table 1 for descriptive statistics.
As described below, the above four indicators of neighborhood disadvantage (i.e., neighborhood safety—parent report, neighborhood safety—adolescent report, neighborhood drug availability, and census poverty data) were subsequently modeled as indicators of a neighborhood disadvantage latent construct.
Family income
Parents reported on the total family income, including money from employment of all adults in the home, public assistance, child support, and any other sources of income. See Table 1 for descriptive statistics.
Adolescent alcohol and marijuana dependence
Current (i.e., past 12 months) alcohol and marijuana dependence symptoms were assessed using the Diagnostic Interview Schedule for Children (DISC; Shaffer et al., 1993). The DISC is a well-validated structured interview for children and adolescents (Fisher et al., 1993; Piacentini et al., 1993) and provides diagnostic scoring based on the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.). Given the relative young age of participants (mean = 16.2), only 4.7% met criteria for alcohol dependence and 7.4% of the sample met criteria for marijuana dependence. Therefore, the total count of alcohol-dependence symptoms and the total count of marijuana-dependence symptoms were used as separate dependent variables in subsequent models. The range of number of symptoms endorsed for both alcohol and marijuana dependence was 0–7 (17% endorsed at least one alcohol symptom and 15.6% endorsed at least one marijuana symptom). See Table 1 for descriptive statistics.
Data Analytic Plan
Analyses were performed using Mplus Version 7.0 (Muthén & Muthén, 1998–2012) with maximum likelihood estimator with robust standard errors, which computes parameter estimates for continuous outcomes with standard errors that are robust to nonnormality and nonindependence of observations. First, measurement modeling was conducted with the complete sample (n = 411) to determine the appropriate factor structure of the four hypothesized indicators of neighborhood disadvantage (i.e., neighborhood safety—adolescent report, neighborhood safety—parent report, neighborhood drug availability, and neighborhood poverty). Next, measurement invariance testing was conducted to examine factor loading invariance across maltreatment status. Results of measurement modeling informed model building in subsequent structural equation models (SEMs).
To account for the nonindependence of the observations (i.e., clustering within neighborhood census tracks), standard errors were adjusted using the “complex” command in Mplus. 1 Missing data for endogenous variables were handled using full information maximum likelihood, and listwise deletion was used for missing on exogenous variables. Model fit for confirmatory factor analyses (CFAs) and SEMs was evaluated using the comparative fit index (CFI), root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). CFI values greater than .95, RMSEA values less than .06, SRMR values less than .06, and a nonsignificant χ2 statistic were considered evidence of good model fit (Hu & Bentler, 1999; Yu and Muthen, 2002).
First, two sets of multiple-group SEMs were conducted to examine whether the effect of the latent variable “neighborhood disadvantage” on adolescent substance dependence (Model 1 = alcohol dependence and Model 2 = marijuana dependence) depended on adolescents’ maltreatment status. Next, an additional set of SEMs were estimated to examine the moderating role of the number of maltreatment subtypes experienced (continuous variable) in the relation between neighborhood disadvantage and adolescent substance dependence (Model 1 = alcohol dependence and Model 2 = marijuana dependence). To test the interaction of number of maltreatment subtypes and neighborhood disadvantage on alcohol symptoms, the XWITH command was used in Mplus. This allows an interaction term to be created between an observed continuous variable (i.e., number of maltreatment subtypes) and a latent variable (i.e., neighborhood disadvantage). Estimating latent variable by observed variable interactions in Mplus requires the “type = random” specification, which disallows the ability to adjust standard errors for clustering. As such, this model was estimated without accounting for the neighborhood-level clustering.
Results
Demographic Characteristics and Substance Dependence Among Maltreated and Non-Maltreated Adolescents
T-tests and chi-square comparisons were conducted to examine the mean-level differences across maltreatment status on demographic variables, neighborhood disadvantage indicators, and alcohol and marijuana dependence symptoms (see Table 1). Parents of maltreated adolescents reported less safe neighborhoods, t = −2.95 (248.08), p < .01, and maltreated adolescents lived in neighborhoods with worse neighborhood poverty, t = −2.76 (332), p < .01. Groups did not differ on adolescent report of neighborhood safety or neighborhood drug availability. Maltreated adolescents endorsed more marijuana dependence symptoms compared to non-maltreated adolescents, t = −2.46 (326.55), p < .05, but groups did not differ on alcohol-dependence symptoms.
Measurement Modeling
CFA was conducted to determine the appropriate factor structure of the four neighborhood variables. Results of the CFA indicated that a one-factor model was a good fit to the data, χ2(1) = .04, p = .85, CFI = 1.00, RMSEA < 0.001, SRMR = 0.002, with factor loadings all significant at p < .001 and ranging from .33 to .78. Measurement invariance testing was conducted to examine factor loading invariance across maltreatment status (n = 141 non-maltreated adolescents and n = 266 maltreated adolescents) for the latent variable neighborhood disadvantage. First, a model which constrained factor loadings to be equal across groups was tested and demonstrated fair fit to the data, χ2(8) = 17.43, p = .03, CFI = 0.93, RMSEA = 0.08, SRMR = 0.07. A model which relaxed all constraints across groups was tested next and evidenced good fit to the data, χ2(4) = 4.97, p = .29, CFI = 0.99, RMSEA = 0.04, SRMR = 0.04, that was significantly better than the constrained model, Satorra-Bentler Δχ2(4) = 15. 91, p = .003. Therefore, there was evidence of factor loading variance across maltreatment status. An investigation of factor loadings revealed that although the rank order for the loadings of the indicators was the same across groups, loadings tended to be lower for maltreated youth. These results informed subsequent model specification as described below.
Multiple-Group SEM
Two sets of multiple-group SEMs were conducted to examine whether the effect of the latent variable neighborhood disadvantage on adolescent substance dependence (Model 1 = alcohol dependence symptoms and Model 2 = marijuana dependence symptoms) depended on adolescents’ maltreatment experience. Neighborhood disadvantage (latent variable), adolescent age and gender, and family income were entered as correlated exogenous variables and a count of adolescent dependence symptoms (Model 1 alcohol and Model 2 marijuana) were endogenous variables. In preliminary models, adolescent gender did not significantly uniquely predict dependence symptoms. Given the lack of theorized gender effects, and to attain a more parsimonious model, gender was trimmed from the final models. 2
Alcohol-dependence symptoms
To examine the interaction of maltreatment status and neighborhood disadvantage, an SEM was first tested which constrained all paths within the structural model (i.e., paths from exogenous variables to endogenous variable) to be equal across maltreatment groups but freed the measurement portion of the model across groups (based on preliminary measurement invariance testing described above). This model evidenced good model fit, χ2(31) = 36.85, p = .22; CFI = 0.96; RMSEA = 0.03; SRMR = 0.06. Next, a partially unconstrained model was tested which allowed the path from neighborhood disadvantage to adolescent alcohol dependence symptoms to vary across maltreatment groups. This model also evidenced good model fit, χ2(30) = 34.96, p = .24; CFI = 0.97; RMSEA = 0.03; SRMR = 0.06, that was not significantly better than the previous model, Satorra-Bentler Δχ2(1) = 1.89, p = .17. Thus, there was no evidence of an interaction between maltreatment status and neighborhood disadvantage. Rather, results indicated that more neighborhood disadvantage predicted more alcohol-dependence symptoms (b = .24, SE = 0.07, p < .01) among all adolescents, regardless of maltreatment history. Family income and adolescent age were not significant predictors of alcohol dependence (bincome = −.01 SE = 0.07; bage = .04, SE = 0.06. ps = ns).
Marijuana-dependence symptoms
Next, the same set of models was tested to examine moderation by maltreatment status in the prediction of marijuana-dependence symptoms. The model which constrained all paths within the structural model to be equal for maltreated and non-maltreated adolescents evidenced fair fit to the data, χ2(31) = 42.21, p = .08; CFI = 0.93; RMSEA = 0.04; SRMR = 0.07. The partially unconstrained model demonstrated good model fit, χ2(30) = 36.31, p = .20; CFI = 0.96; RMSEA = 0.03; SRMR = 0.06, that was significantly better than the previous model, Satorra-Bentler Δχ2(1) = 6.71, p = .009. Thus, results indicated that a model allowing the path from neighborhood disadvantage to marijuana symptoms to vary by maltreatment status was a significantly better fit to the data than a model that constrained this path to be equal across groups. Furthermore, higher levels of neighborhood disadvantage significantly predicted more adolescent marijuana symptoms among maltreated adolescents (b = .22, SE = 0.08, p < .01) but not non-maltreated adolescents (b = −.05, SE = 0.09, p = ns). Therefore, results indicated significant moderation of neighborhood disadvantage on adolescent marijuana-dependence symptoms by adolescent maltreatment status. 3 See Figure 1 for standardized path coefficients from partially constrained multiple-group SEM.

Multiple-group structural equation model of effect of neighborhood disadvantage on adolescent marijuana dependence symptoms. Note. Standardized path coefficients from partially constrained multiple group SEM presented. M = maltreated; N = non-maltreated. Model fit the data well: χ2 (30) = 36.31, p = .20; comparative fit index = .96; root mean square error of approximation = 0.03; and standardized root mean square residual = 0.06. Although not depicted, all correlations among exogenous variables were modeled. Neighborhood disadvantage was coded such that high scores indicate more neighborhood disadvantage. All factor loadings are significant at p < .001. *p < .05. **p < .01.
Moderation by Number of Maltreatment Subtypes
Additional SEMs were conducted to determine whether adolescents who experienced multiple subtypes of maltreatment are especially vulnerable to disadvantaged neighborhoods. Specifically, the number of different maltreatment subtypes (neglect, emotional abuse, physical abuse, and sexual abuse) experienced throughout the adolescent’s life was examined as a moderator of the effect of neighborhood risk on alcohol and marijuana dependence symptoms in separate models (0 = non-maltreated [38.3% of the sample], 1 = 1 subtype [19.8%], 2 = 2 subtypes [18.7%], 3 = 3 subtypes [17.2%], and 4 = 4 subtypes [6.1%]). Among the maltreated children, the mean number of maltreatment subtypes was 2.15 (SD = 1.0).
Alcohol-dependence symptoms
SEM was conducted with adolescent age, family income, and neighborhood disadvantage (latent variable) entered as correlated exogenous variables. The endogenous variable was a count of adolescent alcohol-dependence symptoms. Consistent with the above alcohol model results, a significant interaction was not found between maltreatment subtypes and neighborhood disadvantage in predicting alcohol-dependence symptoms (β = .04, SE = 0.04, p = ns).
Marijuana-dependence symptoms
The same SEM was conducted as described above with the substitution of marijuana-dependence symptoms as the endogenous variable. The pattern of results mirrored those reported in the original multiple-group SEM predicting marijuana dependence, however, moderation was further clarified. Regarding the number of maltreatment subtypes, a significant interaction was found between neighborhood disadvantage and subtypes (β = .11, SE = 0.05, p = .03) and was probed at the levels of 0–4 maltreatment subtypes experienced the following guidelines of Aiken and West (1991). Results indicated that as the number of maltreatment subtypes increases, neighborhood disadvantage was more strongly associated with marijuana dependence symptoms (β1subtype = .09, SE = 0.04, p =.04; β2subtypes = .21, SE = .08, p = .01; β3subtypes = .32, SE = .13, p = .02; and β4subtypes = .43, SE = 0.18, p = .02) but not for non-maltreated adolescents (βnonmal = −.02, SE = 0.04, p = ns). See Figure 2 for graphical representation of interaction.
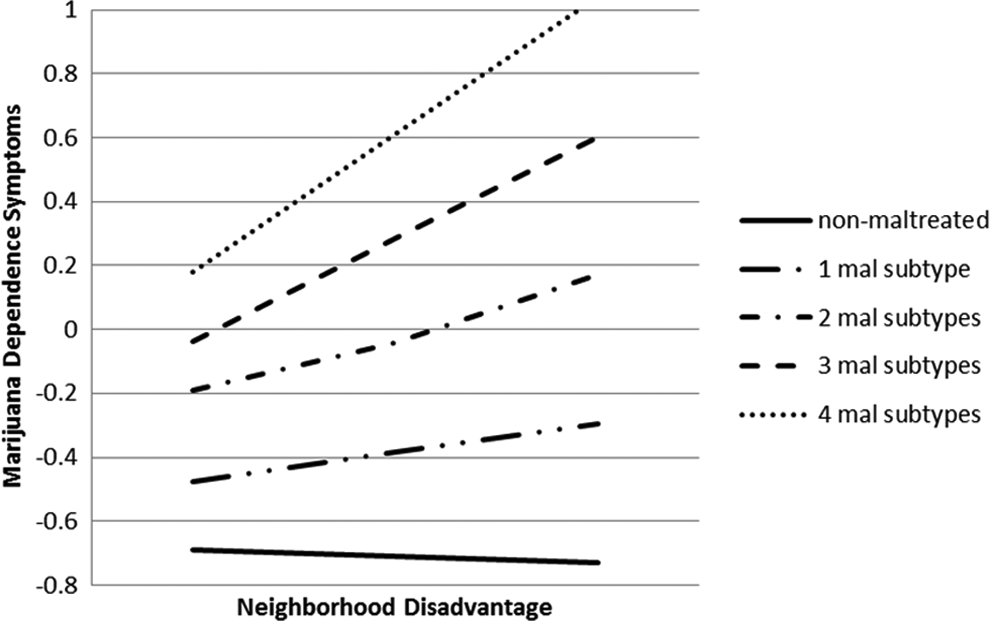
Effect of neighborhood disadvantage on adolescent marijuana-dependence moderated by the number of maltreatment subtypes experienced.
Discussion
The present study investigated the interactive effects of child maltreatment and neighborhood disadvantage in the prediction of adolescent alcohol- and marijuana-dependence symptoms. Although it is well established that child maltreatment enhances risk for substance use and SUDs (see Tonmyr, Thornton, Draca, & Wekerle, 2010 for review), and that neighborhood context is influential in shaping youth substance use and SUDs (Furr-Holden et al., 2011; Tucker et al., 2013), whether adolescents with maltreatment histories are especially vulnerable to the risk associated with neighborhood disadvantage has yet to investigated. Consistent with the ecological–transactional model (Bronfenbrenner, 1977; Cicchetti & Lynch, 1993), our results indicate that higher neighborhood disadvantage was associated with more marijuana-dependence symptoms among maltreated adolescents only. Further clarifying this interaction, we found that among maltreated adolescents, those who endured multiple subtypes of maltreatment (i.e., neglect, emotional maltreatment, physical abuse, and/or sexual abuse) were at greatest risk for problematic marijuana use. Importantly, these effects were over and above family income, a marker of family-level SES, indicating that neighborhood disadvantage is distinctly influential and not a mere marker of family poverty.
According to social disorganization theory (Sampson & Groves, 1989; Shaw & McKay, 1942), neighborhood characteristics such as low SES and high residential mobility thwart neighborhood cohesion, support, and control, which can lead to an environment with less community adult supervision and monitoring of youth (Chung & Steinberg, 2006; Sampson & Laub, 1994; Tolan, Gorman-Smith, & Henry, 2003). Maltreated adolescents may be especially vulnerable in this neighborhood context for a number of reasons. First, maltreated youth are less likely to be effectively monitored by their own parents (Rogosch, Cicchetti, Shields, & Toth, 1995), which enhances the likelihood of affiliation with deviant substance-using peers (e.g., Chassin, Pillow, Curran, Molina, & Barrera, 1993), a robust proximal predictor of adolescent substance use (e.g., Brown et al., 2008). Moreover, maltreated youth have a greater likelihood of a disinihibitory temperament style (Braquehais, Oquendo, Baca-Garcia, & Sher, 2010; Brodsky et al., 2001), which is also associated with seeking out deviant peers (Burt, McGue, & Iacono, 2009; Kirisci, Mezzich, Reynolds, Tarter, & Aytaclar, 2009). This constellation of individual-, family-, and peer-level risk factors associated with child maltreatment may explain why maltreated youth are more vulnerable to marijuana dependence in the context of risky disadvantaged neighborhoods.
A different pattern of results emerged when examining alcohol dependence. Our results suggest that among low-income adolescents, neighborhood disadvantage confers risk for alcohol problems regardless of maltreatment experience. These findings are consistent with the studies demonstrating direct effects of neighborhood disadvantage on alcohol problems (e.g., Cerdá et al., 2010). In understanding why maltreated adolescents may be more susceptible to marijuana dependence versus alcohol dependence in the context of risky neighborhoods, it is important to consider our measurement of neighborhood. Our neighborhood disadvantage latent construct included diverse indicators such as exposure to unemployed adults loitering, gang activity, low household income, and easy access to drugs within the neighborhood. Thus, adolescents in our sample residing in highly disadvantageous neighborhoods likely experienced frequent exposure and access to the sale and use of marijuana. Lambert, Brown, Phillips, and Ialongo (2004) demonstrated that adolescents living in neighborhoods marked by drug use and sales, violence, and the lack of safety were more likely to approve of drug use and less likely to view drug use as harmful, which in turn predicted higher levels of adolescent drug use. Enhanced positive beliefs about marijuana due to neighborhood exposure, in concert with maltreated adolescents’ vulnerability to disinhibition (Braquehais et al., 2010; Brodsky et al., 2001), a personality trait more strongly associated with drug versus alcohol disorder (McGue, Slutske, & Iacono, 1999), may function to enhance the risk for marijuana versus alcohol dependence in the context of risky neighborhoods. Additionally, African American adolescents represented the majority of our sample. Prior research suggests that alcohol use may not be as salient among African American adolescents compared to White adolescents, whereas marijuana use may be more salient among African American adolescents versus White adolescents (Kann et al., 2014). Thus, the racial makeup of our sample may also have contributed to our finding that maltreated adolescents are at heightened vulnerability to marijuana dependence, rather than alcohol dependence, in the context of risky neighborhoods. Given this vulnerability, preventive interventions targeting youth with maltreatment histories may be most effective when incorporating strategies for reducing youths’ unstructured and unsupervised time spent in the neighborhood such as promoting organized and supervised activities in community centers and schools.
The current study contributes to the literature by examining whether neighborhood disadvantage confers risk for adolescent alcohol and marijuana dependence differently for maltreated and non-maltreated youth, utilizing a multi-method assessment of neighborhood context, employing DHS records to determine maltreatment, and further clarifying maltreatment by examining the number of maltreatment subtypes experienced. In spite of these contributions, limitations should be noted. First, this was a cross-sectional study. Although prospective prediction is necessary for inferring directionality, the reverse direction of effect in this study (i.e., adolescent SUD effects on neighborhood disadvantage) is less plausible, therefore, strengthening the likelihood of our interpretations. Second, caution is warranted when generalizing our findings beyond low-income youth. For instance, there is evidence that affluent neighborhoods may exert risk differently compared to low-income neighborhoods (Trim & Chassin, 2008). Moreover, the majority of the adolescents in our study were African American, again limiting generalizability. Given prior research demonstrating greater neighborhood poverty among low-income African American versus low-income Caucasian families (Logan, 2011), future research examining the role of race in these associations would be informative. Finally, we speculated about mechanisms underlying maltreated adolescents’ risk for marijuana dependence in the context of neighborhood disadvantage. Further research is necessary to elucidate the processes by which this risk is conferred and to clarify unique pathways to alcohol versus drug disorders. This information will be vital to effective preventive intervention design.
In sum, results suggest that maltreated adolescents are at risk for marijuana dependence in the context of risky neighborhoods and that adolescents who have experienced multiple different forms of maltreatment are at the greatest risk. Moreover, findings indicate that neighborhood disadvantage transmits risk for alcohol dependence among both maltreated and non-maltreated low-income youth. These results highlight the importance of testing interactions among various levels of ecology to provide a more comprehensive picture of the etiology of SUD and indicate the need to include critical individual-level risk factors, such as child maltreatment, when investigating neighborhood effects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors are grateful to the National Institute on Drug Abuse (DA12903) and the Spunk Fund, Inc. for their support of this work.