
Abstract
Recent changes to federal legislation created a requirement for states to address the needs of infants with prenatal substance exposure. Understanding clinical outcomes among substance exposed infants prior to these changes is important for establishing a baseline of risk and informing systems-level responses. Using North Carolina, Georgia, and Texas Medicaid data, we examined the incidence of inpatient and outpatient diagnoses for injury, maltreatment, and developmental disorders prior to age 12 months and compared types of diagnoses among substance exposed and unexposed infants. The cumulative incidence of maltreatment (1.2% vs. 0.2%) and developmental disorder (10.7% vs. 1.5%) diagnoses prior to age 12 months was significantly higher among substance exposed compared to unexposed infants. The incidence of injury diagnoses was similar (3.7% vs. 3.4%). We observed differences in types of maltreatment and injury diagnoses. For example, diagnoses for neglect were more common among substance exposed infants while diagnoses for physical abuse were more common among unexposed infants. Results provide insight for informing monitoring and intervention by medical and public health professionals.
Substance use in pregnancy is a persistent medical, social, and public health issue in the United States (Substance Abuse and Mental Health Services Administration, 2018; Agrawal et al., 2019; Bateman et al., 2014; Brown et al., 2017; McCabe & Arndt, 2012; Patrick et al., 2012; Desai et al., 2015; Desai et al., 2014). The Comprehensive Addiction and Recovery Act (CARA) of 2016 amended the Child Abuse Prevention and Treatment Act (CAPTA), creating a requirement for states to develop a law or statewide program to address the needs of infants with prenatal substance exposure, including exposure to alcohol and illicit and prescription drugs, following hospital discharge (Lloyd et al., 2019). A detailed understanding of clinical outcomes among substance exposed infants prior to these legislative changes is important for establishing a baseline of risk among substance exposed infants and informing systems-level responses implemented as part of the CARA requirements.
Recent studies have examined clinical outcomes among substance exposed infants (Agrawal et al., 2019; Hwang et al., 2017; Puls et al., 2019; Uebel et al., 2015; Witt et al., 2017) with prior studies demonstrating an increased risk of hospitalization for a variety of conditions during infancy and early childhood among substance exposed infants compared to their unexposed counterparts (Hwang et al., 2017; Puls et al., 2019; Uebel et al., 2015; Witt et al., 2017). For example, a cohort study in Washington State found an increased risk of re-hospitalization prior to age five years for infants with neonatal abstinence syndrome (NAS; i.e. neonatal opioid withdrawal syndrome) compared to non-NAS infants, including an increased risk of re-admission for neurologic, respiratory, digestive, and infectious diseases (Witt et al., 2017). Similarly, a cohort study in Australia observed an increased risk of re-hospitalization up to age 13 years for maltreatment and mental and behavioral disorders among NAS compared to non-NAS infants (Uebel et al., 2015). Among 2003–2009 births in Massachusetts, infants born to mothers with substance use disorders in pregnancy had higher use of hospital-based care, including hospital admissions, observational stays, and emergency department visits, in the first year of life compared to infants of mothers without a documented substance use disorder in pregnancy (Hwang et al., 2017). In a nationally-representative sample of 2013–2014 births, prenatal substance exposure was associated with an increased risk of physical abuse hospitalizations prior to age 6 months (Puls et al., 2019).
While results from these studies contribute substantially to our understanding of the needs of substance exposed infants, there are gaps. First, prior studies have largely been limited to examining outcomes identified in the inpatient setting, excluding those diagnosed in an outpatient setting (Hwang et al., 2017; Patrick et al., 2015; Puls et al., 2019; Uebel et al., 2015; Witt et al., 2017). Some outcomes, such as injuries and developmental disorders, may be more likely to be diagnosed in an outpatient setting. Second, several recent studies have been limited to examining outcomes among infants with NAS, excluding infants with prenatal substance exposure that did not result in diagnosed withdrawal (Patrick et al., 2015; Uebel et al., 2015; Witt et al., 2017). Last, previous studies have not compared specific types of various outcomes (e.g., type of maltreatment or injury) among substance exposed and unexposed infants (Patrick et al., 2015; Uebel et al., 2015; Witt et al., 2017). A more nuanced understanding of clinical outcomes among substance exposed infants can provide important detail for informing programmatic and policy intervention.
The aims of the present study were to use data regarding Medicaid or Children’s Health Insurance Program (CHIP) enrolled infants from multiple states to (1) examine the cumulative incidence of inpatient and outpatient diagnoses for injury, maltreatment, and developmental disorders and (2) compare types of injury, maltreatment, and developmental disorder diagnoses received prior to age 12 months among infants with and without prenatal substance exposure. We examined these clinical outcomes prior to the enactment of CARA and associated amendments to CAPTA to establish a baseline of risk among substance exposed infants. We also examined these outcomes among all substance exposed infants, as laws or statewide programs implemented in response to the 2016 CARA legislation are to address the needs of all substance exposed infants, regardless of substance exposure type or the presence of withdrawal symptoms.
Method
Data Source
We used data from the 2006-2011 Medicaid Analytic eXtract (MAX) files for North Carolina, Georgia, and Texas available through the Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill. State Medicaid agencies submit quarterly eligibility, enrollment, and claims data for all Medicaid and CHIP beneficiaries to the Centers for Medicare (CMS) and Medicaid Services via the Medicaid Statistical Information System (MSIS). MAX data files are then created from the MSIS to support research and policy analysis. MAX files include beneficiary eligibility and demographic data as well as service utilization, diagnoses, and payment source information for inpatient and outpatient visits.
Study Population
Our study population included live born infants who were enrolled in or had a Medicaid or CHIP claim in their year of birth for 2006–2009 births in North Carolina, Georgia, and Texas and 2010 births in North Carolina and Georgia. Consistent with prior research, we excluded non-singleton infants (V31–V39) and, among infants diagnosed with NAS, infants with potential iatrogenic drug withdrawal due to conditions known to require opioid therapy including intraventricular hemorrhage (772.10–772.14), periventricular leukomalacia (779.7), neocrotizing enterocolitis (777.50–777.53), spontaneous intestinal perforation (777.6), and bronchopumonary dysplasia (770.7) as we were interested in outcomes among infants with in-utero substance exposure (Uebel et al., 2015; Witt et al., 2017).
Measures
Prenatal substance exposure
We identified prenatal substance exposure using International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) codes from hospital discharge records. Consistent with previous research (Okoroh et al., 2017; Pan & Yi, 2013; Prindle et al., 2018), we defined prenatal substance exposure as a diagnosis of NAS (779.5) or a diagnosis of alcohol (760.71), narcotic (760.72), hallucinogen (760.73), or cocaine (760.75) exposure via placenta or breastmilk. Among infants with one of these ICD-9-CM codes, we included only infants who received a diagnosis of prenatal substance exposure during the early neonatal period (i.e., within 7 days of birth) as we were primarily interested in outcomes among infants with known substance exposure at birth. Thus, we excluded infants who first received a diagnoses of prenatal substance exposure more than 7 days after birth (N = 162).
Injury, maltreatment, and developmental disorder diagnoses
We identified inpatient and outpatient diagnoses for injury, maltreatment, and developmental disorders prior to age 12 months using ICD-9-CM codes from hospital discharge and outpatient records (i.e., office visits, emergency department admissions). Types of injury, maltreatment, and developmental disorder diagnoses and corresponding ICD-9-CM codes, as well as the prevalence of each code among our study population, are provided in Supplemental Table 1. We excluded outcomes occurring on the date of birth to exclude outcomes, such as clavicle and extremity fractures, that may have been directly related to the delivery. In addition, we excluded outcomes occurring during the early neonatal period (i.e., within 7 days of birth) to exclude diagnoses, particularly maltreatment, that may have been based solely on the fact that the infant was identified as having been exposed to substances prenatally.
We examined outcomes prior to age 12 months as this allowed us to follow five birth cohorts (2006–2010 births) for a uniform 12 month period. In addition, the first year of life is a vulnerable period for experiencing maltreatment (Wildeman et al., 2014), and injuries occurring prior to age 12 months (Sheets et al., 2013) may be indicative of potential risk for future abuse. Last, an in-depth understanding of injury, maltreatment, and developmental disorder diagnoses prior to age 12 months provides information on wellbeing early in the life course, allowing for effective tailoring of intervention and prevention strategies to promote optimal developmental trajectories.
Statistical Analysis
We examined infant characteristics, including sex, race/ethnicity, gestational age (<37 weeks vs. ≥37 weeks completed gestation), and birthweight (<1,500 g vs. ≥1,500 g) by substance exposure status using chi-square or Fisher’s exact tests. As the Medicaid MAX files are not linked for mother-infant dyads, we did not examine maternal demographics.
We calculated cumulative incidence functions and 95% confidence intervals (CIs) for injury, maltreatment, and developmental disorder diagnoses received prior to age 12 months among infants with and without prenatal substance exposure using a competing risk approach and nonparametric estimators. We compared cumulative incidence functions stratified by infant prenatal substance exposure using Gray’s test (Gray, 1988). In these analyses, time at risk began 8 days after birth, due to exclusion of outcomes occurring in the early neonatal period, and ended on the date of the first injury, maltreatment, or developmental disorder diagnosis, respectively, or on the infant’s first birthday if the infant did not experience these outcomes. We identified infants who died, infants with gaps in Medicaid or CHIP enrollment, and infants with a Medicaid eligibility code indicating foster care placement prior to their first birthday and treated the date of death, first enrollment gap, or first foster care placement as a competing risk. For enrollment and foster care placement, we used a monthly indictor of Medicaid or CHIP enrollment and monthly Medicaid eligibility codes to identify gaps in enrollment and infants who were eligible for Medicaid due to foster care placement. We removed these infants from the study population on the first day of the first month in which they were no longer enrolled in Medicaid or CHIP or in which their eligibility code indicated foster care status. We treated the first gap in Medicaid enrollment as a competing risk to exclude infants from our population “at risk” during a time in which we would not be able to observe diagnoses for injury, maltreatment, and developmental disorders in the Medicaid data. We treated foster care placement as a competing risk as a change in the infant’s caregiving environment may alter their risk for injury, maltreatment, and developmental disorders.
We used chi-square or Fisher’s exact tests to compare the prevalence of the most common types (N = 5) of injury, maltreatment, and developmental disorder diagnoses received among substance exposed and unexposed infants prior to age 12 months. In examining the prevalence of these diagnoses, we did not limit to only the first diagnosis, but examined all diagnoses prior to age 12 months. For example, if an infant received a diagnosis of neglect 60 days after birth and a subsequent diagnosis of physical abuse 120 days after birth, this infant would be counted in both the neglect and physical abuse diagnosis categories. As we were interested in the number of infants with different types of diagnoses, if an infant received two diagnoses for neglect prior to age 12 months, for example, this infant would be counted in the neglect diagnosis category once.
We conducted sensitivity analyses to examine the robustness of results to various assumptions (Supplemental Tables 2–7). We conducted analyses examining NAS (Supplemental Table 2) and substance exposure via placenta or breastmilk (Supplemental Table 3) as separate exposure groups to determine whether the incidence of outcomes differed by the presence of withdrawal symptoms. We conducted analyses excluding infants with other (760.70) and unspecified (760.79) substance exposure via placenta or breastmilk from the unexposed comparison group (Supplemental Table 4) as it is unknown what types of substances these infants may have been exposed to prenatally. We also conducted analyses restricted to infants with continuous Medicaid or CHIP enrollment through age 12 months (Supplemental Table 5). In addition, we conducted analyses excluding preterm and very low birthweight infants to exclude infants who may already be at increased risk for morbidity, including our outcomes of interest (Supplemental Table 6). Because most outcomes were diagnosed in an outpatient setting, we conducted analyses restricted to outpatient diagnoses only (Supplemental Table 7). We did not conduct analyses restricted to inpatient diagnoses only as the number of diagnoses was small (i.e., <15) for all outcomes among substance exposed infants. Last, we conducted analyses stratified by state of birth (Supplemental Tables 8–10) to determine whether results differed by state.
All analyses were conducted in SAS 9.4. This study was reviewed and approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill.
Results
There were 1,943,748 infants born in 2006–2010 in North Carolina (N = 381,159; 19.7%), Georgia (N = 497,202; 25.7%), and Texas (N = 1,065,387; 54.6%) who met study eligibility criteria, representing approximately 9% of all U.S. live births in this time period (Table 1). A total of 0.4% (N = 8,434) of infants received a diagnosis of prenatal substance exposure. Among infants with prenatal substance exposure, the most common exposures were cocaine (45.1%) and NAS (30.9%; Table 2). From 2006 to 2010, the prevalence of NAS diagnoses (19.5% in 2006 to 49.0% in 2010) and narcotic exposure (8.5% in 2006 to 16.4% in 2010) increased while the prevalence of cocaine exposure decreased (59.8% in 2006 to 20.8% in 2010), with a test for a linear trend indicating that changes in the prevalence of NAS diagnoses and narcotic and cocaine exposure over time were statistically significant (p < 0.0001).
Characteristics of Substance Exposed and Unexposed Infants, 2006–2010 Birthsa.

a North Carolina, Georgia, and Texas Medicaid and Children’s Health Insurance Program enrolled infants; 2010 births for North Carolina and Georgia only.
Type of Prenatal Substance Exposure Among Substance Exposed Infants by Year, 2006-2010 Birthsa.

a North Carolina, Georgia, and Texas Medicaid and Children’s Health Insurance Program enrolled infants; 2010 births for North Carolina and Georgia only.
The cumulative incidence of maltreatment (1.2% vs. 0.2%) and developmental disorder (10.7% vs. 1.5%) diagnoses prior to age 12 months was significantly higher among infants with prenatal substance exposure compared to their unexposed counterparts (Table 3). In contrast, the cumulative incidence of injury diagnoses prior to age 12 months (3.7% vs. 3.4%) was similar for infants with and without prenatal substance exposure. Substance exposed infants were younger in age at their first injury (median 189 vs. 235 days; p < 0.0001), maltreatment (median 112 vs. 147 days; p = 0.0066), and developmental disorder (median 123 vs. 197 days; p < 0.0001) diagnosis compared to unexposed infants.
Cumulative Incidence of Injury, Maltreatment, and Developmental Disorder Diagnoses Prior to Age 12 Months, 2006–2010 Birthsa.
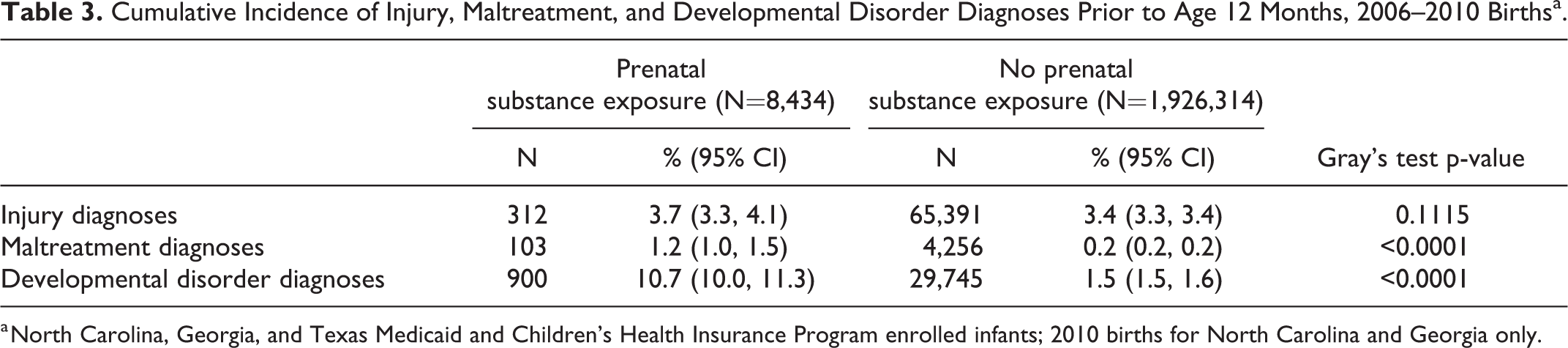
a North Carolina, Georgia, and Texas Medicaid and Children’s Health Insurance Program enrolled infants; 2010 births for North Carolina and Georgia only.
There were differences in the types and prevalence of specific injury, maltreatment, and developmental disorder diagnoses received by substance exposed and unexposed infants prior to age 12 months (Tables 4 –6). Among substance exposed and unexposed infants with an injury diagnosis, the most common diagnoses were poisoning (28.5% and 23.9%, respectively), extremity injuries (27.0% and 29.5%), head injuries (16.4% and 17.9%), and falls (13.1% and 15.8%). Among substance exposed infants with a maltreatment diagnosis, the most common diagnoses were neglect (37.9%) and other abuse or neglect (31.1%). Among unexposed infants with a maltreatment diagnosis, the most common maltreatment diagnoses were for physical abuse (51.4%) and unspecified abuse (24.4%). Among substance exposed and unexposed infants with a developmental disorder diagnosis, the most common diagnosis was an unspecified delay in development (76.4% and 72.5%, respectively).
Types of Injury Among Infants with Injury Diagnosesa Prior to Age 12 Months, 2006–2010 Births.b
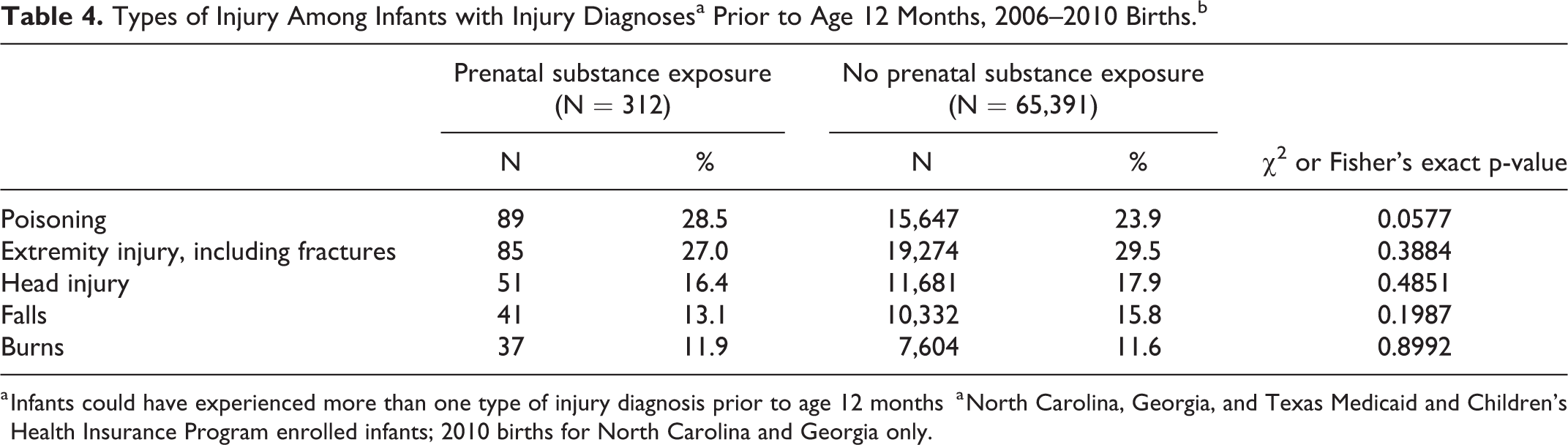
a Infants could have experienced more than one type of injury diagnosis prior to age 12 months
a North Carolina, Georgia, and Texas Medicaid and Children’s Health Insurance Program enrolled infants; 2010 births for North Carolina and Georgia only.
Types of Maltreatment Among Infants with Maltreatment Diagnosesa Prior to age 12 Months, 2006–2010 Births.b
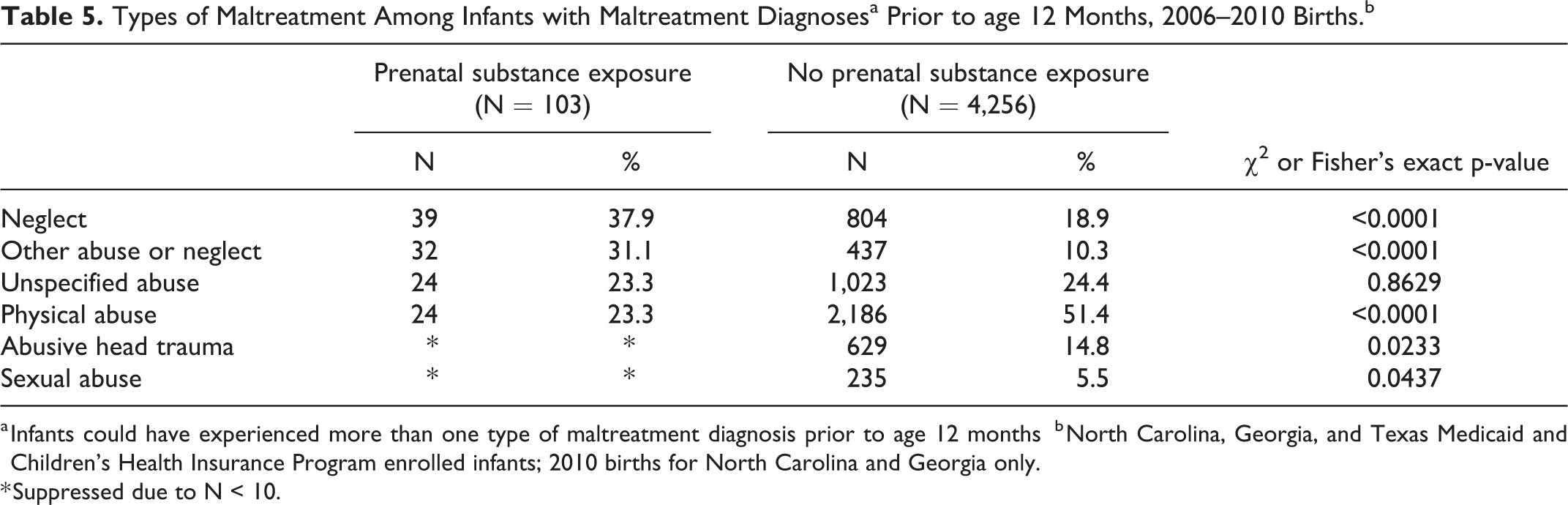
a Infants could have experienced more than one type of maltreatment diagnosis prior to age 12 months
b North Carolina, Georgia, and Texas Medicaid and Children’s Health Insurance Program enrolled infants; 2010 births for North Carolina and Georgia only.
* Suppressed due to N < 10.
Types of Developmental Disorders Among Infants with Developmental Disorder Diagnosesaa Prior to age 12 Months, 2006-2010 Birthsb.
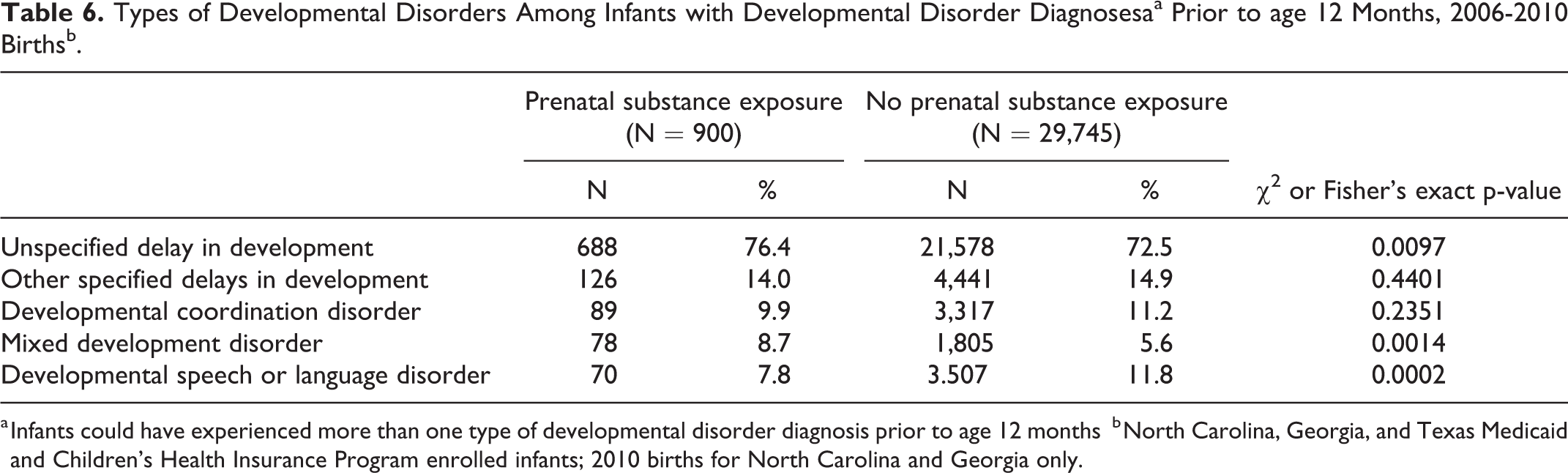
a Infants could have experienced more than one type of developmental disorder diagnosis prior to age 12 months
b North Carolina, Georgia, and Texas Medicaid and Children’s Health Insurance Program enrolled infants; 2010 births for North Carolina and Georgia only.
Overall, results from sensitivity analyses were unchanged from primary analyses. In each sensitivity analysis, the cumulative incidence of maltreatment and developmental disorder diagnoses prior to age 12 months was significantly higher among substance exposed compared to unexposed infants, and the cumulative incidence of injury diagnoses prior to age 12 months was similar for exposed and unexposed infants (Supplemental Tables 2–10). There were some subtle differences in the cumulative incidence of the outcomes by state (Supplemental Tables 9–10). The incidence of diagnoses for injury and maltreatment were slightly lower among Texas births compared to North Carolina and Georgia births and the incidence of diagnoses for developmental disorders was slightly lower among Georgia births compared to North Carolina and Texas births. However, results comparing the cumulative incidence of these outcomes among substance exposed and unexposed infants in each state were similar.
Discussion
To inform the provision of effective programmatic and policy intervention for substance exposed infants, a comprehensive understanding of clinical outcomes in the first year of life is important. Given recent changes in federal legislation requiring states to create a law or program to address the needs of substance exposed infants, knowledge of infant outcomes prior to these legislative changes is key to establishing a baseline of risk. This baseline can be used to inform the development of state-level policies and programs and to monitor their effectiveness in improving outcomes among substance exposed infants. In a population of Medicaid or CHIP enrolled infants, we found a significantly higher incidence of inpatient and outpatient diagnoses for maltreatment and developmental disorders, but not injury, prior to age 12 months among infants with prenatal substance exposure compared to their unexposed counterparts. We observed differences in specific types of injury, maltreatment, and developmental disorder diagnoses among exposed and unexposed infants.
Our results demonstrating a higher incidence of maltreatment diagnoses among substance exposed infants compared to their unexposed counterparts are consistent with prior research. Prior studies document an increased risk of hospitalization for maltreatment up to age 13 years (Uebel et al., 2015) and for injuries inflicted by other persons, including abuse and neglect, prior to age five years (Witt et al., 2017) among infants with NAS compared to non-NAS infants. Our results confirm that this finding is not limited to maltreatment diagnosed in an inpatient setting, which may reflect more severe cases than those diagnosed in an outpatient setting, or only to substance exposed infants with withdrawal symptoms. In addition, our results extend previous findings by examining the types of maltreatment diagnoses received among substance exposed and unexposed infants. Notably, we found that infants with prenatal substance exposure were more likely to receive a diagnosis of neglect and other abuse and neglect compared to unexposed infants. Unexposed infants were more likely to receive diagnoses for physical abuse, abusive head trauma, and sexual abuse compared to exposed infants. To further examine potential risk for and early indicators of physical harm, we conducted post-hoc analyses to examine infants’ history of injury occurring prior to maltreatment diagnoses. Previous research shows that children with confirmed abuse are more likely to have experienced a previous injury compared to children who did not experience abuse (Sheets et al., 2013). We found that, among infants with maltreatment diagnoses, prior injuries were more common among unexposed (24.2%) compared to substance exposed infants (6.8%). Overall, these results suggest a potentially lower risk for physical harm, but greater risk for neglect, among substance exposed compared to unexposed infants, prior to enactment of the CARA legislation.
There are several potential explanations for the higher incidence of maltreatment diagnoses, particularly neglect, among substance exposed infants. Previous research indicates that substance use during pregnancy is associated with demonstrated risk factors for neglect including maternal depression and poverty (Austin & Shanahan, 2017; Dubowitz et al., 2011; Holden et al., 2012; May & Gossage, 2011; McCabe & Arndt, 2012; van Gelder et al., 2010). Additional studies suggest that maternal substance use adversely impacts parenting behaviors, with substance using mothers demonstrating less warmth, responsiveness, and engagement than non-using mothers, potentially increasing the risk of infant neglect (Romanowicz et al., 2019; Slesnick et al., 2014; Solis et al., 2012). However, there may also be bias among healthcare providers toward substance exposed infants and their caregivers. It may be that, given similar conditions, substance exposed infants are more likely to receive a diagnosis for neglect than their unexposed counterparts (Freisthler et al., 2017; Howell, 2008; Lane et al., 2002; Wood et al., 2010). A previous study found that given the same surrounding circumstances, child welfare caseworkers were more likely to substantiate neglect when parental substance use was present (Freisthler et al., 2017).
Our results showing a higher incidence of developmental disorder diagnoses among substance exposed compared to unexposed infants is also consistent with prior research. A previous study found an increased risk of hospitalization for mental and behavioral disorders prior to age 13 years among infants with NAS compared to non-NAS infants (Uebel et al., 2015). Existing evidence suggests that prenatal substance exposure can affect fetal and infant neuro-development, resulting in deficits in learning, attention, and motor skills (Nygaard et al., 2016; Ornoy et al., 2010; Thompson et al., 2009). In addition, maternal substance use can adversely impact parenting behaviors, potentially leading to a caregiving environment that may contribute to developmental delays among infants (Romanowicz et al., 2019; Slesnick et al., 2014; Solis et al., 2012). Most developmental disorder diagnoses among infants with and without prenatal substance exposure were for unspecified delays in development, though the overall prevalence was significantly higher among substance exposed compared to unexposed infants. In addition to reflecting true developmental delays, it is possible that diagnoses for unspecified delays are to ensure that infants and caregivers are eligible for clinical and community services. For example, in Georgia, children <3 years are eligible for early intervention services if they have a diagnosed physical or mental condition known to result in developmental delays (e.g., Down syndrome) or have a diagnosed developmental delay (Georgia Department of Public Health, 2019). Given the likelihood of multiple social and economic stressors among families of substance exposed infants (Austin & Shanahan, 2017; May & Gossage, 2011; van Gelder et al., 2010), providers may be particularly aware of the need for these types of services and assign an unspecified developmental disorder diagnosis accordingly.
Results indicating a similar incidence of inpatient and outpatient injury diagnoses among infants with and without prenatal substance exposure align with a previous study that did not find an increased risk of hospitalization for injury or poisoning prior to age five years among NAS compared to non-NAS infants (Witt et al., 2017). While the overall incidence of injury diagnoses was similar, we observed some differences in the prevalence of specific types of injury diagnoses among substance exposed and unexposed infants. Poisoning was the most common type of injury diagnosis among both infants with and without prenatal substance exposure. However, the prevalence of poisoning was slightly higher among substance exposed compared to unexposed infants. In post-hoc analyses, we found that a higher percent of poisonings among substance exposed infants were due to alcohol or other drugs compared to those among unexposed infants (47.2% vs 26.1%), potentially reflecting a greater availability of alcohol and other drugs in the homes of infants whose mothers used substances prenatally (Finkelstein et al., 2017). The median age at poisoning diagnosis among substance exposed infants (median = 183 days) indicates that many of these infants may have been mobile at the time of the poisoning and potentially ingested an improperly stored substance. This underscores the need for continued safe medication storage education to caregivers as well as a need for increased implementation of passive safety features that do not rely on caregivers to cap and safely store medications or other substances after use (Lovegrove et al., 2014).
Limitations
Results should be interpreted in light of several limitations. First, we used administrative claims data to identify infants with prenatal substance exposure. Prenatal substance exposure may be under-identified in administrative data sources (Burns & Mattick, 2007). In North Carolina, Georgia, and Texas, healthcare providers are not required by law to test for prenatal substance exposure if substance use in pregnancy is suspected (Guttmacher Institute, 2019). Moreover, policies and protocols for screening pregnant women for substance use disorders and conducting maternal and infant toxicology tests vary by hospital within states (Jarlenski et al., 2017; Kerker et al., 2004; Wood et al., 2017). Thus, it is possible that some infants with prenatal substance exposure were not diagnosed. If some infants with prenatal substance exposure were not diagnosed and therefore included in our unexposed group, our results may have been biased toward the null. However, if only the most severe cases of prenatal substance exposure were diagnosed, and these infants were at greater risk for our outcomes, our results may have been biased away from the null. Second, data were specific to Medicaid or CHIP enrolled infants, potentially limiting generalizability to infants with other forms of health insurance. However, Medicaid finances more than half of all births in the U.S., and recent data indicate that Medicaid finances more than 80% of NAS-related births, underscoring the importance of examining outcomes among Medicaid or CHIP enrolled infants (Patrick et al., 2012). Third, data were specific to three Southern states, potentially limiting the generalizability to other states. Fourth, we did not have data regarding maternal demographics and mental health or substance use disorder diagnoses, which may be potential confounders in the association of prenatal substance exposure with our outcomes. However, regardless of whether the associations observed are causal, our results underscore the increased risk of various clinical outcomes, diagnosed both in the inpatient and outpatient setting, among substance exposed infants and provide additional nuance regarding the most common types of injury, maltreatment, and developmental disorder diagnoses received among substance exposed infants.
Conclusions
Our results provide an important perspective on clinical outcomes among substance exposed infants prior to recent changes in federal legislation. The results suggest a need for monitoring and intervention by medical and public health professionals (Campbell et al., 2010) as part of state-specific responses to the CARA legislation to address the risk of maltreatment, specifically neglect, developmental disorders, and poisoning among substance exposed infants during the first year of life. Future research is needed to evaluate the impact of state-specific policies and procedures on early outcomes among substance exposed infants.
Supplemental Material
Supplemental Material, Supplemental_File_12-18-19 - Incidence of Injury, Maltreatment, and Developmental Disorders Among Substance Exposed Infants
Supplemental Material, Supplemental_File_12-18-19 for Incidence of Injury, Maltreatment, and Developmental Disorders Among Substance Exposed Infants by Anna E. Austin, Molly Curtin Berkoff and Meghan E. Shanahan in Child Maltreatment
Footnotes
Acknowledgment
The database infrastructure used for this project was funded by the Department of Health Policy and Management, UNC Gillings School of Global Public Health; the Cecil G. Sheps Center for Health Services Research, UNC; the CER Strategic Initiative of UNC’s Clinical & Translational Science Award (UL1TR001111); and the UNC School of Medicine.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.