
Abstract
This study aimed to examine the relationship between exposure to childhood sexual abuse (CSA) and the occurrence of mental illness in adulthood in Nigeria. An age- and gender-matched case–control study was conducted in the University of Port Harcourt Teaching Hospital, Nigeria, from January to March 2014. Cases were defined as individuals aged 18 to 60 years diagnosed with mental illness while controls were aged 18 to 60 years who did not have mental illness. The study had 304 subjects comprised of 152 case–control pairs. This case–control study showed a statistically significant association between exposure to CSA and occurrence of mental illness in adulthood (pair-matched odds ratio = 3.25, 95% CI = [1.70, 6.21]). The association between CSA and mental illness was still significant (adjusted odds ratio = 3.11, 95% CI = [1.67, 5.82]) after controlling for family functionality. A robust CSA prevention and treatment strategy that considers the victim and the perpetrator in Nigeria is hereby advocated. This could be achieved by the collaborative efforts of the government of Nigeria and non-governmental organizations.
Introduction
Childhood sexual abuse (CSA) is a major public health problem with negative lifelong consequences for the well-being of the victims (World Health Organization [WHO], 2014). CSA is a global health and human rights issue that has been largely under-reported and under-studied in Nigeria (Abdulkadir et al., 2011) and sub-Saharan Africa (Bowman & Brundige, 2014). Noteworthy, the concept of sexuality in the traditional African society has been shrouded in secrecy, with cultural mores against reporting CSA (Bowman & Brundige, 2014; Lalor, 2004). Therefore, the cases reported represent only a “tip of the iceberg” (Abdulkadir et al., 2011). Also, the stigma, fear of being blamed, and a desire to keep the abuse secret make disclosure uncommon (Fontes & Plummer, 2010; Goodman-Brown, Edelstein, Goodman, Jones, & Gordon, 2003; Lalor, 2004).
The WHO consultation on child abuse prevention defines CSA as
the involvement of a child in sexual activity that he or she does not fully comprehend, unable to give consent to, or for which the child is not developmentally prepared and cannot give consent, or that violates the laws or social taboos of society. (WHO, 2006, p. 10)
It further states that this may include but is not limited to “the inducement or coercion of a child to engage in any unlawful sexual activity, the exploitative use of a child in prostitution or other unlawful sexual practices and the exploitative use of children in pornographic performance and materials” (WHO, 2006, p. 10). This definition captures all forms of CSA, both penetrative and non-penetrative.
In Nigeria, there is no clearly elaborate CSA definition in the national legislation. However, Section 34 of the 1999 Constitution prohibits all forms of torture, inhuman or degrading treatment, and slavery, forced, or compulsory labor and ensures the child’s right to dignity of his or her person (Federal Republic of Nigeria, 1999). The Child Rights Act (CRA) of the Federal Republic of Nigeria (2003) defines a child as a person who has not attained the age of 18 years. Thus, the age consideration of less than 18 years is used in defining CSA.
CSA has attracted much interest in the past two decades worldwide mainly due to the increasing research revealing its serious mental health sequelae for victims (Li, Ahmed, & Zabin, 2012). However, there is a dearth of studies on this problem in sub-Saharan Africa, especially in Nigeria, as the few available studies center simply on CSA prevalence (Audu, Geidam, & Jarma, 2009; Ikechebelu, Udigwe, Ezechukwu, Ndinechi, & Joe-Ikechebelu, 2009; Obisesan, Adeyemo, & Onifade, 1999; Ogunyemi, 2000; Olley, 2008) and perception (Ige & Fawole, 2011; Nuhu & Nuhu, 2010). Interestingly, these studies have shown that CSA is not uncommon in Nigeria, with 2.1% (Obisesan et al., 1999) being the lowest reported prevalence rate while the highest reported rate was 77.7% (Audu et al., 2009). This wide disparity could be explained by the dissimilarities in the study populations and CSA definitions employed.
The CSA prevalence of 2.1% was reported in a community-based study that was limited to the penetrative form of CSA (Obisesan et al., 1999). Another community-based study by Ogunyemi (2000), which captured both penetrative and non-penetrative forms of CSA, reported higher prevalence rates of 38% and 28% among female and male respondents, respectively. However, a much higher prevalence rate of 55% was reported in a school-based study by Olley (2008), which also captured both forms of CSA. This high prevalence rate reported among schoolchildren may be attributed to the poor supervision and low CSA perception by parents/guardians (Ige & Fawole, 2011). Noteworthy, very high prevalence rates of 60.9% (Ikechebelu et al., 2009) and 77.7% (Audu et al., 2009), have also been reported in Nigeria among female hawkers (street vendors of food and common household items). These very high rates may not be surprising as female hawkers are more vulnerable to all forms of abuse (Akpan & Oluwabamide, 2010).
Although studies in non-African nations (Baboolal et al., 2007; Chen et al., 2014; Cutajar et al., 2010; Li et al., 2012; MacMillan et al., 2001; Spinhoven et al., 2010) have reported an association between CSA and mental illness in later life, there is a need to elucidate such association in an African setting due to the socio-cultural differences, which could influence the perception and response to traumatic events such as CSA. A striking socio-cultural difference is the communal nature in Nigeria and most African settings, which is believed to promote resilience to life’s traumatic experiences (Muhammad, 2010). This could possibly decrease the odds of mental health problems among victims in such settings. However, it is worth noting that within the context of current globalization trends, the potential for the gradual erosion of such traditional African values remains glaring. This is evidenced by the influence of mass media and Internet, which could alter the African traditional values over time. The recent influx of cable satellite television networks into the Nigerian media space has widened the horizon for viewers. Therefore, there is a tendency for modeling of lifestyles according to cultures that could be described as foreign to most of the populace.
Another socio-cultural difference is the tendency for secrecy regarding CSA. Most African settings do not promote early disclosure (Abdulkadir et al., 2011; Lalor, 2004). The cultural practice in these settings is to extol the virtue of a virgin bride, and a court case would thus publicize the victim’s violation and bring shame (Okonkwo & Ibeh, 2003). The absence of early disclosure of CSA following occurrence makes it impossible for victims to seek early psychological assistance, thus increasing their odds of experiencing mental illness in adulthood (O’Leary, Coohey, & Easton, 2010).
The poverty in Nigeria and sub-Saharan Africa could also contribute to socio-cultural differences. The National Bureau of Statistics (NBS; 2010) reported that 60.9% of the Nigerian population live in absolute poverty. Remarkably, the presence of poverty has been identified as a trigger for mental illness (Funk, Drew, & Knapp, 2012). The general prevalence of mental illness among the Nigerian population is 20% (Mental Health Leadership and Advocacy Programme, 2012). Bryant-Davis, Ullman, Tsong, Tillman, and Smith (2010) noted that the occurrence of CSA in low resource setting could increase the vulnerability of such victims to suffer from mental illness. It is therefore possible that the poverty in Nigeria could contribute to the burden of mental illness.
In examining any association between CSA and mental illness, the possible confounding aspect of family functionality needs to be considered (Li et al., 2012). Family functions refer to the processes by which the family operates as a whole, including communication (Mosby’s Medical Dictionary, 2009) and the ability to adapt to new situations and manage conflicts (Vera et al., 2015). The role of family functionality is therefore an important factor when considering the long-term effects of CSA. A dysfunctional family setting may affect the level of support received following the CSA experience and could increase the risk of subsequent abuse as well as psychological disturbance in adulthood (Cecil & Matson, 2001). Alternatively, a functional family setting, independent of life stressors, could foster positive psychological adjustment (Draucker, 1997).
The current study aimed to determine the relationship between exposure to CSA and the occurrence of mental illness in adulthood. Furthermore, the study also examined the role of family functionality on any observed association between CSA and mental illness. The research set out to test the null hypothesis, which states that exposure to CSA is not significantly associated with the occurrence of mental illness in adulthood in the Nigerian setting.
Method
Site of Study
The study was carried out in Nigeria, located within the West African region. The Federal Republic of Nigeria consists of 36 states and the Federal Capital Territory. Specifically, this study was done in Rivers State, Southern part of Nigeria, West Africa. It is among the states that constitute the Oil Producing Niger-Delta region and had a total population of 5,198,176 people by the 2006 census (NBS, 2013). This hospital-based study was carried out in the mental health and the general out-patient clinics of the University of Port Harcourt Teaching Hospital in Rivers State between January and March, 2014. These clinics operate on week days with an average weekly patient turnover of 80 and 900, respectively.
Participants
This matched case–control study had a total of 304 participants, comprised of 152 cases and 152 controls. This was based on the sample size calculation for case–control studies (Kasiulevičius, Šapoka, & Filipavičiūtė, 2006). It was computed at 95% confidence level, power of 80%, minimum odds ratio of two, and a CSA prevalence of 38% from a Nigerian study by Ogunyemi (2000). The age range of the 304 participants was 18 to 57 years. The mean age and standard deviation (SD) for cases and controls were 32.3 ± 8.8 years and 32.6 ± 8.6 years, respectively (see Table 1).
Socio-Demographic Characteristics of Cases and Controls.
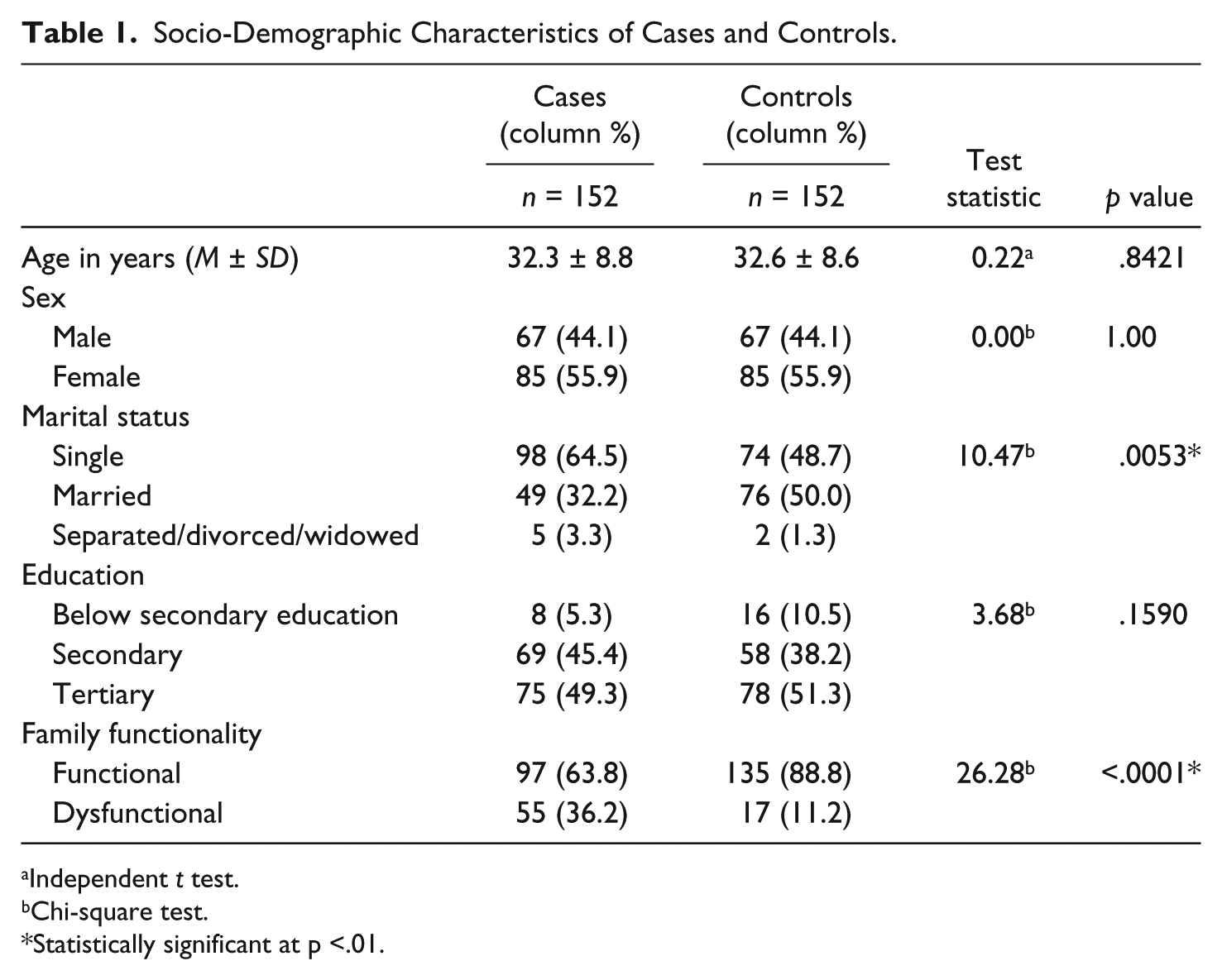
Independent t test.
Chi-square test.
Statistically significant at p <.01.
Cases
The cases were recruited from the mental health clinic of the University of Port Harcourt Teaching Hospital using systematic sampling. The cases were defined as individuals aged 18 to 60 years who were diagnosed with mental illness by the attending psychiatrist according to the ICD-10 Classification of Mental and Behavioral Disorders. The following exclusion criteria were applied: individuals with history of mental illness originating in childhood because of the study’s interest in examining the relationship between CSA and the occurrence of mental illness in adulthood, individuals who were severely disturbed and not in touch with reality thus unable to respond to the study questionnaire, or individuals with memory impairment due to the retrospective recall method of assessing CSA exposure in this study. The cases were comprised of 85 females and 67 males. The mean ages and SD (years) for the females and males were 33.5 ± 8.7 and 31.1 ± 8.8, respectively.
Controls
The controls were recruited from the general out-patient clinic of the University of Port Harcourt Teaching Hospital based on individual matching technique of 1:1 for sex and age ± 3 years. The controls were individuals aged 18 to 60 years who had no known mental illness. Individuals who were too ill to respond to the questionnaire were excluded. To ensure that the controls had no mental illness, the General Health Questionnaire (GHQ-12), which is a tool for screening psychiatric morbidity, was used. Similar to the cases, the controls consisted of a total of 85 females and 67 males because of the 1:1 matching for sex. The mean ages and SD in years for females and males were 33.6 ± 8.8 and 31.6 ± 8.8, respectively.
Materials
CSA exposure
This was assessed using a content-validated self-administered questionnaire on childhood sexual abuse adapted from Halperin et al. (1996). This questionnaire captured all forms of CSA as outlined in the WHO definition. CSA exposure was defined by an affirmative response of “yes” to exposure to any of the following experiences perpetrated by an adult during childhood: sexual touching, child pornography, photographing child’s naked body, sexual intercourse, and insertion of fingers/objects in child’s genitals.
Mental illness
The diagnosis of mental illness for each of the cases was made by the attending psychiatrist. The controls, which consisted of attendees of the general out-patient clinic, were screened for mental illness using the GHQ-12 to ensure the absence of mental illness. The GHQ-12 is a self-administered questionnaire, widely validated and found to be reliable with Cronbach’s alpha between .8 and .94 (Glozah & Pevalin, 2015; Molina, Rodrigo, Losilla, & Vives, 2014; Romppel, Braehler, Roth, & Glaesmer, 2013). It consists of 12 items, each with four answer options rated on a scoring of 0-0-1-1. It has been used in Nigeria, and a total GHQ-12 score of 3 or more on this instrument indicates psychiatric morbidity (Coker, 2014).
Family functionality
Family functionality was assessed using the Family APGAR (Adaptation, Partnership, Growth, Affection and Resolve) questionnaire. It is a five-item validated scale of family functionality with Cronbach’s alpha of .78 and .8 (Gómez-Bustamante, Castillo-Ávila, & Cogollo, 2013; Silva et al., 2014). It has been widely used in Nigeria to elicit the level of emotional, communication, and social interactive relationships between the respondents and their families (Muyibi, Ajayi, Irabor, & Ladipo, 2010; Shittu et al., 2014). It consists of scores of 0 (hardly ever), 1 (sometimes), and 2 (almost always). The total score ranges from 0 to 10. The total score on the family APGAR scale is categorized into functional family (7-10 points) and dysfunctional family (0-6 points).
Procedure
Ethical approval was granted by the ethical committee of the University of Port Harcourt Teaching Hospital before proceeding with the study. Informed consent was obtained from all participants before inclusion into the study. The cases were first selected by systematic sampling, after which eligibility criteria were applied. The controls were recruited from the general out-patient clinic based on the matching criteria of 1:1 for sex and age ± 3 years. The GHQ-12 was administered to the controls and only those with total GHQ-12 score of less than 3 continued in the study. The respondents with GHQ-12 scores of ≥3 were attended to by the family physicians in the general out-patient clinic of the hospital. The normal referral practice of the hospital still applied in the case of need for referral to the mental health clinic. The eligible participants were given the study questionnaires, comprised of the questionnaire on CSA and Family APGAR. After completion of the questionnaires, the participants were requested to drop them in the box provided to ensure confidentiality. Anonymity was maintained by the use of research numbers.
Data entry and analysis were done using the EPI Info Version 7 statistical package designed by the Centers for Disease Control and Prevention (CDC). Socio-demographic variables (age, sex, marital status, educational level, and family functionality) of cases and controls were presented as means and proportions as appropriate. Chi-square tests were used to test for differences in proportion while independent t tests were used for differences in means. The data on exposure to CSA and outcome of mental illness were presented in tabular form reflecting the paired matching and showing the concordant and discordant pairs. McNemar’s chi-square test was used to test for differences in the proportions among the pairs, while a matched odds ratio was used to determine the strength of association between exposure to CSA and outcome of mental illness in adult life. The categories of mental illness were compared among CSA exposed and unexposed cases. Conditional logistic regression was used to investigate the confounding effect of family functionality. The level of statistical significance was set at p < .05.
Results
This hospital-based case control study revealed that the socio-demographic characteristics of the cases were not statistically significantly different from the controls except for marital status (p = .0053) and family functionality (p = .0001), as shown in Table 1.
The prevalence of CSA in the entire sample (N = 304) was 21.4% (n = 65). Among the cases (n = 152), the CSA prevalence was 29.6% (n = 45), while for the controls (n = 152) it was 13.2% (n = 20). Twenty-seven out of the 45 cases exposed to CSA were females, giving a proportion of 60%. Similarly, in the controls, 11 of the 20 controls exposed to CSA were females, giving a proportion of 55%. Thus the proportion of CSA was higher in females in both the cases and controls.
Table 2 shows the different forms of CSA occurring among the cases and controls who were exposed to CSA. Penetrative CSA was reported in 40% (n = 18) of the cases and 50% (n = 10) of the controls. This difference was not statistically significant (p = .4524).
Forms of CSA Among Cases and Controls Exposed to CSA.
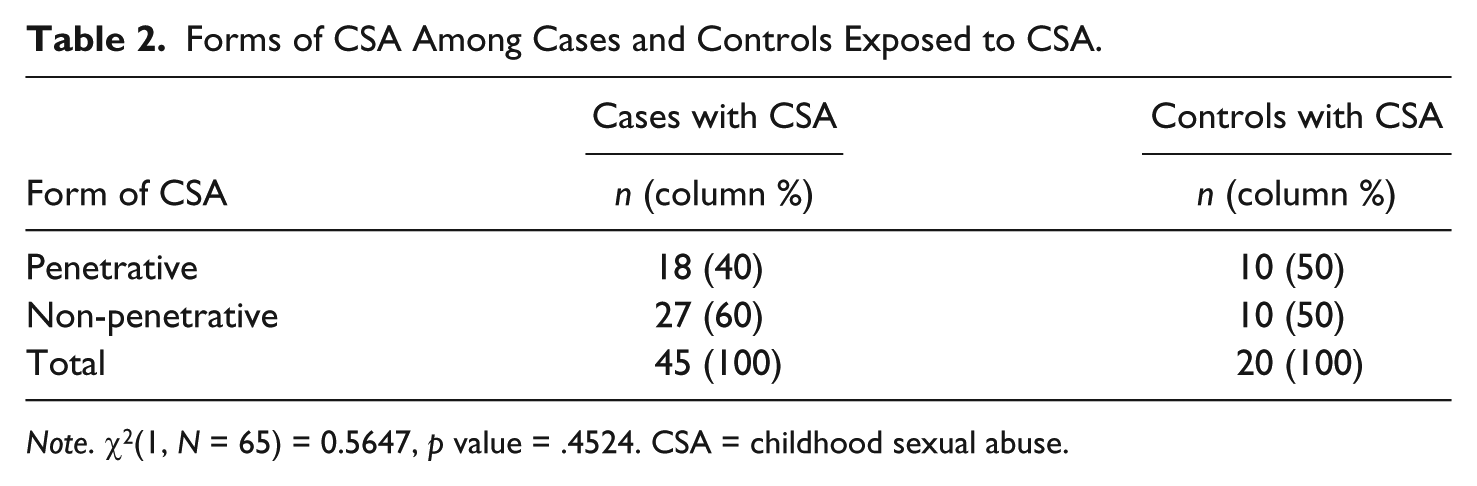
Note. χ2(1, N = 65) = 0.5647, p value = .4524. CSA = childhood sexual abuse.
As a result of the individual matching of controls to cases in 1:1, there were 152 case–control pairs. The proportion of exposure to CSA was higher among the adults with mental illness (i.e., the cases; 46 out of the 152 case–control pairs) than among the adults with no mental illness (i.e., the controls; 19 out of the 152 case–control pairs). This difference was statistically significant (p = .00016). The study showed that the odds of the occurrence of mental illness in adulthood was about 3 times greater among those exposed to CSA than those not exposed (matched-pair odds ratio = 3.25, 95% CI = [1.7, 6.2]; see Table 3).
CSA Exposure Among Case–Control Pairs.
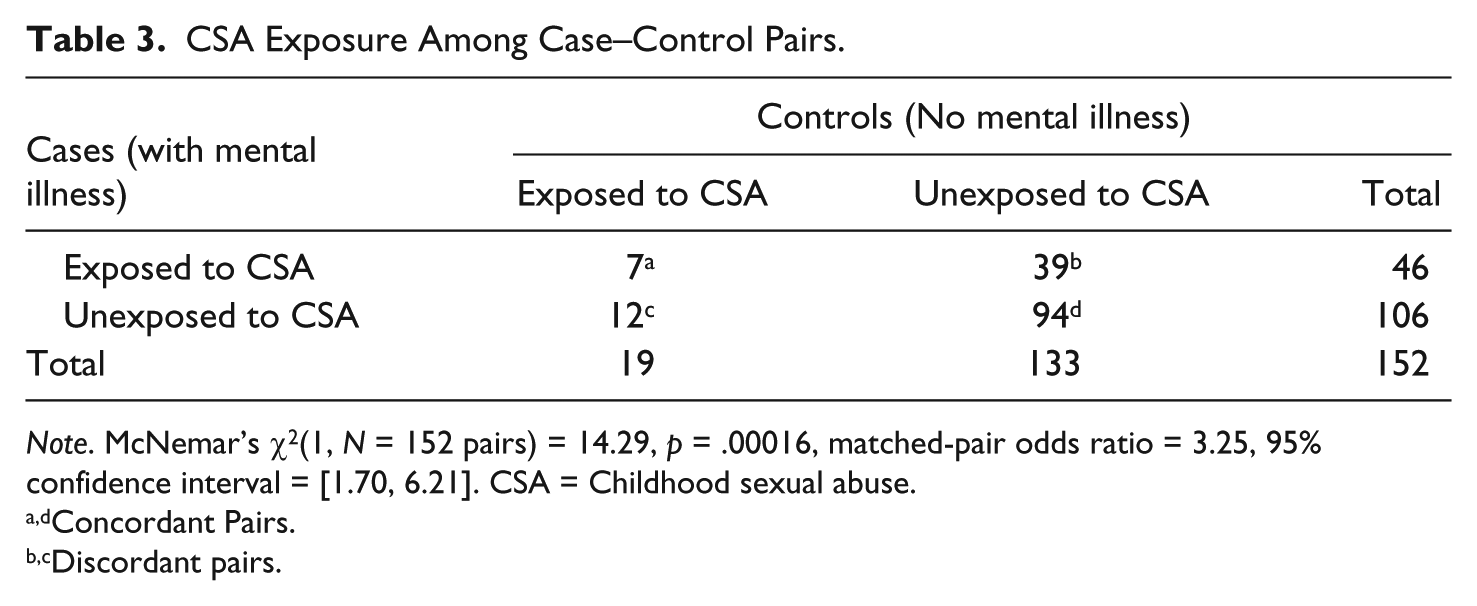
Note. McNemar’s χ2(1, N = 152 pairs) = 14.29, p = .00016, matched-pair odds ratio = 3.25, 95% confidence interval = [1.70, 6.21]. CSA = Childhood sexual abuse.
Concordant Pairs.
Discordant pairs.
The comparison of the categories of mental illnesses between the CSA exposed and unexposed cases showed that depressive disorders had the highest prevalence among the CSA exposed cases (35.6%, n = 16), while schizophrenia and other related psychotic disorders had the highest prevalence in the cases not exposed to CSA (27.2%, n = 29; see Table 4). The differences in the proportions of the various categories of mental illness occurring in CSA exposed and unexposed cases were not statistically significant (p = .1567).
Categories of Mental Illnesses Among CSA Exposed and Unexposed Cases.
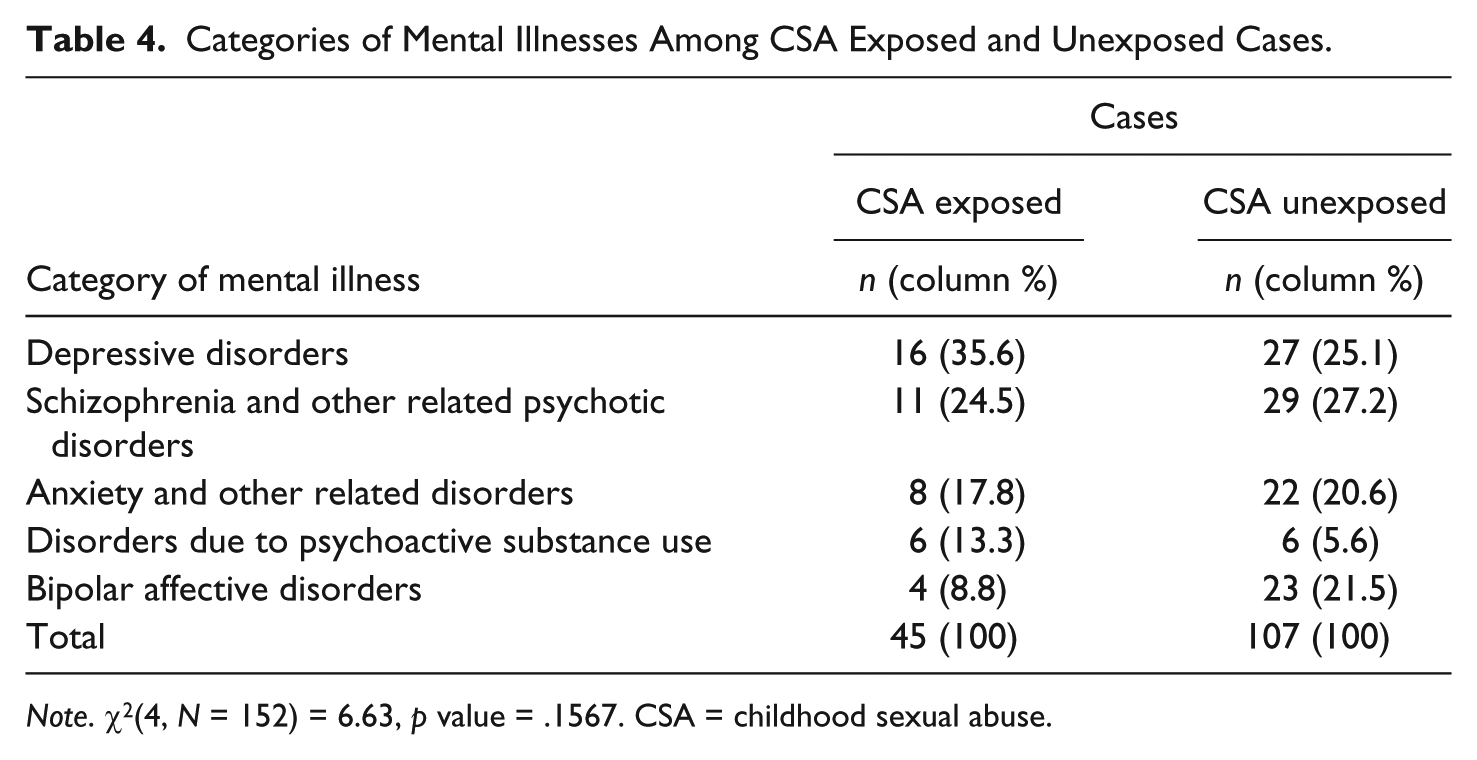
Note. χ2(4, N = 152) = 6.63, p value = .1567. CSA = childhood sexual abuse.
Table 3 illustrates that CSA is significantly associated with mental illness in adulthood. Thus, to exclude the possible confounding effects of family functionality, a conditional logistic regression analysis was performed. The association between CSA and mental illness in adulthood was still significant after controlling for family functionality (adjusted odds ratio = 3.11, 95% CI = [1.67, 5.82]; see Table 5). The logistic regression model also revealed that the odds of the occurrence of mental illness in adulthood was about 4 times higher among participants from the dysfunctional family than the functional family (adjusted odds ratio = 4.02, 95% CI = [2.16, 7.49]).
Conditional Logistic Regression Model of Mental Illness in Adulthood (Dependent Variable) With Covariates of CSA, Family Functionality, and Marital Status.
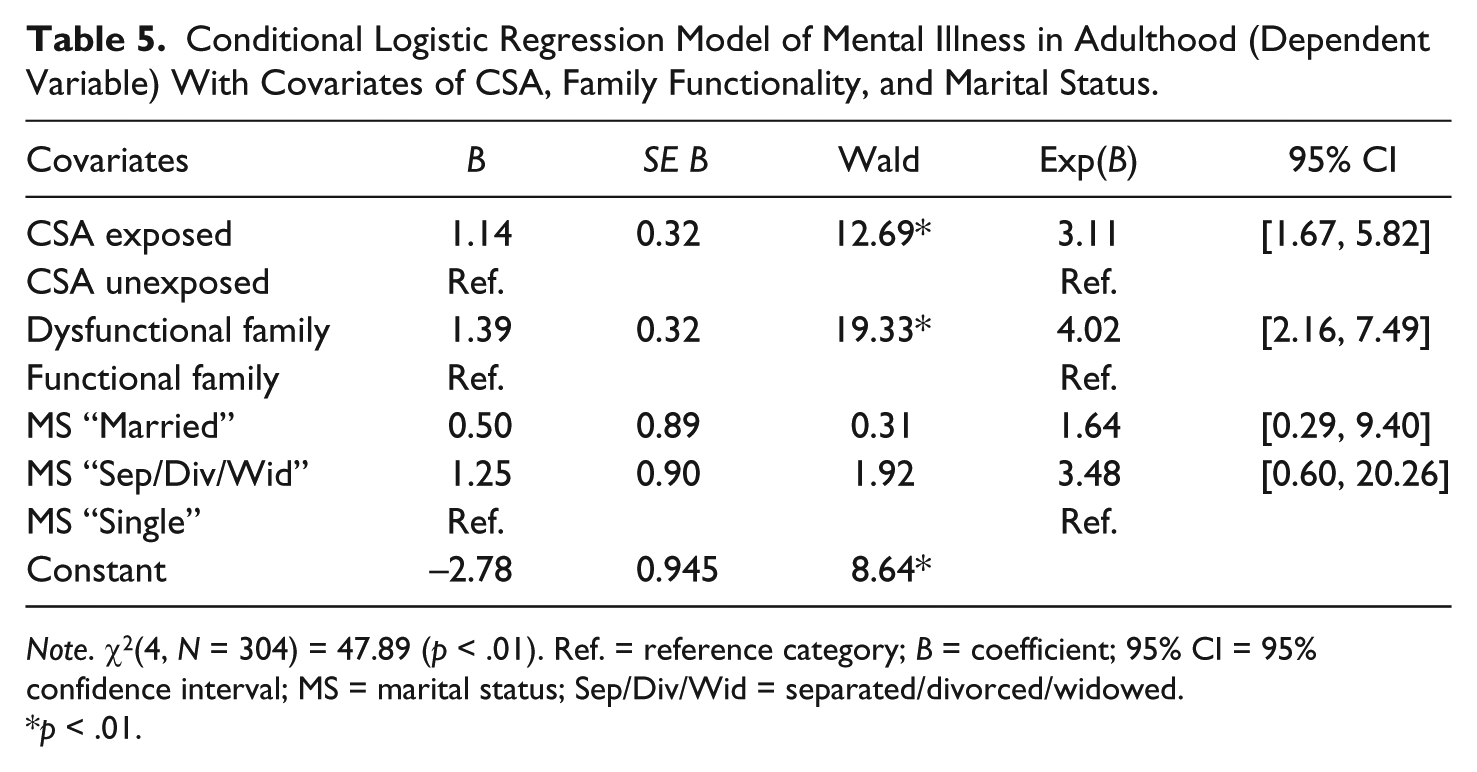
Note. χ2(4, N = 304) = 47.89 (p < .01). Ref. = reference category; B = coefficient; 95% CI = 95% confidence interval; MS = marital status; Sep/Div/Wid = separated/divorced/widowed.
p < .01.
Discussion
This study, along with other studies (Lalor, 2004; Ogunyemi, 2000; Olley, 2008), has shown that CSA is not uncommon in sub-Saharan Africa. It further challenges the general notion that CSA does not exist due to acclaimed cultural beliefs that regard sex as sacred, thus abhorring all forms of sexual misconduct in the society (Lalor, 2004).
Our finding of a significant association between exposure to CSA and mental illness in adult life, is in keeping with similar studies carried out in Canada (MacMillan et al., 2001), New Zealand (Fergusson, McLeod, & Horwood, 2013), Netherlands (Spinhoven et al., 2010), and China (Chen et al., 2014). The odds of the occurrence of mental illness in adult life was 3 times higher (odds ratio of 3.25) among those exposed to CSA than those not exposed. The odds ratio reported in this study is comparable with a similar study in China by Chen et al. (2014). However, lower odds ratios were reported by Baboolal et al. (2007), MacMillan et al. (2001), and Cheasty, Clare, and Collins (1998). These studies were carried out in developed nations. In such nations, the presence of anonymous help lines, call-in-centers, and social support networks may promote early CSA disclosure. Victims, therefore, benefit from immediate mental health care, consequently decreasing their risk of mental illness in later life. In contrast to the setting of the current research, in which adults reported past CSA, children exposed to abuse may scarcely make a disclosure due to the fear of being doubted or blamed, as well as the stigma and shame brought to the family (Lalor, 2004). The absence of early disclosure forestalls the needed interventions for such victims, thus increasing their risk of having mental illness in later life. Furthermore, the absence or non-implementation of laws against CSA as well as the non-existence of organized treatment services for CSA perpetrators in most African settings could make early disclosure an illusion. It is therefore imperative that appropriate laws regarding CSA are enacted and enforced in these settings.
In Nigeria, the CRA (2003) prohibits all forms of abuse against children. However, progress toward the implementation of the CRA has been sluggish. The basis of the Nigerian legal system is multifaceted in nature, with roots from English common law, cultural customs, and Sharia law (Gwangndi, 2016; Ojo, 2014). Therefore, discrepancies and inconsistencies emanating from these plural legal frameworks may pose a challenge to the implementation and interpretation of the CRA (Akinwumi, 2010; Ojo, 2014). Although a considerable number of states within the Federal Republic of Nigeria have incorporated the CRA into their state laws, most of these states have not yet implemented these laws in accordance with the provisions of the act (Chinda, 2016). The CRA is classified under the residual list by section 4 (7) of the Constitution of the Federal Republic of Nigeria (1999), giving the states the discretion to make laws that relate to specific issues within their jurisdiction. Culture and beliefs have been a challenge to the implementation of the CRA. Some of these beliefs oppose the dictates of the CRA; for instance, some states in the country uphold that a girl child should be married off before the age of 18, or as soon as she attains puberty (Chinda, 2016). However, Section 21 of the CRA (2003) defines a child as a person below the age of 18 years and objects to early child marriage or betrothal. Some states thus view this provision as contrary to their culture, customs, and religion (Chinda, 2016). These states, mostly within the northwestern and northeastern geopolitical zones of Nigeria, have yet to sign the CRA into their state laws. Notably, the Sharia penal code as a legal system is operational in 12 states of northern Nigeria (Nwauche, 2014).
In addition, there is an absence of family courts in most states of the Federal Republic of Nigeria. The CRA holds that cases relating to children are to be adjudicated in family courts established in accordance with its provisions at the high court and magistrate court levels (CRA, 2003). It also provides for the establishment of Child Rights Implementation Committees at the state level. The lack of these provisions in most states of the federation has contributed to the slow pace of effective implementation and enforcement of the CRA, even in states that have incorporated the CRA.
Civil Society Organizations (CSOs) act as a driving force for the implementation of laws in Nigeria. They serve as the voice of the public in relating to the legislative arm of the government and are also involved in widespread campaigns to achieve the desired result. Although the activities of these organizations have assisted in sensitizing the government and the populace about the CRA, their activities need to be formalized to ensure the proper implementation of this act. The current research advocates increasing awareness about CSA in Nigeria and the need to protect children from CSA through implementation of laws such as the CRA.
Also, the non-enforcement of the CRA has been attributed to non-existence of complaints of violations of the provisions of the act (Ojo, 2014). This may stem from ignorance about such provisions in the law. Hence there is need to translate the CRA into Nigerian local languages as a way of dissemination. Efforts should also be made to reach out to religious and community leaders, as they are important for effective mobilization of citizens to protect children from the menace of CSA. The government should also give adequate budgetary allocations to relevant agencies directly linked to the protection of the rights of the children.
Apart from the enactment of relevant laws against CSA, treatment centers must also be available for victims to curb the effects of CSA. Organized setups solely dedicated to the treatment of CSA victims are scarce in Nigeria. These treatment centers could be located within the tertiary hospital(s) in each state, as these institutions are likely to have adequate capacity in terms of staff and infrastructure. Furthermore, there is also need to establish anonymous help lines, call-in-centers, and social networks, which could all be integrated with treatment centers. These allow for early detection and appropriate treatment of victims. Another need is for treatment services for perpetrators of CSA. Sadly, this dimension is missing in Nigeria and probably most parts of Africa. This could be attributed to the focus on only punishment for perpetrators. Appropriate treatment in the form of more intensive aftercare programs for perpetrators has been associated with the reduction of recidivism rates (James, Stams, Asscher, De Roo, & van der Laan, 2013). The treatment of CSA perpetrators can contribute to sexual abuse prevention efforts by reducing their tendencies to engage in such act. Hence, it is necessary to ensure that adequate capacity and infrastructure to provide services for the treatment of perpetrators is put in place within and outside the reformatory facilities in Nigeria.
The higher proportion of CSA among females in both the cases and controls of this study is in keeping with the studies by Baboolal et al. (2007), Chen et al. (2014), Abdulkadir et al. (2011), and Ogunyemi (2000), which all report that CSA occurs commonly among females. It is possible that early sexual maturation in girls may increase their vulnerability to sexual abuse (Mullen & Fergusson, 1999). Also, the vulnerability of females to sexual abuse has been attributed to the practice of engaging females as domestic servants in Nigeria and parts of Africa (Bugaje, Ogunrinde, & Faruk, 2012). However, Lalor (2004) postulates that the seemingly higher rates of CSA in females is due to the lack of CSA disclosure by males. Nonetheless, there is need for closer supervision of children of both sexes at the family level.
Concerning forms of CSA, we detected both penetrative and non-penetrative forms among both cases and controls. This is unlike a similar case control study by Cheasty et al. (1998) in which the penetrative form of abuse occurred only in the cases, thus linking penetrative abuse to mental illness. Also, similar studies by Baboolal et al. (2007) and Lee, Lyvers, and Edwards (2008) have reported statistically significant associations between the penetrative form of abuse and mental illness. Our results did not support this assertion. However, Briere and Elliott (2003) noted that all forms of sexual abuse affect the victim’s mental health.
Although, depressive disorders were most prevalent among those who experienced CSA, there was no statistically significant difference in the proportion of diagnostic categories of mental illness occurring between the CSA exposed and unexposed cases. This may indicate that CSA may not increase the risk for any particular category of mental illness. This is consistent with Maniglio (2009), who suggests that CSA should be considered as a general and non-specific risk factor for mental disorder.
The current study found that the association between CSA and mental illness diagnosis in adulthood was not due to the confounding effect of family functionality. This contrasts with Claussen and Crittenden (1991), who found that a history of CSA does not lead to greater vulnerability for mental illness in adulthood, but rather the confounding influence of family functionality does. However, more recent research has affirmed the non-confounding effect of family functionality on the association between CSA and mental illness (Fergusson et al., 2013; Li et al., 2012). This highlights the need for focus on measures that would prevent CSA to lessen the burden of the adult mental illness associated with it.
The hospital-based nature of this study may affect the generalizability of the findings. Hence, future studies using community- and population-based samples to examine the association between CSA and adult mental illness are needed. The recall of childhood experiences by adults may be prone to error due to the limitations in human memory; nonetheless, studies have demonstrated that the recall of major childhood experiences such as CSA has validity (Hardt & Rutter, 2004) even among patients with mental disorders (Applebaum, Nemets, Kaplan, Witztum, & Belmaker, 2012). Anonymity, confidentiality, and use of self-administered questionnaires employed in the current research were precautions to limit social desirability bias.
Conclusion
This study reveals an association between CSA and the occurrence of mental illness in adult life irrespective of the status of family functionality. In addition to increasing the body of knowledge on CSA and its mental health sequelae, this study also highlights the peculiarities of the Nigerian setting, which is similar to most African settings with regard to these issues. Public sensitization campaigns are crucial for raising awareness of CSA and the need for instituting appropriate preventive measures against this societal malady. Thus, the Nigerian CRA, which has hitherto been relatively moribund, needs to be enforced. In addition, CSA treatment services should be established in the different states of the Federal Republic of Nigeria in collaboration with non-governmental organizations. Furthermore, consideration should also be given to the initiation of programs that will offer appropriate treatment to perpetrators as this could contribute to a holistic approach to CSA prevention.
Footnotes
Acknowledgements
The authors are grateful to the Editor-in-Chief, Michael C. Seto, the Action Editor, Jill Stinson, the reviewers and the administrative staff of SAJRT for all their support and constructive criticisms that have enriched the content of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.