
Abstract
ADHD is a common mental health disorder prevalent in 5.3% of children and adolescents worldwide (Polanczyk, De Lima, Horta, Biederman, & Rohde, 2007). In addition to the core symptoms of inattention and/or hyperactivity-impulsivity, children with ADHD experience a range of academic, social, and behavioral impairments and high rates of comorbid mental health problems (e.g., depression, conduct disorder) all of which impact negatively on their schooling (Jensen & Steinhausen, 2015; Sciberras, Roos, & Efron, 2009; Zendarski, Sciberras, Mensah, & Hiscock, 2017).
Adolescents with ADHD experience greater academic adversities in comparison with typically developing students in early high school. Lower academic achievement on standardized tests, lower class grades, high academic risk (i.e., 40% below grade expectations), and high levels of suspension (20%-30%) have been reported (Zendarski et al., 2017), as well as increased homework and classroom behavior problems (Langberg et al., 2016). Academic risk is similar for both males and females with ADHD (Zendarski et al., 2017). Additional learning and support services are required to help students with ADHD and additional education needs adjust to high school and to support them to make academic progress.
A wide variation in rates of education support have previously been reported, from low use (27%) to relatively high use (70%) in children and adolescents with ADHD (Capriotti & Pfiffner, 2017; Murray et al., 2014; Sawyer et al., 2004). Inconsistencies may be partly attributed to the differing sample characteristics, which include specific ADHD-subtypes (Capriotti & Pfiffner, 2017), wide age-ranges (Sawyer et al., 2004), and the varied definition of supports and services ranging from tutors, counseling and to Individualized Educational Plans (IEPs) and 504 plans (learning accommodations and supports). A single study has examined educational support in high school students with ADHD (Murray et al., 2014). Rates of special education supports and other school-based services were examined for adolescents (n = 337) participating in the Multimodal Treatment Study of Children with ADHD (MTA) study when participants were in Grades 10 and 11 (average age = 16.7 years, SD = 0.95). Results showed 52% of students were accessing educational support delivered through formalized IEP or 504. They also accessed a range of other supports including case management (55%), mental health services (32%), vocational support (33%), and behavioral support (17%). It is worth noting that support rates in this sample may be elevated, due to the large proportion of students (35%) enrolled in special education settings (Murray et al., 2014), as in these setting IEPs and extra support are accessed by all students. Overall, rates of support use were not reported. No study to date has specifically examined educational support use for adolescents with ADHD in the important early adolescent period.
A number of factors have been associated with education support utilization in children with ADHD including poor academic achievement and high levels of child functional impairment (Capriotti & Pfiffner, 2017; Murray et al., 2014), as well as comorbid problems (Larson, Russ, Kahn, & Halfon, 2011; Sawyer et al., 2004). There is some evidence that increased ADHD symptom severity is associated with higher support use (Murray et al., 2014; Sawyer et al., 2004), although this relationship was not evident for children with a predominantly inattentive type ADHD (ADHD-I; Capriotti & Pfiffner, 2017). There also remain other factors that are likely to be important that have not been examined. For example, given additional educational supports are employed at the discretion of school principals and parents, provision may vary as a result of school and family characteristics such as school sector and location (Murray et al., 2014). Factors such as socioeconomic disadvantage, language and culture, and state government policy may influence access to services for students with ADHD. Understanding the factors that influence support use may inform future strategies to enhance education support for students with ADHD in early high school.
Student education and support services within Victorian schools include a range of services provided by allied health professionals including psychologists, speech pathologists, and social workers, as well as pastoral care services in religious schools. Supports will vary at each local school. Services are broad and not well defined but can include services provided to the students to address peer difficulties and social skills, academic support (e.g., math and literacy, homework help, speech therapy and occupational therapy, mentoring, and counseling), as well as disability support services (e.g., IEP) for students who meet criteria across seven disability categories, of which ADHD is not included (Department of Education & Training, 2018).
The current study examines the rates of educational support use and predictors of support use for Victorian students with ADHD in early adolescence. We aim to (a) describe educational support use for a cohort of adolescents with ADHD in early high school (M age = 13.7 years) and (b) compare the individual (e.g., academic risk), family (e.g., parent education), and school (e.g., sector) factors associated with support use versus no use over the previous 6 months. It is hypothesized that support use, in comparison with no support use, will be associated with more severe ADHD symptoms, academic risk status, and increased behavioral problems.
Method
Study Design and Participants
This study presents cross-sectional data obtained from the 3-year follow-up of a longitudinal study of school-age children with ADHD. Participants are students in the first and third year of high school in Australia (equivalent to middle school seventh grade and high school ninth grade in the United States), with a mean age of 13.7 years (SD = 1.1, range = 12-16 years; 89% male). Participants attended government (59%), Catholic (20%), independent (15%), and special education (6%) high schools in Victoria, Australia, and ranged in socioeconomic advantage (M SEIFA [Socio-Economic Indexes for Areas] scores = 1,011.2, SD = 67, range = 816-1,114; population M = 1,000, SD = 100). Ethics approval was obtained from the Human Research Ethics Committee of The Royal Children’s Hospital (#33206).
To be included in the 3-year follow-up, children were required to be aged 12 years or older, confirmed as having transitioned to high school, and had agreed to be approached about future research (n = 200), of which 130 (65%) enrolled. A comparison between participants and nonparticipants found no differences on baseline measures of child age, gender, ADHD symptoms, medication use, and socioeconomic status (SES). Children with a pediatrician diagnosis of ADHD were recruited (average age = 10.1 years, SD = 1.9). Diagnosis was confirmed by researchers against Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000), via parent-reported symptoms (off-medication) on the ADHD Rating Scale–IV (Dupaul, Power, Anastopoulos, & Reid, 1998) and specific questions to parents of the level of impairment, setting, and symptom duration. Other exclusion criteria included intellectual disability, having a severe medical condition (i.e., cerebral palsy), sleep apnea, and poor parent English skills. A detailed protocol is published elsewhere (Zendarski, Sciberras, Mensah, & Hiscock, 2016).
Procedures
The 3-year follow-up study was conducted in two waves (2014 and 2015). Consenting parents and adolescents took part in a face-to-face home visit. During the visits, a trained researcher conducted a direct assessment of the adolescent’s cognitive functioning and the adolescent completed a separate online survey about their daily school life, attitudes toward school, health, and behavior. Parents also completed a separate online survey about their adolescent’s school life, education support use, ADHD symptom severity, behavior, and family life. Surveys were collected from the participating adolescent’s homeroom teacher about their student’s school-based support and service use, classroom performance, and behavior.
Measures
Educational support was identified from the parent and teacher questionnaires that asked about supports used in the past year. The questions were study-designed based on similar study questions addressing education support in primary school-aged students with ADHD (Sciberras et al., 2013). Parents were asked whether their adolescent received any specialized education support to support their child’s additional learning needs (yes/no). If the parent marked “yes,” then they were asked to select which supports had been accessed in the past 6 months from a list including academic support, social support (e.g., well-being and social development), counseling, homework support, mentoring, speech therapy, occupational therapy, behavioral interventions, or other.
Teachers were asked whether their student received any additional school-based support or services (yes/no). If they answered yes, they were asked to select supports provided from a list including IEP (referred to as an individual learning plan in the Australian context), student support group (SSG) which is a group that monitors student learning and progress, disability funding, and other. Teachers who were not aware of the service use history of their student were given the option to select “don’t know.” Parent and teacher support use (yes/no) were combined and dichotomized into an educational support use (yes or no) indicator, which was set to yes if either the teacher or parent indicated use.
A range of adolescent, family, and school variables were examined in relation to support use; these are described in Table 1.
Explanatory Variables for Service Use.

Note. SDQ = Strengths and Difficulties Questionnaire; ASD = autism spectrum disorder; CD = conduct disorder; OCD = obsessive-compulsive disorder; NAPLAN = National Assessment Program–Literacy and Numeracy; NMS = national minimum standard; SES = socioeconomic status; SEIFA = Socio-Economic Indexes for Areas.
Statistical Analyses
Descriptive statistics were used to describe the participant characteristics. Students were grouped as having accessed additional educational support in the current school year (n = 78; 60%), or not (n = 52; 40%), based on parent- and/or teacher-reported support use in the current school year. Logistic regression was used to test for associations between support use (yes/no) and explanatory variables of interest which included individual, family, and school variables. All continuous explanatory variables were converted to SD units prior to analysis. Logistic regression models were rerun adjusting for potential confounding variables including adolescent age, gender, ADHD medication use, and SES (SEIFA). Odds ratios (ORs), 95% confidence intervals (95% CIs), and p values are reported. Analyses were conducted using Stata V.14.0.
Results
Overall, a total of 78 participants (60%) were reported by parents or teachers to have used a school-based support in the current school year. Figure 1 shows the proportion of the sample who were receiving specific educational supports. Parents reported that their adolescents used a range of additional educational supports, most commonly social, counseling, and mentoring, while IEPs and SSGs were the most common supports reported by teachers.
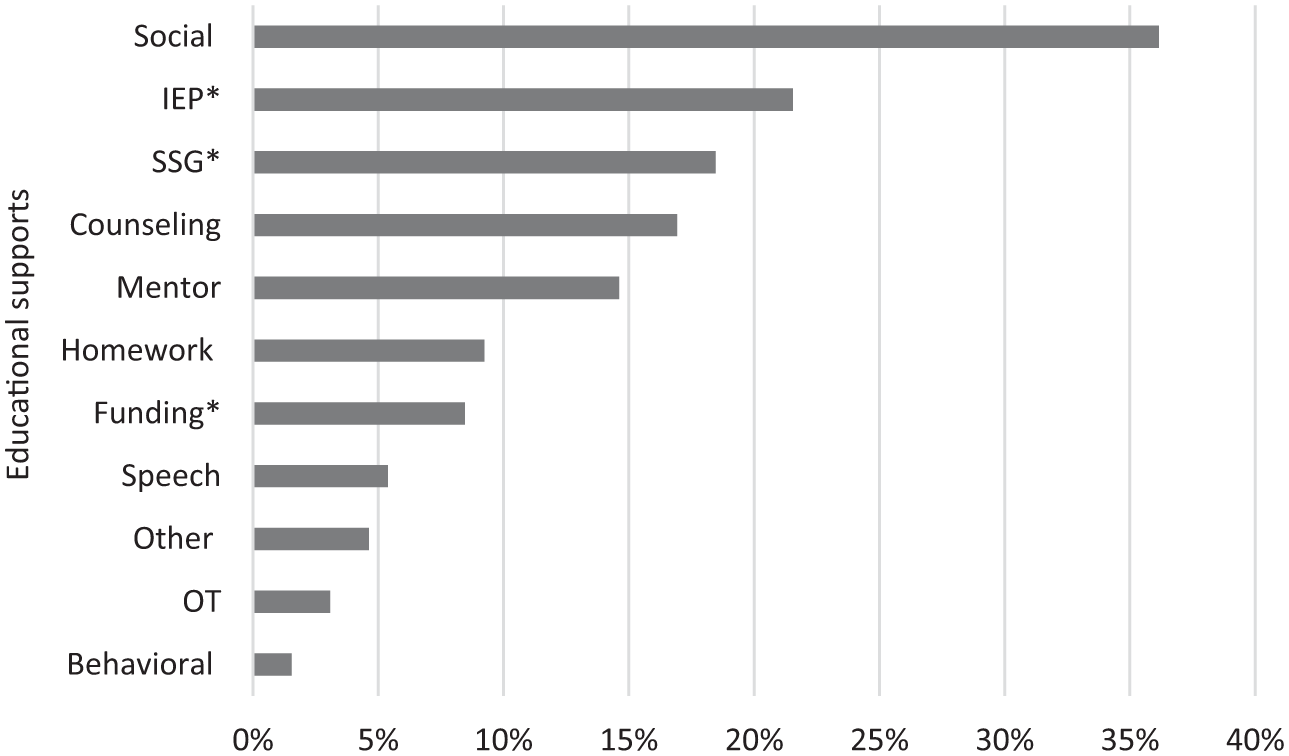
Participant (N = 130) educational support by support category.
Table 2 provides details of the adolescent, family, and school characteristics for the sample.
Characteristics of Participants.
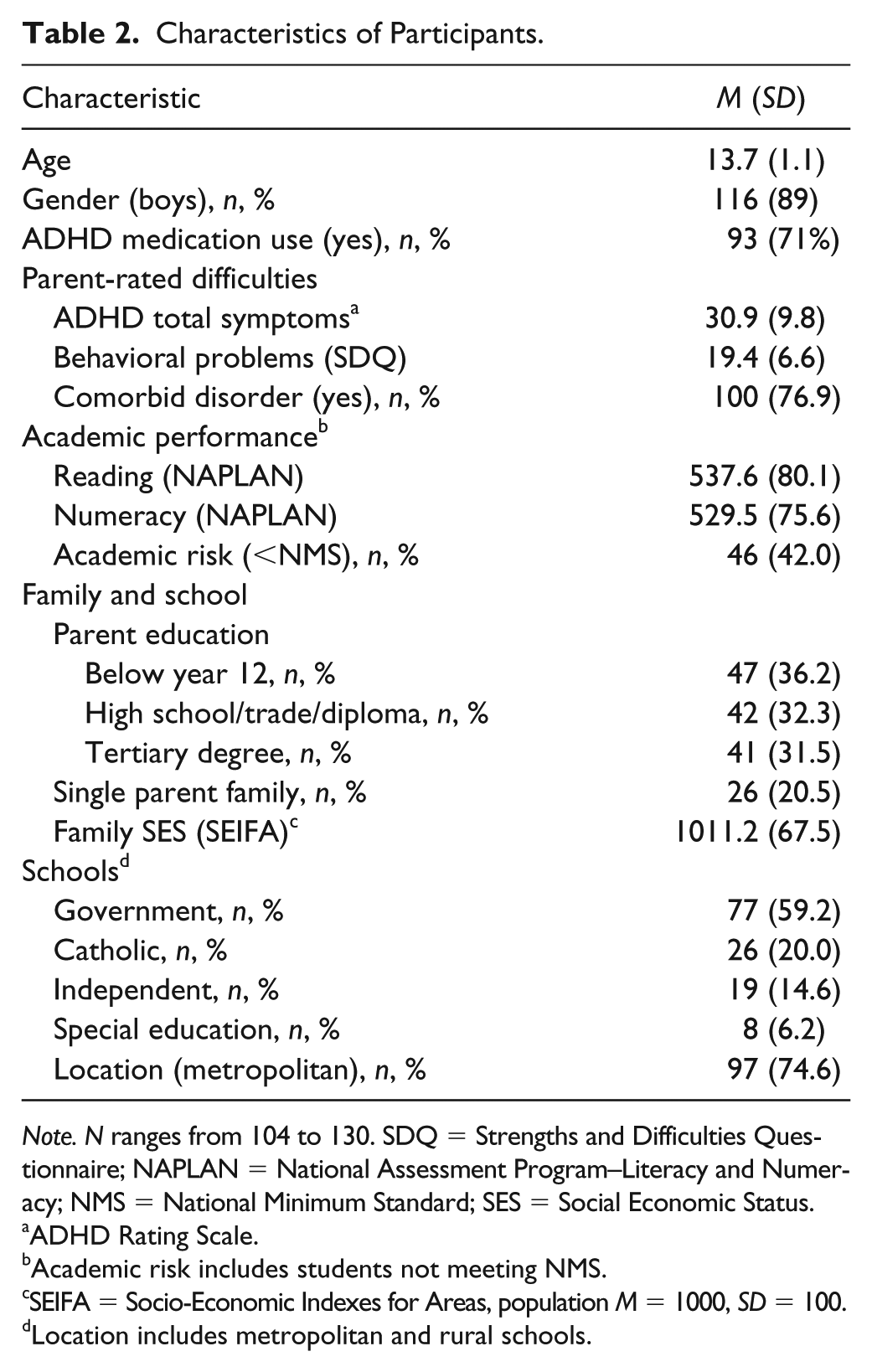
Note. N ranges from 104 to 130. SDQ = Strengths and Difficulties Questionnaire; NAPLAN = National Assessment Program–Literacy and Numeracy; NMS = National Minimum Standard; SES = Social Economic Status.
ADHD Rating Scale.
Academic risk includes students not meeting NMS.
SEIFA = Socio-Economic Indexes for Areas, population M = 1000, SD = 100.
Location includes metropolitan and rural schools.
Univariable and adjusted multivariable logistic regression results are shown in Table 3. Unadjusted results show a general trend toward higher support use for students with lower achievement, more severe ADHD symptoms, and poorer behavior and for students in the Catholic school sector. In the adjusted models, academic risk (OR = 2.30, 95% CI = [1.03, 5.14], p = .04), behavioral problems (OR = 1.47, 95% CI = [1.01, 2.14], p = .047), and attending a Catholic school (OR = 5.10, 95% CI = [1.59, 16.42], p = .006) were independent predictors of educational support.
Predictors of Educational Service Use Versus No Use, in Adolescents With ADHD.
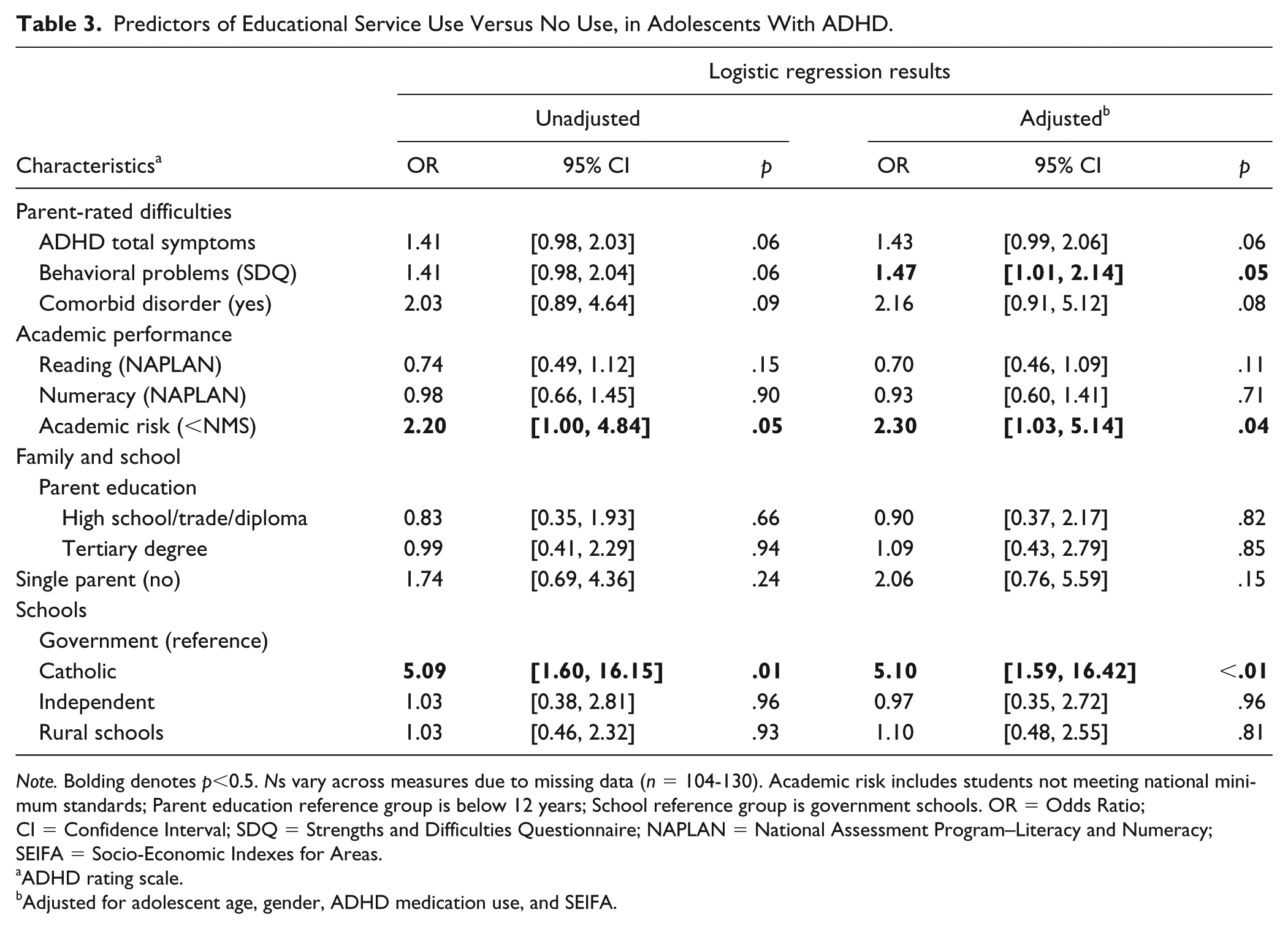
Note. Bolding denotes p<0.5. Ns vary across measures due to missing data (n = 104-130). Academic risk includes students not meeting national minimum standards; Parent education reference group is below 12 years; School reference group is government schools. OR = Odds Ratio; CI = Confidence Interval; SDQ = Strengths and Difficulties Questionnaire; NAPLAN = National Assessment Program–Literacy and Numeracy; SEIFA = Socio-Economic Indexes for Areas.
ADHD rating scale.
Adjusted for adolescent age, gender, ADHD medication use, and SEIFA.
Discussion
This study examined educational support for students with ADHD in early high school. We found that 60% of students were accessing additional educational support. Social and counseling services, as well as IEPs and SSGs were the main educational supports accessed. Academic risk (OR = 2.30, 95% CI = [1.03, 5.14], p = .04), behavioral problems OR = 1.47, 95% CI = [1.01, 2.14], p = .047) and attending a Catholic school (OR = 5.10, 95% CI = [1.59, 16.42], p < .01) predicted support use. However, a large proportion of students (40%) were not accessing support, some of whom (27.7%) were at academic risk.
Our educational support rates are on the higher end of rates previously reported for students with ADHD (Jensen et al., 2004; Murray et al., 2014). However, overall rates of particular supports (e.g., IEPs and SSGs) were much lower (28%) in comparison with the rate (52%) reported for the 337 high school students (Grades 10 and 11) with ADHD participating in the 8-year follow-up of the MTA study (Murray et al., 2014). It is worth noting that the differences between countries likely reflect different funding models and the fact that in this study only 6% of students were attending schools in special education settings compared with 36% in the MTA study. Outside of these specific academic supports, students accessed a range of psychosocial support including social support, counseling, and mentoring. Surprisingly, less than 10% students were accessing homework support, despite homework difficulties being widely reported for middle school and adolescents with ADHD and linked with poorer academic performance (Langberg et al., 2016). It is possible that students are not accessing these types of supports because they are not available in their school setting. Future research is needed to identify the antecedents to educational service use for students with ADHD.
We found that educational support was associated with increased academic risk (below the national minimum standard), which is consistent with previous findings (Capriotti & Pfiffner, 2017; Murray et al., 2014). While most at risk students (67%) were receiving additional support, only one in four received formal support in the school setting, for example, IEP or SSG. It may be that adolescents with substantial academic impairment also experience difficulties in other domains of functioning, for example, social support which need to be addressed in the school setting, but it is also likely there are unmet needs. Service use was also associated with increased adolescent behavioral problems. Behavioral problems have been linked with poor academic functioning and lower educational outcomes for children with ADHD (Sciberras et al., 2009). Poor classroom behavior can be disruptive and impede with learning. Our finding that service provision was substantially higher within the Catholic education system is novel. Students in the Catholic sector were 5 times more likely to access support compared with students in government schools. We speculate that this may reflect the Catholic school ethos and established pastoral care programs (Catholic Education Commission of Victoria, 2014). Support rates were similar for students in rural and metropolitan settings.
There are a number of limitations to this study. These data are cross-sectional and we report factors associated with education support only. The validity of the support data would have been improved if we were able to access the school records regarding the provision of school-based support and funding. However, privacy rules did not allow access to such data. Additional support data with regard to duration, cost, and satisfaction would provide a more detailed picture of educational support usage. We were unable to confirm diagnoses relating to parent-reported comorbidities. Finally, the small sample size limited our ability to conduct more complex analyses and results need replication.
Implications and Future Research
We know that the high school environment poses additional challenges for adolescents with ADHD and many will continue to experience academic, social, and behavioral problems that adversely impact their daily school lives (Barkley, 2006). Our research shows that more than half of these students are receiving at least some extra educational support. Future research needs to evaluate the efficacy of support provided. It would be valuable to examine in detail the range of individual accommodations being provided in the high school setting under the IEPs (i.e., extra time on tests, extended deadlines for long-term projects, note-taking accommodations). In addition, we need to understand why some students with considerable need are not accessing support, and finally to better understand the lack of equivalence in the provision of educational support between school sectors.
The current level of support may not be sufficient to improve academic and school functioning in students with ADHD. Presently, evidence-based academic or psychosocial intervention programs developed for students with ADHD are not being used within Australian high schools (Zendarski et al., 2017). In addition, finding interventions that provide lasting academic and social improvements in adolescents with ADHD is proving difficult (Hinshaw & Arnold, 2015). Some interventions that show promise include individualized learning support and help with organizational skills and homework (Evans, Langberg, Egan, & Molitor, 2014; Langberg et al., 2016; Schultz, Storer, Watabe, Sadler, & Evans, 2011). Tailored educational supports may be more beneficial to struggling students with ADHD.
In conclusion, our results show that a high proportion of participants in this study were accessing education support services. Academic risk and attending a Catholic school were the strongest independent predictors of education support use. Future research needs to establish whether these supports are meeting the individual student needs, and why some students who are at academic risk miss out on support at this important education juncture. More information is needed on the efficacy of services being utilized by adolescents with ADHD and how these services affect educational outcomes. This information is critical to help families and schools advocate for better education support.
Supplemental Material
Correlation_Matrix_Table_supplementary – Supplemental material for Factors Associated With Educational Support in Young Adolescents With ADHD
Supplemental material, Correlation_Matrix_Table_supplementary for Factors Associated With Educational Support in Young Adolescents With ADHD by Nardia Zendarski, Emma Sciberras, Fiona Mensah and Harriet Hiscock in Journal of Attention Disorders
Footnotes
Acknowledgements
The authors would like to acknowledge all research assistants and students who contributed to study. Thank you to the families, teachers, and schools for their participation in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by Murdoch Children’s Research Institute (MCRI), supported by the Victorian Government’s Operational Infrastructure Support Program. Dr. Zendarski is funded by a postdoctoral award from the Cripps Foundation. The Australian National Health and Medical Research Council funds Dr. Sciberras through a career development fellowship (CDF; No. 1110688), and Dr. Mensah (CDF No. 1037449 and 1111160) and Professor Hiscock’s position (CDF No. 607351).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.