
Abstract
Objective:
This study investigated subfactors of cognitive disengagement syndrome (CDS; previously referred as sluggish cognitive tempo) among adults referred for neuropsychological evaluation of attentiondeficit/hyperactivity disorder (ADHD).
Method:
Retrospective analyses of data from 164 outpatient neuropsychological evaluations examined associations between CDS subfactors and self-reported psychological symptoms and cognitive performance.
Results:
Factor analysis produced two distinct but positively correlated constructs: “Cognitive Complaints’’ and “Lethargy.” Both correlated positively with symptom reports (rs = 0.26–0.57). Cognitive Complaints correlated negatively with working memory, processing speed, and executive functioning performance (rs = −0.21 to −0.37), whereas Lethargy correlated negatively only with processing speed and executive functioning performance (rs = −0.26 to −0.42). Both predicted depression symptoms, but only Cognitive Complaints predicted inattention symptoms. Both subfactors demonstrated modest to nonsignificant associations with cognitive performance after accounting for estimated premorbid intelligence and inattention.
Conclusion:
Findings indicate a bidimensional conceptualization of CDS, with differential associations between its constituent subfactors, reported symptoms, and cognitive performance.
Introduction
Cognitive disengagement syndrome (CDS), previously referred to as sluggish cognitive tempo (SCT), describes a constellation of distinct inattention symptoms including mind-wandering, mental confusion, lethargy, and hypoactivity (Barkley, 2014; Cerny et al., 2023). The change in terminology from SCT to CDS reflects recent efforts to more accurately characterize the core features associated with the syndrome and avoid stigmatizing language attached to the original terminology (Barkley, 2014; Becker et al., 2023). The core features of CDS are theorized to comprise two primary domains: cognitive and motor. Cognitive features reflect disengagement from the individual’s present context, as exemplified by staring, daydreaming, mind-wandering, mental confusion, fogginess, withdrawal, and/or sleepy appearance, whereas motor features include hypoactivity, slow motor movement, lethargy, drowsiness, and/or prolonged sedentary periods (Barkley, 2014; Becker et al., 2023).
At the time of this writing, there are no specific diagnostic criteria for CDS in the Diagnostic and Statistical Manual for Mental Disorders (DSM-5-TR; American Psychiatric Association, 2022). Therefore, CDS is a syndrome, not an independent disorder (Barkley et al., 2022; Becker et al., 2023). Lack of diagnostic criteria and poor specificity of its core symptoms have contributed to challenges in the conceptualization and assessment of CDS. Originally, CDS was proposed to be an expression of the primarily inattentive presentation of attention-deficit/hyperactivity disorder (ADHD-I; e.g., Milich et al., 2001); however, factor analytic studies have revealed that CDS is distinct from ADHD in children and adults (Barkley, 2012, 2013; Becker et al., 2016; Jacobson et al., 2012; Penny et al., 2009). Still, clinically significant CDS co-occurs with ADHD diagnosis at rates ranging from 39% to 59% (Barkley, 2012, 2013, 2014; Becker et al., 2016; Jacobson et al., 2012; Penny et al., 2009).
External validation of CDS has revealed that CDS symptomatology is positively associated with ADHD-related inattentive symptoms, as well as symptoms of internalizing psychopathology. Therefore, CDS may be better understood as an internalizing rather than externalizing syndrome, particularly given that the symptoms of CDS often demonstrate negative associations with ADHD-related hyperactivity/impulsivity and other forms of externalizing psychiatric symptoms (Barkley, 2012; Becker, 2021; Becker et al., 2014, 2018, 2020, 2023; Kamradt et al., 2018; Nelson & Lovett, 2023; Z. R. Smith et al., 2019; J. N. Smith & Suhr, 2021; Wåhlstedt & Bohlin, 2010). Moreover, CDS symptoms are uniquely linked with self-reported negative functional outcomes in the domains of social, academic, household, employment, and general executive functioning after accounting for ADHD symptoms (Barkley, 2012; Becker et al., 2023; Flannery et al., 2016; Lunsford-Avery et al., 2021; J. N. Smith & Suhr, 2021; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017). However, research on the impact of CDS on objective measures of cognitive performance has been comparatively sparse. Among samples of children, CDS has been associated with broad deficits in the cognitive domains of attention, working memory, processing speed, and executive functions (Barkley et al., 2022; Becker et al., 2016, 2019, 2020; Creque & Willcutt, 2021; Tamm et al., 2023; Willcutt et al., 2014). Fewer studies have investigated the association between CDS and cognitive performance among adults, and those that have, generally found null to weak associations between CDS symptoms and objective cognitive performance (Cerny et al., 2023; Jarrett et al., 2017; J. N. Smith & Suhr, 2021; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017).
Most studies investigating the cognitive sequelae of CDS have done so using a unitary factor structure. However, several studies have demonstrated subfactors within the CDS construct, suggesting that investigations of CDS utilizing a unitary factor can obscure potential relationships that specific subfactors may have with cognitive functioning. Among pediatric samples, factor analytic studies of CDS have identified 2 to 3 subfactors indicative of daydreaming/sleepiness and lethargy/hypoactivity (Barkley, 2013; Jacobson et al., 2012; Penny et al., 2009). Barkley (2013) extracted two CDS symptom clusters: Sluggish, indicative of underactivity, lethargy, and slow motor movements, and Daydreaming, indicative of daydreaming, staring into space, and confusion. The two subfactors align with the broad motor and cognitive symptom domains outlined above and had modestly differential associations with self-reported executive functioning (Barkley, 2013). To our knowledge, only two studies have investigated the subfactors that comprise CDS in an adult population (Lunsford-Avery et al., 2021; J. N. Smith & Suhr, 2021). J. N. Smith and Suhr’s (2021) study’s identified three subfactors associated with CDS in an undergraduate volunteer sample: Cognitive Complaints, which was indicative of slow information processing and confusion; Daydreaming/Bored, indicative of daydreaming, poor alertness, spacing out/fogginess and boredom; and Lethargy, indicative of underactivity, slow movement, and lethargy. Further, Smith and Suhr’s study is the only one to evaluate the associations between these subfactors and objective neurocognitive test performance. The authors found that higher Daydreaming/Boredom symptoms predicted better working memory performance, while no CDS subfactors were significantly associated with processing speed or executive functioning performance. Similarly, another study by Lunsford-Avery et al. (2021) discovered three subfactors of CDS in an adult clinical sample referred for an outpatient ADHD evaluation: Slow/Daydreamy, reflecting confusion, spacing out/fogginess, slow information processing, and daydreaming; Sleepy/Sluggish, which was identical to J. N. Smith and Suhr’s (2021) Lethargy subfactor; and Low Initiation/Persistence, reflecting boredom and poor alertness. While the authors did not examine neuropsychological performance, they found that severity of CDS symptoms was positively associated with self-reported functional impairment across multiple domains after accounting for ADHD symptoms. The three factors extracted by Lunsford-Avery et al. (2021) were cross-validated an undergraduate volunteer sample by Nelson and Lovett (2023), who demonstrated differences in CDS subfactor symptom reporting across students with and without ADHD and co-occurring mood disorders. Moreover, Nelson and Lovett (2023) demonstrated a modest increase in clinical utility of utilizing a three-factor structure of CDS symptoms. Specifically, examining individual CDS factors demonstrated that only the Sleepy/Sluggish factor was associated with self-reported functional impairment after accounting for ADHD and internalizing symptoms.
The present study seeks to expand upon the findings reported by J. N. Smith and Suhr (2021), Lunsford-Avery et al. (2021), and Nelson and Lovett (2023) by examining the factor structure of CDS in an adult outpatient neuropsychiatric sample and investigating whether the identified factors can predict objective performance on measures of working memory, processing speed, and executive functioning performance, as well as self-reported symptoms of depression, anxiety, and inattention. Similar to J. N. Smith and Suhr (2021), this study controlled for the impact of estimated premorbid intelligence and inattention on cognitive performance and excluded individuals with invalid cognitive test performance. By expanding upon earlier studies, this study may provide a more comprehensive understanding of the subfactors that constitute CDS and their influence on neuropsychological functioning in adults.
Method
Participants
Data for this cross-sectional study were collected from a clinical sample of 586 consecutive adults referred for neuropsychological evaluation by treating medical or psychiatric providers for diagnostic clarification and treatment planning related to known or suspected ADHD at a Midwestern academic medical center. All patients provided written informed consent for inclusion of their neuropsychological test scores and demographic information in an IRB-approved database study. Patients were included in the study if they completed all measures of interest. The Barkley Adult ADHD Rating Scale-4th Edition (BAARS-IV; Barkley, 2011) was added to the uniform battery at a later date than other measures relevant to the study. As such, a total of 164 patients were administered the BAARS-IV. Patients were excluded if they (1) demonstrated invalid test performance as defined by failure of two or more of the five performance validity tests (PVTs) administered, consistent with current empirically supported practice standards (see Jennette et al., 2022; Rhoads et al., 2021; Sweet et al., 2021), or (2) produced invalid symptom reporting profiles (see below). Of 164 individuals who completed the BAARS-IV, nine had invalid neuropsychological performance data. An additional 18 participants produced invalid ADHD symptom reporting on the Clinical Assessment of Attention Deficit-Adult (CAT-A) based on failure of one or more CAT-A embedded symptom validity tests (SVTs), consistent with the CAT-A manual (Bracken & Boatwright, 2005). All 164 individuals who completed the BAARS-IV were included in the exploratory factor analysis (EFA), and the 27 who produced invalid performance or symptom reporting were excluded from subsequent analyses. Reasons for this selection are threefold: (1) No validity scale exists for the BAARS-IV SCT Scale, (2) performance and symptom validity are dissociable constructs (e.g., Ovsiew et al., 2023; White et al., 2022), and (3) the CAT-A embedded SVTs have not been evaluated for use in determining BAARS-IV SCT Scale validity and prior research has demonstrated that embedded SVTs have extremely limited, if any, utility in determining valid symptom reporting on separate measures (e.g., Leib et al., 2022).
Demographic and clinical characteristics of the sample are detailed in Tables 1 and 2. Briefly, the sample, including all participants, consisted of 63 male (38.4%) and 101 female patients (61.6%) whose mean age was 28.6 (SD = 7.3). 37% identified as non-Hispanic White (n = 61), 22.6% as Hispanic (n = 37), 19.5% as non-Hispanic Black (n = 32), 13.4% as Asian/Pacific Islander (n = 22), and 7.3% as multiracial or other race/ethnicity (n = 12). Mean level of education for this sample was 16.2 years (SD = 2.2). Two-thirds (66.5%) of the final sample was diagnosed with ADHD by a board-certified clinical neuropsychologist at the completion of the evaluation. ADHD diagnoses were established based on a standard diagnostic protocol involving the following: (1) review of past medical and psychiatric health records, academic history, and results of past psychological or neuropsychological assessments; (2) a patient history questionnaire evaluating self-reported medical, psychiatric, substance use, social, developmental, educational, and occupational history; (3) a clinical interview performed by a board-certified clinical neuropsychologist assessing Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR; American Psychiatric Association, 2022) criteria for ADHD and criteria for other present psychiatric disorders; and (4) completion of the CAT-A, Beck Depression Inventory-2nd Edition (BDI-II; Beck et al., 1996), and Beck Anxiety Inventory (BAI; Beck et al., 1988). In addition to the diagnostic protocol, patients completed a standard neuropsychological test battery which assessed estimated premorbid intelligence, language, visuospatial abilities, verbal/visual memory, attention/working memory, sustained attention, processing speed, and executive functioning. Because all participants were clinically referred for diagnostic clarification and treatment planning of known or suspected ADHD, all measures were selected to assess cognitive and psychological domains of functioning that are relevant to ADHD (e.g., attention, hyperactivity/impulsivity, co-occurring depressive symptoms, anxiety symptoms, executive functioning).
Descriptive Statistics for all Individuals Included in the Factor Analysis.

Note. N = 164. SCT = Sluggish Cognitive Tempo; CDS = Cognitive Disengagement Syndrome; ADHD = Attention-Deficit/Hyperactivity Disorder; CAT-A = Clinical Assessment of Attention Deficit-Adult.
Descriptive Statistics for Individuals With Valid Performance and Valid CAT-A Data.
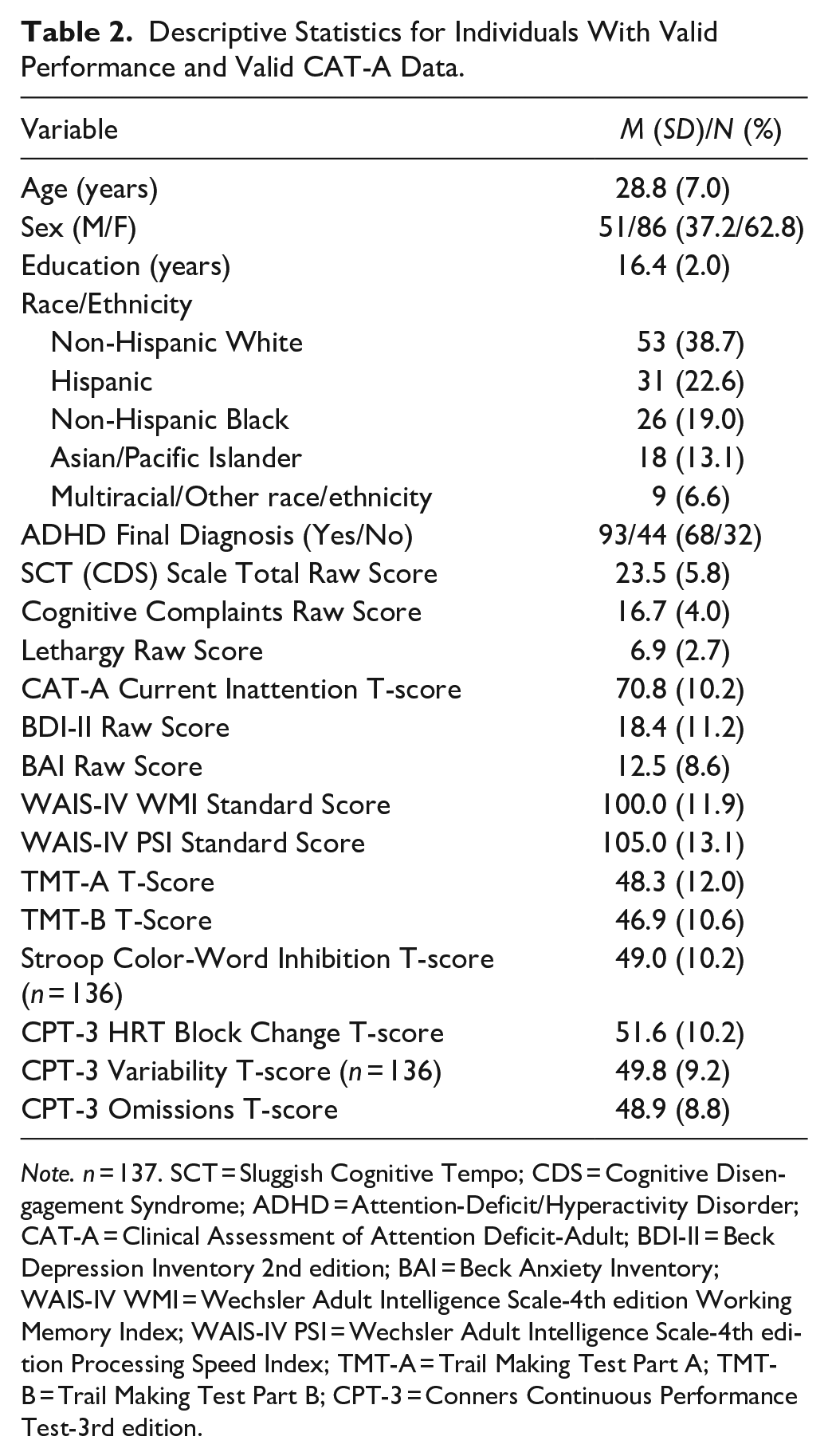
Note. n = 137. SCT = Sluggish Cognitive Tempo; CDS = Cognitive Disengagement Syndrome; ADHD = Attention-Deficit/Hyperactivity Disorder; CAT-A = Clinical Assessment of Attention Deficit-Adult; BDI-II = Beck Depression Inventory 2nd edition; BAI = Beck Anxiety Inventory; WAIS-IV WMI = Wechsler Adult Intelligence Scale-4th edition Working Memory Index; WAIS-IV PSI = Wechsler Adult Intelligence Scale-4th edition Processing Speed Index; TMT-A = Trail Making Test Part A; TMT-B = Trail Making Test Part B; CPT-3 = Conners Continuous Performance Test-3rd edition.
Measures
Performance Validity Tests (PVTs)
All patients were administered two freestanding and three embedded PVTs throughout their test batteries, consistent with the number of PVTs typically used by neuropsychologists in clinical evaluations (Martin et al., 2015). Freestanding PVTs were the Dot Counting Test (Abramson et al., 2023) and the Rey 15-Item Test Recall + Recognition (Poynter et al., 2019). Embedded PVTs administered were the Reliable Digit Span from the Wechsler Adult Intelligence Scale-4th Edition (Bing-Canar et al., 2022), Rey Auditory Verbal Learning Test Effort Score (Phillips et al., 2023), Brief Visuospatial Memory Test-Revised Recognition Discrimination (Phillips et al., 2023), and the Stroop Color and Word Test Word Reading subtest (Khan et al., 2022).
Barkley Adult ADHD Rating Scale-Fourth Edition Ed., Sluggish Cognitive Tempo Scale (BAARS-IV)
The BAARS-IV Sluggish Cognitive Tempo Scale is a nine-item measure of self-reported CDS symptoms (Barkley, 2011). Each symptom is rated on a 4-point scale (1 for “Never or rarely,” 2 for “Sometimes,” 3 for “Often,” and 4 for “Very often.”). The nine constituent SCT items were used as indicators for the exploratory factor analysis, and the resulting factors were used as predictors in the regression analyses.
Clinical Assessment of Attention Deficit-Adult (CAT-A)
The CAT-A is a 108-item self-report measure of ADHD symptoms in childhood and adulthood (Bracken & Boatwright, 2005). The CAT-A produces scales for current and childhood symptoms of inattention, impulsivity, and hyperactivity, as well as total clinical index scores. Patients rate the degree to which symptoms apply to them using a 4-point scale that ranges from 1 for “Strongly disagree” to 4 for “Strongly agree.” This measure also has three embedded symptom validity scales to assess overreporting or underreporting of ADHD symptoms. The CAT-A Current Inattention scale was used as a covariate in the present analyses.
Advanced Clinical Solutions Test of Premorbid Functioning (TOPF)
The TOPF (Pearson, 2009) provides an estimate of general intellectual functioning, which has been shown to correlate robustly with actual Full-Scale IQ (FSIQ) scores (Kirton et al., 2020). Patients read a list of phonetically irregular words aloud, resulting in a raw score that is converted to an age-corrected standard score. Reading scores are then combined with several demographic variables (i.e., sex, highest educational attainment, race/ethnicity, U.S. geographic region, and occupation) to provide an estimated Wechsler Adult Intelligence Scale-4th Edition (WAIS-IV; Wechsler, 2008) FSIQ. The TOPF + Simple Demographics estimated FSIQ was used as a covariate in the present analyses.
Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV) Working Memory Index (WMI) and Processing Speed Index (PSI)
The WMI (Wechsler, 2008) assesses complex attention/working memory abilities. The WMI standard score used in this study was derived from performance on the Digit Span and Letter-Number Sequencing subtests. Notably, Letter-Number Sequencing was prospectively substituted for the more common Arithmetic subtest in order to mitigate the confounding effects of potential comorbid specific learning disorder in mathematics in the sample, given the high co-occurrence with ADHD (Capano et al., 2008; Tosto et al., 2015). The PSI (Wechsler, 2008) assesses psychomotor speed. The WMI and PSI standard scores were used as outcomes in the present analyses.
Trail Making Test Parts A & B (TMT-A & TMT-B)
TMT-A assesses divided attention, visual scanning, and psychomotor speed (Heaton et al., 2004; Linari et al., 2022). TMT-B assesses the same domains as TMT-A as well as cognitive flexibility (Heaton et al., 2004; Linari et al., 2022). Raw scores are completion times, which are converted to demographically-corrected T-scores based on age, sex, race, and years of education. The TMT-A and TMT-B T-scores were used as outcomes in the present analyses.
Conners Continuous Performance Test-3rd Edition (CPT-3)
The CPT-3 (Conners, 2014) is a computerized test that assesses sustained attention, vigilance, inattentiveness, and impulsivity over a period of 15 min. CPT-3 T-scores are automatically generated for Detectability (differentiation of non-targets to targets), Omissions (missed targets), Commissions (incorrect hits on non-targets), Perseverations (random, repetitive, or anticipatory responses), Hit Reaction Time (mean response speed), Hit Reaction Time Standard Deviation (consistency in reaction times), Variability (variability in reaction times), Hit Reaction Time Block Change (changes in average response speed across blocks), and Hit Reaction Time Inter-stimulus Interval Change (changes in average response speed across inter-stimulus intervals). The T-scores for Hit Reaction Time Block Change, Variability, and Omissions were used in our analyses as outcome measures of sustained attention.
Stroop Color and Word Test (SCWT)
The SCWT (Golden, 1978) is a widely used measure of attention, response inhibition, and processing speed in which examinees are required to inhibit an automatic response in favor of a non-automatic target response. SCWT raw scores were converted to age and education corrected T-scores. The SCWT Color-Word Inhibition T-score was used as an outcome measure in the present analyses.
Beck Anxiety Inventory (BAI)
The BAI (Beck & Steer, 1993) is a 21-item self-report inventory of current anxiety symptom severity in adults and older adolescents. Patients rate the degree to which they have been bothered by each symptom during the past week on a 4-point scale. Higher total raw scores indicate greater anxiety. The BAI raw score was used as an outcome in the present analyses.
Beck Depression Inventory-2nd Edition (BDI-II)
The BDI-II (Beck et al., 1996) is a 21-item self-report measure of current depression symptoms in adults and older adolescents. Patients rate the level of severity for each symptom that they may have experienced during the past 2 weeks on a 4-point scale. Higher total raw scores indicate greater depression. The BDI-II raw score was used as an outcome in the present analyses.
Statistical Analyses
All analyses were conducted using Jamovi (Version 2.0.0; The Jamovi Project, 2020). Normality assumptions were met for most independent variables of interest (i.e., skewness and kurtosis < 1.5), except for CPT-3 Omissions (skewness = 2.96, kurtosis = 9.17) and CPT-3 Variability (skewness = 1.62, kurtosis = 1.91). Logarithmic transformation corrected CPT-3 Variability but only modestly improved normality statistics of CPT-3 Omissions (skewness = 2.51, kurtosis = 6.34). An EFA with Oblimin rotation examined the factor structure of the nine items that comprise the BAARS-IV SCT Scale. Pearson correlations investigated the relationships between the CDS subfactors, psychiatric self-report measures, and cognitive performance assessments. Due to the continued non-normal distribution of CPT-3 Omissions values following logarithmic transformation, nonparametric Spearman correlations compared the association of the transformed values with other variables. A series of multiple linear regression analyses examined whether the resulting CDS factors predicted symptoms of depression, anxiety, and ADHD-related inattention, using the BDI-II and BAI raw scores and CAT-A Current Inattention T-score, respectively. Another series of hierarchical multiple linear regression analyses examined whether the CDS factors uniquely predicted cognitive performance after controlling for estimated intelligence and ADHD inattention symptoms. CDS factors were entered in Block 1; estimated premorbid FSIQ and ADHD inattention symptoms were entered in Block 2. A linear regression was used to assess associations between predictor variables and the transformed CPT-3 Omissions variable, and results were interpreted cautiously due to its non-normality.
Results
Kaiser-Meyer-Olkin measure [KMO = 0.79] and Bartlett’s test of sphericity [χ2(36) = 490, p < .001] suggested the data were appropriate for factor analysis. A parallel analysis scree plot and Kaiser’s (1960) criterion suggested that a two-factor solution was optimal. This two-factor solution accounted for 46.0% of overall variance in SCT [χ2(19) = 31.9, p < .05]. Item factor loadings are available in Table 3. The first factor consisted of items indicative of daydreaming, trouble staying alert, easily confused, easily bored, spacey or foggy, and not processing information quickly. Due to the cognitive nature of these complaints, we labeled this first factor as “Cognitive Complaints.” Internal consistency for Cognitive Complaints was adequate (ω = 0.76). The second factor was identical to Lunsford-Avery et al.’s (2021) “Sleepy/Sluggish” factor and J. N. Smith and Suhr’s (2021) “Lethargy” factor: lethargy, moving slowly, and being underactive. We similarly labeled this factor “Lethargy” and observed adequate internal consistency (ω = 0.84). We opted to utilize the more parsimonious two-factor model rather than the three-factor models extracted by J. N. Smith and Suhr (2021) and Lunsford-Avery et al. (2021) for external validation. Our Cognitive Complaints factor was skewed (2.11) and kurtotic (14.8) and corrected using a logarithmic transformation (skewness = −0.34; kurtosis = 2.12) prior to its inclusion in correlation and regression analyses.
BAARS-IV Sluggish Cognitive Tempo Scale Item Factor Loadings.
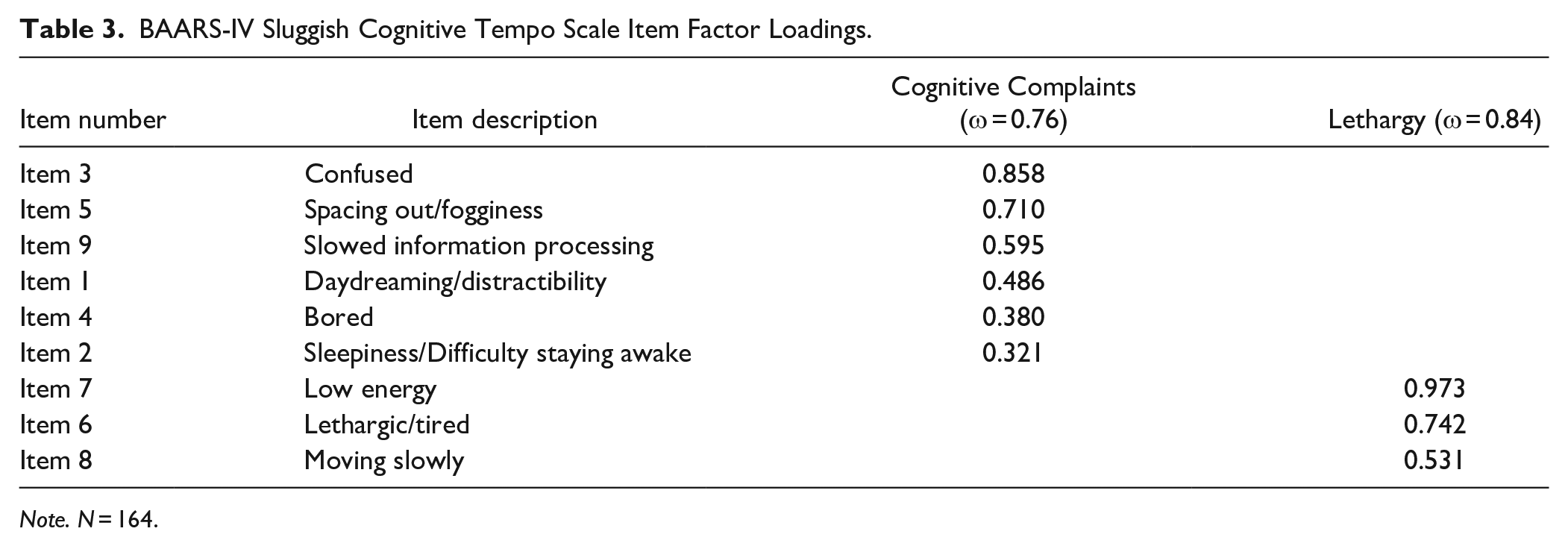
Note. N = 164.
Results from the Pearson and Spearman correlations are available in Table 4. Briefly, cognitive complaints and Lethargy were significantly positively correlated with one another (r = .50). Both factors were significantly positively correlated with the self-report measures: BDI-II, BAI, and CAT-A current inattention (rs = 0.26 to 0.57). Cognitive complaints was negatively correlated with WAIS-IV WMI (r = −.27), WAIS-IV PSI (r = −.21), TMT-A (r = −.34), SCWT color-word inhibition (r = −.37), and CPT-3 omissions (ρ = 0.24). Lethargy was significantly negatively correlated with WAIS-IV PSI (r = −.27), TMT-A (r = −.32), TMT-B (r = −.26) and SCWT color-word inhibition (r = −.42).
Pearson correlations between study variables.

Note. n = 137. BDI-II = Beck Depression Inventory 2nd edition; BAI = Beck Anxiety Inventory; WAIS-IV WMI = Wechsler Adult Intelligence Scale-4th edition Working Memory Index; WAIS-IV PSI = Wechsler Adult Intelligence Scale-4th edition Processing Speed Index; TMT-A= Trail Making Test Part A; TMT-B = Trail Making Test Part B; SCWT CW = Stroop Color-Word Inhibition; CPT-3 = Conners Continuous Performance Test-3rd edition.
n = 136.
Spearman correlations.
p < .05. **p < .01. ***p < .001.
Full results of the regression analyses are available in Tables 5 to 15. Regarding psychiatric self-reports, both Cognitive Complaints and Lethargy significantly predicted depressive symptoms, sharing 26.4% variance. Neither CDS subfactor significantly predicted anxiety symptoms, though the overall model was statistically significant and accounted for 8.4% of the variance. Only Cognitive Complaints significantly predicted inattentive symptoms, with the overall model sharing 33.5% variance. Regarding cognitive performance, hierarchical multiple regression analyses indicated Cognitive Complaints significantly, but modestly, predicted WAIS-IV working memory performance. However, this association was no longer statistically significant after accounting for estimated premorbid FSIQ and inattentive symptoms as only estimated premorbid FSIQ was significant in the overall model. Neither CDS subfactor significantly predicted WAIS-IV processing speed performance. Only Lethargy significantly predicted TMT-A performance, sharing 14.1% variance, although Lethargy was no longer statistically significant in the second block. Lethargy significantly predicted TMT-B performance, sharing 5.4% to 5.6% variance, but the overall model was no longer statistically significant after accounting for estimated FSIQ and inattention. Both factors significantly predicted SCWT Color-Word Inhibition performance in Block 1, sharing 20.2% variance, although only Lethargy remained significant after the covariates were entered into the model, which did not explain significantly more variance. Cognitive Complaints was significantly associated with CPT-3 HRT Block Change in Block 1 only, and the overall model failed to reach significance in Blocks 1 and 2. Neither CDS subfactor was significantly associated with CPT-3 Variability or CPT-3 Omissions. Cook’s distance values were well within acceptable limits for CPT-3 Omissions (<0.2), indicating no major influence of outlying values on the model.
BDI-II.

Note. n = 137. BDI-II =Beck Depression Inventory 2nd edition. *p < .05. ***p < .001.
BAI.

Note. n = 137. BAI = Beck Anxiety Inventory. **p < .01.
CAT-A Current Inattention.

Note. n = 137. CAT-A = Clinical Assessment of Attention Deficit-Adult. ***p < .001.
WAIS-IV WMI.

Note. n = 137. WAIS-IV WMI = Wechsler Adult Intelligence Scale-4th edition Working Memory Index. *p < .05. ***p < .001.
WAIS-IV PSI.

Note. n = 137. WAIS-IV PSI = Wechsler Adult Intelligence Scale-4th edition Processing Speed Index. *p < .05.
TMT-A.
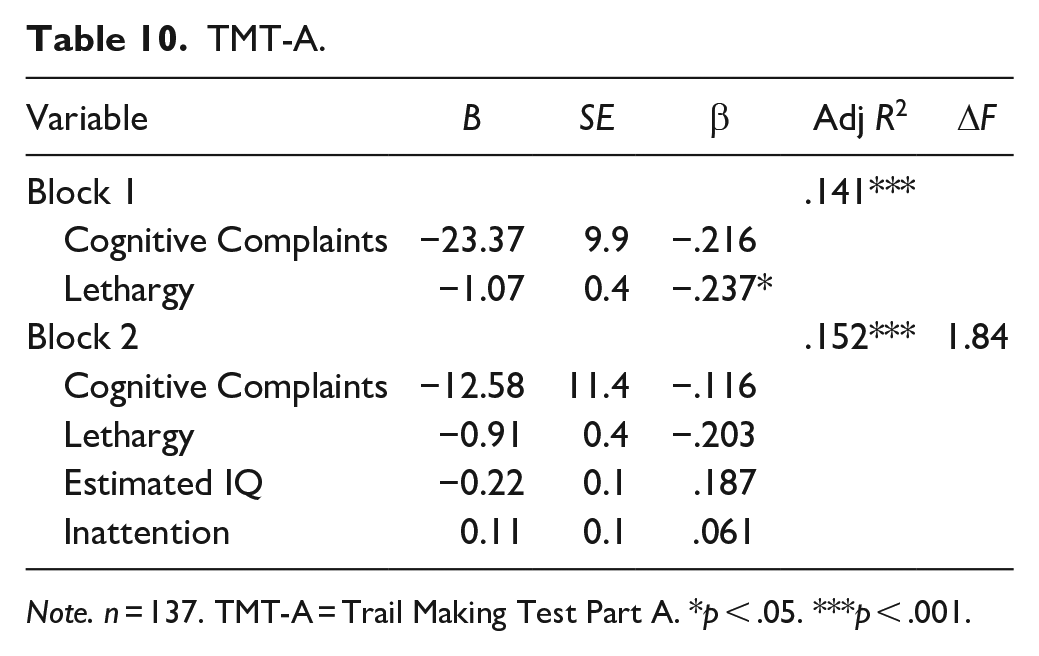
Note. n = 137. TMT-A = Trail Making Test Part A. *p < .05. *** p < .001.
TMT-B.

Note. n = 137. TMT-B = Trail Making Test Part B. *p < .05.
SCWT Color-Word Inhibition.
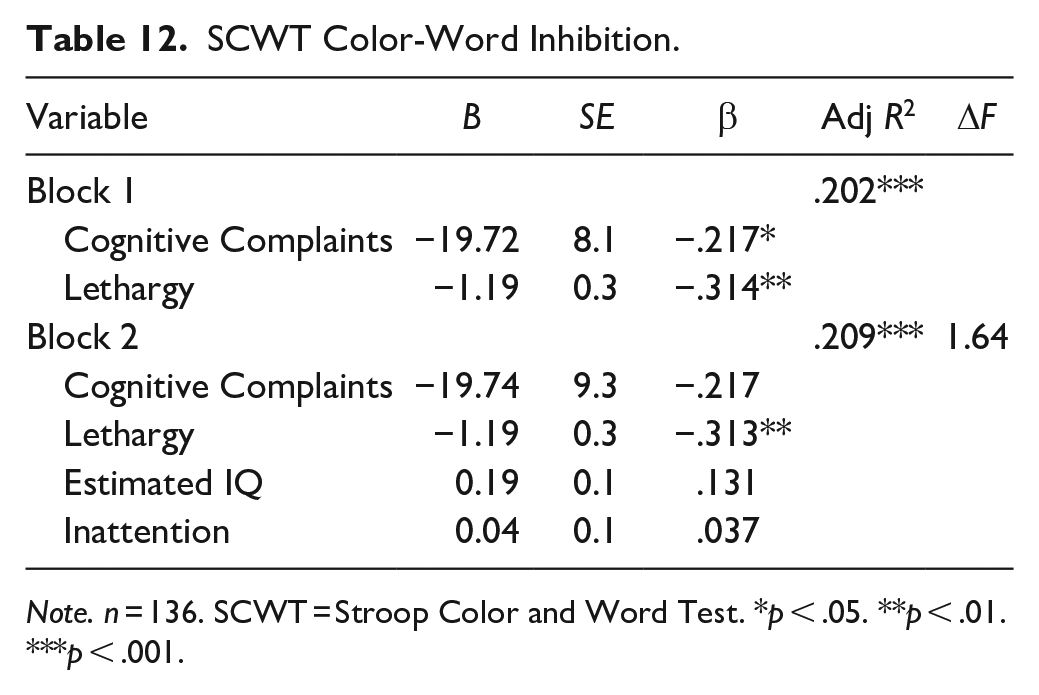
Note. n = 136. SCWT = Stroop Color and Word Test. *p < .05. **p < .01. ***p < .001.
CPT-3 Hit Rate Block Change.
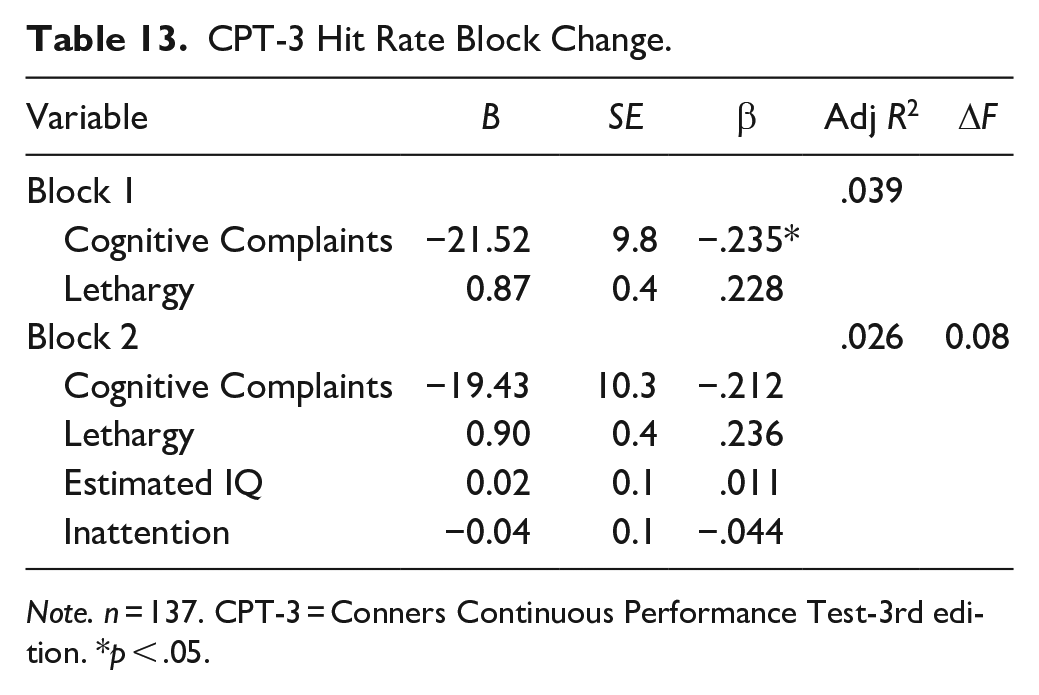
Note. n = 137. CPT-3 = Conners Continuous Performance Test-3rd edition. *p < .05.
CPT-3 Variability.

Note. n = 136. CPT-3 = Conners Continuous Performance Test-3rd edition. *p < .05.
CPT-3 Omissions.
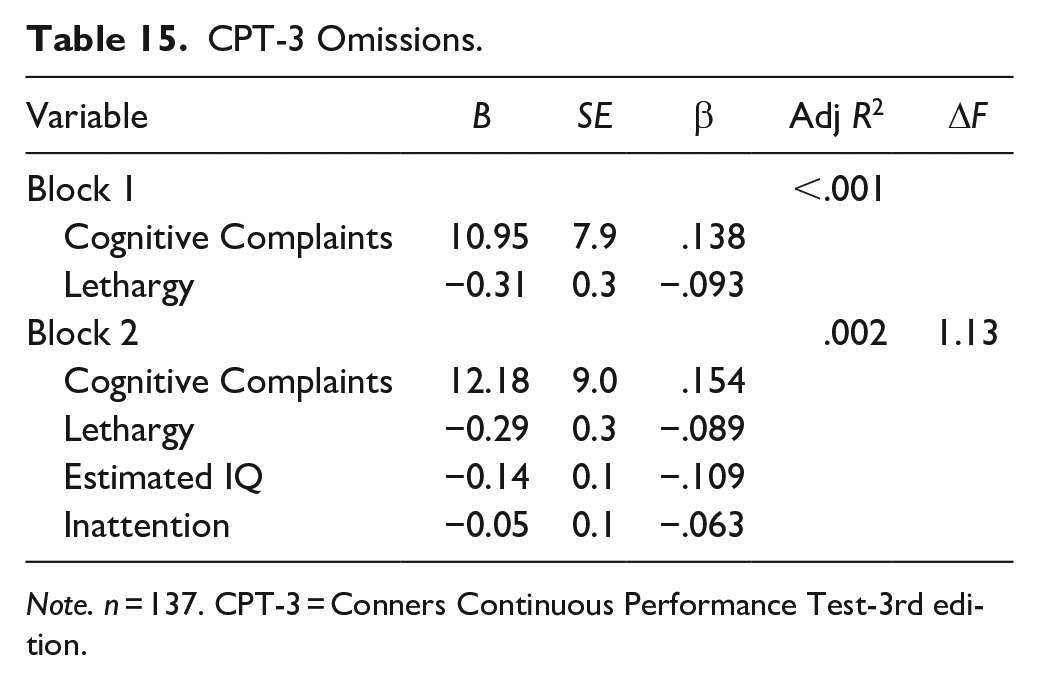
Note. n = 137. CPT-3 = Conners Continuous Performance Test-3rd edition.
Discussion
The current study had three general aims. First, it examined the factor structure of the BAARS-IV SCT (CDS) scale in an outpatient neuropsychiatric adult population. Second, it evaluated the associations between the CDS subfactors and working memory, processing speed, and executive functioning performance before and after accounting for estimated intelligence and inattention. Third, it investigated whether identified subfactors could also predict depression, anxiety, and inattention symptoms. Results revealed CDS is composed of two subfactors: “Cognitive Complaints” and “Lethargy.” Cognitive Complaints consisted of six items indicative of daydreaming, poor alertness, confusion, boredom, spacing out/fogginess, and slowed information processing. Lethargy consisted of three items indicative of lethargy, slow movement, and underactivity. We decided to employ the more parsimonious two-factor model as opposed to previous three-factor models (Lunsford-Avery et al., 2021; J. N. Smith & Suhr, 2021). Cognitive Complaints and Lethargy were positively correlated with one another and with all psychiatric self-report measures. The subfactors demonstrated comparable correlations with the cognitive performance variables. Results showed that both factors were significantly predictive of depressive symptoms and shared modest variance with anxiety symptoms. Cognitive Complaints specifically shared a relatively large amount of variance with inattentive symptoms. Regarding cognitive performance, both Cognitive Complaints and Lethargy demonstrated weak to null associations with all variables, apart from SCWT Color-Word Inhibition. In the final SCWT Color-Word Inhibition model, Lethargy was the sole significant predictor in a model sharing 20.9% variance.
The identified subfactors align with those extracted in earlier factor analyses of CDS (Barkley, 2013; Jacobson et al., 2018; Lunsford-Avery et al., 2021; Penny et al., 2009; J. N. Smith & Suhr, 2021). To illustrate, the current study’s Lethargy subfactor is identical to the Lethargy subfactor extracted by J. N. Smith and Suhr (2021) as well as the Sleepy/Sluggish subfactor extracted by Lunsford-Avery et al. (2021). The present study’s Cognitive Complaints subfactor is a combination of Smith and Suhr’s Cognitive Complaints and Daydreaming/Bored subfactors and Lunsford-Avery et al.′s Slow/Daydreamy and Low Initiation/Persistence subfactors. Moreover, the two items with the lowest factor loadings on the Cognitive Complaints subfactor (Bored and Sleepiness/Difficulty staying awake) were the two items that comprised (Lunsford-Avery et al., 2021) Low Initiation/Persistence subfactor. Cognitive Complaints and Lethargy are also similar to the Sluggish and Daydreaming subfactors identified in a large sample of children with and without clinically significant CDS and/or ADHD (Barkley, 2013). Moreover, the present subfactors support Becker et al. (2023) conception of CDS, which includes a cognitive component (i.e., Cognitive Complaints) and a motor component (i.e., Lethargy). Taken together, while the present study’s results align with the conceptual two-domain structure of CDS symptomatology, minor discrepancies between the factors extracted in present study those observed in previous research (i.e., Lunsford-Avery et al., 2021; J. N. Smith & Suhr, 2021) indicate the need for continued exploration into this area to better clarify CDS factor structure.
Results of this investigation generally support the majority of extant literature demonstrating moderate to strong associations between CDS symptoms and psychiatric self-report symptoms and weak to null associations between CDS symptoms and objective cognitive performance (Cerny et al., 2023; J. N. Smith & Suhr, 2021; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017). However, the current study found more widespread significant correlations between CDS symptoms and objective cognitive performance among adults than has been observed in previous literature. The robust correlations between CDS subfactors and broad performance on tasks related to processing speed (i.e., TMT, WAIS-IV PSI, Stroop) contrasts the weak and inconsistent correlations observed in previous literature (Cerny et al., 2023; Jarrett et al., 2017; Kamradt et al., 2018; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017). Among measures examined, the SCWT Color-Word Inhibition is the most sensitive to CDS symptomatology, as approximately 20% of the variance in SCWT Color-Word Inhibition performance is shared by the two CDS subfactors. It is possible that speed-based measures dependent on reading rather than psychomotor speed, such as SCWT Color-Word Inhibition, may be more sensitive to CDS symptomatology than other performance-based measures. This is partially supported by previous studies that observed significant correlations between speed-based reading tasks and CDS symptomatology (J. N. Smith & Suhr, 2021; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017); however, the associations between speeded reading and CDS symptoms in previous studies were no longer significant after accounting for the influence of other variables (J. N. Smith & Suhr, 2021; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017). Moreover, Jarrett et al. (2017) did not observe a significant association between CDS symptoms and SCWT Color-Word Inhibition performance. Interestingly, in the present study, Lethargy was significantly correlated with several measures of processing speed and showed a more robust and specific association with TMT than Cognitive Complaints, particularly TMT-A. Lethargy aligns well with the broad motor domain of CDS symptomatology (Becker et al., 2023), though it may be better characterized as a domain of psychomotor speed rather than pure motor speed. Additional research is needed to clarify whether different speed-based tasks (e.g., psychomotor speed versus reading) have differential associations with CDS symptomatology, and may better elucidate the extent and nature of motor/psychomotor deficits in clinically significant CDS. Differences in results between this investigation and extant literature are likely due to methodology. The major difference between the present study and extant research is that most prior studies examined CDS as a unitary construct, rather than its component subfactors (e.g., Cerny et al., 2023; Jarrett et al., 2017; Kamradt et al., 2018; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017). This study demonstrated that the CDS subfactors have differential associations with objective cognitive performance variables, and such differences cannot be captured when examining CDS as a unitary construct. Moreover, all studies, with the exception of Cerny et al. (2023), utilized volunteer, rather than clinical, samples (Jarrett et al., 2017; Kamradt et al., 2018; Wood, Lewandowski et al., 2017; Wood, Potts et al., 2017). Differences in sample characteristics is also the most likely explanation for the differences between results of this study and those of J. N. Smith and Suhr (2021), the first to explore associations between CDS subfactors and objective cognitive performance among adults. J. N. Smith and Suhr (2021) utilized an age-restricted (18–24 years old), nonclinical undergraduate sample, of which 14.8% had a diagnosis of ADHD. The current study utilized a clinical neuropsychiatric outpatient sample, of which 66.5% were diagnosed with ADHD. The clinical setting suggests that individuals may have been experiencing more significant symptoms than would be expected in a community or undergraduate volunteer sample.
Select pediatric studies have demonstrated significant associations between CDS symptoms and sustained attention (Wåhlstedt & Bohlin, 2010; Willcutt et al., 2014). The current study observed a correlation between Cognitive Complaints and sustained attention, as measured by CPT-3 Omissions, but such associations were not observed after controlling for the influence of other variables. These differences in results may also be largely due to methodological differences. Studies among children have utilized a unitary CDS factor structure and assessments of CDS symptoms other than the BAARS-IV, given that the BAARS-IV is only validated for use in adults. Taken together, these findings support the need for additional research clarifying differential associations between CDS subfactors and objective cognitive performance in adult populations.
Regarding psychiatric symptomatology, results generally support prior research that CDS symptoms are associated with internalizing dysfunction (i.e., anxiety and depression) and inattention, with several caveats (Becker et al., 2023; Cerny et al., 2023; Kamradt et al., 2018; J. N. Smith & Suhr, 2021). J. N. Smith and Suhr (2021) observed that the Cognitive Complaints subfactor uniquely predicted anxiety symptoms, similar to the present study. Interestingly, Daydreaming/Bored did not, despite the items making up Smith and Suhr’s Daydreaming/Bored and Cognitive Complaints subfactors formed the single Cognitive Complaints subfactor of the present study. Although the current study indicated that both CDS subfactors significantly predicted depressive symptoms, only J. N. Smith and Suhr’s (2021) Daydreaming/Bored subfactor did so. Consistent with this study’s findings, both J. N. Smith and Suhr’s (2021) Cognitive Complaints and Daydreaming/Bored subfactors predicted self-reported inattention, though the current study utilized the CAT-A to measure inattentive symptoms, while the prior utilized the Conners Adult ADHD Rating Scale (CAARS; Conners et al., 1998). Further, results were generally consistent with earlier studies demonstrating that CDS symptoms are associated with internalizing symptomatology, despite previous studies also utilizing a unitary CDS factor structure (e.g., Becker et al., 2019; Cerny et al., 2023; Kamradt et al., 2018).
This study had several methodological strengths. The sample was large and ethnically diverse. Performance validity was controlled, using empirically supported criteria for invalidity (Jennette et al., 2022; Rhoads et al., 2021; Sweet et al., 2021). Symptom validity was also controlled, using manual-specified and independently validated criteria (Bracken & Boatwright, 2005; Leib et al., 2022). Methodology was based on J. N. Smith and Suhr’s (2021) study, and similarly controlled for potential confounding variables of estimated intelligence and ADHD-related inattention when predicting cognitive performance. Additional cognitive domains not included in J. N. Smith and Suhr’s (2021) study were also included (i.e., sustained attention). Nevertheless, this study had noteworthy limitations. First, our participants were individuals referred for an ADHD evaluation often following express complaints of inattention, which may limit generalizability of findings to populations without subjective complaints. Secondly, we did not examine any co-occurring medical or psychiatric disorders, which may influence cognitive performance. Future studies would benefit from investigating subfactors of CDS and their associations with neuropsychological functioning in a more diagnostically diverse sample of adults. Another limitation, which is posed by one of the instruments employed, is that it was not possible to fully account for non-credible symptom reporting on the BAARS-IV, given that it does not include a symptom validity scale. A fourth limitation is that our population was highly educated, and results may not fully generalize to populations with lower educational attainment. This study also utilized a cross-sectional design, whereas future studies would benefit from assessing associations between CDS symptoms and cognitive performance over time.
In summary, CDS symptomatology generally shows weak to nonsignificant associations with objective cognitive performance and robust associations with symptoms of depression and inattention. In contrast, the present study observed robust associations between specific speed-based cognitive tasks and CDS subfactors, suggesting a more granular approach to studying CDS symptomatology may reveal specific tasks to be affected by CDS symptomatology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.