
Abstract
Objective:
Cognitive disengagement syndrome (CDS), previously referred to as sluggish cognitive tempo (SCT), is characterized by symptoms such as excessive daydreaming, mental confusion, and hypoactivity. CDS symptoms are associated with emotional, social, and daily life impairments. The way in which one solves problems in their daily life is associated with experiences of further problems, such that maladaptive problem-solving can lead to further physical and psychological problems. However, there is limited information on how CDS symptoms are associated with problem solving. The current study examined CDS symptoms in relation to different social problem solving approaches.
Method:
A total of 280 college students (ages 18–23 years; 77.9% female) completed measures of psychopathology symptoms and social problem solving.
Results:
Above and beyond ADHD and internalizing symptoms, CDS symptoms were independently associated with negative problem orientation and avoidance style domains of maladaptive problem solving.
Conclusion:
Findings indicate that CDS symptoms are related to specific difficulties with social problem solving. CDS symptoms may lead to difficulties attending to problems or working through relevant steps needed to identify solutions for the problem, which may then lead to avoidance and social withdrawal. Longitudinal research is needed to evaluate maladaptive problem solving as a potential mechanism in the association between CDS, social withdrawal, and internalizing symptoms.
Cognitive disengagement syndrome (CDS), previously referred to as sluggish cognitive tempo (SCT), is represented by a set of both cognitive and motor symptoms that are developmentally inappropriate, associated with functional impairment, and related to other psychopathologies (Becker et al., 2023). The cognitive symptoms are related to difficulties engaging with the external world and include slow thinking/processing, losing one’s train of thought/cognitive set, seeming to be “in a fog,” daydreaming, getting lost in one’s thoughts, staring blankly, being easily confused, and feeling apathetic/unmotivated (Becker et al., 2023). The motor symptoms include physical hypoactivity, such as sluggishness, feeling tired/lethargic, underactivity, sleepiness/drowsiness, and slow or delayed motor movement (Becker, Leopold, et al., 2016; Becker et al., 2023). Originally conceptualized as representing a “pure” form of the inattentive presentation of attention deficit/hyperactivity disorder (ADHD-IN), increased empirical evidence has accumulated over the past 15 years demonstrating that CDS is a construct distinct from, but highly related to, ADHD (Becker & Barkley, 2018; Becker et al., 2023; Becker, Leopold, et al., 2016; Kaçmaz et al., 2024). Recent discussions have focused on how to best conceptualize CDS: as a formal disorder in future editions of the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; American Psychiatric Association, 2022), a transdiagnostic factor relevant to multiple psychopathologies, or a unique subtype or specifier within ADHD (Barkley, 2014; Becker et al., 2023; Becker & Willcutt, 2019).
The distinct nature of CDS is further evidenced by research highlighting the unique associations between CDS and impairment. Within the available adult studies, CDS remains related to functional impairments when controlling for ADHD (Barkley, 2012; Becker et al., 2023; Becker, Leopold, et al., 2016). Specifically, studies in adults have found CDS symptoms to be associated with executive functioning deficits and impairment across emotional, social, academic, and daily life domains above and beyond ADHD symptoms (Becker, Langberg, et al., 2014; Becker, Leopold, et al., 2016; Flannery et al., 2017; Lunsford-Avery et al., 2021; Wood, Lewandowski, et al., 2017). Notably, adults with both elevated CDS and ADHD symptoms experience greater impairment compared to those with ADHD symptoms only (Barkley, 2012). As approximately half of adults with elevated ADHD symptoms also have elevated CDS symptoms (Barkley, 2012), understanding the association between CDS symptoms and functioning is important for adults with and without ADHD alike.
CDS is also related to poorer functioning across numerous domains, including internalizing symptoms and interpersonal problems (Becker et al., 2023; Becker, Leopold, et al., 2016; Lovett et al., 2021). Although both ADHD and CDS demonstrate positive associations with anxiety and depression, CDS remains related to these internalizing domains even when controlling for ADHD (Becker et al., 2020; Becker, Leopold, et al., 2016; Burns et al., 2013; Leikauf & Solanto, 2017; Penny et al., 2009) and this association further remains even when accounting for the high overlap between anxiety and depression (Becker, Luebbe, et al., 2014). Previous research has also indicated that CDS symptoms are associated with difficulties that are commonly seen for those with internalizing symptoms (i.e., anxiety and depression), including suicide behaviors (Becker, Holdaway, et al., 2018; Becker, Withrow, et al., 2016), social impairment, and emotion dysregulation (Becker, Burns, Garner, et al., 2018; Becker, Leopold, et al., 2016). CDS also remains significantly related to these impairments when controlling for internalizing symptoms. Further, although ADHD is strongly related to externalizing behaviors (e.g., oppositional defiant disorder symptoms), CDS is not significantly related or is negatively related to externalizing symptoms when controlling for ADHD (Becker & Barkley, 2018; Becker & Langberg, 2013; Becker, Leopold, et al., 2016; Lee et al., 2014). Considered together, these findings have led to the possibility that CDS may be best conceptualized as within the internalizing spectra of psychopathology (Becker et al., 2020; Becker & Willcutt, 2019; Saxbe & Barkley, 2014; Smith et al., 2019).
Another consistent finding shows that CDS symptoms are associated with increased social difficulties. Longitudinal studies have found CDS symptoms predict lower popularity, greater negative social preference ratings, greater peer impairment, and higher peer rejection (Becker, 2014; Bernad et al., 2016). There is growing evidence that CDS symptoms in children are specifically related to higher levels of social isolation, social withdrawal, and loneliness (Becker, Burns, Leopold, et al., 2018; Becker et al., 2019; Becker et al., 2024; Mikami et al., 2007; Willcutt et al., 2014; for a review, see Fredrick & Becker, 2023). Interestingly, a recent study found that symptoms of CDS in children were related to social withdrawal, but not overall parent-reported social problems, suggesting that CDS may be related more specifically to difficulties with social engagement and initiation (Rondon et al., 2020). Another study found that children with higher levels of CDS symptoms had increased physiological reactivity during a social stress task, indicating that CDS may relate to how specific stressful social situations are managed (Becker & McQuade, 2020).
Most studies examining CDS symptoms and social functioning have been conducted in children. However, the handful of studies conducted in adults report similar findings. Specifically, symptoms of CDS in adults are related to deficits in social interactions and interpersonal relationships (Barkley, 2012; Flannery et al., 2016, 2017; Lunsford-Avery et al., 2021), as well as higher reports of loneliness and lower self-esteem (Becker, Burns, Garner, et al., 2018). Notably, higher CDS symptoms remain significantly related to increased loneliness and lower self-esteem in adults when controlling for internalizing symptoms (Becker, Burns, Garner, et al., 2018).
Social Problem Solving
Despite strong evidence that CDS is related to social impairment, and specifically, withdrawn and socially disengaged behavior, less is known about why individuals with CDS have these social deficits. Social problem solving plays a significant role in the relationship between stressful events and psychological distress (D’Zurilla & Nezu, 2010; Nezu et al., 2015). Further, ineffective problem solving and psychological distress have a reciprocal causal relationship, suggesting that individuals that are unable to effectively cope with stress are likely to experience more stress and so on, potentially leading to long-term problems (D’Zurilla & Nezu, 2010; Nezu, 2004).
Social problem solving includes both problem orientation and problem-solving styles. A problem orientation refers to one’s mostly stable, general cognitive-emotional schemas (i.e., beliefs, self-perceptions, attitudes, appraisals, and motivations) learned through experiences with previous problems that can influence one’s awareness, motivation, or appraisal of specific problem situations, whereas problem-solving styles are the ways in which one attempts to understand, solve, or cope with specific problem (D’Zurilla, Nezu, et al., 2004; Nezu, 2004). Importantly, the term “social” is not meant to exclusively refer to social situations or problems, but refers to problems encountered in real-life social environments that can influence an individual’s daily functioning (D’Zurilla, Nezu, et al., 2004; Nezu, 2004).
Compared to emotional disorders, less research has been conducted examining the relationship between problem orientation and specific problem solving styles and behavioral problems (D’Zurilla, Chang, et al., 2004). In general, children and adults with ADHD have been found to have more social problem solving deficits compared to those without ADHD (Matthys et al., 1999; Sibley et al., 2010; Young, 2005). Specifically, boys with ADHD demonstrated lower social problem solving skills (i.e., deficits encoding social cues and generating possible responses) compared to children without ADHD (Matthys et al., 1999). In adults with ADHD, lower use of planful problem solving, and greater use of confrontational and avoidant strategies when faced with a stressor has been observed (Young, 2005). It has been suggested that deficits in social problem solving in individuals with ADHD may be due to decreased sustained attention or impulsivity (Matthys et al., 1999; Sibley et al., 2010).
However, these studies did not consider the potential impact of CDS symptoms on social problem solving. Whereas ADHD is often associated with strong tendencies of being distracted by external stimuli, CDS is hypothesized to be characterized by internal distraction (Becker & Barkley, 2021; Becker et al., 2023; Wiggs et al., 2024). These internal distractions may decrease their external attention (Becker & Barkley, 2021; Wiggs et al., 2023), which could potentially impede their ability to appropriately respond to a problem in the external environment, resulting in higher reports of avoidance style. In a recent qualitative study, parents of children and adolescents with CDS expressed that social interactions can be difficult for their children due to difficulties getting lost in thought and expressing themselves (Becker et al., 2022). Subsequently, individuals with CDS may interpret social situations as stressful or overwhelming, resulting in withdrawal or avoidance (Becker & Barkley, 2021; Becker et al., 2022). This withdrawal and social isolation appears similar to social difficulties experienced by those with social anxiety, which has recently been linked to CDS (Romano et al., 2019). Given what is known about CDS and social withdrawal and internalizing symptoms, it may be that CDS is related to specific difficulties with social problem solving.
The Current Study
Given the increased social impairment related to CDS, above and beyond internalizing symptoms (Becker, Burns, Garner, et al., 2018; Becker, Leopold, et al., 2016), understanding how CDS symptoms relate to problem-solving could have utility when determining future directions of CDS research and application. Of particular interest is how CDS symptoms relate to social problem solving in college students, as CDS symptoms are reported at a higher rate in college students compared to children and adults this population (Flannery et al., 2016; Wood, Potts, et al., 2017). Furthermore, college students often face high levels of stress and are at increased risk for mental health concerns (Regehr et al., 2013). This study examined CDS symptoms in relation to college students’ social problem solving, above and beyond ADHD and internalizing symptoms. We hypothesized that CDS symptoms would be uniquely related to greater negative problem orientation, lower positive problem orientation, and higher avoidance style when controlling for commonly associated domains of psychopathology (i.e., ADHD, anxiety, and depression).
Methods
Participants
Participants were 280 undergraduate students at a Southeastern university aged 18 to 23 years (M = 19.57, SD = 1.20). Freshman students made up 47.5% of the sample, followed by sophomores (25.4%), juniors (14.3%), and seniors (12.9%). Most of the sample identified as White (91.4%), Non-Hispanic/Latinx (97.5%), and female (77.9%).
Procedures
The study was approved by the institutional review board and all participants read an information letter and provided informed consent prior to completing the study through Qualtrics on an electronic device of their choice. Participants were recruited through an online research board for students enrolled in psychology courses at the institution. For their participation, participants earned 1 hour of credit that could be applied to a psychology course in which they were enrolled. Participants were excluded if more than 20% of their responses were missing, if (via validity questions) their responses indicated they may have responded in a careless manner, or if they themselves indicated that they did not respond accurately throughout the study. Finally, because the focus of the study is on understanding problem solving in a young adult college sample, individuals that were over the age of 23 and/or past their fourth year of undergraduate education were excluded.
Measures
CDS Symptoms
The Adult Concentration Inventory (ACI; Becker, Burns, Garner, et al., 2018) was used to assess self-reported CDS symptoms in the past 6 months. The ACI consists of 16 items with response options ranging from 0 (not at all) to 3 (very often), with higher scores indicating higher rate of CDS symptoms. Research with the ACI has demonstrated strong psychometric support (Becker, 2021). Through confirmatory factor analyses, 10 items on the ACI were determined to have good convergent and discriminant validity in distinguishing CDS from ADHD-inattention, anxiety, and depression in a large sample of college students (Becker, Burns, Garner et al., 2018). The 10-item ACI was found to have satisfactory reliability (α = .89) and concurrent validity in correlating with external constructs that have been previously identified as being related to CDS (i.e., executive dysfunction, functional impairment, and socioemotional adjustment; Becker, Burns, Garner, et al., 2018). In the present study, the scores from the ACI had an alpha of .89.
ADHD Symptoms
The Barkley Adult ADHD Rating Scale—IV (BAARS-IV; Barkley, 2011) was used to evaluate self-reported symptoms of ADHD. The 18 DSM-based items (1 = never or rarely; 4 = a lot) on the BAARS-IV contribute to ADHD-IN and ADHD-HI scores. The BAARS-IV has been found to have satisfactory internal consistency in samples of adults with ADHD (ADHD Inattention α = .902; ADHD Hyperactive–Impulsive α = .798) and adequate test-retest reliability (ADHD Inattention α = .66, ADHD Hyperactive-impulsive α = .74; Barkley, 2011). Research has also supported the measure’s construct validity, discriminant validity, criterion-related validity and rating relationship with adverse outcomes in several domains. The scores from the BAARS-IV had alphas of .77 and .85 for ADHD-HI and ADHD-IN, respectively.
Anxiety Symptoms
Anxiety symptoms were assessed using the Generalized Anxiety Disorders—7 (GAD-7; Spitzer et al., 2006), a 7-item self-report measure that assesses an individual’s symptoms of anxiety over the last 2 weeks. Item responses range from 0 (not at all) to 3 (nearly every day). The GAD-7 has been found to have satisfactory internal consistency (α = .92) and convergent validity with other measures of anxiety (e.g., Beck Anxiety Inventory, r = .72; Symptom Checklist-90, r = .74; Spitzer et al., 2006). In the present study, the scores from the GAD-7 had an alpha of .87.
Depressive Symptoms
The Patient Health Questionnaire—8 (PHQ-8; Kroenke et al., 2009) was used to evaluate symptoms of depression. The PHQ-8 includes eight of the nine symptoms used to assess DSM-based major depressive disorder, leaving out the item that inquiries about suicidal or self-injurious behavior, as it is less frequently endorsed and does not change the utility of the measure (Kroenke & Spitzer, 2002). Item responses range from 0 (not at all) to 3 (nearly every day). The PHQ-8 has shown to be valid in large populations and has demonstrated good sensitivity (70%) and specificity (98%) in detecting depressive disorders. In the present study, the scores from the PHQ-8 had an alpha of .85.
Social Problem-Solving
To assess ability to resolve problems in everyday living, the Social Problem-Solving Inventory-Revised (SPSI-R; D’Zurilla et al., 2002) was administered. The SPSI-R consists of 52 self-report items (0 = not at all true of me; 4 = extremely true of me), with higher scores on the two adaptive problem-solving dimension subscales indicating effective problem solving and higher scores on the three dysfunctional dimension subscales indicating ineffective problem solving (D’Zurilla et al., 2002). The SPSI-R measures five problem solving dimensions: positive problem orientation (e.g., “When I have a problem, I believe that it can be solved”), negative problem orientation (e.g., “I hate having to solve the problems that occur in life”), rational problem solving (e.g., “When I am trying to solve a problem, I keep in mind what my goal is at all times”), impulsivity/carelessness style (e.g., “When making decisions, I do not evaluate all my options carefully enough”), and avoidance style (e.g., “I put off solving problems until it is too late to do anything about them”). Within a normative sample of young adults, internal consistencies for the SPSI-R subscales ranged from acceptable to excellent (positive problem orientation α = .76, negative problem orientation α = .91, rational problem solving α = .92, impulsivity/carelessness style α = .83, avoidance style α = .88). In the present study, the scores from the SPSI-R subscales had alphas ranging from .71 to .92 (positive problem orientation α = .71, negative problem orientation α = .88, rational problem solving α = .92, impulsivity/carelessness style α = .79, and avoidance style α = .82).
Analyses
Bivariate correlations were conducted to investigate correlations among demographic variables, ADHD dimensions, anxiety, depression, CDS, and social problem solving dimensions. Regression analyses were conducted to examine the unique relationship of CDS with problem solving dimensions. Self-reported gender, ADHD dimensions, anxiety, and depressive symptoms were included as covariates in the regression models. Semi-partial correlations (spr) were obtained to examine the unique variance each individual independent variable explained in the full models. There were no violations of the main assumptions of linear models, as assessed by plotting residuals, examining the spread of scores, and checking variance inflation factors (VIF) and tolerance values.
Results
Correlation Analyses and Descriptive Statistics
Table 1 presents the descriptive statistics and correlations for the study variables. Positive problem orientation was positively related to gender (r = .14) and negatively related to depression (r = −.22), anxiety (r = −.21), ADHD-IN (r = −.26), and CDS (r = −.21), while negative problem orientation was negatively related to gender (r = −.15) and positively related to depression (r = .49), anxiety (r = .51), ADHD-IN (r = .51), ADHD-HI (r = .30), and CDS (r = .53). Rational problem solving was negatively related to ADHD-IN (r = −.12). Impulsivity/carelessness style was positively related to gender (r = .13), depression (r = .35), anxiety (r = .24), ADHD-IN (r = .42), ADHD-HI (r = .28), and CDS (r = .32). Avoidance style was negatively related to gender (r = −.14) and positively related to depression (r = .33), anxiety (r = .33), ADHD-IN (r = .50), ADHD-HI (r = .23), and CDS (r = .44). Men reported greater impulsivity/carelessness style whereas women reported greater avoidance style. Age and race were not significantly related to independent or dependent study variables.
Descriptive Statistics and Bivariate Correlations for Study Variables.

Note. For Gender 0 = female, 1 = male; For race 0 = white, 1 = non-white; ADHD-IN = ADHD inattention; ADHD-HI = ADHD hyperactivity-impulsivity; CDS = cognitive disengagement syndrome; PPO = positive problem orientation; NPO = negative problem orientation; RPS = rational problem solving; ICS = impulsivity/carelessness style; AS = avoidance style.
p < .05. **p < .01. ***p < .001.
Regression Analyses
Table 2 depicts the results of the regression analyses of CDS symptoms in relation to social problem solving orientation dimensions (i.e., negative problem orientation and positive problem orientation). Above and beyond gender, ADHD dimensions, and internalizing symptoms, CDS symptoms were significantly associated with negative problem orientation (spr = .12, p = .011). ADHD-IN contributed the most variance in the model (spr = .20, p < .001), followed by anxiety (spr = .18, p < .001). Gender, depression, and ADHD-HI were not significantly associated with negative problem orientation above and beyond the other variables in the model. In the regression examining the relationship with positive problem orientation, ADHD-IN (spr = −.19, p = .001), ADHD-HI (spr = .14, p = .013), and gender (spr = .12, p = .042) were significant, whereas CDS symptoms and internalizing symptoms were not significantly related to positive problem orientation (Table 2).
Regression Analyses Examining Gender, Internalizing Symptoms, ADHD Dimensions, and CDS Symptoms in Relation to Negative Problem Orientation and Positive Problem Orientation.
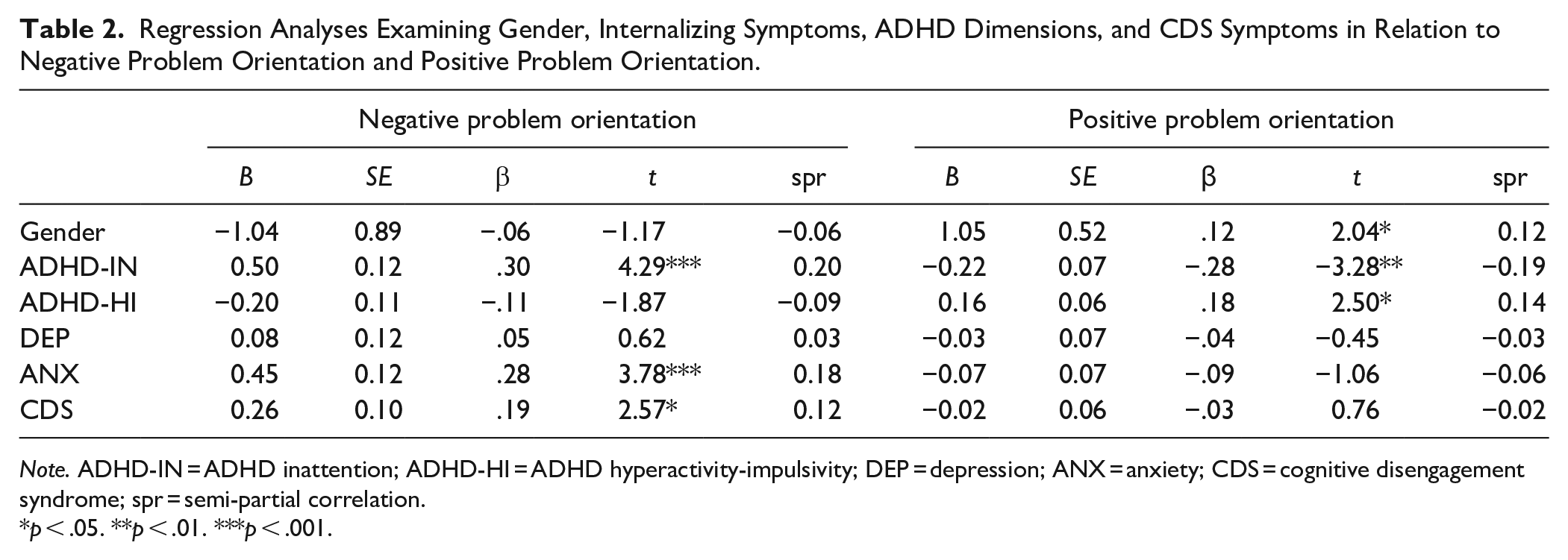
Note. ADHD-IN = ADHD inattention; ADHD-HI = ADHD hyperactivity-impulsivity; DEP = depression; ANX = anxiety; CDS = cognitive disengagement syndrome; spr = semi-partial correlation.
p < .05. **p < .01. ***p < .001.
Table 3 depicts the results of the regression analyses of CDS symptoms in relation to problem solving styles (i.e., avoidance style and impulsivity/carelessness style). Above and beyond gender, ADHD dimensions, and internalizing symptoms, CDS symptoms were significantly associated with avoidance style (spr = .11, p = .028). ADHD-IN contributed the most variance in the model (spr = .30, p < .001), followed by ADHD-HI (spr = −.12, p = .016). Gender, depression, and anxiety were not significantly related to avoidance style when accounting for other variables. In the regression examining the association with impulsivity/carelessness style, ADHD-IN (spr = .20, p < .001), gender (spr = .16, p = .003), and depression (spr = .13, p = .019) were significant, whereas CDS symptoms, ADHD-HI, and anxiety were not significantly related to impulsivity/carelessness style (Table 3).
Regression Analyses Examining Gender, Internalizing Symptoms, ADHD Dimensions, and CDS Symptoms in Relation to Avoidance Style and Impulsivity/Carelessness Style.

Note. ADHD-IN = ADHD inattention; ADHD-HI = ADHD hyperactivity-impulsivity; DEP = depression; ANX = anxiety; CDS = cognitive disengagement syndrome; spr = semi-partial correlation.
p < .05. **p < .01. ***p < .001.
Discussion
The current study provides novel insight on the relationship of CDS and problem solving dimensions when accounting for commonly co-occurring difficulties (i.e., ADHD, anxiety, and depressive symptoms). This study adds to the growing literature highlighting the unique association between CDS and everyday functioning.
When accounting for ADHD and internalizing symptoms, CDS symptoms were significantly related to negative problem orientation and avoidance style but were not significantly related to positive problem orientation or impulsivity/carelessness style. The lack of association between CDS and positive problem orientation suggests that CDS symptoms (e.g., daydreaming, mind-wandering, and mental fog) may not impact one’s perception or knowledge of how to solve problems in a systematic way, but rather impact functioning in the moment and lead to social difficulties (Flannery et al., 2016). Social and other daily life impairments experienced by individuals with CDS may not be due to lack of knowledge when faced with social problems, but rather due to other factors.
Our finding that CDS is uniquely related to negative problem orientation, which includes avoidance of the problem, lack of confidence in one’s ability to solve the problem, and viewing the problem as a threat, aligns well with Yung et al.’s (2022) suggestion that individuals with CDS may have increased difficulties in responding or attending to information when faced with conflict or difficult situations. Difficulties sustaining attention could lead to increased difficulty in recognizing or attending to social cues, which may lead to more withdrawal in social situations. When individuals with high CDS symptoms are faced with a daily life problem, they may have difficulties attending to the problem or working through relevant steps needed to identify solutions for the problem, which may then lead to lower confidence, withdrawal, and avoidance. Indeed, previous research found emotion dysregulation, which includes the ability to engage in goal-directed behavior, to cross-sectionally mediate the association between CDS and social impairment in college students (Flannery et al., 2016). Difficulty engaging in goal-directed behavior is likely to increase avoidance when faced with problems, which aligns with the social withdrawal associated with CDS symptoms.
Indeed, CDS symptoms were significantly related to avoidance style even after controlling for the other variables. ADHD-HI and ADHD-IN symptoms were also significant in the model, with ADHD-IN accounting for the most variance. Interestingly, ADHD-HI was negatively related to avoidance style, whereas CDS and ADHD-IN were both positively related to avoidance style. This suggests that the impairment in problem solving faced by individuals with ADHD may be due to different deficits. Specifically, inattentive symptoms may impact social perception and lead to avoidance, whereas hyperactive/impulsive symptoms may impact behavior inhibition and impulsivity in situations (Semrud-Clikeman, 2010). Differences in social deficits have been identified between subtypes of ADHD in children, such that ADHD-IN is related to deficits in assertiveness and ADHD-HI is related to deficits in self-control (Solanto et al., 2009). The impulsivity that characterizes the hyperactive/impulsive presentation of ADHD may eliminate the likelihood of avoidance when faced with problems and lead to more of a confrontational approach, whereas inattentive symptoms may lead to an escape-avoidance approach. One study found that adults with ADHD-IN had greater harm avoidance and less self-directedness (e.g., ability to regulate and adapt behavior when faced with a situation) compared to those with ADHD-combined subtype (which includes symptoms of hyperactivity and impulsivity), indicating that inattentive symptoms may lead to greater avoidance when faced with problem situations (Salgado et al., 2009).
Another interesting finding was that anxiety and depression symptoms were not significantly related to avoidance style in the regression analysis, despite previous research indicating a strong relationship between both anxiety and depression and avoidance style. It may be that the association between internalizing symptoms and avoidance style is better attributed to other factors that commonly co-occur with internalizing symptoms, but are not always measured in research studies, such as inattention, daydreaming, withdrawal, or rumination. One study found that avoidance mediated the association between ADHD and internalizing symptoms, indicating that avoidance may actually contribute to the development of anxiety or depression for individuals with ADHD (Bodalski et al., 2019). In addition, findings from a recent qualitative study indicated that children and their parents reported that cognitive CDS symptoms (e.g., daydreaming and getting lost in thought) impacted their ability to finish their thoughts or express themselves, resulting in challenges in social interactions (Becker et al., 2022). This indicates that the cognitive challenges related to CDS may lead to withdrawal, avoidance, and subsequent social difficulties.
Limitations and Future Directions
The cross-sectional nature of this study precludes establishing temporal precedence, and longitudinal research is needed to evaluate the relationship between social problem solving, CDS, and internalizing symptoms to better understand if problem solving deficits potentially mediate the association between CDS and internalizing symptoms. Additional limitations include limited generalizability, as the current study collected data from college students enrolled in psychology undergraduate courses at a Southern university, with a sample consisting of primarily White females in the first year of college. Future research should aim to prioritize diverse and underrepresented samples. In addition, this study relied on self-report measures to evaluate psychopathology symptoms, as well as social problem solving processes, which is susceptible to mono-informant bias. Replication of these findings is needed in longitudinal studies using a multi-method (e.g., clinical interview) and multi-informant (e.g., caregivers and romantic partners) design. In addition, the inclusion of other methods to evaluate problem solving should be considered in future research, including measures that can evaluate one’s actual abilities when faced with a problem.
Conclusions
Findings contribute to the growing CDS literature by evaluating for the first time the association between CDS symptom severity and social problem solving processes. Specifically, even when controlling for common co-occurring symptoms of ADHD, anxiety, and depression, we found CDS to be significantly related to maladaptive problem solving processes (i.e., negative problem orientation and avoidance style). Findings indicate that evaluating for CDS symptoms may be useful for college students that exhibit maladaptive problem solving. Results further highlight the potential utility of interventions that reduce negative problem orientation in adults with CDS symptoms to prevent development of anxiety or depression. Further, ADHD symptoms were significantly associated with social problem solving deficits. ADHD and CDS symptoms commonly co-occur in adults, and those with elevated symptoms of both ADHD and CDS face increased impairment compared to those with only ADHD symptoms or only CDS symptoms. This highlights the importance of considering problem solving interventions for those with elevated ADHD and CDS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.