
Abstract

Background
Radiation dermatitis is a common side effect of radiation therapy. While significant dermatitis rarely results from lower dose radiotherapy (e.g., single fraction palliative radiotherapy), it is common with higher dose radiation typically used in the definitive or adjuvant treatment of cancer. It results from skin damage due to ionizing radiation and typically develops within 1–4 weeks of starting therapy. This Fast Fact will discuss the clinical presentation and management of radiation dermatitis.
Natural History
Radiation dermatitis is characterized by acute and late skin effects. The first dose of radiation damages basal keratinocytes of the epidermis, leading to an inflammatory response in the epidermis and dermis. It also disrupts the barrier function and self-renewing property of the epidermis, damages epidermal DNA, and alters the dermis. Subsequent treatments do not allow time for cells to repair or proliferate, thus significant skin reactions occur.1,2 Use of sensitizing chemotherapy and intrinsic factors such as chronic sun exposure, smoking, obesity, or diabetes can worsen its severity. 3
Clinical Presentation
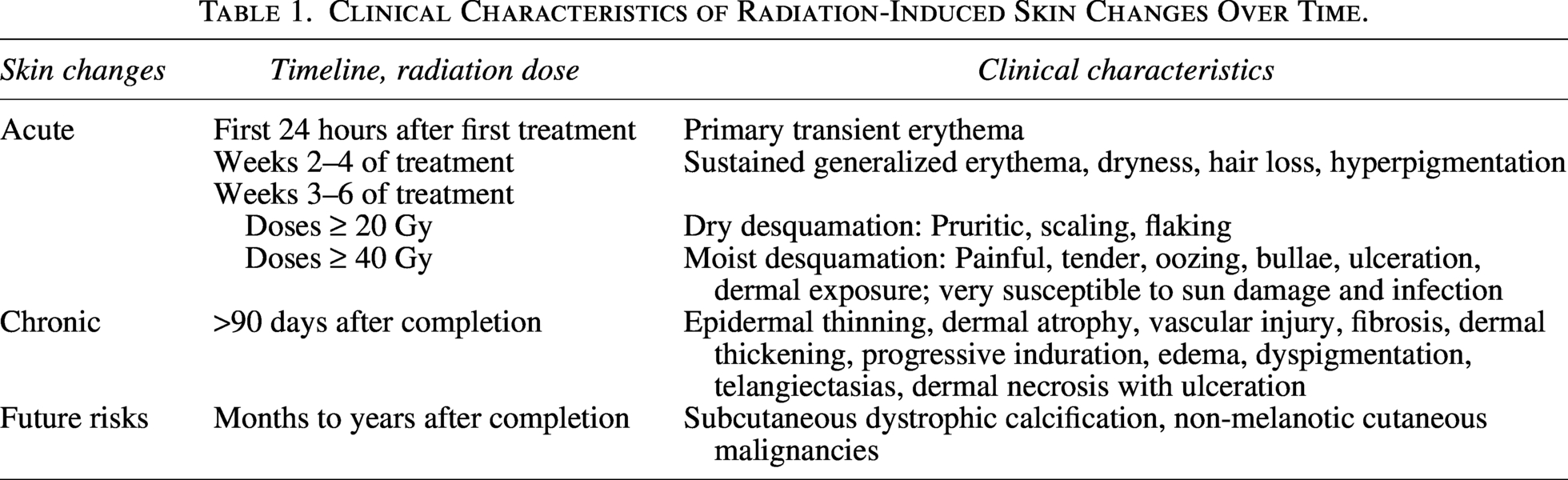
Severe radiation dermatitis is painful and markedly worsens quality of life. It can lead to hospitalization, interruption of radiotherapy, and is occasionally life-threatening 3 (Table 1).
Clinical Characteristics of Radiation-Induced Skin Changes Over Time.
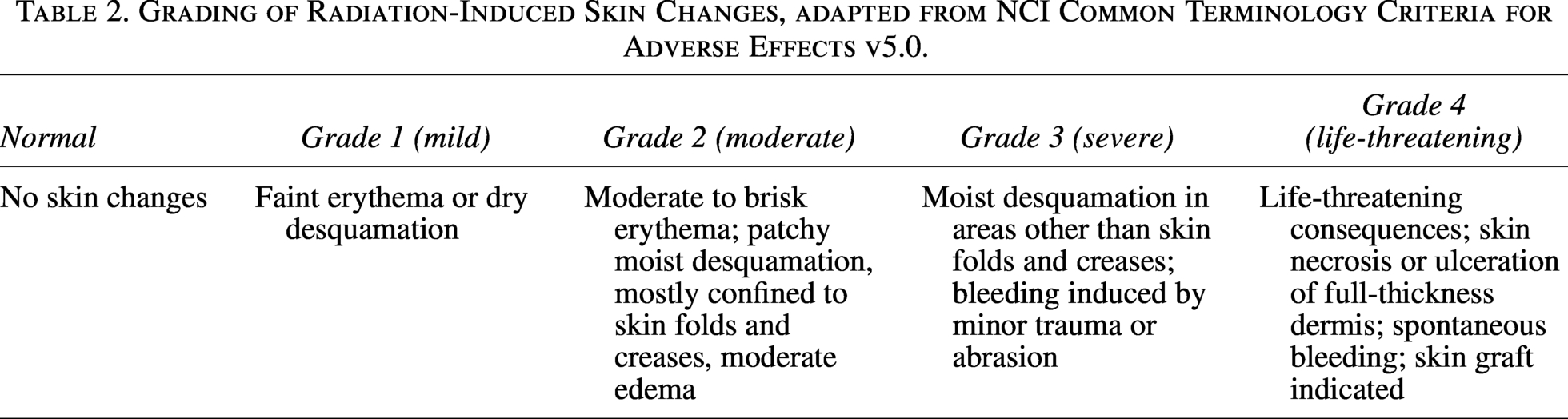
Grading
This table is adapted from NCI Common Terminology Criteria for Adverse Effects 4 (Table 2).
Management
Data are very heterogeneous; however, broad consensus exists in some areas. The Oncodermatology Study Group of the Multinational Association of Supportive Care in Cancer published guidelines for the prevention and management of radiation dermatitis.
5
Prevention: there is broad consensus on recommending daily washing of irradiated skin with mild soap and water, moisturizing irradiated skin with non-fragranced lotions such as Aquaphor, and the use of topical mometasone, betamethasone, or silver sulfadiazine to prevent dermatitis.3,6 Treatment:
Grades 1 and 2: Apply a saline-soaked gauze to the affected area for 10 minutes, followed by an occlusive emollient application such as Aquaphor, one to three times daily. Grade 3: Use hydrogel dressings and silver sulfadiazine for moist desquamation. Topical steroids can be used for inflammation or itching in surrounding dry and intact skin. Systemic analgesia is indicated to manage moderate-to-severe pain, usually with acetaminophen, non-steroidal anti-inflammatories, and/or opioids. Provide patient education on the avoidance of friction, trauma, and irritants such as perfume or alcohol-based products, and watch for signs of infection such as purulence or malodor. Grade 4: Hospitalize and involve specialists (wound care, plastic surgery, etc.) as necessary.
Summary
Although radiation oncologists are usually the primary specialists addressing dermatitis, it is essential for all clinicians involved in a patient’s care to actively assess radiation dermatitis, recognize its presentation, and deliver effective management while maintaining clear, coordinated communication with specialty teams. Wound care, pain management or palliative care, and surgeons may need to be consulted for optimal management.
Footnotes
Author Disclosure Statement
The authors have no relevant conflicts of interest to disclose.
Funding Information
The authors have no funding to report.