
Abstract
In recent years, the spread of mobile communication devices such as smartphones has been markedly rapid. With this technological diffusion, mobile health (mHealth) has become an increasingly important issue. In particular, there is an increasing interest in smartphone apps improving public health. Although there is increased availability of mobile devices and health apps, little is known about motivational factors predicting health app adoption and use. The aim of this study was to identify motivational factors that predict the adoption and use of health apps (i.e. health app engagement). To identify the motivational factors, 391 college students were surveyed and survey questions considered the effects of media exposure to health information, interpersonal communication on health issues, and psychological factors (e.g. attitude, usefulness, peer norm, and self-efficacy) on health app engagement. Our results confirm the effect of attitude (β = 0.36) and usefulness are (β = 0.33) on mHealth App usage. Furthermore, we found that age (β = 0.11) and reading news articles about health (β = 0.13) predict mHealth App usage. Theoretical and practical implications and suggestions for future research are discussed.
Introduction
In recent years, the popular use of mobile communication devices including mobile phones (e.g. 2G feature phones), smartphones (e.g. iPhone and Android-based phones), and tablet computers (e.g. Apple iPad and Samsung Galaxy Note)—hereafter, smartphones will be used to also refer to app utilizing devices including iPads—has markedly increased worldwide. According to a Pew report (Pew Research Center, 2014), 90% of American adults have a cell phone, 58% of which are smartphones. This represents 64% of total mobile phone users, a 10% increase in 2 years from December, 2012. Furthermore, the adoption rate of smartphones is notable among younger generations (over 80% of young adults aged 18–29; 74% of 30–49 adults; 49% of 50–64 adults).
With this technological diffusion, mobile health (mHealth)—the use of mobile computing and communication technologies in health care—has become an increasingly important issue in a number of disciplines such as health communication, public health, and health promotion. In particular, there is a growing interest in smartphone apps as a tool for interventions that deliver health information. For example, there has been a significant increase in the numbers of health-related applications (apps) available on the two major mobile device software platforms, App Store for iOS-based mobile devices (e.g. iPhones and iPads) and Google Play for Android-based mobile devices (e.g. Samsung Galaxy, Google Nexus, HTC, and Motorola Droid). According to Kamerow (2013), there are approximately 100,000 health-oriented apps on these software platforms—a number that will continue to grow. In addition, with the development of mobile technology, such GPS-based exergames and gamified geosocial apps as mobile, location-aware apps, and devices with social and gamification functions contributed to engagement in physical activity as well as health app involvement among youth (Boulos and Yang, 2013; Brauner et al., 2013). Furthermore, as to the mobile use in public health, literature on communication technology in health has yielded positive outcomes. For example, Kristjánsdóttir et al. (2013) found that a smartphone-delivered intervention with diaries and personalized feedback could reduce catastrophic events, functional impairments, and symptoms in women with chronic widespread pain. In addition, Snuggs et al. (2012) found that health-oriented mobile intervention helped prevent relapses among ex-smokers and were implemented economically and quickly.
However, with respect to the app use, while 84% of smartphone users have downloaded at least one app, only 19% had downloaded apps intended to improve health (Fox and Duggan, 2012). In other words, from a health promotion perspective, the fact that less than a quarter of app users utilized health-related apps can be concerning. For example, consider the high levels of obesity among the American adult population, which poses both health and financial concerns. Medical costs associated with obesity were US$147 billion in 2008 in the United States (Finkelstein et al., 2009). What if there were a simple and inexpensive method of distributing health information and preventive practices for not only obesity, but other harmful diseases? In addition, there is an increasing interest in psychological wellness and well-being enhancing the quality of life and health (Alagöz et al., 2010). Furthermore, the need for well-documented methods for promoting wellness is large as a very important part of public health and mHealth (Kjellgren et al., 2007). For this reason, health communication scholars and public health professionals are exploring smartphone health apps as a tool for addressing public health problems.
Despite the increased availability of smartphones and health apps, little is known about motivational factors that lead one to adopt and utilize health apps. In other words, most of the previous studies in this area have investigated the effectiveness of specific health apps (Cho et al., 2014), focusing on convenience, effectiveness, and uniqueness for certain health conditions such as obesity (e.g. Carter et al., 2013), health behavior modification (e.g. Willems et al., 2013 for smoking cessation), and disease management such as diabetes (e.g. Årsand et al., 2008 ; Tsai et al., 2007 ). Although these studies meaningfully contribute to the development of literature on public health and mHealth, without understanding of factors that facilitate adoption and use of health apps, it would be difficult to fully comprehend individuals’ health apps activities (Alagöz et al., 2010), designing of mobile medical (or telemedical) applications including self-care technology for the elderly or people who are suffering from chronic diseases (Holzinger et al., 2011; Ziefle et al., 2013), and create communication strategies for the improvement of public health (Cho et al., 2014). For this reason, the aim of this study is to identify motivational factors that encourage the adoption and use of health apps.
In this study, a three-step procedure is used to gain a deeper insight of what leads to an individual actually use a health-related application. First, existing information available from previous research in communication, health promotion, information and communication technology (ICT), and psychology is employed to identify key concepts that may predict app adoption and use. Second, the resultant hypotheses are tested empirically with a survey of 391 university students, indicating what factors actually predict app-related behavior. Finally, the empirical results and their implications are discussed as well as suggestions for future research.
Literature review
Communication technology use and public health
In recent years, the use of communication technologies has grown exponentially. This advancement of ICT has presented unprecedented opportunity in public health campaigns and research. Specifically, ICTs (e.g. smartphones, Personal digital assistants (PDAs), etc.) make it easier to reach large audiences and monitor users’ health-related behavior patterns quickly and conveniently (Owen et al., 2002). In addition, new communication technologies have greater capacities for providing appropriate and tailored functions and information at the user’s convenience (Owen et al., 2002). Additionally, the technology enables health programs and services to utilize dynamic graphics, sound, and tailored program content, leading to users’ involvement in the use of the programs. This allows for the use of graphical and audio interfaces that enable users with limited reading skills to get information that may not be accessible through conventional print media such as books, newspapers, and magazines (Owen et al., 2002). Thus, the enhanced involvement may contribute to the improvement of public health.
In fact, research has already begun to indicate that ICTs are effective platforms for delivering interventions aimed at lifestyle behavior modification in a wide variety of preventive, health-care, and/or clinical contexts. For example, Holzinger et al. (2010) found graphical analysis results offered by an app may encourage the app users to use the app and check their health information in terms of smoking, alcohol, obesity, dietary habits, and physical activity, resulting in the increase in and reinforcement of one’s health awareness. In addition, Lee et al. (2010) developed a smartphone game application, SmartDiet, providing personalized diet profile and information about nutrition and investigated the relationships between app use, users’ daily nutrition intake, and patterns of daily physical exercise. During a 6-week study period, with the data transmitted from participants’ smartphones, the authors evaluated the effectiveness of the app on the knowledge of dietary information, weight control, and user satisfaction. The authors found a positive effect of the app use on body composition measures: fat mass, weight, and body mass index all decreased among active users.
Health-related smartphone apps show great potential for promoting positive changes in health behavior and an ability to contribute to the improvement of public health. However, understanding the influencers regarding what factors both facilitate the app installation and the frequency of app usage is a prerequisite step to build up communication strategies for public health campaigns to encourage smartphone users to use health apps—what is it that actually facilitates app use?
Contribution of communication to public health
Media exposure to health information
When it comes to promoting behavior modifications, scholars have considered the role of traditional mass media. For example, Rojas et al. (2011) examined the effect of media exposure to social issue-related information through traditional media such as newspapers, magazines, radio, and TV on a series of pro-social behavioral outcomes such as doing voluntary work, participation in community work, and attending a local civic forum. The authors found that media exposure to social issues had a positive effect on social participatory behavior. In addition, Shah et al. (2009) examined the role of media use, especially public affairs news consumption via broadcast, print, and online sources in youth socialization such as civic participation and political participation. In general, the authors found that media use had a positive impact on the behavioral outcomes as well.
The connection between media and behavior in the health context has been supported by past research. For instance, Kwon et al. (2013) investigated how informational media use contributes to the improvement of health behaviors, including fruit and vegetable consumption. The authors found positive relationships between traditional media (e.g. TV health news and print health news), new media (e.g. the Internet health news), and fruit and vegetable consumption. In addition, with the data from the 2005 Health Information National Trends Surveys (HINTS), Redmond et al. (2010) examined the relationship between the source type of mass media and adoption of health behaviors (e.g. vegetable intake, exercise, and nonsmoking) and preventive health behaviors (e.g. mammography, Pap test, colonoscopy, and sigmoidoscopy). In terms of adopting positive health behaviors, their first analysis on 2005 HINTS revealed that reading printed media (e.g. health sections on newspaper and magazine) has a positive impact on participants’ diet and nonsmoking behavior. With regard to preventive health behavior, traditional media (e.g. print media and TV) and new media (e.g. the Internet) positively increased the willingness to take screening tests for women, such as mammograms, Pap, and/or colonoscopy tests.
Following the previous research considering the effect of media on behavioral outcomes, this study expects the positive relationship to be found in a health-related technology use context.
Specifically, the more people watch health-related TV contents, the more they are likely to use a health app. Also, the more people consume print media regarding health issues, the more they are likely to accept health apps. Finally, the intensity of health apps use is dependent on how much people read health information on the Internet. Thus, the following hypotheses are posited:
Health-related interpersonal communication: Face-to-face versus online
Along with the positive effect of health media use on health behavior modification, research has drawn attention to the role of interpersonal communication. Scholars have tried to explore how interpersonal communication either increases people’s health knowledge or persuades them to modify their behaviors toward a healthy lifestyle.
In general, similar to media, people may obtain health information through interpersonal communication (Jones et al., 2007). Social interactions fostered by interpersonal communication can contribute to people’s intention to change their preexisting unhealthy behavior like smoking (van den Putte et al., 2011). Previous research in this area has found evidence that interpersonal communication has a positive impact on adaptive health behaviors. For example, Noar et al. (2006) found that the greater the likelihood of a person talking with his or her sexual partner about safer sex is, the greater the likelihood of condom use is.
Recently, research on the relationship between interpersonal communication and health behavior has been interested in online environments (Ancker et al., 2009; Gooden and Winefield, 2007; Johnsen et al., 2002; Schwarzer and Satow, 2012). Similar to the effects of face-to-face communication, Ancker et al. (2009) found that web-based peer-to-peer communication promotes disease prevention behaviors in relation to cancer risks. In addition, Schwarzer and Satow (2012) found that those who tended to post frequent messages regarding smoking cessation programs on a bulletin board are less likely to smoke. Given the discussion above, this study expects similar relationships in a health app context. That is, the more people engage in face-to-face communication as well as online communication on health issues, the more they are likely to use health apps. Thus, the following hypotheses are posited:
Psychological determinants
Along with the effect of communication (e.g. media use and interpersonal communication) on communication technology adoption and use, understanding why people accept or reject communication technologies from a psychological perspective has been one of the most challenging issues in the disciplines of communication, health management, public health, and strategic communication (Park et al., 2007; Swanson, 1988). To fulfill the need, various efforts addressing why people decide to adopt and use communication technologies have identified a number of psychological factors facilitating the actual adoption and use of communication technologies. Technology acceptance research has tested many models such as the theory of reasoned action (TRA) (Fishbein and Ajzen, 1975) (see Figure 1), the theory of planned behavior (Ajzen, 1991), which is an advanced model of the TRA, and the technology acceptance model (TAM) (Davis et al., 1989) (see Figure 2), which is based on the TRA and innovation diffusion theory (Rogers, 1995). In addition, Venkatesh et al. (2003) reviewed and evaluated models on technology acceptance including the TAM 1–3. Then, they yielded the Unified Theory of Acceptance and Use of Technology that integrates and unifies the characteristics and elements of TAM-related models and suggested four key facilitators such as performance expectancy, effort expectancy, social influence, and facilitating conditions.
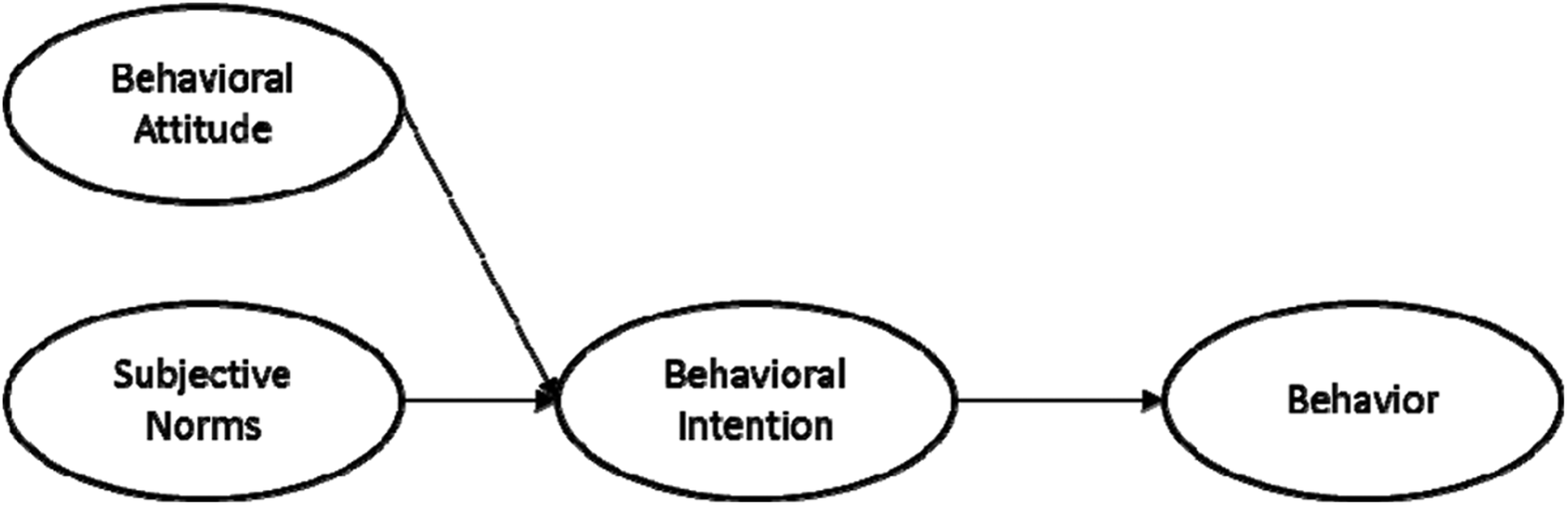
The model of theory of planned behavior.

Technology acceptance model.
Although a significant amount of new communication technology adoption research has accumulated, efforts to integrate different user characteristics regarding the technology adoption are relatively scarce (Park, 2010). Since this study seeks to better understand perceptual and attitudinal factors that may facilitate the adoption and use of health apps, along with media factors, this study investigates the roles of the following factors selected through the literature review on technology adoption: self-efficacy, usefulness, subjective norm, and attitude.
The present study has the following two purposes. First, the study will identify the factors affecting users’ health app involvement. They include not only users’ personal/individual factors related to technology adoption. Next, this study is designed to suggest an integrated model identifying communication effects.
Attitude toward actual behavior
One variable often measured to predict technology adoption is the attitude toward the recommended behavior, in this case, app adoption. An attitude can be described as “a relatively simple unidimensional concept, referring to the amount of affect for or against a psychosocial object” (Fishbein, 1967: 478). Based on this notion, in this study, attitude refers to an individual’s positive or negative feeling (evaluative affect) about performing a target behavior, that is, the adoption and use of health apps (Fishbein and Ajzen, 1975: 216). Such attitudes have been found to predict behavior directly or indirectly working through intention toward the target behavior, which has been considered and used as a crucial predictor of (future) actual behavior. This relationship has been identified in a number of health contexts. For example, Kwon et al. (2013) found a positive relationship between attitude toward healthy eating and healthy eating behavior. Also, Deng et al. (2014) found that attitude can be used to predict intention to use mHealth services for both the middle-aged and older users. In addition, attitude has been found to be a strong determinant of actual health behaviors such as smoking (Borland et al., 1991); weight loss (Schifter and Ajzen, 1985); having basic health checkups, screenings, and seeking medical care (Conner and Norman, 1994; Devellis et al., 1990; Godin et al., 1992); limiting infant sugar intake (Beale and Manstead, 1991); eating behavior (Sparks et al., 1992); and exercising (Yordy and Lent, 1993). Given these consistent findings linking attitudes as a key antecedent of behaviors, we expect that a favorable attitude toward health apps is an important precursor of willingness to use the health app. Thus, the following hypothesis is posited:
Subjective norms: Peer norm
As a concept, a subjective norm represents the influence of the social environment on a target behavior (Fishbein and Ajzen, 1975
, 2010). It pertains to whether social norms encourage or disapprove of a particular behavior. In general, previous work on subjective norms has yielded evidence that they have an important effect on outcomes including behavioral intentions and actual behavior. For example, Hauser et al. (2011) examined the role of perceived subjective norms on volunteering and found a positive relationship. In a technology context, Cheung and Lee (2010) found a positive influence of subjective norms in social networking site use. In health contexts, the consistent findings have been identified. For instance, Hyde and White (2009) investigated the role of subjective norms in registration for organ donation and found the positive impact. Recently, Xue et al. (2012) found subjective norms significantly predict adoption intentions to use Infohealth, a mobile phone-based intervention, among aging women in Singapore. In addition, extensive work in social psychology maintains that peer norms (as a subjective norm) can exert forceful influences on behavior decision among young people (Gunther et al., 2006). For this reason, this study investigates the role of norms in the adoption and use of health apps. That is, the more people perceive peer norm as being supportive, the more they are likely to use health app. Thus, this study posits the following hypothesis:
Usefulness
In a technology adoption context, usefulness refers to job-related productivity and performance (Davis, 1989). Previous research on the theme has generated evidence that perceived usefulness has a direct effect on intention toward a target behavior, leading to actual behavior or direct effect on one’s actual behavior. For example, Wu et al. (2007) examined what determines mobile health-care system acceptance by health-care personnel. They found that perceived usefulness along with compatibility and perceived ease of use significantly impact the behavioral intention of accepting mobile health-care systems. Also, Curioso and Kurth (2007) examined the perception of communication technologies such as the Internet, cell phones, and PDAs being used by HIV-positive people in Peru. People living with HIV regard communication technologies as useful in supporting their HIV care and staying connected with society. Qin et al. (2011) investigated the effect of usefulness on intention to use a communication technology, social networking sites (e.g. Facebook and Twitter) and found a positive relationship between them. In addition, Pena et al. (2009) found that mobile phone technology can be adopted by parents who have children with type 1 and type 2 diabetes in order to help manage their children’s diabetes. Also, Jen (2010) examined the adoption of mobile weight management services in a virtual community. The results revealed that perceived usefulness of the service had an impact on user’s intention to use the service. Also, Svendsen et al. (2009) found a direct as well as a mediating effect of perceived usefulness on intention to use mobile system. Thus, it is expected that the more people perceive the health-related technology to be useful, the more they are likely to use health app. Based on those findings, the following hypothesis is suggested:
Self-efficacy
The most common concept used in research on communication technology adoption and use is Bandura’s concept of self-efficacy (Bandura, 1977). According to social cognitive theory, self-efficacy refers to the assessment of one’s own ability to perform a particular behavior (Bandura, 1977). Individuals tend to be more likely to engage in a particular behavior if they believe that they have an enough capability to perform the target behavior. The concept of self-efficacy has been explored in the mHealth context and a variety of communication technology-related contexts. For example, Lv et al. (2012) examined mHealth service acceptance with three different age groups using protection motivation theory. The results revealed that response efficacy and self-efficacy were significant predictors of service adoption intentions for the group of young adults and middle age group. In addition, Lin and Huang (2008) investigated the effect of self-efficacy on the adoption of knowledge management systems and found the positive effect. Given the findings, it is expected that the more confident people are in dealing with communication technology devices, the more likely they are to adopt the health app. Thus, the present study posits the following final hypothesis:
In sum, we hypothesize that the media exposure to health-related TV, print, and Internet messages may positively impact health app use. Also, face-to-face communication and online communication regarding health issues will positively influence health app adoption. In addition, psychological factors are expected to play important roles in adoption behavior. Specifically, attitude toward health app use behavior, peer norms, usefulness, and self-efficacy will positively affect the intensity of health app use. Based on the arguments above, the hypothetical research model is provided below (see Figure 3).
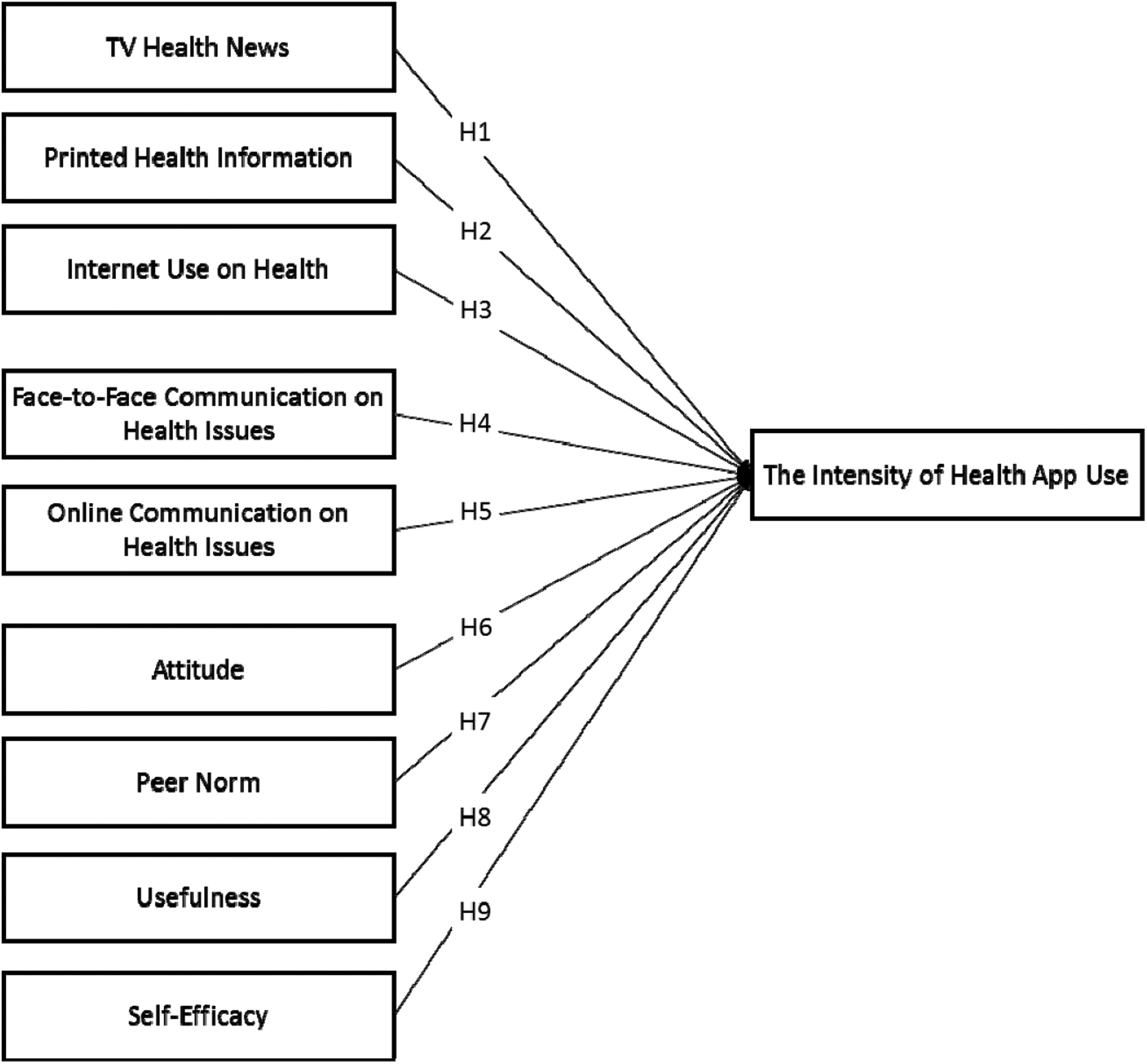
Hypothetical research model.
Method
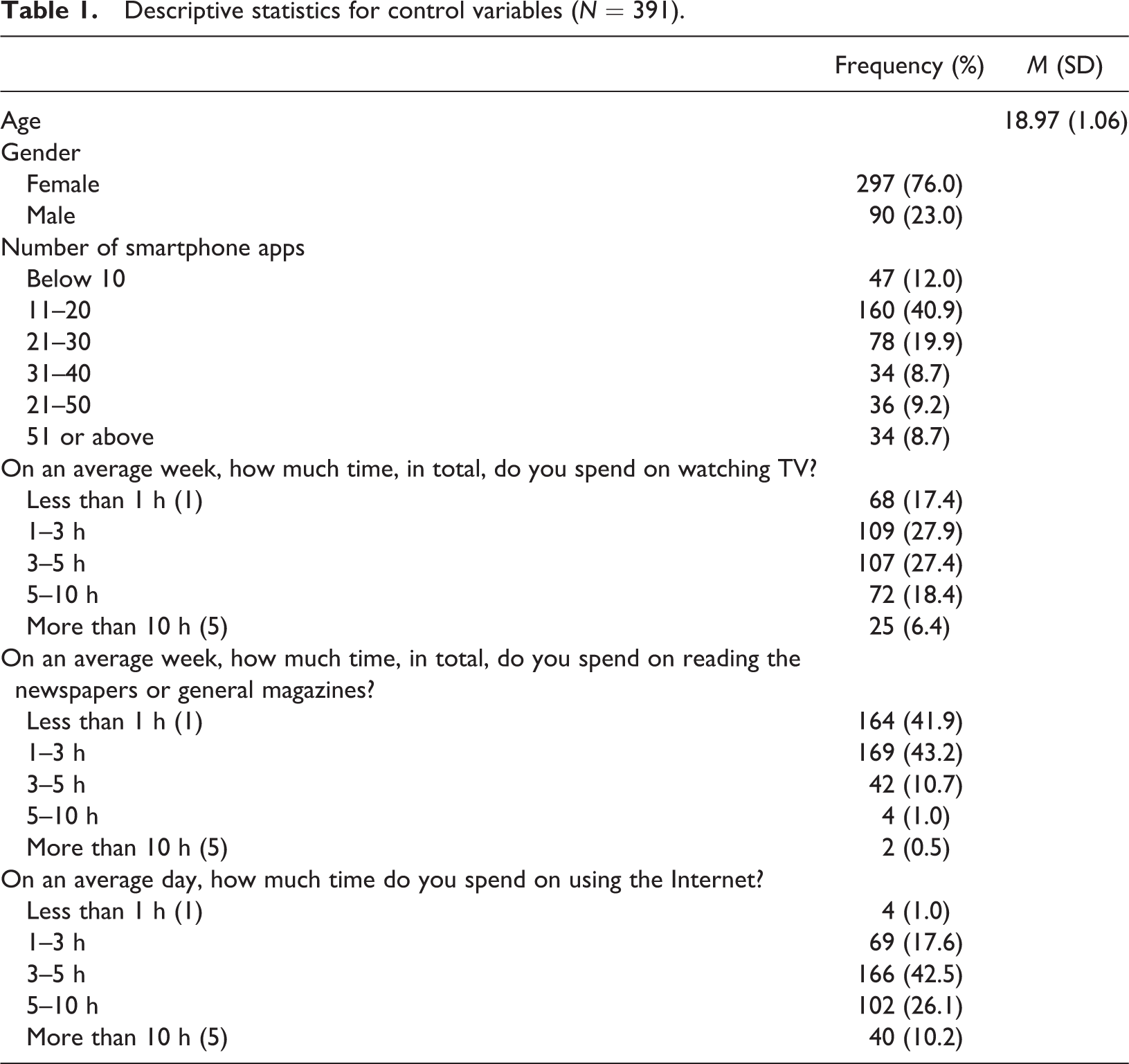
To obtain the sample, a survey invitation with a short description of the study, information about confidentiality, participation incentives, and a sign-up page was sent through a website that advertises ongoing research studies to classes at a large Midwestern University after obtaining instructor’s permission. A total of 462 undergraduate students signed up and 85% (N = 391) participants completed the online survey and received extra credit. Of the 391 subjects, 76.7% (n = 297) were female. The participants’ average age was 18.97 years (SD = 1.06). With respect to the narrow age range and the majority of the participants, young female participants, recent reports on health and communication technology adoption have considered young college female students as a broadly representative sample of health app users. For example, Fox and Duggan (2012, 2013) reported that some demographic groups such as those between the ages of 18 and 29, college and college graduates, and females are more likely to use their cell phone including smartphone use for health purposes such as health information seeking and tracking a health indicator or symptom than others. In addition, the reports mentioned that younger people are more likely to own a smartphone. Therefore, the sample of the study would be a general representation of health-oriented smartphone app research. Additional demographic characteristics of the respondents are shown in Table 1.
Descriptive statistics for control variables (N = 391).
Operationalization
Intensity of smartphone health apps use
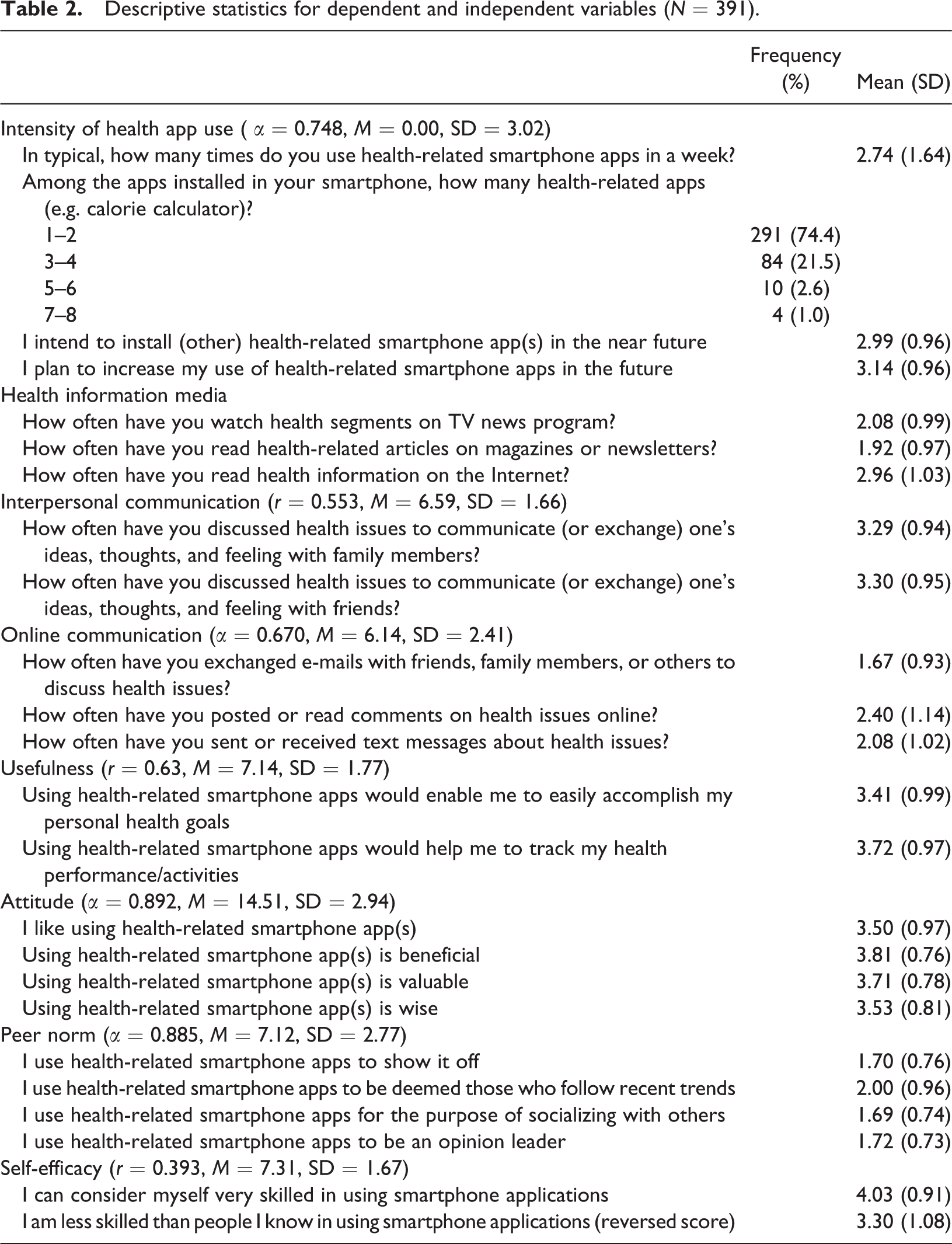
In literature on media, among the popular approaches to measure media use are the frequency of exposure/use and time spent using the medium. However, such approaches have some limitations in capturing the richness of media experiences, such as the depth of involvement with interactive communication technologies (Valenzuela et al., 2009). To account for this limitation, the current study employed a more complete measure: intensity of smartphone health apps use, an approach was suggested by Ellison et al. (2007). This intensity measure was created to measure users’ active engagement in smartphone health apps, based on (1) the numbers of smartphone health apps installed on one’s smartphone, (2) the frequency of app use, and (3) intention to both download/install other health apps and increase the frequency of app use in the near future. Participants were asked questions such as, “How many times do you use health-related smartphone apps in a week?” To create the intensity measure, four individual items were first recoded to range from 0 to 1 before taking an average due to the different response scales of the four items and to ease the interpretation of the statistical analyses (Cronbach’s α = 0.75, M = 0.00, SD = 3.02, see Table 2).
Descriptive statistics for dependent and independent variables (N = 391).
Health media exposure
To measure media exposure to TV health information including news content, we assessed the frequency of viewing TV news programs on health subjects. The item: “How often have you watch such health segments, which were embedded in some local or national TV news programs, in the past 30 days?” was measured on a 5-point scale, ranging from 1 (not at all) to 5 (very frequently) (M = 2.08, SD = 0.99). Print health news use was measured by a single item: “How often have you read such magazines or newsletters that focus on health in the past 30 days?” on a 5-point scale ranging from 1 (not at all) to 5 (very frequently) (M = 1.92, SD = 0.97). Finally, Internet health news use was measured by a single indicator about the amount of exposure to health news online. Respondents were asked to answer how often they have read health information on the Internet in the past 30 days, followed by a 5-point scale ranging from 1 (not at all) to 5 (very frequently) (M = 2.96, SD = 1.03).
Interpersonal communication: Face-to-face and online
Face-to-face communication consisted of two items gauging how often respondents talked about health with (1) family members and (2) friends. Next, online interpersonal communication was measured using the following three items: (1) communication through e-mails on health issues, (2) reading health-related comments posted online, and (3) communication through text messages on health issues. A 5-point scale, ranging from 1 (not at all) to 5 (very frequently) was used to measure each item and the index variables were constructed by averaging the score from these items (r = 0.55, M = 6.59, SD = 1.66 for face-to-face communication; Cronbach’s α = 0.67, M = 6.14, SD = 2.41 for online communication).
Attitude toward adoption
Attitude toward adoption was assessed by averaging respondents’ scores on the following four items: (1) I like using health-related smartphone app(s); (2) Using health-related smartphone app(s) is beneficial; (3) Using health-related smartphone app(s) is valuable; and (4) Using health-related smartphone app(s) is wise. The four items were measured on a 5-point response scale ranging 1 (strongly disagree) to 5 (strongly agree) (Cronbach’s α = 0.89, M = 14.51, SD = 2.94).
Peer norms
Peer norms were measured measured with four statements: (1) I use health-related smartphone apps to show it off, (2) I use health-related smartphone apps to be deemed those who follow recent trends, (3) I use health-related smartphone apps for the purpose of socializing with others, and (4) I use health-related smartphone apps to be an opinion leader, anchored by a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree) (Cronbach’s α = 0.89, M = 7.12, SD = 2.77).
Self-efficacy
Self-efficacy, which concerns the extent to which respondents perceived themselves as being able to use app technology was measured with: (1) I consider myself very skilled in using smartphone applications and (2) I am less skilled than people I know in using smartphone applications (reverse coding). The two items were measured on a 5-point response scale ranging 1 (strongly disagree) to 5 (strongly agree) (r = 0.39, M = 7.31, SD = 1.67).
Usefulness
Usefulness was measured using four items: (1) Using health-related smartphone apps would enable me to easily accomplish my personal health goals (e.g. weight loss, exercise regularly, healthy eating) and (2) Using health-related smartphone apps would help me to track my health performance/activities, all scored 1 (strongly disagree) to 5 (strongly agree) (r = 0.63, M = 7.14, SD = 1.77).
Control variables
To isolate the effects of certain factors impacting on the results of this study, this study employed controls such as demographics (e.g. age and gender). In addition, the study controlled the effects of general media use (e.g. the spending time on TV, print media, and the Internet) and the total numbers of apps installed on one’s smartphone. Table 1 involves descriptive statistics of these control variables and measures.
Result
First, the assumptions for multiple regression analysis (normality of residuals, independence of residuals, linearity, homoscedasticity of residuals, and non-multicollinearity) were checked by visual inspection of such plots as the normal P–P plot of regression standardized residuals, the residual scatterplot plot of standardized residuals by the regression standardized predicted value, partial regression plots of each independent with the dependent variable, and the values of tolerance and variance inflation factor which are two collinearity diagnostic factors and were met.
To test H1–H9, hierarchical regression was used to examine relationships to the intensity of health app use. The first two blocks included demographic and media use factors, which accounted for 14.7% of the variance (R 2 = 0.139, F = 19.75, p < 0.001 for demographics; R 2 = 0.008, F = 1.18, p = 0.32 for general media factors). Although the hypotheses regarding media exposure to health information were proposed first, followed by the hypotheses on interpersonal communication on health issues and psychological factors, psychological variables were added into the analysis earlier than interpersonal communication and health media exposure factors because psychological factors such as attitude (r = 0.70) and usefulness (r = 0.66) showed the strongest positive correlation with the dependent variable, followed by interpersonal communication on health issues and media exposure to health information (see Table 3). The psychological variables raised the R 2 for the outcome variable to 0.417 (F = 86.20, p < 0.001). Next, the two interpersonal communication factors on health issues were included with the rise of the R 2 to 0.014 (F = 6.01, p < 0.01), followed by the three health media factors with the R 2 values to 0.022 (F = 6.68, p < 0.001).
Correlation coefficients (N = 372).
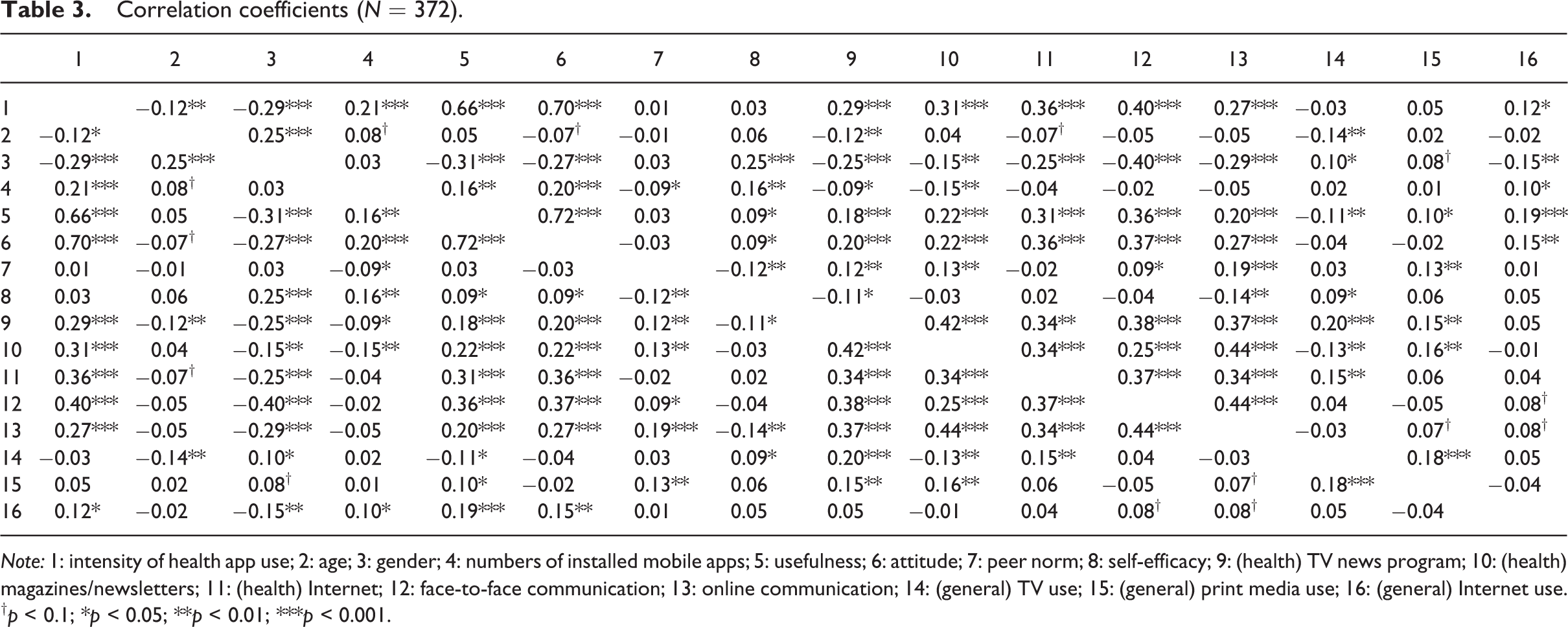
Note: 1: intensity of health app use; 2: age; 3: gender; 4: numbers of installed mobile apps; 5: usefulness; 6: attitude; 7: peer norm; 8: self-efficacy; 9: (health) TV news program; 10: (health) magazines/newsletters; 11: (health) Internet; 12: face-to-face communication; 13: online communication; 14: (general) TV use; 15: (general) print media use; 16: (general) Internet use.
† p < 0.1; *p < 0.05; **p < 0.01; ***p < 0.001.
With respect to hypothesis tests, the H1 regarding TV news (marginally) and H2 regarding the effect of print media use for health information were supported by the data (β = 0.07, p < 0.1 for TV news; β = 0.13, p < 0.01 for print media). In addition, this study found the positive effect of face-to-face interpersonal communication on the outcome (β = 0.11, p < 0.05). Therefore, H1, H2, and H4 were supported. However, this study didn’t find the effects of Internet use and online communication on the outcome. Therefore, the H3 and H5 were not supported in this study. As for the psychological variables, the perception variables, attitude (β = 0.42, p < 0.001) and usefulness (β = 0.35, p < 0.001) were supported by the data. That is, higher levels of each factor, attitude toward the health app use and usefulness, may generally enhance the levels of health app use. Thus, H6 and H8 were supported. Unlike our expectation, no significant impact of peer norm and self-efficacy were found. Thus, H7 and H9 were not supported. Table 4 provides additional information about the hypotheses results.
Ordinary least squares (OLS) regression predicting the intensity of health apps use (N = 372).
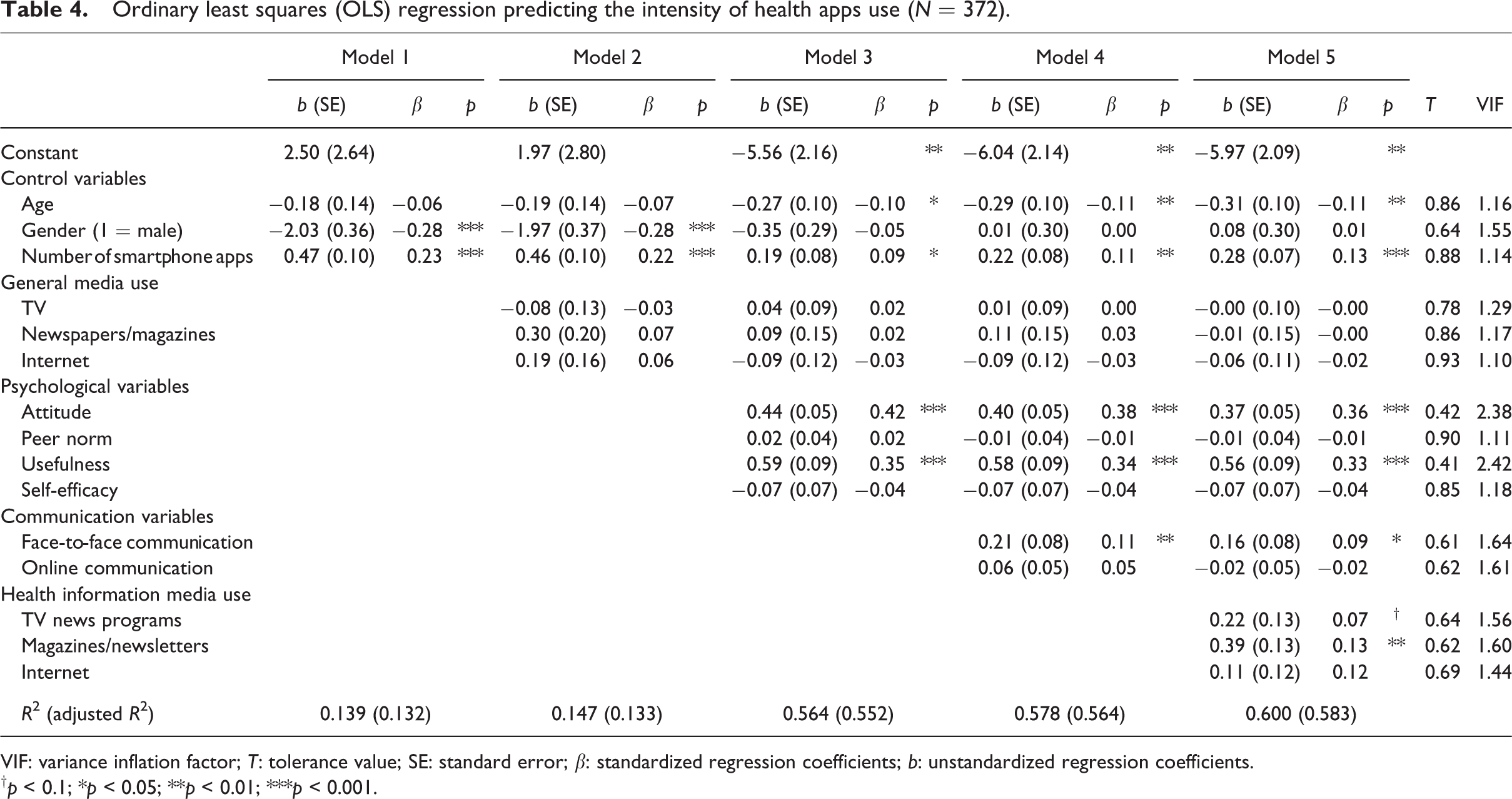
VIF: variance inflation factor; T: tolerance value; SE: standard error; β: standardized regression coefficients; b: unstandardized regression coefficients.
† p < 0.1; *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
Considering the lack of research investigating motivational factors of health app adoption and use, the main goal of this study was to identify which factors motivate individuals’ health app adoption behavior. In particular, this study aimed to understand the role of communication such as media (e.g. TV, print media—magazine and newsletter on health information, and the Internet) and interpersonal communication (e.g. face-to-face and online), and personal psychological factors (e.g. attitude and usefulness) on the adoption and use of health apps for the development of public health.
First, consistent with prior research, the results of this study indicate that health information exposure via media (e.g. TV news and print media) exerts positive effects on health app adoption and use. That is, this study confirmed that the media approach for behavior modification, health app use in this study, remains valid and useful, as in the past (Owen et al., 2002). With respect to the findings, the present study may indicate that media exposure toward health information may be served as a health information source and as a health educator. Media exposure toward health information may enhance recognition of the importance of health and let the audiences know some ways to improve their health conditions, such as the adoption of health-related apps and the use of them. Even more noteworthy is the role of print media in the development of public health. The findings of this study revealed that the standardized β value of print media such as magazine and newsletters was approximately two times greater than that of TV media on the intensity of health app use, although both of them were found to be important predictors. While print media has been displaced by digital media in recent years, the results of this study indicate that print media is still influential in encouraging an awareness of health and in promoting health behavior as measured by health app use. Therefore, although media use tendency has been toward digital media such as TV and the Internet among younger generations, health practitioners and educators need to maintain print media strategies and take print media into account as a key media platform for public health (Kwon et al., 2013). In addition, the coefficients regarding traditional media such as TV and print media may imply that health communication strategies for broadcast and print media targeted at young generations may still have a more effective advantage over new media such as the Internet.
Although the development of mHealth and smart health care environments will gradually reduce information gap between traditional media and digital media by providing new interactive technologies (Holzinger et al., 2015; Weiner, 2012), mHealth is at the beginning stage of mobile era compared with traditional media. A recent national study found that people regard information from different online sources conflicting or contradictory to unreliable (Wartella et al., 2015). Thus, it would be important to provide accurate and appropriate health information online so that consumers can get quality health information on the Internet.
With respect to the role of interpersonal communication, previous work in this area has often characterized communication activities as goal oriented (Lewis et al., 2002), especially for (1) managing self-concept, (2) behaving effectively, and (3) building and maintaining relationships (Cialdini and Trost, 1998). While interpersonal communication seems to influence each communication actors to achieve one or any combination of these goals, this study focused mainly on the second of these goals, that is, how interpersonal communication affects one’s health behavior. Consistent with previous research on the theme, this study found a significant, positive effect of health-related face-to-face interpersonal communication on the health app use. Recently, it was found that the leading source of health advice for young generation still come from face-to-face communication such as their parents, followed by health subjects in school, and medical professionals (Wartella et al., 2015). However, there was no effect of online communication on health app use. The finding may be have occurred because this study focused on various platforms (e.g. e-mails, text messages, and posting/reading online comments) for online communication rather than communication actors such as family members and friends. Therefore, future research should consider communication partners as well as communication platform preference to find the significant effects of online communication.
Next, consistent with prior research, this study shows that attitudes toward the health apps adoption and usefulness are the two crucial determinants of health app usage. First, supporting the findings of previous research regarding the positive function of attitude, this study found that those who have a more positive attitude toward health app use are more likely to use health apps than individuals with a less positive attitude. In addition, this attitude has the strongest coefficient, meaning that it could be one of the most dominant factors, encouraging the adoption of communication technologies for the improvement of public health. In addition, this study found a positive role of perceived usefulness. This study shows that individuals are more likely to use communication technologies when they perceive the use of technologies to be effectively and economically useful to accomplish certain tasks or purposes compared with other options (or services) such as face-to-face counseling services for weight loss or personal one-on-one fitness training. In addition, it is true that there is still a large population of people who do not trust the benefits of mHealth for various reasons such as the lack of apps for certain specific medical uses; improvements needed for some existing medical apps, security, and privacy protection; and the inability of health-care organizations to consistently implement mHealth-related policy. However, the benefits of moving to mHealth will be obvious in that it will save patients’ time in accessing health information and records, reduce medication errors, and help them learn about new treatment path (Weiner, 2012). Therefore, individuals would find the benefits and usefulness of health apps and then generate positive attitude toward the health apps eventually.
Self-efficacy did not predict health app usage. Although self-efficacy is often associated with technology adoption, in this study, self-efficacy may not be such a concern for the participants who are relatively young and are familiar with technology use or have a stronger confidence in their ability to adopt new technologies quickly (Chung et al., 2010). However, the finding does not mean that self-efficacy is not important in research. Future research should continue to consider this factor as a crucial determinant of behavior decision in a communication technology context for a certain audience such as older generations (Deng et al., 2014; Nischelwitzer et al., 2007; Xue et al., 2012). Finally, although this study expected the positive effect of subjective norms (peer norms) on the outcome, it was not found. One possible explanation could be that health behavior is relatively private in nature. The use of the technology may not subject the user to public scrutiny. For example, when using a weight-loss app, it is unlikely that a college student will share their use with a friend. In other words, health is more oriented to personal factors rather than social factors. Thus, it could be that subjective norms do not significantly impact the intensity of health app use.
In summary, the findings of this research provide useful guidance for developing effective mHealth systems. Policies regarding mHealth systems may have a profound impact on people, patients, clinicians, and managers at health-care organizations. First of all, health-care managers and marketers should be aware that during health-related promotion or prevention campaign, traditional media as source of health information should be included as one of the major elements of integrated marketing communication to effectively penetrate target audiences. In doing so, people will be interested in health information and they will be more likely to adopt health apps. In addition, the Internet can potentially play a complimentary role in encouraging individuals, particularly for younger generations, to adopt health apps as in the future consumer health experience will be mostly supported by digital devices (Weiner, 2012).
Secondly, as evidenced by the findings, face-to-face communication with family members and friends is critical in obtaining health-related advice as they may be perceived to be trustworthy and credible compared with unknown online sources. Perhaps close relationship with communication actors as source of health information could be more important than the media platform itself. In order to utilize online communication more effectively, it would be desirable to provide accurate and valid health information readily available and accessible to younger generations so that they will more likely to use health apps.
Finally, it would be important to internally motivate individuals by informing them of the usefulness and various benefits of using health apps, which will generate positive attitudes toward using health apps. Marketers should let people know that digital devices will enable people to manage their health care and wellness-enhancing process by expediting synchronous and asynchronous interactions with physicians. Once people generate positive attitudes toward health apps, they will more actively use health apps to achieve their health-related goals.
Limitations
This study has a number of limitations to be considered. First, the present study was conducted with college students in one university. While this study tried to maintain representativeness of the sample in the given university, the results should be generalized with caution. Therefore, future studies should analyze a more representative sample to validate the relationships between the independent variables and the outcome, which would also likely yield greater variance in willingness to use health apps.