
Abstract
Introduction
This study compared the differences in recorded speech variables between people treated with conventional ‘in person’ Lee Silverman Voice Treatment (LSVT) and those treated remotely via iPad-based ‘Facetime’.
Method
Eight participants were selected for the iPad LSVT, and 21 similarly matched subjects were selected from existing data to form the ‘in person’ group. Participants in both groups had diagnosed idiopathic Parkinson’s disease and moderate hypokinetic dysarthria. Eighteen sessions of prescribed LSVT comprising a pre-treatment assessment, 16 treatment sessions, and a six months’ post-treatment assessment were administered for each person. In both groups, pre- and post-treatment assessments were conducted face-to-face. Performance measures were recorded during assessment and treatment. Average measures were determined for all tasks at all time points and a summary outcome variable was composed from across-task performance.
Results
Non-inferiority testing confirmed that iPad LSVT was non-inferior in treating all LSVT task 3 variables except generating words, with the 90% upper confidence intervals (CI) lying between the non-inferiority margin of ± 2.25 and zero. The iPad was superior in treating the task 3 rainbow reading passage and describing motor task variables with upper and lower 90% CI values being negative. The improvement in the summary outcome variable score was also superior in the iPad group.
Discussion
Non-inferiority testing implies that the iPad LSVT is non-inferior in treating task three variables when compared to traditional LSVT. The study supports further development of remote delivery solutions involving the Apple iPad and ‘Facetime’ system as a means of improving access to services and the participant’s experience.
Introduction
Significant communication impairments are a common feature of Parkinson’s disease (PD). In 75% of people diagnosed with PD, hypokinetic dysarthria occurs at some stage of disease progression. Hypokinetic dysarthria is typically characterised by reduced speech volume, monotone pitch and amplitude, imprecise articulation, and changes in vocal quality.1–4 These changes often have adverse effects on people’s quality of life, resulting in social withdrawal, an altered familial role, reduced ability to conduct working practices, and poor psychological well-being.1,2 The Lee Silverman Voice Treatment (LSVT) has been shown to be effective in improving speech in people with PD, with patients maintaining positive effects for up to two years post-treatment.1,4 The approach focuses upon vocal loudness as the single parameter of treatment and uses clinician feedback to achieve the recalibration of perceptual and motor functioning in respect to vocal loudness. The treatment relies on intensive practice and requires a four-week period of attendance, within which subjects undertake therapy for one hour four times a week.1–5
The level one evidence for LSVT often persuades speech and language therapy services to fund the certification of clinicians so that the treatment can be offered in preference to other approaches that lack comparable evidence. However, despite the evidence for the effectiveness of the LSVT, the intensive nature of therapy can be a concern for clinicians and participants alike, particularly within the context of increasingly stretched statutory health services. Clearly, the level of clinic attendance required for LSVT can be demanding for the recipient, with associated monetary and time costs, but the physical symptoms of PD and related mobility challenges can sometimes render inclusion impossible.2–7 In a rural area, access to the therapy can be limited to the mobile patient who has the time and the means to travel to a clinic. Hospital transport services are often available to support inclusion, but the financial costs to health service providers and the time costs to treatment recipients are often substantial,2–7 and occasionally prohibitive.
Using technology to enable the patient to access the therapy from home has clear advantages for all groups, and several researchers have sought to deliver LSVT using a secure broadband connection and webcam or telehealth system. Constantinescu et al.2,3 and Howell et al. 8 have reported that the delivery of LSVT online is reliable and feasible, and specific technologies are now being developed to support therapy delivery. For example, Halpern et al. 7 developed the LSVT companion, which uses a microphone that interfaces with computer software to support the LSVT programme, allowing the clinician to provide direct feedback. However, research into the effectiveness of online LSVT is in its infancy, with many studies failing to compare online LSVT to ‘in person’ therapy and failing to incorporate all elements of the treatment. 4 In those studies which have compared online LSVT to ‘in person’ treatment, the changes seen to date appear comparable. With the increasing availability of Wi-Fi internet, hand held devices such as the Apple iPad, and software that allows real-time video conferencing, the feasibility of LSVT online can be explored further. Using an ‘off the shelf’ platform for treatment is appealing from a cost perspective, and the potential for iPads or similar tablets to be accessed via 3G or 4G data-roaming functionality offers the possibility of providing services to people with mobility or geographical access issues and no computer experience or home internet connection.
The present study examines the outcomes of subjects treated with LSVT via an iPad-to-iPad connection (using Facetime), and compares the results with the outcomes recorded for subjects treated ‘in person’ as prescribed.
Methods
Participants
Twenty-nine participants took part in the study. All participants were diagnosed with idiopathic PD with moderate hypokinetic dysarthria. Eight participants were selected for the iPad LSVT, with a mean age of 67 years (SD 6.05). This group received their treatment in 2013, with some follow up reviews occurring in the early part of 2014. Twenty-one similarly matched (for age, moderate hypokinetic dysarthria, and exclusion of additional morbidity) subjects formed the ‘in person’ treatment group, with a mean age of 69 years (SD 7.98). This group was derived from existing data that was held from LSVT conducted within a clinic setting between 2009 and 2013. All time points associated with the delivery of LSVT were observed consistently across all subjects, with pre-assessment occurring one week ahead of the commencement of treatment, four sessions a week for four weeks at an agreed time of day, and post-assessment occurring in the sixth month following treatment. There were no drop-outs and no significant disruptions to attendance during the prescribed delivery of treatment. Of the eight subjects treated via iPad, two would have been required to make at least eight 30 mile round trips to attend clinic-based therapy of the same kind (as well as eight shorter trips to a clinic nearer their homes).
Experimental procedure
In both groups LSVT comprised a total of 18 sessions, including a pre-therapy assessment, treatment sessions with a ratio of one to 16, and a post-treatment review approximately six months after treatment. In both the iPad and traditional treatment groups, pre- and post-assessment was completed face-to-face. Sessions one to 16 in the traditional treatment group were also conducted face-to-face; however, in the iPad group, therapy was conducted interactively through an Apple iPad device. The patient stayed at home whilst they communicated with the delivering clinician through ‘Facetime’ software on each of two Apple iPads.
Lee Silverman Voice Treatment patient measures.

Hierarchical speech loudness training total (HSLTT) (dB) = The average of all average RRP, C, DMT, and GW recordings for a participant in each session. dB: decibel; Hz: Hertz: SPL; sound pressure level.
Task two data measures (relating to pitch) have been excluded from the study owing to difficulties achieving accurate readings of frequency via the iPad speakers (iPad group only). Disruption to some early iPad sessions relating to technical issues resulted in the delayed commencement of treatment for four subjects, but the issues are not considered to have had any detrimental effect upon defined time points. Home visits to subjects in the iPad group were restricted to pre- and post-assessment sessions (incorporating iPad delivery, setup, and collection), but four additional home visits were required for the subjects who experienced initial technical difficulties.
Equipment
In the iPad group, Apple iPads were used with Apple ‘Facetime’ videoconferencing software to achieve a synchronous ‘face-to-face’ connection with patients. The ‘Provide’ information governance department appreciated Facetime’s encryption and Health Insurance Portability and Accountability Act Compliance with WPA2 Enterprise security settings, and approval was gained prior to the purchase of equipment. All participants in the iPad group were issued with loan devices (excepting one participant who was eager to use his own), from the ‘Provide’ Adult Speech and Language Therapy department. All participating subjects had personal Wi-Fi connections within their homes and were competent IT users. All home wireless connections were tested and approved before commencement of treatment.
In both treatment groups, RadioShack digital sound level metres were used to measure vocal loudness. These devices were provided to iPad therapy subjects with training so that they could be consistently positioned 30cms from the subject’s mouth and that all settings remained the same across sessions. The digital display of the sound level metre was positioned by iPad therapy subjects so that it was clearly visible to the treating clinician without impeding face-to-face view. All measures were recorded without difficulty. A Korg OT-120 orchestral tuner was used to record measures of vocal frequency in treatment tasks geared towards the development of increased pitch range and variation (task two). This piece of equipment was held with the clinician in both treatment groups.
Statistical analysis
The primary analysis of this study was concerned with establishing non-inferiority of the iPad LSVT. As published in previous non-inferiority trials using LSVT, a minimum improvement of 4.5db on the sound pressure level within the conversation monologue task is considered clinically relevant, with the non-inferiority margin being set at half of this value (2.25db). 5 The change from baseline to post session 16 scores calculated for both the iPad and ‘in person’ group, and independent t-tests conducted to compare these values for each of the sound pressure variables measured (sustained vowel phonation (SVP), rainbow reading passage (RRP), conversation monologue (CM), describing motor tasks (DMT), generating words (GW), and hierarchical speech loudness training total (HSLTT – calculated as an average of all outputs but sustained vowel phonation)). It was then determined whether the 90% confidence intervals of these differences lay between the non-inferiority margin (±2.25db) and zero.
A two-way mixed subjects ANOVA with Bonferroni corrected post-hoc t-test was then performed to compare patients’ outputs for SVP, RRP, CM, DMT, and GW between the traditional ‘in person’ LSVT and the iPad LSVT conditions, as well as between the three time intervals (pre-therapy assessment, session 16, and six months post-treatment). A two-way mixed ANOVA was also conducted on the HSLTT. The Statistical Package for the Social Sciences for Windows v19 (SPSS Inc., Chicago, IL) was used for statistical analysis.
Results
The 90% confidence intervals for the difference in the mean change in SVP between the ‘in person’ and iPad LSVT did not lie between the non-inferiority margin, with the upper 90% CI of the differences between groups being 8.09. This was also the case for the task 3 GW measure, where the upper 90% CI was 3.41. Non-inferiority of the iPad treatment in treating these variables cannot therefore be confirmed. However, the 90% CI for the difference in the mean change between the ‘in person’ and iPad LSVT in task 3 variables of RRP, C, and DMT did lie between the non-inferiority margin, confirming non-inferiority of iPad LSVT in improving these variables. Furthermore, the upper and lower 90% CI of the differences between groups for RRP, DMT, and HSLTT were all negative values, indicating superiority of the iPad group for treating these variables.
The 90% CI for the difference in the mean change between the ‘in person’ and iPad LSVT in the HSLTT variable score was also between the non-inferiority margin, confirming non-inferiority of iPad LSVT in improving the summary score. The upper and lower 90% CI of the differences between groups for the HSLTT variable score were both negative, indicating superiority of the iPad group for treating these variables.
Sound volume and duration measures. Mean ± Standard deviation (95% CI).
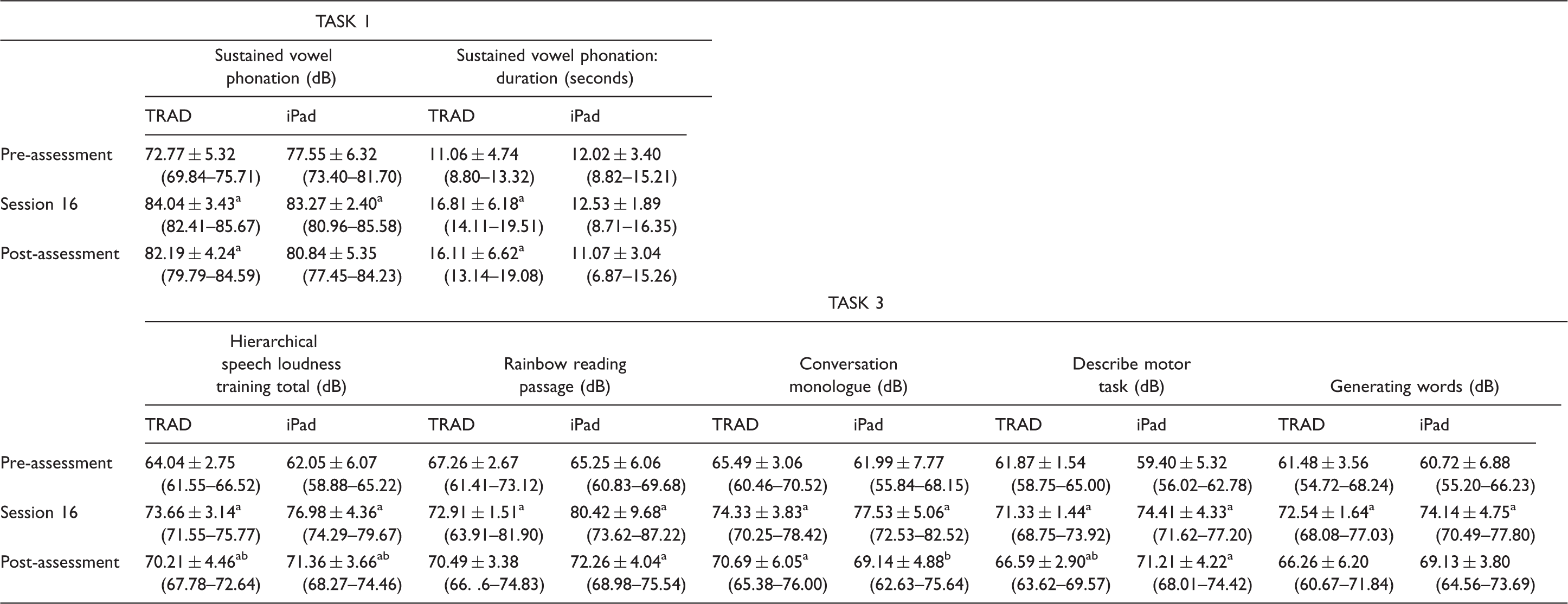
p ≤ .017
significantly different from pre-assessment; p ≤ .017.
significantly different from session 16.
TRAD: Traditional means of conveying the therapy (i.e. face-to-face); dB: decibel.
A Bonferroni post-hoc test was conducted to determine between which time intervals the significant differences were present. In both the traditional LSVT and iPad LSVT there were significant differences in SVP, SVP: duration, RRP, C, DMT, and GW between pre-assessment and session 16 (p < 0.017), with the exception of iPad SVP: duration.
There were also significant differences between pre- and post-assessment in the same variables (p < 0.017) within both groups, with the exception of iPad LSVT SVP, C, and GW, and traditional LSVT RRP and GW (p > 0.017).
Differences between session 16 and post-treatment are similar between the iPad and traditional LSVT. IPad C shows a significant decrease (p < 0.017) from session 16 to post-assessment, whilst traditional LSVT DMT also presents the same significant decrease (p < 0.017) from session 16 to post-assessment.
The summary HSLTT variable score (f = 115.29) also showed significant differences over the three time intervals (p < 0.05). Bonferroni post-hoc tests revealed that there were significant differences between pre-assessment and session 16 HSLTT scores (p < 0.017) and pre- and post-assessment scores (p < 0.017). HSLTT also showed a significant decrease (p < 0.017) from session 16 to post-assessment in both treatment groups.
Average % change between each of the recorded time frames.

p < .017.
indicates statistical significance. dB: decibel.
Between pre- and post-assessment time intervals, traditional LSVT induces the greatest changes in task 1 variables, whilst the iPad LSVT led to the greatest changes in task 3 variables and the HSLTT summary score. Scores for all outcomes and the summary outcome decreased between session 16 and post-assessment; however, reductions in the iPad group were greater than in the traditional group except for GW and CMT.
Discussion
The aim of this study was to compare the outcomes of LSVT for patients engaged in traditional treatment and treatment using an iPad-to-iPad connection. The study identified that the iPad treatment was non-inferior in treating all task 3 variables except GW and was superior in treating RRP, DMT, and in the HSLTT. The study also identified that there were no differences between traditionally conducted LSVT and interactive Apple iPad LSVT, in any of the variables across the three time periods. However, it was clear that both modalities produced significant improvements from baseline (i.e. pre-therapy assessment) to the last session (session 16) for SVP, HSLTT, RP, C, DMT, and GW. Similarly, pre- and post-treatment measures were significantly improved in the same variables (SVP, HSLTT, RP, C, DMT, and GW) within both groups with the exception of iPad SVP, C, and GW, and traditional RP and GW. These results are in agreement with Constantinescu et al.2,3,5 and Howell et al., 8 who identified that LSVT online is a reliable and feasible treatment option for Parkinson’s disease patients suffering from hypokinetic dysarthria. As well as the efficiencies in transport cost, time, and impact, all sessions were able to commence promptly at the agreed scheduled time and reliability compared favourably with clinic-based provision where transportation delays were frequently liable to disrupt clinic timings.
Despite the consistency between the two treatment modes in improving outcome variables from pre-treatment to session 16 and pre-treatment to post-treatment, examination of task 1 and task 3 variables separately reveals some differences between the treatment groups. Improvements in task 1 variables favour the traditional treatment mode, with non-inferiority not being established for SVP, whilst improvements in task 3 variables favour the iPad treatment group, with superiority being established for RRP, DMT, and HSLTT. Furthermore, in all task variables except DMT and GW, the iPad LSVT was less proficient in maintaining change after the LSVT therapy ceased. Scores reduced in all outcome measures in both groups; however, these reductions were generally larger in the iPad group.
One potential explanation for this discrepancy in the rate of decay between groups could be that the clinician-supported loud conversation outside of the clinical environment (ideally within a noisy setting unrelated to the therapy), which typically commences in treatment session 11 and which becomes a part of the session until the end of the therapy period, is difficult to apply remotely and consequently not undertaken. Fears for the safety of the subject and the equipment as well as concerns regarding the range of the Wi-Fi connection precluded therapeutic conversation outside of remote therapy participants’ homes. Solutions such as the introduction of background noise into clinical sessions at session 11 might be worth considering, but whether such alternatives could establish comparable generalisation and longer-term maintenance effects would require examination.
All candidates within the iPad therapy group expressed high levels of satisfaction with the intervention, and appreciated the cost and convenience benefits (these opinions were offered anecdotally and were not collected via formal questioning). Of the eight subjects treated via this methodology, two would have been required to make at least eight 30-mile round trips to attend clinic-based therapy, one would have been required to undertake a 15-mile round trip for all 16 sessions, and four subjects would have been required to have made eight 20-mile round trips and eight 25-mile round trips to attend. One subject would have also needed to have undertaken eight 40-mile round trips and eight 70-mile round trips to participate. Furthermore, this candidate would have relied upon hospital transport for access and the costs to him and the health service would have been considerable.
In opposition to these facts, the introduction and early deployment of the iPad system was not without technological mishap and several early sessions were aborted, disrupted, or delayed by connection difficulties and problems with device settings. Clinician attendance at subjects’ homes was required on four separate occasions across the study to troubleshoot operating issues, and there was disruption to session scheduling on occasions. Whilst the need for troubleshooting and physical support reduced as both clinicians and subjects developed familiarity with the equipment, the cost implications of equipment delivery, demonstration, and collection do need to be addressed to maximise efficiency. Therapy assistants can be employed in this role, but established telehealth services could be considered to assist with the distribution and technical support of equipment.
In conclusion, non-inferiority testing implies that the iPad LSVT was non-inferior in treating all task 3 variables except GW and was superior in treating RRP and DMT, and in the HSLTT. In addition, iPad LSVT matches traditional LSVT in elevating pre-therapy assessment measures to session 16 measures. However, the rate of decay shown in post-treatment recordings (> six months after therapy) appears greater in iPad LSVT than traditional LSVT. This study suggests that administering LSVT by the use of an iPad and internet connection is a viable alternative to face-to-face therapy, and there is scope for other therapies (specifically those that use modelling and cues to establish change) to use this form of delivery. The potential to achieve better equity of access to intensive treatments such as LSVT is supported, but there are operational considerations with the use of remote technology that require still more efficient solutions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by ‘Provide’ C.I.C. – a healthcare organisation delivering services to the NHS and local authorities in the UK. ‘Provide’ Adult Speech and Language Therapy Service offer LSVT via certified clinicians and have no organisational association with ‘LSVT Global, Inc.’ 3323 N. Campbell Ave, Suite 5, Tucson, AZ 85719.