
Abstract
Introduction
Regional cancer patients face various barriers in accessing specialist cancer services. Teletrials are a new model of care that utilise communications technologies to enable access to and participation in clinical trials close to home. The present study aimed to explore the experiences of regional cancer patients and their carers while participating in a teletrial, and those of regional patients who travelled to a metropolitan centre for trial participation.
Methods
A concurrent, mixed methods study design was used to address the study aim. Patient quality of life data were gathered for both groups and an audio-recorded semi-structured interview undertaken to explore patients’ and carers’ experiences of the two modes of trial participation. Greater weighting was given to the qualitative data.
Results
Participants described teletrials as an acceptable and valuable initiative that reduced overall burden of trial participation. Irrespective of mode of delivery, patients and carers identified access to trials and specialist cancer services as an important equity issue for regional cancer patients.
Discussion
From the perspective of regional cancer patients and carers, a teletrial offers convenient, acceptable access to a clinical trial. Although not all patients may want to engage in a teletrial, patients and carers agree that it offers equity of opportunity for trial participation, irrespective of where people live.
Keywords
Introduction
Australians living with cancer in rural or remote communities experience >10% reduction in survival compared to their metro counterparts. 1 The disparity in health outcomes is related to various factors, including geographic constraints, lack of investment in infrastructure and limited availability of and access to specialist cancer services such as clinical trials, with <5% of regional and rural patients participating in clinical trials.2–6 Despite recommendations to increase access to clinical trials, patients in regional and rural areas continue to face challenges to participation. 7
Telehealth is an increasingly adopted approach to deliver clinical trials, associated with reduced patient burden and increased trial accrual rates. 8 Telehealth has been shown to reduce requirements for trial-related hospital visits, enable effective management of symptoms and adverse effects, as well as positively impact quality of life. 9 , 10 Building on the National Telehealth Framework, a teletrial model utilising digital tools for trial conduct and delivery, telehealth has gained considerable traction as an effective and efficient model of care that provides a solution to existing barriers. 11 , 12 The Australasian Teletrial Model (ATM) consists of a trial cluster with primary and satellite sites working in collaboration to recruit, consent and manage patients at the satellite site. 13 , 14 The cluster model aims to address barriers to trial participation for rural patients and increase collaboration between metropolitan and rural cancer centres. The ATM was used to develop a teletrial framework for Victoria, Australia. 13
Although teletrials have been piloted in Australia, patients’ experiences of participation via the teletrial model, compared with the experience of traveling to a metropolitan centre to take part in a clinical trial, are not well documented. The aim of this study was to explore and describe the experiences of two groups of regional patients and their carers: those with experience of the teletrial model and those travelling who were required to participate in all trial activities at a metropolitan cancer centre.
Methods
Study design and setting
A concurrent, mixed methods study design was used. Quantitative survey data were collected alongside qualitative (semi-structured interview) data. Although a concurrent design (where data are gathered simultaneously to generate understanding from a breadth of perspectives), greater weighting (priority) was given to the qualitative data in keeping with the study aim and constructivist research paradigm. 14 Ethics approval was obtained from Peter MacCallum Human Research Ethics Committee (19/153L).
The Victorian Comprehensive Cancer Centre (VCCC) 15 situated in metropolitan Melbourne is an alliance organisation of 10 clinical, research institute and university partners that aims to connect and integrate organisations to achieve the best cancer care for all Victorians. The VCCC piloted the teletrial program with a metropolitan primary site and two regional satellite cancer centres, 13 through an investigator-initiated study preventing thromboembolism for lung and gastrointestinal cancer patients (ACTRN12618000811202). The primary site was a metropolitan tertiary cancer centre.
Participants included regional patients and their carers enrolled in a clinical trial via telehealth (teletrial group) and the comparison was regional patients travelling to the primary site to participate in a range of cancer clinical trials (regional-metro group). Eligibility criteria were: (a) over 18 years old; (b) able to read and respond in English; (c) residing in a regional location as defined by the Victorian government; 16 , 17 and (d) current clinical trial participation in a Phase II or III cancer clinical trial.
Data collection
Potential teletrial patients were identified by clinical trial nurses at the two participating regional sites and by the clinical trial coordinator for regional patients at the metropolitan centre. Eligible patients were invited to take part in the study via email or post by the research coordinator. At the end of the survey, participants were made aware that they could take part in an audio-recorded interview if they chose and that they could nominate a carer to take part as well. Nominated carers were invited by the research coordinator to take part in the interview together with the patient or individually. All invitations were made clear that participation is voluntary. Interviews were all conducted via telephone by the research officer.
Measures
A study specific online survey was developed using a combination of validated measures that included the National Comprehensive Cancer Network (NCCN) Distress Thermometer (DT), Problem List (PL) for patients and Edmonton Symptom Assessment System (ESAS). The DT is a one-item measure of self-reported distress during the past week, accompanied by a visual graphic of a thermometer. 18 Patients rate their distress on an 11-point Likert-type scale, ranging from 0 = no distress to 10 = extreme distress. This is often followed by the PL, which consists of 40 items reflecting five domains of commonly experienced problems for cancer patients. 19 The ESAS is a 10-item visual analogue scale (VAS) assessing physical and psychological symptoms. 20 Each item is rated with a VAS score ranging from 0–10. The ESAS has been widely used in cancer research. 21
The audio-recorded interviews included a series of study-specific, open-ended questions to generate data to address research questions. Interview questions covered three main domains: (a) the experience of participating in clinical trial; (b) barriers and enablers to clinical trial participation; and (c) views about access to clinical trials for regional patients.
Analysis
Quantitative survey data were analysed using descriptive statistics (range, medians, average, frequencies and percentages). Audio-recorded interview data were transcribed verbatim. NVivo 12 data analysis software was used for qualitative data management. 22 Through an iterative process, inductive, thematic descriptive analysis was undertaken to identify dominant themes. 23 The research officer initially analysed the data with continuous verification 24 , 25 and through discussion with another project member. Afterwards, 10% of the data were co-coded by a qualitative researcher not involved in the study. Minor differences in interpretation of codes were discussed between the two coders and applied to the analysis. No major discrepancies were found hence no further co-coding was done.
Results
In total, 55 regional patients were participating in teletrials at the time of recruitment and 13 patients were eligible and interested to participate in the study. A total of 65 eligible regional-metro patients were identified.
Survey
Overall, 11 teletrial patients (85% response rate) and 26 regional-metro patients (40% response rate) agreed to take part. Patient demographics and clinical characteristics are outlined in Table 1 below.
Teletrial (n = 11) and regional-metro (n = 26) patient demographics.
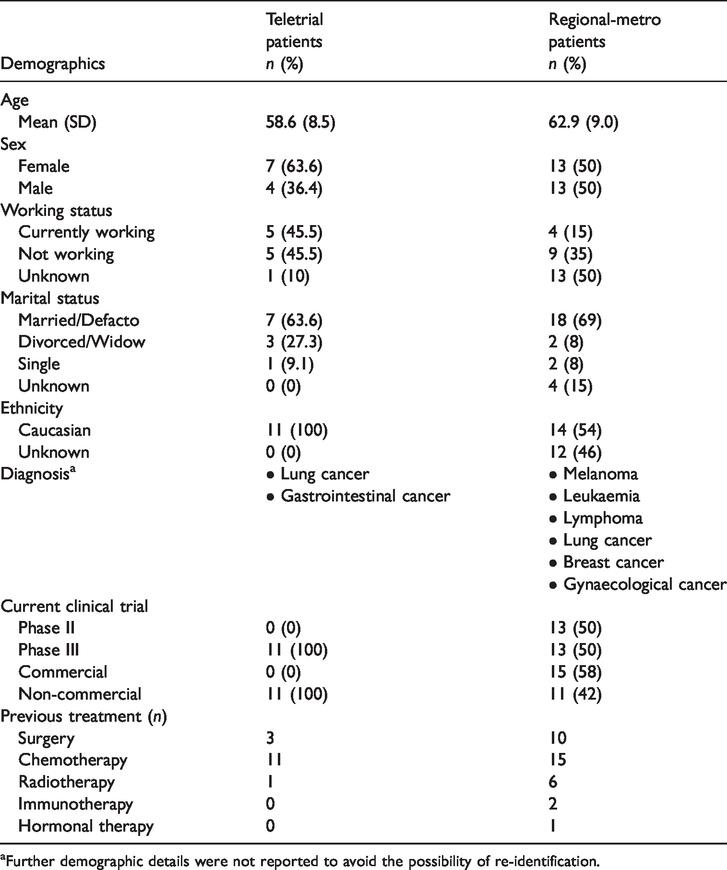
aFurther demographic details were not reported to avoid the possibility of re-identification.
Patients' responses to the NCCN DT and PL and the ESAS questionnaires are reported in Table 2. Teletrial and regional-metro patients reported a low median score of 2 out of a possible maximum score of 10 on the DT, indicating low levels of distress. Out of a maximum score of 10, teletrial patients scored higher on the ESAS domains for pain, depression, anxiety and appetite than regional-metro patients, but overall, there was no observable difference across groups for the DT and ESAS scores.
Survey descriptive statistics.
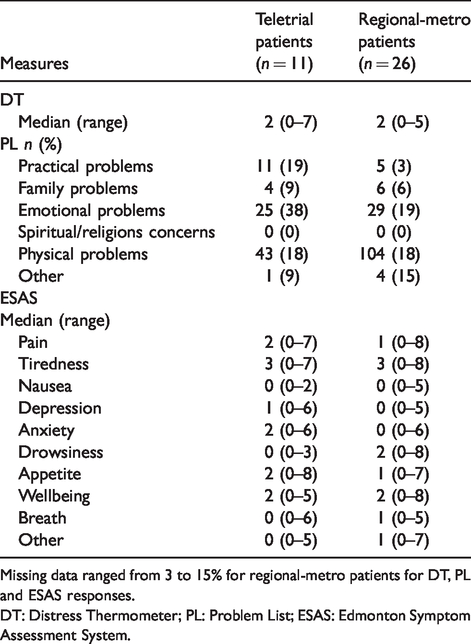
Missing data ranged from 3 to 15% for regional-metro patients for DT, PL and ESAS responses.
DT: Distress Thermometer; PL: Problem List; ESAS: Edmonton Symptom Assessment System.
Interviews
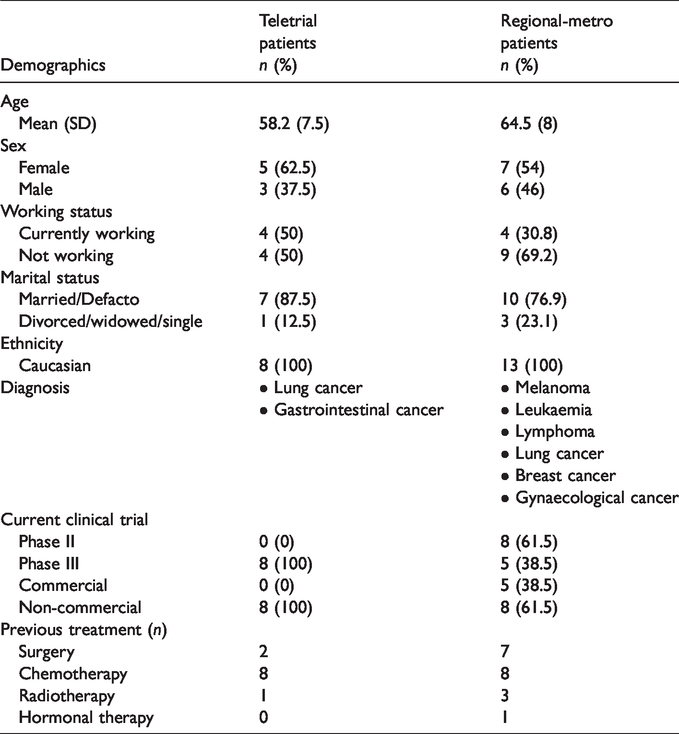
A total of 23 participants were interviewed (eight teletrial patients, two teletrial carers and 13 regional-metro patients). On average, interviews took 21 minutes (10–42 minutes) to complete. Table 3 details the demographic information of patients who were interviewed. The two teletrial carers were female family members who were full time carers of the patients, residing regionally, who had attended all teletrial appointments with the patient. Further demographic details were not reported to avoid the possibility of re-identification.
Demographics of teletrial (n = 8) and regional-metro (n = 13) patients interviewed.
Teletrial patients and carers
Teletrial patients and carers had participated in up to three teleconferences and had been part of the trial for 4–18 months. Analysis of their interviews revealed four broad themes with a range of subthemes as outlined below in Table 4.
Teletrial group interview themes and subthemes.

Acceptability of teletrials
The teletrial model was well-accepted by patients and carers with no reports of any negative financial, social or emotional impact. Patients and carers reported that the quality of care was not compromised because of the remote delivery and the personal nature of the interaction was still present: I thought it was very well done. It was basically just like having them just sitting across the desk from you, actually it might have been a little bit easier than having them sitting there straight across from you, because it gave you a little bit of time, while they’re talking you had a little bit of time to consider your answers before you said anything. I thought it was good. (Patient 1) And you got your answers. If you had any questions they were able to get answered and you could see each other, it was still like you were in the one room anyways […] I think it was really, really good. Seeing you can watch someone talk and you can gauge on facial you know expressions and everything else well. (Carer 1) I think just the connection. I think you need good internet further […] If it was dropping out all the time it won’t be much value, I wouldn’t think. (Patient 2)
Decreased burden and increased reassurance
Patients and carers described experiencing a valued expansion to their care team and enhanced support through the visible connection between their regional clinicians and staff at the metropolitan site: Well … for a person who is going through cancer and knowing that you guys are there as well … not as back up, but you are there as well in my care. That meant so much for me […] that’s why it’s 10 out of 10, I’m very grateful. (Patient 5) Well it saves people having [sic] travelling to Melbourne, it’s a great thing, I think. Especially from up where we live you know, if you’re feeling a bit crook you don’t want to be doing that, do you really. (Patient 2) Financially as well. Having to go down to Melbourne you know there’s an expense there. Just travelling down we would more than likely have to stay the night. Very rare that we would go up and down in 1 day. And also other factors like I said we got family here so and that’s emotional and mental in a sense. But just also the comfort of being at home with everyone else here. (Carer 2)
Increased equity of care
All patients and carers highlighted the importance of having access to clinical trials. Teletrials were described as increasing accessibility and opportunity for regional patients to take part in a clinical trial: I wasn’t well enough. Not well enough now to make that journey [to Melbourne]. Which is on the train, and then trams, and back on the train, and get home, and get to the station and all that sort of business. It would be physically impossible for me to do. (Patient 4) As a patient, absolutely. I think it makes [it] a lot more accessible, because I couldn’t drive for a while […] I think the only thing that would have made me say no would have been me needing to go to Melbourne to actually take part. (Patient 7)
The value of teletrials
Teletrials were identified as a valuable addition to cancer care for regional Victorians. Being able to stay close to family and maintain consistency of care with the local hospital was repeatedly identified as important to patients and carers: I often say, it must have been so hard for the people previously who had to go to Melbourne or anywhere else to get the treatment. I’m very appreciative of the fact that it is local. (Patient 8) It was good that I could help by being on it. So that’s probably why it benefited, as I said because if I had to go to Melbourne I would have second thoughts about doing it, but because I was in my home town where I could go to the doctors or the hospitals. (Patient 6)
Regional-metro patients
All regional-metro patients were current participants in a haematology or medical oncology clinical trial at the metropolitan cancer centre and had been participating in a trial for 2–30 months. Data from the interviews with participants resulted in four broad themes with a range of sub-themes as shown in Table 5 below.
Regional-metro group interview themes and subthemes.
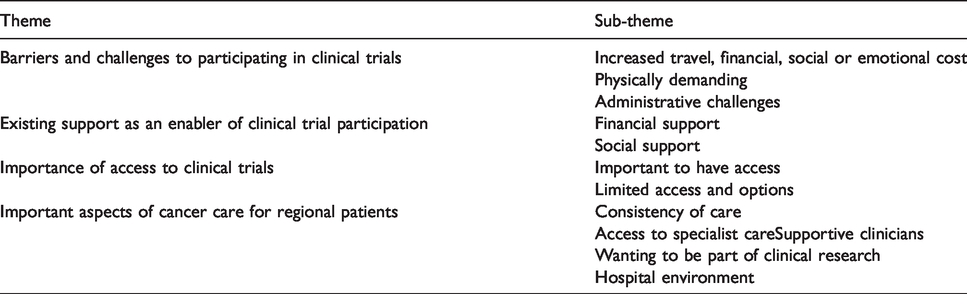
Barriers and challenges to participating in clinical trials
The burden of travelling and challenges associated with participating in clinicals trials at a metropolitan centre was evident for some regional participants. Patients talked about the stress of travelling, the financial and social cost of attending a metropolitan centre, including disruption to work and reduced time for oneself: At the moment I’m on sick leave but the trial continues to almost [a month] so it will mean me taking a couple of days sick leave every … at least every 3 weeks, which will put a bit of burden on my workload. Because I work full time normally. (Patient 12) The only thing I’ll say, even the trial team folks talk about this sometimes because they get a bit frustrated when they can’t get me in for an earlier booking […] That frustrates them, as much as it frustrates me. Because it means that instead of being there for a couple of hours, I gotta be there for the whole day, which is a long time. (Patient 13)
Existing support as an enabler of clinical trial participation
The presence of various support systems was a major factor in enabling regional patients to take part in a trial at the metropolitan centre. Several patients reported having family or friends in Melbourne, which meant they could ‘use it as a time to catch up with [family]’ (Patient 17) and it reduced accommodation costs. For some participants, financial flexibility or reimbursements and the absence of work commitments contributed to their positive experience of clinical trial participation: I can do that because I’m retired. But if I was working then that’s a whole other story […] I shouldn’t work the day before or the day after, so that would impact on employment. (Patient 16)
Importance of access to clinical trials
Similar to teletrial participants, patients attending the metropolitan centre said it was important to have access to and opportunity to be involved in a clinical trial. For many patients the opportunity to take part in a clinical trial was described as ‘life and death’ (Patient 19).
The absence of opportunity for trial participation locally and the clinical importance of the trial meant patients felt they had no other choice and were willing to accept or overlook the burdens that came along with travelling to a metropolitan centre: It would have been easier if I could have had the treatment near where I am, but being that was where the trial was, I just went with it. (Patient 9)
Important aspects of cancer care for regional patients
Regional patients valued having specialist cancer services and supportive clinicians embedded in their care: Well, just the overall caring nature, you know, there was no one who tried to hurry me or [sic] and a willingness to explain repeatedly. (Patient 20)
Discussion
To our knowledge this is the first study to explore and describe the experiences of regional and rural patients with cancer participating in a teletrial. For the study participants, the teletrial provided access to a trial that would not otherwise have been available to them. Importantly, the strategy offered an acceptable model for trial participation, overcoming challenges and reducing burden of commitment, maintaining ability to remain close to home, as well as continuity of care with their local oncology team.
All participants indicated it was important that regional and rural patients have equity of access to clinical trials, reinforcing findings from previous Australian surveys. 2 However, it was apparent from the interviews with both groups, that inequity of access to trials for regional and rural patients persist due to geographical constraints. 7 In the current standard model of care the majority of clinical trials, especially those testing complex, novel agents, are delivered in major metropolitan centres. Participants spoke of a necessity to travel to access ‘cutting-edge’ trials. But as many participants stated, this requires financial capability and a social support network that they may not have. This compounds disparity in opportunity and outcomes between regional and rural patients with cancer and their metropolitan counterparts. 5 , 6 , 26
Regional-metro participants spoke of the high-quality care they received through attending a specialist cancer centre. Importantly, teletrial patients reported they felt clinically reassured and supported through participation, because it brought together their local oncology team with leading expert trial teams based at the metropolitan centre. Participants advocated for choice in mode of trial participation, seeing teletrials as a valued additional approach to trial conduct.
An important challenge will be the ongoing support for local healthcare infrastructure and personnel. Consistent with past telemedicine literature,27–29 teletrial patients and carers talked about technological limitations that affected the overall experience of participation. Efficient and safe sharing of data on trial participants was valued by regional-metro patients and recognised as being very important to the safety of their care. The establishment of data management strategies, accountability and reporting structure as well as regulatory harmonisation remain critical to the retention of integrity and successful implementation of teletrials as a strategy for successful trial conduct.30–32
Although this is one of the first studies of its kind, the findings should be considered within the limitations of the research. Due to the localised recruitment and utilisation of convenience sampling, the results may not fully reflect the views of other regional patients, such as people who were participating in trials at regional centres. Additionally, the unique clinical context of the patients should be understood when interpreting the results. Teletrial patients were part of a Phase III trial, whereas the regional-metro patients were participating in different clinical trials, varying in risk and phase. Although sample size is a limitation of this study, this represents a proof of concept and provides early insight into the potential for transferability (scalability and sustainability) of teletrials. Patients’ acceptability of this approach, which overcomes an enormous unmet need in terms of access to trials for regional and rural patients, was evident. Furthermore, the capabilities and outcomes of teletrials extend beyond patient access to novel diagnostics and therapeutics, including potential to increase local capability and research capacity to achieve systematic best cancer care through trial opportunities and partnerships. 33
Conclusion
The teletrial model provides a strategy that enables clinical trial participation to regional and rural patients who may not otherwise have been able to access a trial. Currently, low numbers of regional and rural patients participate in cancer-related clinical trials. The importance of addressing this gap and bringing the opportunity close to home is supported by the teletrial patients and carers who took part in this study. However, investment in teletrial infrastructure is needed to maximise its efficacy and potential to benefit regional patients with cancer. Integration of patient-reported outcomes within teletrials should be considered an important mechanism for ongoing evaluation of this novel model of trial participation.
Footnotes
Acknowledgements
We would like to acknowledge Hannah Cross, Marian Lieschke, Renae Davies and Clinical Trials Australia for their considerable help and support; Monika Tenic for co-coding the interview data; and most importantly to all of the regional patients and carers who gave their time to take part in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kate Burbury, Dr Craig Underhill, Dr Samuel Harris, Jacquiline McBurnie, Narelle McPhee, Felicity Osmond, Kathleen Wilkins and Paul Baden are involved in the VCCC Teletrial Program. However, the project was primarily led by Professor Meinir Krishnasamy and Jin Joo Lee, who are affiliated with VCCC, but have had no direct involvement with the Teletrial Program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the VCCC, as part of the Victorian government initiative supporting cancer prevention, treatment and care for all Victorians.