
Abstract
Affective dimensions of cancer have long been a central concern in the field of psycho-oncology. Recent developments in the field of affective science suggest the value of incorporating insights from the burgeoning literature on affect regulation. Accordingly, the objective of this article is to build on prior work in this area by applying a process-oriented affect regulation framework to the various phases of the cancer trajectory. The Affect Regulation in Cancer framework is adapted from Gross’ process model of emotion regulation, and its aim is to integrate recent advances in affective science with work in the field of psycho-oncology. The basic elements of the affect generative and affect regulatory processes are outlined across the various phases of the cancer trajectory. Our proposed model provides a useful heuristic framework in advancing research on the ways people manage their affective responses throughout the cancer trajectory.
Being diagnosed with and treated for cancer frequently causes considerable emotional upheaval. However, research has demonstrated that over two-thirds of adults diagnosed with cancer do not experience clinical levels of anxiety and/or mood disorders (e.g. Linden et al., 2015; Mitchell et al., 2011). This finding suggests that the majority of adults are able to effectively regulate their affective reactions in response to their cancer experience.
What is not yet clear is what individuals are doing to effectively regulate their affective responses throughout the cancer trajectory. Drawing on recent work in affective science, we build on foundational work by prior researchers working within the stress and coping framework. In particular, we bring insights from the field of affective science, which has considered the specific processes individuals use to manage their affective responses, including those associated with the cancer trajectory. Our goal is to provide a heuristic framework, the Affect Regulation in Cancer (ARC) framework which includes testable predictions that can guide future research. This article comprises three sections. First, we provide a brief overview of self-regulatory models that have commonly been used in the psycho-oncology field. Second, we describe the different phases of the cancer trajectory and outline how the ARC framework explains the affect generative and affect regulatory processes at each stage of the cancer trajectory. Finally, we consider the implications this process-oriented framework has for future research in the field of psycho-oncology.
Self-regulatory models in psycho-oncology
A number of conceptual frameworks have guided research in evaluating factors contributing to emotional adjustment, health behaviors, and quality of life (QOL) in oncology patients. Building on Lazarus and Folkman’s (1984) Transactional Model of Stress and Coping, a number of cognitively oriented theories have been proposed to explain emotional adjustment to cancer, including Lepore’s (2001) Social-Cognitive Processing Model and the Cognitive-Social Health Information Processing (C-SHIP) model (Miller et al., 1996; Roussi and Miller, 2014). Perhaps, the most prominent of these is Leventhal and colleagues’ (Leventhal et al., 1980) self-regulation theory, commonly referred to as the Common-Sense Model (CSM) of self-regulation of health and illness (Leventhal et al., 1992). The CSM provides a framework for understanding adjustment to illness, including cancer. According to the CSM, when individuals are confronted with a health threat such as cancer, an illness representation is activated which has six attributes: identity, timeline, consequences, cause, control/cure, and illness coherence (Leventhal et al., 1992). These attributes interact and activate emotional illness representations that guide coping strategies following the health threat. Although considerable research over the last 50 years has evaluated various components of the model (Leventhal et al., 2016), surprisingly little research has evaluated the specific link between emotions and cognitive processes.
This gap in the field may be due to the lack of a cancer-specific framework for considering affect regulatory processes across the cancer trajectory. Although Cameron and Jago (2008) provided an initial step in this direction by accentuating the role of emotion regulatory processes following illness, their expanded model of the CSM is limited to “illness-related anxiety” per se. Notably, the emotion generative and regulatory processes across the cancer trajectory have not been considered in the extension of the coping component of Cameron and Jago’s extension of the CSM framework. The need for a more comprehensive process-oriented affect regulation framework to further our understanding of cancer is supported by the findings of a recent systematic review by Brandao et al. (2016). They evaluated the characteristics and psychometric properties of 16 scales used to measure emotion regulation and/or “emotional expression” in breast cancer patients. Importantly, the disparate findings from this review attest to the need for a conceptual framework in guiding research across the cancer trajectory. Presently, there are calls to incorporate an affective science perspective in furthering our understanding of the affective processes of adult individuals diagnosed with cancer (e.g. Ferrer et al., 2015). To that end, although there is increasing recognition of the role of emotions and/or self-regulatory processes in further new models emerging in the oncology field (e.g. Arndt et al., 2014; Conley et al., 2016), none of these proposed frameworks account for both the affect generative and affect regulatory processes across the different stages of the cancer trajectory. Accordingly, we propose the ARC framework, which builds on Gross’ (1998, 2015) process model of emotion regulation and applies it to the cancer trajectory.
Affect regulation across the cancer trajectory “journey”
“Affect” may be conceptualized as an umbrella term that covers: (1) stress responses activated by highly demanding stimuli, (2) emotions (e.g. fear, anger, sadness, and happiness), and (3) moods (e.g. feeling content, worried, and down; Gross, 2015). In line with Lazarus’ (1993) definition, stress responses refer to negative affective states when confronted with highly taxing circumstances (e.g. being diagnosed with advanced stage lung cancer). Conversely, emotions encapsulate both positive (e.g. happy and excited) and negative (e.g. angry and sad) affective states. Indeed, they are multifaceted responses that involve “loosely coupled changes” in three broad domains of subjective experience, behavior (i.e. involving tendencies to act or not, in certain ways), and peripheral physiology (Mauss et al., 2005). Emotions are also typically acute affective states (commonly unfolding over seconds to minutes) and elicited by specific events (therefore, are context specific). Conversely, moods may not always have a precipitating event; they last longer and tend to be more diffuse (e.g. dysphoria). Hence, moods tend to last for a longer time than emotions, and comparable to body temperature, a shift in mood tends to be noticed at more extreme ranges (Ellenbogen, 2005).
We will use the modal model (Gross, 1998) to describe the affect generation process. Affective responses arise when a person is confronted with a psychologically relevant situation or event (e.g. being notified of one’s cancer diagnosis). This situation is attended to and appraised in terms of the person’s current or desired goals (e.g. desire to maintain good health) and activates experiential, behavioral, and physiological response tendencies (cf. Gross, 1998). Given that an affective response (e.g. heightened anxiety) can initiate changes to the “activating situation” (e.g. avoiding medical tests), the modal model contains a feedback loop that can occur between one’s affective response tendencies and the targeted situation (Gross, 1998). The ARC framework as extended to the cancer experience is depicted in Figure 1.
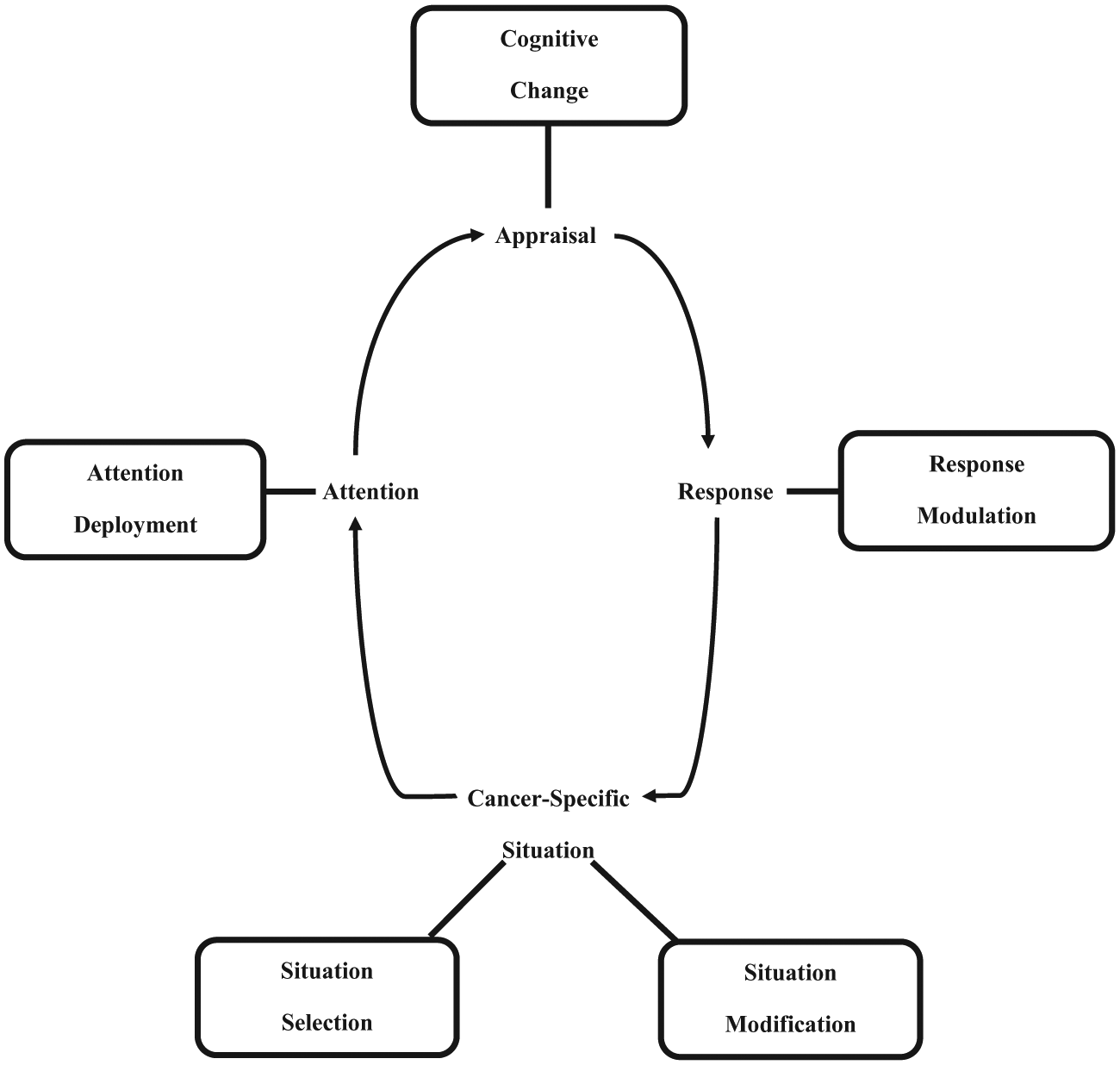
The Affect Regulation in Cancer (ARC) framework. The ARC framework depicts an affect generation and regulation cycle; regulatory processes depicted in rectangular boxes.
Relative to other types of more acute (e.g. stroke/myocardial infarction) or chronic (e.g. arthritis) medical conditions, cancer is a dynamic medical experience. Although there is no universal consensus concerning the definitive stages of the cancer trajectory, it typically consists of 5–8 stages, contingent on whether pre-diagnostic stage is included, and how recurrence and palliative phases are classified (e.g. Reyna et al., 2015; Ziegler et al., 2011). The cancer trajectory transpires over months to decades, contingent on a person’s prognosis and/or recurrence of disease. Indeed, there is growing recognition that for individuals diagnosed with cancer, they will go through a number of phases (Ziegler et al., 2011). For present purposes, we find it useful to distinguish six specific cancer stages which can vary on a continuum pertaining to the degree of certainty to uncertainty contingent on one’s current and future prognosis. These comprise (1) pre-cancer diagnostic (acute symptom) phase, (2) formal diagnostic phase, (3) treatment phase, (4) treatment recovery and survivorship phase, (5) metastatic disease or recurrence phase, and (6) end-of-life care phase. Importantly, this trajectory is nonlinear, given that a person can be diagnosed with metastatic disease from the outset. A person can also be diagnosed with advanced staged disease from the initial diagnosis, and consequently, palliative and end-of-life care may be the only feasible options available. Individuals may also reach the recovery phase and then experience a recurrence of disease. Hence, the cancer trajectory is a dynamic experience which may substantially differ across individuals diagnosed even with the same type of cancer.
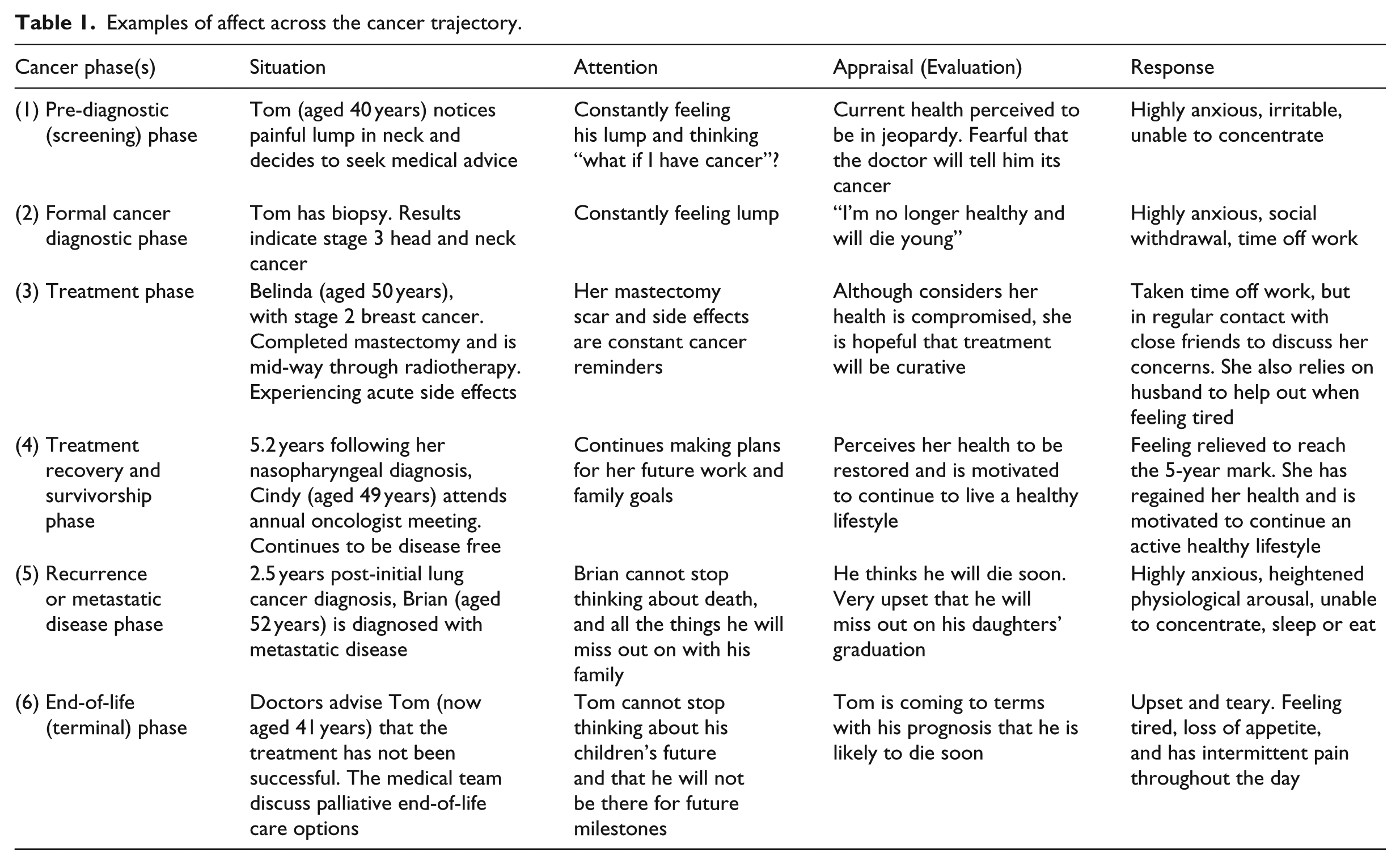
At each phase, individuals are likely to experience a range of affective responses which need to be addressed (see also Table 1). Given that individuals may also experience setbacks at any particular phase, this is also likely to lead to further affect regulatory efforts. Moreover, we acknowledge that at each phase of the cancer trajectory, individuals are faced with making important decisions (Reyna et al., 2015), which may further contribute to affect generative and regulatory processes.
Examples of affect across the cancer trajectory.
The term “affect regulation” is an umbrella term that includes coping, emotion regulation, and mood regulation (Gross, 2015). Coping refers to managing one’s reactions to a stressful circumstance and, therefore, has an emphasis on alleviating stress responses. It also tends to comprise a relatively longer temporal horizon (e.g. grieving for the loss of a loved one over a number of months; Gross, 2015) relative to emotion regulation. In contrast, emotion regulation involves regulating emotional responses to a much broader range of affective and situational experiences (Brandao et al., 2016). Specifically, emotion regulation can be defined as “the processes by which individuals influence which emotions they have, when they have them, and how they experience and express them” (Gross, 1998: 275). The defining feature is the activation of a goal to influence the emotion trajectory (Gross et al., 2011).
The foundation of our ARC framework derives from the process model of emotion regulation (Gross, 1998, 2015) and takes the modal model of affect generation as its starting point. As depicted in Figure 1, five families of affect regulatory strategies may be distinguished based on where in the affect generative process they have their primary impact. These families of affect regulatory strategies include situation selection, situation modification, attentional deployment, cognitive change, and response modulation.
For situation selection, the individual has the option to “select” whether to approach or avoid the targeted cancer-related situation which is likely to initiate an affect generative cycle. Approach behaviors typically increase the affective state, while avoidance behaviors downregulate the affective state. In the oncology context, approach behaviors may include deciding to undergo a particular treatment procedure, while avoidance would involve declining screening for cancer or avoiding medical treatment following a diagnosis. This proposition is supported by a recent study based on 252 patients with colorectal cancer, which found that greater avoidance and especially denial coping at the pre-diagnostic phase significantly delayed seeking medical assistance for their symptoms relative to patients who utilized more action-oriented coping strategies (Rogers et al., 2017).
Situation modification involves modifying the external situation in order to modulate the affective impact of the targeted cancer-specific situation. This could include asking family members to accompany the individual to medical appointments for support. For example, research has shown that actively seeking social support in breast cancer patients was a significant predictor of better QOL at 6 months following the completion of cancer treatment (Silva et al., 2012).
Attentional deployment involves directing one’s attention away from or toward the targeted situation and its cues. Distraction is one of the most common attentional deployment strategies individuals use when shifting their attention away from the targeted situation (Gross, 2015) in order to downregulate negative affect. Research has indicated that distraction is typically initiated very early on in the affect generative process (Thiruchselvam et al., 2011) and tends to be preferred in highly emotional intense situations (e.g. Sheppes et al., 2011). Thought suppression is an alternative form of attention deployment strategy which involves focusing one’s attention away from specific cognitions pertaining to the targeted situation. To that end, individuals may use several attentional deployment strategies, during each phase of the cancer trajectory, for example, by focusing on work and/or hobbies to avoid having to talk or reflect on one’s cancer experience. Moreover, in a recent study, Bauer et al. (2017) found a reciprocal relationship between intrusions and avoidance symptoms in a large sample of breast cancer patients between 2 and 5 months post-diagnosis. However, by 8 months post-diagnosis, this reciprocal association had declined which the authors attributed to the likelihood of patients having adapted following the initial acute distress period of being diagnosed with cancer; hence, they proposed that patients were more likely to use more adaptive emotional processing by 8 months post-diagnosis. These findings further attest to the fluctuating course of affect regulatory processes as patients come to terms with each phase of their cancer experience.
The fourth family of affect regulation strategies involves cognitive change. This entails modifying one’s appraisals of the targeted situation (i.e. cognitive reappraisal) in order to alter the affect generative process. This strategy has typically been found to be effective in downregulating negative affect (e.g. Mauss et al., 2007). It tends to be particularly useful when the individual needs to engage with the targeted stimulus (situation; e.g. having to undergo blood tests as part of the medical testing procedure) or when the situation is unavoidable (e.g. internal physiological arousal, including racing heart when attending medical appointments; Troy et al., 2017). This has particular relevancy for cancer patients during the initial diagnostic and treatment phases as they come to terms with having to be treated for a potentially life-threatening condition. Indeed, the use of adaptive cognitive reappraisal strategies (relative to anxious preoccupation and/or rumination) has commonly been associated with less psychological distress during the first year following cancer diagnosis and treatment across various cancer samples (e.g. Andreu et al., 2012; Hubert-Williams et al., 2012; Peh et al., 2016).
The fifth set of affect regulation strategies comprises response modulation. Response modulation occurs once the affective response is fully activated. This involves strategies utilized to directly influence the outward expressions of emotions including behavioral/postural gestures and actions, vocal tone/intonation, facial expressions, as well as the experiential and physiological components of the emotional response. One of the most well-studied forms of response modulation is suppressive expression (Cutuli, 2014). This refers to outwardly controlling one’s emotion-expressive behavior so that other people are unable to recognize one’s affective state. The majority of studies have found that expressive suppression tends to be less effective in downregulating negative emotions (e.g. anxiety) than reappraisal (Cutuli, 2014). Conversely, emotional expression may facilitate coping in stressful circumstances. For example, in a recent breast cancer study, emotion expression was predictive of less depressive symptoms on average 11 months following cancer diagnosis (Marraquin et al., 2016). Experiential avoidance is a further response modulation strategy. For persons with cancer, this may include avoiding particular people at certain phases, by declining social invitations or taking extended leave from work. Indeed, experiential avoidance strategies may be more detrimental to well-being particularly as social support has been found to have a buffering effect, with lower social support being associated with poorer QOL in cancer patients (e.g. Ringdal et al., 2007).
In the sections that follow, we briefly describe how these five families of affect regulatory processes are engaged across the cancer trajectory, complemented by the examples in Table 2 (which build on the four case exemplars depicted in Table 1). Given that there is a notable dearth of studies tracking affect regulation strategies across even several stages of the cancer trajectory, the examples in the tables must be seen as providing a heuristic framework on the basis of our ARC framework that need to be tested in prospective and longitudinal studies.
Examples of affect regulation across the cancer trajectory.

Pre-diagnostic/screening phase
The pre-diagnostic stage occurs when the person detects symptoms in which they seek medical advice and has been referred to as time-to-presentation (Balasooriya-Smeekens et al., 2015). During this period, for situation selection, individuals primarily have two options: to either ignore the symptoms or decide to seek medical advice. An individual may choose to ignore his or her symptoms as a way to downregulate anxiety. As noted, a recent study has shown that denial and avoidance was associated with delays in seeking medical advice in a sample of colorectal cancer patients (Rogers et al., 2017). Conversely, as depicted in Table 1, other people, such as Tom, may choose to seek medical advice, although this may (temporarily) enhance their anxiety as they are confronted with the real possibility of being diagnosed with cancer. The individual may also opt to modify his or her circumstances to help them cope (e.g. relying on social support). Distraction as an attentional deployment strategy may also be used to regulate anxiety and fear. Cognitive change may also be reflected in the individuals’ acceptance that it is highly probably he or she may be diagnosed with cancer. To that end, Rogers et al. (2017) found that individuals who utilized cognitive reappraisal strategies as well as planning and humor sought help for their cancer-related symptoms much earlier than patients who relied on avoidance or denial strategies during the pre-diagnostic phase.
Formal cancer diagnostic phase
Once a cancer diagnosis is confirmed, individuals are confronted with further decisions in context of treatment options (Reyna et al., 2015). Individuals can either opt to proceed with recommended treatment procedures or they may choose to refrain from being treated for cancer as a way to downregulate their fear and anxiety. Individuals who also experience heightened fear and anxiety may alternatively choose to proceed with treatment. To regulate their anxiety, these individuals may modify their situation using either approach or avoidant behavioral responses (e.g. “Tom” in Table 2). For individuals who opt to undergo medical treatment, it may be difficult to avoid all cancer-related cues which may result in some individuals ruminating about their cancer prognosis and how they appraise their health and future outlook. Other individuals may utilize thought suppression and/or distraction strategies to intentionally focus their attention away from their cancer diagnosis. Although traditionally, such strategies have been deemed maladaptive (Bonanno and Burton, 2013), distraction strategies (e.g. choosing to reflect on a pleasant recent holiday), may also help individuals (at least in the short term) to regulate their anxiety responses during this phase, particular with high-intensity responses. Similarly, individuals may also try to put on a stoic appearance using expressive suppression strategies when interacting with family and friends. To this end, individuals may use a blend of strategies for affect regulation. In fact, oscillating between focusing on one’s cancer-related thoughts (i.e. intrusions) and avoiding focusing on cancer has been documented to occur within the initial diagnostic and treatment phases as patients adapt to their circumstances, although the reciprocity between cancer-related intrusions and avoidance diminishes over time (Bauer et al., 2017). Hence, the rigid, chronic use of a particular strategy (or restricted set of strategies) is pivotal in determining whether an affect regulation strategy has a maladaptive effect.
As illustrated in Table 2, Tom relies on rumination, experiential avoidance, and expressive suppression to curtail his anxiety during the formal diagnostic phase. However, if he continues to restrict himself to these three strategies, whether used sequentially or concurrently across the cancer trajectory, this may contribute to maintaining his anxiety rather than alleviating it as these sets of affect regulatory strategies have been documented to be maladaptive in the longer term. In particular, both prolonged reliance on rumination and experiential avoidance have been found to be associated with anxiety and depressive disorders and which have tended to interfere with goal-directed behavior (e.g. Watkins, 2009). Hence, Tom’s continual reliance on these strategies may prove to be maladaptive in relation to his personal goals beyond the acute diagnostic phase. Accordingly, the effectiveness of regulatory strategies also need to be considered in context of how adaptive the behavior is in terms of one’s physical and emotional well-being beyond the current (acute) time period (cf. Aldao and Christensen, 2015).
Treatment phase
Although individuals cannot modify the duration of their treatment(s), these individuals can modify their treatment situation by choosing to attend sessions with support from family members or friends (e.g. Table 2). Indeed, the oncology treatment setting provides numerous cues to trigger cancer-related thoughts and rumination patterns. Hence, some individuals may try to modify their situation by minimizing the waiting period at the hospital by trying to get to the appointment as close as possible to the designated time (e.g. Kangas et al., 2014). For persons who are employed at the time of diagnosis, typically, most individuals take some leave from work during the acute treatment phase. During this phase, it may be difficult for individuals to not have their attention focused on their cancer and health, particularly for persons who have to attend daily treatment sessions. However, some individuals may intentionally utilize distraction techniques (e.g. listening to music) while receiving treatment to try to redirect their attention to non-cancer related matters.
Unavoidably, the main forms of oncology treatments all give rise to treatment side effects (e.g. Saligan et al., 2015). These can further activate cognitive changes (e.g. Arndt et al., 2014). While some individuals may interpret the physical side effects in a catastrophizing manner (e.g. fear that the pain will worsen and is indicative of declining health), others may adopt a more problem-solving approach and appraise their circumstances in a more objective, neutral, or even optimistic outlook, acknowledging that treatment side effects are typical and necessary process of trying to eradicate cancer (e.g. Belinda’s case in Table 2). For individuals akin to Belinda, who elicit cognitive change by adopting a more objective approach, they may further modulate their acute distress reactions by continuing to proactively engage with their social networks, even when feeling physically and emotionally depleted. That is, even for persons who have an objective or even optimistic outlook, this does not mean they are immune to experiencing transient heightened affective states including anxiety, sadness, or anger. Studies have shown that patients who utilize adaptive cognitive strategies including proactively seeking social support in the diagnostic and treatment phases have reported better QOL including less distress by 6 months following cancer treatment (e.g. Silva et al., 2012).
For persons who engage in negative cognitive appraisals, although they may also rely on close family support networks during this phase, they may be more withdrawn from engaging with extended social support networks, thus placing a greater demand on family members. However, experiential (social) avoidance per se does not necessarily denote a maladaptive affect regulation strategy in the short-term. It is the chronicity as well as rigidity of utilizing such strategies that would determine the utility of relying on this approach over time. Indeed, some individuals opt to primarily focus on their treatment and recovery, while temporarily ceasing social and occupational activities until they recover from the acute cancer side effects. Similarly, some individuals may use expressive suppression strategies when interacting with family and friends during this phase for various reasons including trying not to burden or worry family members with how they are feeling, trying to remain “stoic” and “strong” even when feeling unwell or despondent, and as a tactic to not excessively dwell on their cancer. However, this may impede emotional processing and subsequent adjustment as studies have shown that cognitive avoidance and emotional suppression to be predictive of subsequent psychological distress (Andreu et al., 2012).
Treatment recovery and survivorship phase
The majority of individuals try to resume their usual routine (i.e. situation selection) as soon as their acute side effects subside, although they may continue to experience some residual side effects (e.g. fatigue; Lo-Fo-Wong et al., 2016). For some persons, their cancer is the impetus which motivates them to pursue current and future goals post-treatment and into the survivorship phase (e.g. Cindy in Table 2). In fact, research has revealed that young adult cancer patients who engage in approach-oriented coping strategies including goal engagement reported better emotional well-being than patients with reduced approach-oriented coping responses (e.g. Hoyt et al., 2016).
Furthermore, some individuals may intentionally try to eradicate any reminder of their cancer experience; for instance, by filing away medical documents and avoiding cancer-related media and conversations (i.e. situation modification), while focusing on pursuing and enacting their current and future goals (attentional deployment and response modulation). Others may be more vigilant in making a conscious effort to attend annual medical check-ups (comparable to Cindy) as a way to help assuage their health concerns in the longer term. To this end, an individual’s appraisal of their current and anticipated future health may lead to a positive cognitive shift which may influence short-term goals and further contribute to how effectively they regulate their emotions during both the acute recovery and survivorship phases. Firmin et al. (2014) reported that individuals adopt a pragmatic approach (which participants referred to as a “Carpe Diem attitude”) during the survivorship phase, as well as intentionally changing their health behaviors given that health becomes a key priority during this phase. Conversely, individuals who adopt a more negative, catastrophizing outlook during this phase may have more elevated chronic distress and further modulate their affective state by avoiding health check-ups, or alternatively enduring them with trepidation, and which may further interfere with their current and future goal pursuits including health behavior changes.
Notably, however, there is very limited theory-driven longitudinal studies during the survivorship phase (Mosher et al., 2016), which have examined the different trajectories of adjustment inclusive of tracking affect regulatory processes that may predict better or worse psychosocial outcomes over time. This is an important line of research to pursue given that studies have shown that the transition from post-cancer treatment to the survivorship period involves numerous emotional, physical, and social changes (e.g. Allen et al., 2009). Not surprisingly, fear of cancer recurrence (FOCR) also arises during this phase.
In the past decade, there is a burgeoning body of predominantly cross-sectional studies which have demonstrated that FOCR is quite common in newly diagnosed and recently treated cancer patients (Simard et al., 2013). Of the limited studies which have examined FOCR longitudinally between diagnosis and post-treatment recovery, mixed findings have emerged as to whether the rates of FOCR remain stable (e.g. Llewellyn et al., 2008) or decline between diagnosis and post-treatment recovery (e.g. Sarkar et al., 2014). However, there is a notable paucity of research examining the relationship between affect regulation strategies and FOCR across the cancer trajectory. This is an important avenue for future research given that FOCR can serve both as an adaptive function by way of leading to healthy behavioral changes during the survivorship phase (e.g. Taylor et al., 2011), as well as being detrimental for others (cf. Simard et al., 2013), especially if it contributes to entrenched maladaptive strategies (e.g. daily hyper vigilance of checking body symptoms for signs of cancer).
Recurrence or metastatic disease
Receiving the news that one has a recurrence of cancer or metastatic disease can give rise to an array of affective states including anger, sadness, grief, and fear. Some individuals with recurrent or metastatic disease may still have treatment as an option. For individuals who may no longer have the option of conventional medical oncology treatment, they may seek alternative therapies as an attempt to try to prolong their life (e.g. Gross et al., 2007). Given the prognosis of being diagnosed with recurrent disease, or metastatic cancer is typically not favorable for the medium to longer term, individuals may start to ruminate about the prospects of dying. Individuals may also experience a cognitive shift where they may try to remain hopeful, for example, that treatment may work to prolong their life even by a few years (such as Brian in Table 2). This does not mean that these individuals may not still fear death; hence, to regulate this fear, they may use a combination of response strategies including engaging in hobbies when they can as well as expressive suppressive strategies to not show their fear in the presence of family and friends. Indeed, research has documented that the use of more disengagement coping contributed to poorer mental health in breast cancer patients who experienced a recurrence of disease, while stressed patients who adopted more active-oriented coping reported better mental health outcomes 4-months later (Yang et al., 2008).
To date, studies have shown that coping is not necessarily stable over time (e.g. Geyer et al., 2015). Importantly, there is no distinct set of coping styles that have been documented to predict better or worse functioning during the survival and cancer recurrence phases (Petticrew et al., 2002). This further attests to the need for more conceptually driven longitudinal research in oncology to investigate the affect regulatory processes that patients utilize across the survivorship phase and which may extend into the cancer recurrence and end-of life phases, in order to further our understanding as to which intrapersonal, interpersonal, medical, and other contextual factors contribute to better adjustment across the cancer trajectory.
End-of-life phase
Persons who have reached a terminal phase also have to contend with many different emotional and physical symptoms (e.g. O’Connor et al., 2010; Teunissen et al., 2007) and may also explore palliative options (e.g. Tom in Table 2). Individuals may also modify their situation by resigning from work and relying on family and close friends for practical and social support. Understandably, the thought of dying is salient during this final phase. Hence, individuals may oscillate between ruminating about their plight, while trying to wrap up loose ends and also experiencing a cognitive change in terms of reflecting on their life experiences (e.g. Tom in Table 2) and being appreciative of all they have accomplished, and with support coming to terms with dying, as they try to spend as much time with family and close friends.
Understandably, social support has been documented to be pivotal in maintaining or enhancing well-being during the end-of-life phase (e.g. Ringdal et al., 2007; Walshe et al., 2017). Indeed, in a recent study based on a mixed sample of advanced cancer patients, participants noted that their social support network, including learning from peers facilitated their own psychological well-being in utilizing helpful coping strategies (Walshe et al., 2017). Conversely, palliative care patients who feel depressed, demoralized, and experience a loss of meaning and purpose in life have been found to have an increased desire to hasten death (Robinson et al., 2017). This latter finding aligns with research by Tang et al. (2015) who found that palliative care patients who did not initially experience a sense of defeat reported growth during the palliative phase, whereas patients with low growth had severe symptoms of distress, weak social support, and low acceptance of their prognosis. Similarly, Goodwin et al. (2014) have also found that palliative cancer patients with a greater acceptance of their prognosis as well as positivity had lower desire for hastened death relative to patients with lower acceptance and positivity. Moreover, social support was significantly positively associated with acceptance and positivity in this study, which further accentuates the pivotal role that strong social support has in facilitating emotional adjustment during this end-of-life phase. Similarly, research has also accentuated the importance of relying on a strong social support network to enhance mental well-being in family members of patients with advanced cancer (Sjolander and Ahlstrom, 2012).
Contribution of intrapersonal and environmental factors and flexibility
Across each of the five main cancer phases, we further propose that affect regulatory strategy selection is influenced by a range of intrapersonal attributes as well as environmental factors. Intrapersonal factors that may influence strategy selection include the individuals’ habitual use of any particular strategy or series of strategies, their predisposition to utilize particular forms of affect regulatory tactics, their beliefs in the utility as well as their ability to apply particular regulation strategies to manage their affective state, psychological history as this may also influence their habitual use of specific strategies, and whether the person has had any formal training in specific strategies (e.g. previous psychotherapy taught to implement cognitive reappraisal). In terms of environmental attributes influencing affect regulatory strategy selection, we propose at least two types of factors: interpersonal attributes and environmental stressors. For interpersonal factors, a person’s access to and quality of social support may also influence their strategy selection and implementation. A robust finding in the trauma field (e.g. Ozer et al., 2003) as well as the psycho-oncology literature (e.g. Carpenter et al., 2010) is that quality of social support can have a buffering effect against the emotional impact of adverse events, for patients and their partners as well as other family members.
Additional environmental factors that may impact affect regulatory processes for oncology patients include the professional interactions they have with health-care providers. Notably, studies have shown that how doctors and other health-care providers deliver news including the diagnosis, prognostic updates, and treatment options can have an impact on patients subjective well-being including adherence to treatment (Cao et al., 2017; Diefenbach et al., 2009). Importantly, good doctor–patient communication behaviors include health-care providers asking about the patient’s emotional well-being (Diefenbach et al., 2009). To that end, in a recent study, doctors’ emotional support was a key predictor which was positively related to cancer patients’ perceived trust and hope following disclosure of their cancer diagnostic status (Cao et al., 2017). Accordingly, the interactions patients have with health-care providers can further shape their affect regulatory responses.
Concurrent environmental stressors may further influence affect regulatory strategy selection. For example, if a person is already utilizing a specific form of regulatory process to manage a current crisis (e.g. relying on distraction strategies to get through the acute cancer diagnostic crisis), they may also be inclined to rely on applying this strategy to subsequent stressors that may arise in the short term (e.g. experiencing treatment complications post-operatively).
Moreover, we propose that a person’s flexibility in applying affect regulatory strategies when challenges arise both within and across each of the cancer phases is instrumental in adapting to stressors. Although there is no universal definition of the term “emotion regulation flexibility,” from an individual differences perspective, it has been operationalized as matching regulatory strategies to the environmental contextual demands to facilitate one’s personal goals (e.g. Aldao et al., 2015; Bonanno and Burton, 2013), which attests to the importance of context specificity. The flexibility in shifting selection and implementation of various types of affect regulatory tactics is important. That is, while a specific strategy may be adaptive in one context, the continued implementation of this strategy in changing contextual demands may prove to be maladaptive in terms of one’s goals and hence shifting one’s mood over time. For example, as illustrated in Table 1, following his diagnosis, Tom avoids social interactions, as well as primarily relying on utilizing one form of reappraisal (i.e. catastrophizing), which if he continues to do throughout his treatment phase, his mood may further deteriorate. This also highlights the scope for the concurrent use of various blends of emotion regulatory strategies to manage affective states. We propose that selecting which combination of affect regulatory strategies to simultaneously as well as sequentially implement within and between phases, across the cancer trajectory, requires affect regulation flexibility.
Future research directions
As emphasized above, there is a notable paucity of studies that have systematically examined the selection and implementation of specific affect regulation strategies across the different phases of the cancer trajectory. Although our proposed ARC framework needs to be empirically evaluated, the utility of our model is that it comprises core elements that provide more process specificity, which can be tested across the various cancer phases.
Multiphase, longitudinal research is warranted to assess the implementation of affect regulatory strategies in managing affect within and across the cancer trajectory. In line with the current directions for research in the affective sciences field (Gross, 2015), the cancer domain provides a fruitful avenue to specifically test the sequencing and concurrent use of specific affect regulatory strategies both within each cancer phase and across the trajectory in terms of influencing emotional adaptation both in the short and long terms. Brandao et al.’s (2016) recent systematic review highlighted that the bulk of psycho-oncology studies that have tested coping strategies and emotion regulatory tactics have been based on cross-sectional designs. Even for studies that have used longitudinal or multiphased assessments, these have typically been conducted within one phase of the cancer trajectory. This result further attests to the need to conduct more multiphase, longitudinal psycho-oncology studies to further delineate the affect regulatory processes across the cancer trajectory and between different oncology populations.
To date, researchers have tended to use a categorical perspective in evaluating the effectiveness of affect regulation strategies. However, a more process-oriented method is warranted in psycho-oncology in light of recent advances in the broader affective science field including the role of context specificity and individual differences (inclusive of emotion regulation flexibility; Aldao et al., 2015; Bonanno and Burton, 2013; Gross, 2015) in determining the effectiveness and adaptability of regulatory processes. For example, factoring in context specificity when examining the utility and effects of affect regulation tactics in cancer patients within different phases across the trajectory, reappraisal may not always be more effective than utilizing alternative strategies such as distraction or expressive suppression to manage heightened emotional states. Studies have shown that under very high emotionally intensive contexts, individuals show a preference for distraction, while for more moderate to lower levels of emotional intensity, reappraisal is commonly the preferred and typically more effective strategy (e.g. Sheppes et al., 2011). Therefore, in terms of evaluating the sequential implementation of affect regulation strategies across the cancer trajectory, emotional intensity is an important moderator to consider. For instance, an individual may be utilizing social avoidance, distraction, and expressive suppression strategies to manage his/hers anxiety and stress during the acute cancer treatment phase. Although at the completion of their treatment, individuals may experience some relief accompanied by a decline in anxiety as they switch to using a more positive appraisal approach as well as socially re-engaging with their peer networks as they progress into the recovery phase. However, the proposition that emotional intensity may moderate the implementation of different affect regulation tactics within and between different cancer phases remains to be empirically tested in future research.
We further suggest that in addition to emotional intensity, other individual difference variables also need to be considered. Specifically, it will be important to assess whether the implementation of specific affect regulation strategies are modulated by personal beliefs in utilizing specific strategies to manage one’s affect at various phases of their cancer experience (i.e. “affect-regulation self-efficacy”). A related and further avenue for future research is investigating the simultaneous blends versus sequential implementation of specific affect regulation tactics within and between different cancer phases. To date, the bulk of research in the main affective science field has focused on examining the effectiveness and adaptability of single types of affect regulation strategies. Hence, which simultaneous blends as well as sequences of affect regulatory strategies are more or less effective in specific contexts have yet to be empirically investigated (Gross, 2015). As aforementioned, we propose that selecting which combination of regulatory strategies to simultaneously as well as sequentially implement within and between phases, across the cancer trajectory, requires affect regulation flexibility. The psycho-oncology domain provides a fruitful avenue to systematically pursue this important line of inquiry in elucidating which patterns of affect regulatory strategies in combination or sequentially facilitate emotional adaptation across the cancer trajectory. Moreover, the extent to which specific affect regulation tactics, or blends of strategies, serve to modulate the adaptive versus maladaptive function of FOCR as well as promote authentic growth are two further key areas that warrant empirical investigation.
Finally, interpersonal attributes may further influence the affect regulatory processes. In particular, a person’s access to and quality of social support may also influence their strategy selection and implementation. Indeed, there is increasing recognition that affect generative and regulatory processes are shaped by social factors across the lifespan (Reeck et al., 2016). Accordingly, cancer patients may be influenced and may also shape the affect regulatory responses of family members. To this end, studies which assess the regulation of affect between cancer patients and their partners as well as other family members would help delineate what effects the co-regulation of emotions has between couples and extended family members across the cancer trajectory. Similarly, cultural factors may also modulate a person’s affect regulatory choices and expression and warrant testing in future oncology studies. Additionally, as aforementioned, the interpersonal interchanges between health-care providers and patients may also modulate patients’ affect regulatory processes. However, prospective, longitudinal studies are needed to investigate how health-care providers’ interactions influence patients’ affect regulatory strategies across pivotal medical consultations across the cancer trajectory.
In the last two decades, the field of affective science has experienced an exponential growth in laboratory and field studies examining affect regulatory processes (Gross, 2015). However, the field of psycho-oncology has lagged behind in terms of understanding the affect generative and affect regulatory processes elicited across the various phases of the cancer trajectory. Given that cancer is a dynamic experience, to further advance our understanding of what types and patterns of affect regulatory processes are related to emotional well-being, it is time to systematically integrate the insights from affective science within the oncology field. In this article, we have described how our ARC framework may help to achieve this goal.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.