
Abstract
Accurately diagnosing autism spectrum disorders in adulthood can be challenging. Structured questionnaires and diagnostic measures are frequently used to assist case recognition and diagnosis. This study reviewed research evidence on structured questionnaires and diagnostic measures published since the National Institute for Health and Care Excellence evidence update. The Cochrane library, Medline, Embase and PsycINFO were searched. In all, 20 studies met inclusion criteria. Sensitivity and specificity of structured questionnaires were best for individuals with previously confirmed autism spectrum disorder diagnoses and reduced in participants referred for diagnostic assessments, with discrimination of autism spectrum disorder from mental health conditions especially limited. For adults with intellectual disability, diagnostic accuracy increased when a combination of structured questionnaires were used. Evidence suggests some utility of diagnostic measures in identifying autism spectrum disorder among clinic referrals, although specificity for diagnosis was relatively low. In mental health settings, the use of a single structured questionnaire is unlikely to accurately identify adults without autism spectrum disorder or differentiate autism spectrum disorder from mental health conditions. This is important as adults seeking an autism spectrum disorder diagnostic assessment are likely to have co-existing mental health conditions. Robust autism spectrum disorder assessment tools specifically for use in adult diagnostic health services in the presence of co-occurring mental health and neurodevelopmental disorders are a research priority.
Introduction
The importance of evaluating autism spectrum disorder diagnostic tools in adult populations
Research on the diagnosis of autism spectrum disorder (ASD) has to date predominately focussed on childhood. Compared to the number of studies recruiting child populations, there are few studies (e.g. Brugha et al., 2015; Lehnhardt et al., 2013) specifically examining the psychometric properties of tools used in the diagnosis of suspected ASD in adulthood, for example, the Diagnostic Interview for Social and Communication Disorders (DISCO; Wing et al., 2002). The tools used in the diagnosis of ASD are structured questionnaires (SQs) that are generally self-report or informant completed brief measures developed as ASD screening tools; and diagnostic measures (DMs), which are more in-depth assessment tools that tend to involve semi-structured interviews and interactive tasks to inform an ASD diagnosis (National Institute for Health and Care Excellence (NICE), 2012; Scottish Intercollegiate Guidelines Network (SIGN), 2016). For adults with a suspected ASD diagnosis, there are significant limitations in access to high-quality diagnostic assessments. The reasons for this include both the availability of diagnostic services and psychometrically established measures (Brugha et al., 2015; Lehnhardt et al., 2013; Powell and Acker, 2016). SQs and DMs can assist clinicians making a diagnosis (NICE, 2012; SIGN, 2016) and can be used in conjunction with direct observation and other sources of information (APA, 2013; ICD-10, 1992). However childhood measures are not always suitable for adults where the presentation of ASD may be masked by maturation, learned compensatory skills and the presence of co-occurring mental health and neurodevelopmental disorders. Furthermore, informants (particularly parents) and information about early history may be unavailable (Brugha et al., 2012, 2015).
The NICE guidelines on case recognition and diagnosis of ASD in adults
As part of the development of evidence-based clinical guidelines for the assessment and management of ASD in adults, the UK NICE (2014) reviewed and published evidence on the use of SQs and DMs for case recognition and diagnosis in adults with suspected ASD. These guidelines recommended a battery of SQs and DMs that could contribute to an ASD diagnosis (see Table 1 for a summary).
ASD screening and diagnostic measures for adults and evidence recommended by NICE (2012, 2014).
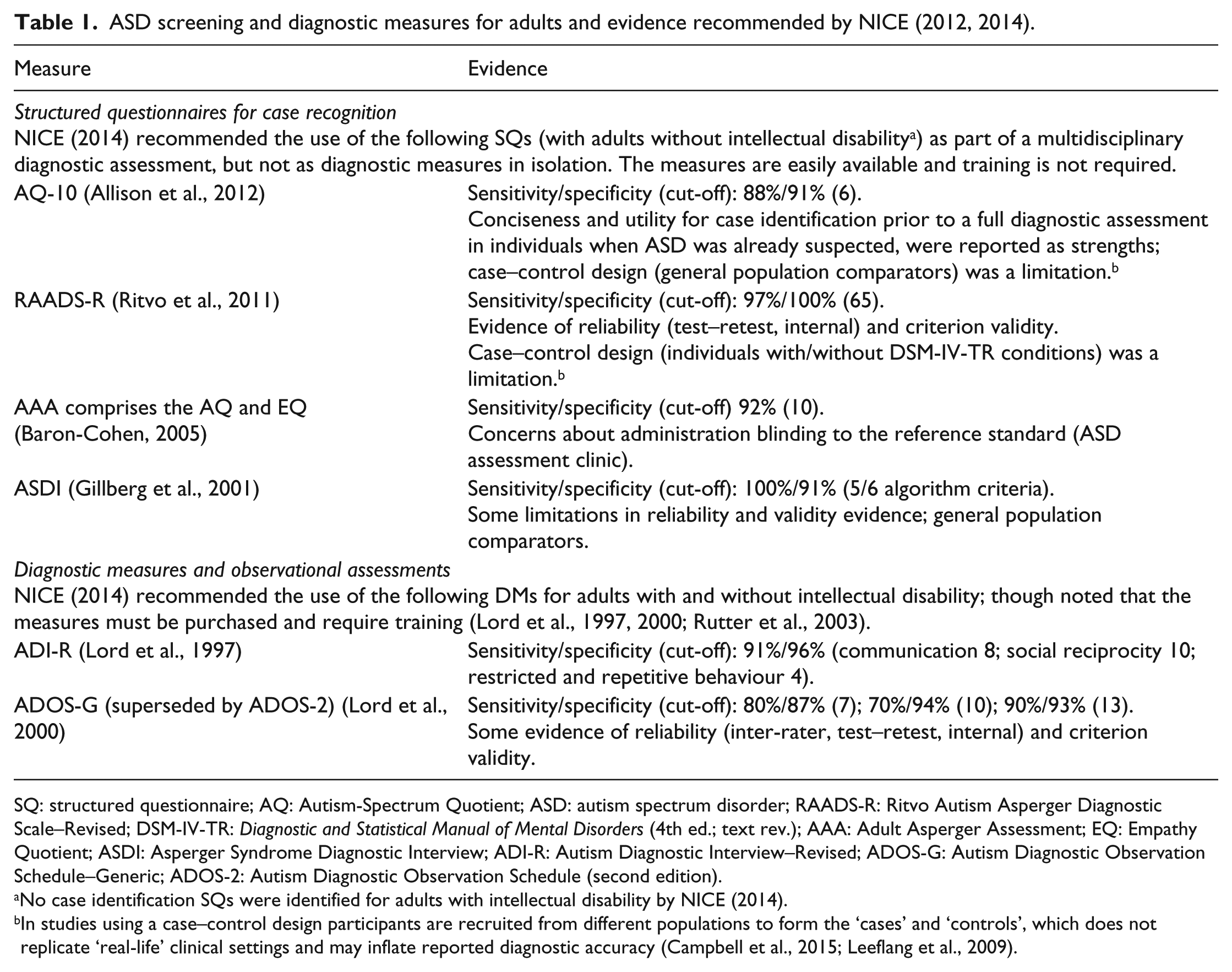
SQ: structured questionnaire; AQ: Autism-Spectrum Quotient; ASD: autism spectrum disorder; RAADS-R: Ritvo Autism Asperger Diagnostic Scale–Revised; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders (4th ed.; text rev.); AAA: Adult Asperger Assessment; EQ: Empathy Quotient; ASDI: Asperger Syndrome Diagnostic Interview; ADI-R: Autism Diagnostic Interview–Revised; ADOS-G: Autism Diagnostic Observation Schedule–Generic; ADOS-2: Autism Diagnostic Observation Schedule (second edition).
No case identification SQs were identified for adults with intellectual disability by NICE (2014).
In studies using a case–control design participants are recruited from different populations to form the ‘cases’ and ‘controls’, which does not replicate ‘real-life’ clinical settings and may inflate reported diagnostic accuracy (Campbell et al., 2015; Leeflang et al., 2009).
In practice, clinicians and researchers use a range of SQs and DMs to aid diagnosis, not all of which were included in the NICE recommendations (Rogers et al., 2015; Rutherford et al., 2016). For example, when the NICE (2014) review was completed, no diagnostic test accuracy studies were included regarding the use of the DISCO (Leekam et al., 2002; Wing et al., 2002) or the Developmental, Dimensional and Diagnostic Interview (3DI; Skuse et al., 2004), in adult populations. In addition, some published SQs (usually in self-report format) have been developed to measure ASD traits that may not directly map onto diagnostic criteria, for example, the AQ (Autism Spectrum Quotient; Baron-Cohen et al., 2001). Given the current availability of various different tools, the psychometric properties of the SQs and DMs used in clinical and research practice require further consideration (Rogers et al., 2015; Rutherford et al., 2016).
Aims of the study
The aims of this systematic review were therefore to
Identify studies published since the NICE (2014) guidelines update on evidence for the assessment of ASD in adults that describe the psychometric properties of the SQs and DMs available to clinicians and researchers for identifying ASD in adults.
Examine the quality of the identified studies.
Make recommendations about which of the measures, if any, might be most appropriate for the diagnostic assessment of ASD in adults, based on current evidence.
Method
NICE first published the adult autism clinical guideline (CG142) in 2012 (with an evidence update in 2014). This systematic literature review includes papers published between January 2013 and October 2017 and coincides with the publication of Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) and the revised criteria for ASD that are used throughout this article (APA, 2013). The review search terms and inclusion criteria are shown in Table 2.
Search terms, study sources including databases and study inclusion criteria.
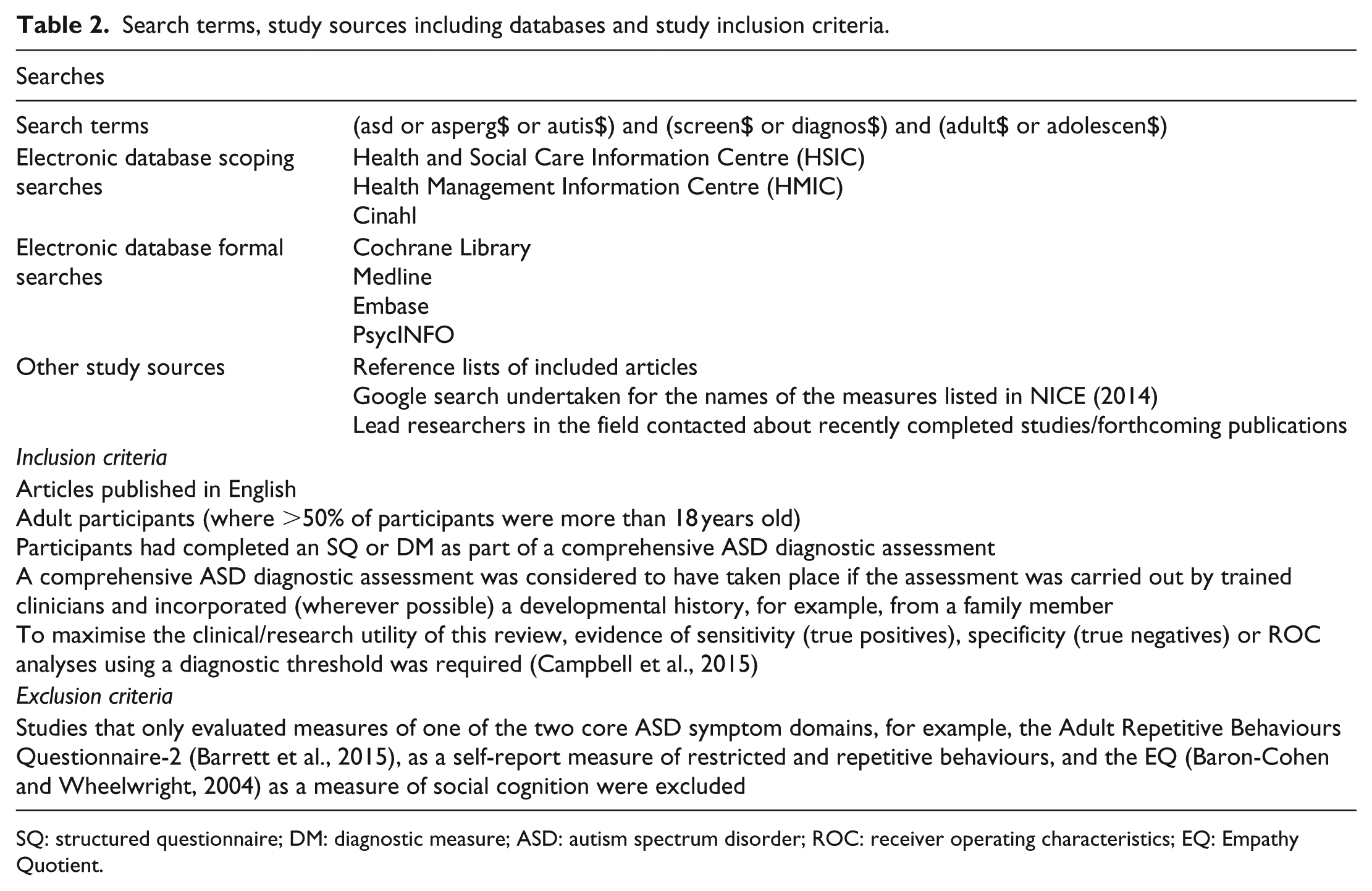
SQ: structured questionnaire; DM: diagnostic measure; ASD: autism spectrum disorder; ROC: receiver operating characteristics; EQ: Empathy Quotient.
Titles and abstracts were screened by S.W. with 20% screened independently by a second reviewer (T.B.). S.W. and T.B. reviewed full texts of selected articles independently; uncertainties about inclusion were resolved through discussion with the research team. The selection process to determine eligibility of articles for inclusion in the review is shown in Figure 1. Data were synthesised narratively, and risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) measure for examining the quality of diagnostic studies (Campbell et al., 2015; Whiting et al., 2011). The second reviewer independently rated 20%; reviewers 1 and 2 had 96% agreement on bias ratings.
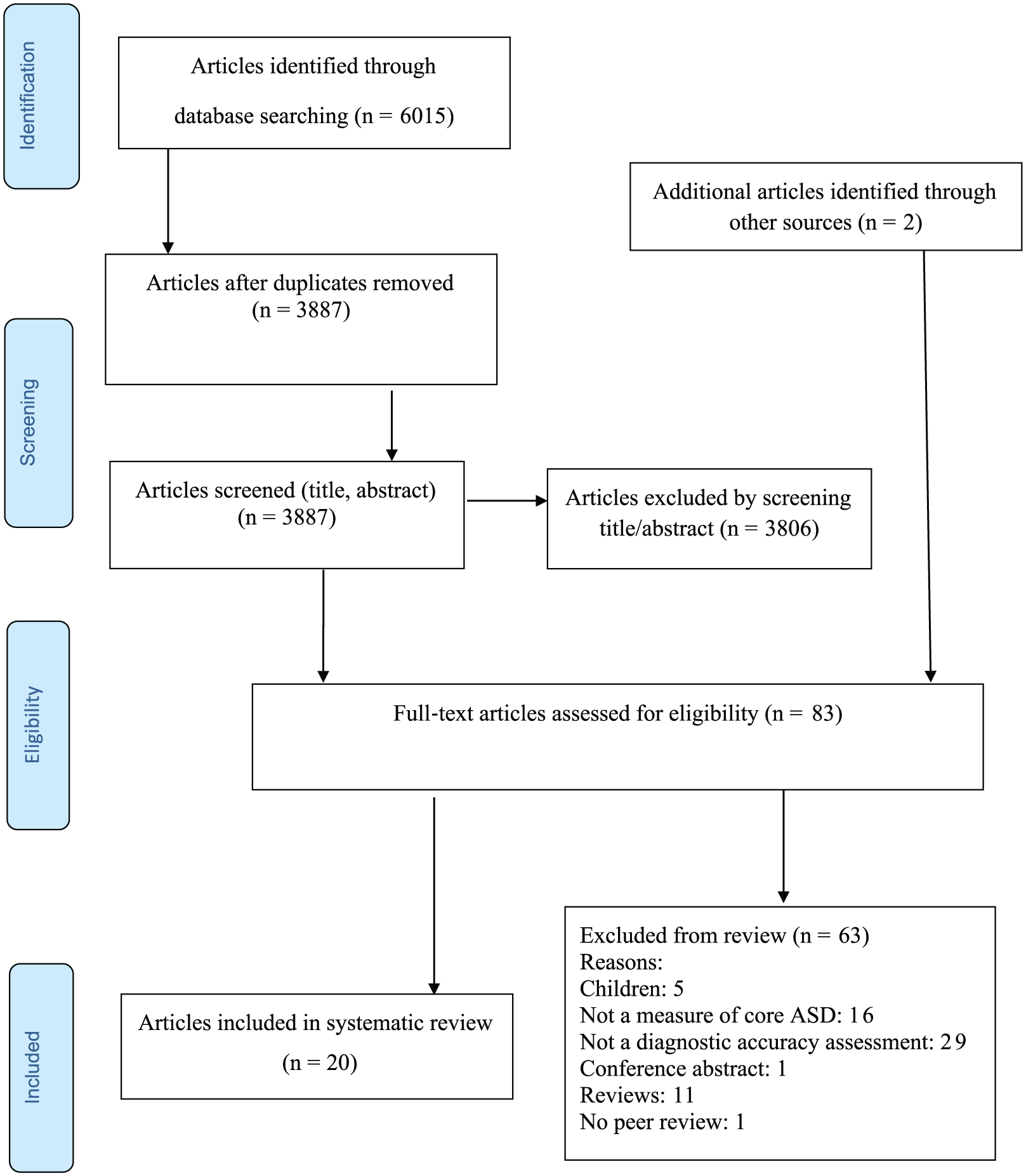
Summary of the search selection process.
Results
In all, 3887 articles were identified after removal of duplicates (Figure 1). 83 articles were read in full and 20 articles were selected for inclusion in the review. A brief summary of the characteristics of the measures from the selected articles is provided in Table 3.
Summary of characteristics of SQs and DMs evaluated in the studies included in this review.
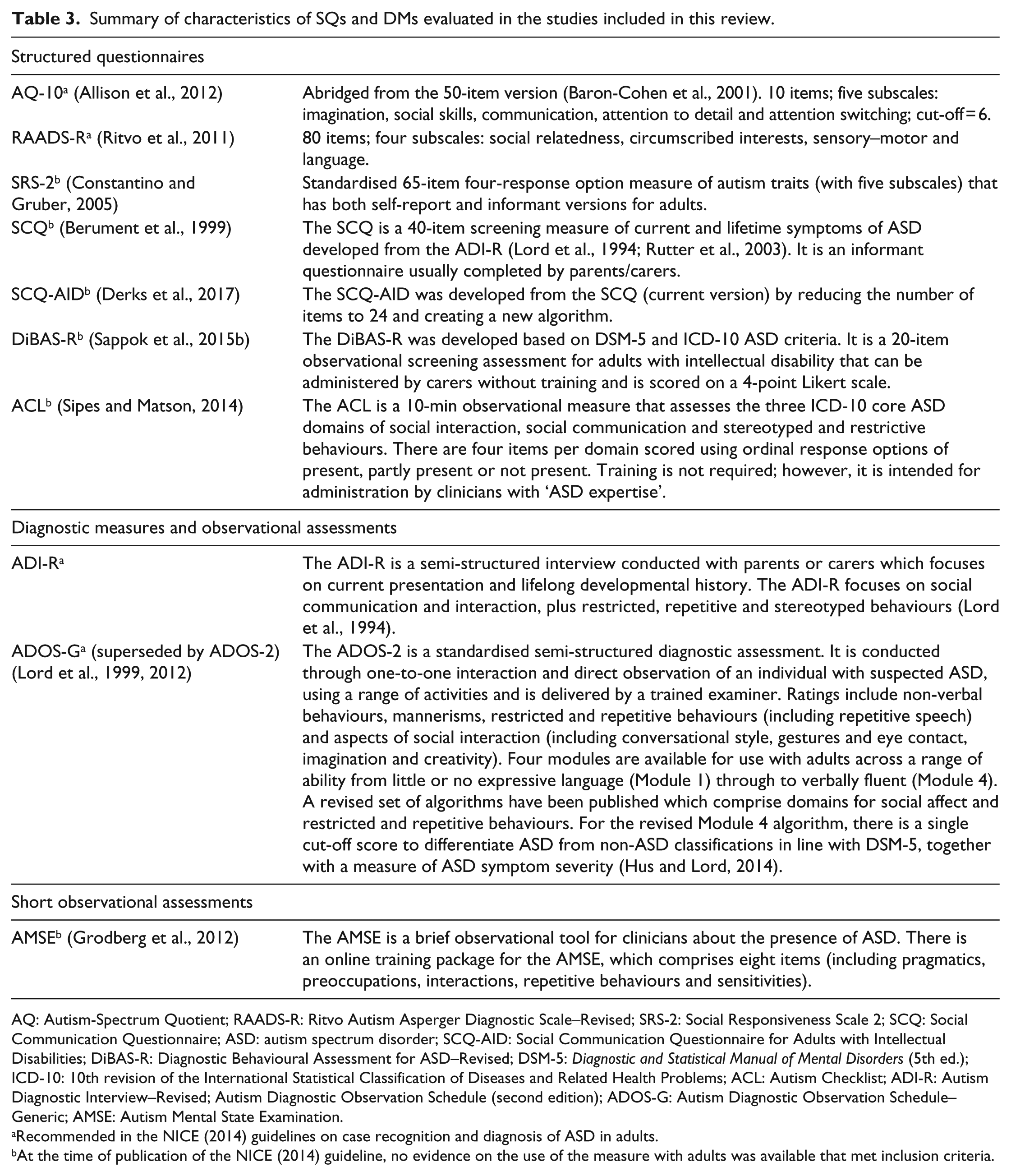
AQ: Autism-Spectrum Quotient; RAADS-R: Ritvo Autism Asperger Diagnostic Scale–Revised; SRS-2: Social Responsiveness Scale 2; SCQ: Social Communication Questionnaire; ASD: autism spectrum disorder; SCQ-AID: Social Communication Questionnaire for Adults with Intellectual Disabilities; DiBAS-R: Diagnostic Behavioural Assessment for ASD–Revised; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.); ICD-10: 10th revision of the International Statistical Classification of Diseases and Related Health Problems; ACL: Autism Checklist; ADI-R: Autism Diagnostic Interview–Revised; Autism Diagnostic Observation Schedule (second edition); ADOS-G: Autism Diagnostic Observation Schedule–Generic; AMSE: Autism Mental State Examination.
Recommended in the NICE (2014) guidelines on case recognition and diagnosis of ASD in adults.
At the time of publication of the NICE (2014) guideline, no evidence on the use of the measure with adults was available that met inclusion criteria.
Bias ratings are shown online in the Supplementary material and summarised with the current review’s findings for each measure. Most studies were conducted in Europe, two in Japan (Nishiyama et al., 2014; Takei et al., 2014) and four in the United States (Grodberg et al., 2014; Hus and Lord, 2014; Maddox et al., 2017; Pugliese et al., 2015). Two studies were multi-site with participants recruited from the United States, United Kingdom and Germany (Derks et al., 2017; Sappok et al., 2017). Six studies focussed on adults with intellectual disabilities (Derks et al., 2017; Heinrich et al., 2017; Mutsaerts et al., 2016; Sappok et al., 2014, 2015a, 2017). Study designs were case–control, cross sectional or retrospective.
Structured Questionnaires (SQs)
SQs are usually self-report (but can be informant completed), do not require training for administration and have been used in epidemiological studies, and to gather information prior to a full diagnostic assessment (Mutsaerts et al., 2016; NICE, 2014). Evidence for SQs available at the time of the NICE (2014) recommendations is shown in Table 1; new evidence identified in the current review from studies evaluating SQs since the NICE (2014) guideline is shown in Table 4.
Findings from the studies evaluating structured questionnaires.
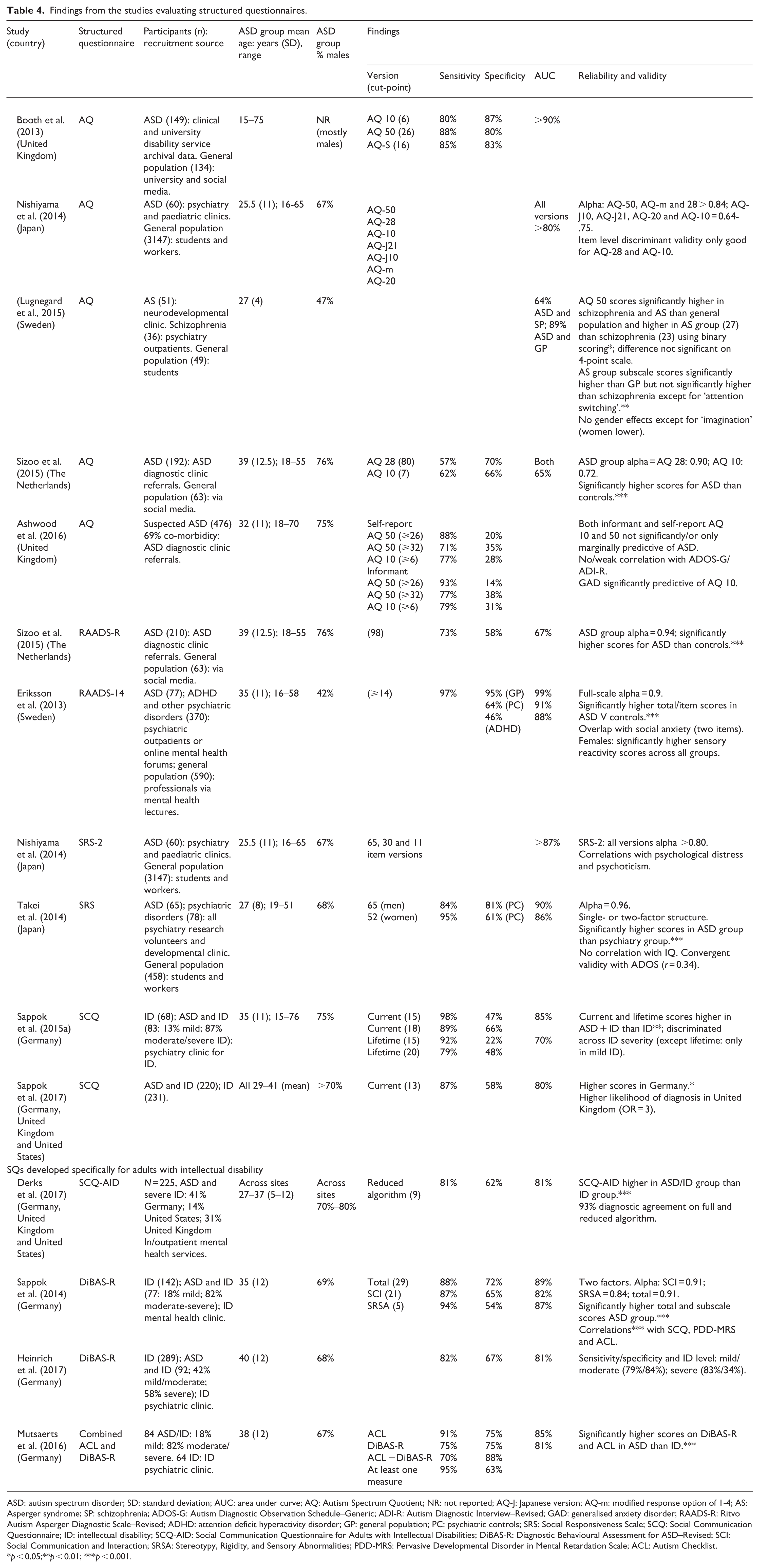
ASD: autism spectrum disorder; SD: standard deviation; AUC: area under curve; AQ: Autism Spectrum Quotient; NR: not reported; AQ-J: Japanese version; AQ-m: modified response option of 1-4; AS: Asperger syndrome; SP: schizophrenia; ADOS-G: Autism Diagnostic Observation Schedule–Generic; ADI-R: Autism Diagnostic Interview–Revised; GAD: generalised anxiety disorder; RAADS-R: Ritvo Autism Asperger Diagnostic Scale–Revised; ADHD: attention deficit hyperactivity disorder; GP: general population; PC: psychiatric controls; SRS: Social Responsiveness Scale; SCQ: Social Communication Questionnaire; ID: intellectual disability; SCQ-AID: Social Communication Questionnaire for Adults with Intellectual Disabilities; DiBAS-R: Diagnostic Behavioural Assessment for ASD–Revised; SCI: Social Communication and Interaction; SRSA: Stereotypy, Rigidity, and Sensory Abnormalities; PDD-MRS: Pervasive Developmental Disorder in Mental Retardation Scale; ACL: Autism Checklist.
p < 0.05;**p < 0.01; ***p < 0.001.
Autism-Spectrum Quotient (AQ)
The evidence for the psychometric properties of the AQ published since the NICE (2014) guidelines and covered in the current review is not consistent, varying according to study design and recruitment source (Baron-Cohen et al., 2001). The sensitivity and specificity of the AQ-50 and the AQ-10 were good (⩾80%) when comparing archival clinical data from adults with ASD, against a general population group (Booth et al., 2013). However, this is not equivalent to the population of subjects presenting to ASD diagnostic assessment settings. In such settings, case recognition and the need to consider both differential diagnosis and the identification of additional mental health problems can be challenging.
In a Japanese study (Nishiyama et al., 2014) recruiting individuals with a known diagnosis of ASD, and a comparison general population sample, the internal consistency and construct validity of short versions of the AQ were inconsistent. A strength of the study was that a battery of screening measures were administered to all participants, including the general population comparator group, to identify any co-occurring mental health conditions.
A further study recruiting individuals with schizophrenia (Lugnegard et al., 2015) from a psychiatric clinic, adults with ASD and individuals from the general population, found that ASD and schizophrenia were both significantly associated with a higher AQ-50 score. In addition, only the AQ version with a binary response option discriminated reliably between ASD and schizophrenia and only on one subscale (attention switching; Lugnegard et al., 2015). There was no significant difference in AQ-50 scores between individuals with ASD and those with schizophrenia when using the 4-point response option. Participants were diagnosed prior to the study, though diagnoses of ASD and schizophrenia were confirmed in this study using the DISCO-11 (Wing et al., 2002) and the SCID-1 (Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; DSM-IV; First and Gibbon, 2004), respectively. However, such purposive recruitment of individuals with a defined specific diagnosis is not comparable to the use of the AQ in ASD diagnostic assessment clinical settings.
In the fourth article (Sizoo et al., 2015), individuals attending an ASD diagnostic clinic completed abbreviated versions of the AQ prior to a clinical assessment. The comparison group again consisted of individuals from the general population. Reported specificity (more than 66%) and sensitivity (57%–62%) were lower than in the Booth et al. (2013) study. A strength of the study was the recruitment of participants from ASD clinics and administration of the AQ prior to their full assessment, which is similar to procedures in clinical settings.
Finally, Ashwood et al. (2016) reported findings using the subject and informant versions of the AQ-50 and the AQ-10. Participants were consecutively referred to an ASD assessment clinic and had high rates of comorbid mental health conditions. Across both AQ versions, sensitivity was above 71% but specificity was less than 38%, and the relationship between the AQ scores and the Autism Diagnostic Interview–Revised (ADI-R) and the Autism Diagnostic Observation Schedule–Generic (ADOS-G) was weak. Thus, the AQ did not reliably identify those individuals who did not have ASD. The presence of mental health conditions (such as a generalised anxiety disorder) also increased the risk of false-positive ASD diagnoses using the AQ-10 (Ashwood et al., 2016). This study highlights the limitations of the AQ in a more ecologically valid setting compared to studies using non-clinical general population comparison groups.
Thus, overall, the findings from these studies suggest that due to low levels of specificity, the AQ is not a reliable indicator of which people should progress to a full ASD assessment.
Ritvo Autism Asperger Diagnostic Scale–Revised
When the Ritvo Autism Asperger Diagnostic Scale–Revised (RAADS-R) was used in an ASD assessment service (Sizoo et al., 2015) and compared to a general population group, sensitivity was good (73%) but specificity was low (58%) (Ritvo et al., 2011). This indicated some problems accurately identifying those without ASD (Sizoo et al., 2015). Limitations in this study are similar to those reporting on the AQ, including the use of a case–control design and purposive recruitment of a general population comparison group that lacked mental health or developmental assessment. A study strength was that participants were recruited from ASD assessment services and administered the RAADS-R prior to full ASD assessment. The low levels of specificity reported suggest that the RAADS-R was not a reliable indicator of those who should progress to a full ASD assessment.
The psychometric properties of a 14-item version (the RAADS-14) were tested by Eriksson et al. (2013) in an ASD group, a clinical control group (individuals with ADHD, mood, psychotic and borderline personality disorders) and a general population group. The ASD group had significantly higher scores compared with the clinical control group. However, although both sensitivity (97%) and specificity (95%) were good with general population controls, the specificity for comparison with the clinical control group was reduced (to 46% with ADHD; Eriksson et al., 2013). Comparison to a psychiatric control group was clinically relevant, but study limitations again included case–control design and the lack of a consistent use of ASD and/or other mental health assessments in the control group; in addition, some participants were recruited online and for these individuals diagnoses were self-reported and not confirmed.
Social Responsiveness Scale 2
Full and shortened versions of the adult self-report Social Responsiveness Scale 2 (SRS-2) were translated into Japanese (Nishiyama et al., 2014) and completed by individuals recruited from the general population and from clinical services (Constantino and Gruber, 2005). These versions had good internal consistency but were correlated with symptoms of psychoticism and distress as measured by the Brief Symptom Inventory (BSI; Derogatis and Melisaratos, 1983) and the K10 (Kessler et al., 2002). A strength of the study was that the general population group was administered a battery of mental health screening measures; a limitation was diagnosis of participants prior to the study.
A Japanese translation of the SRS informant version (Takei et al., 2014) demonstrated good sensitivity in both genders, and good specificity in men with ASD, compared to individuals in a control group with mental health difficulties. However, specificity in women was reduced (61%) indicating limitations in identifying women who did not have ASD (Takei et al., 2014). A strength of this study was confirmation of diagnosis by the research team; a limitation was that only individuals in the ASD group completed a reference standard (the ADOS), and the control group had no clinical assessment to exclude the presence of ASD.
Social Communication Questionnaire
The Social Communication Questionnaire (SCQ; German version) was completed by parents or professional carers (in the majority of cases), of adults with intellectual disability and suspected ASD as part of routine clinical assessments of consecutive admissions to an intellectual disability mental health service (Berument et al., 1999; Sappok et al., 2015a). Interestingly, the SCQ current version (assesses the last 3 months) was found to be more effective than the lifetime version; the best combination of sensitivity (89%) and specificity (66%) was achieved by raising the SCQ cut-score for ASD from 15 to 18. When the focus was on lifetime development, specificity decreased to 48%. This finding may have been because the SCQ was completed by a professional carer who may not have known about a subject’s early development, rather than a family member. About 87% of included participants had a moderate/severe intellectual disability, so the findings may not generalise to adults with milder intellectual disability (Sappok et al., 2015a). A strength of the study was that no exclusions were made on grounds of neurodevelopmental or mental health comorbidities, increasing the clinical validity of the sample.
Cross-cultural validity of the SCQ current version was examined in a study recruiting adults with intellectual disability from mental health services in Germany, the United Kingdom and the United States (Sappok et al., 2017). In contrast to the previous study (Sappok et al., 2015a), a lower cut-score of 13 was found optimal and made for sensitivity of 87% and specificity of 58%. More severe levels of intellectual disability were associated with higher scores. In some cases, administration of the SCQ was prior to an ASD assessment so informants completing the measure were blind to diagnosis; however, variations in administration of the SCQ in different countries may have introduced bias. SCQ scores were influenced by gender and country with males and those recruited in Germany having higher scores.
Structured Questionnaires (SQs) developed for use with adults with intellectual disability
Social Communication Questionnaire for Adults with Intellectual Disabilities
International data (from Germany, the United States and United Kingdom) were collected from individuals recruited via intellectual disability mental health settings with the SCQ for Adults with Intellectual Disabilities (SCQ-AID) completed by carers or researchers (Derks et al., 2017). The new algorithm with a cut-point of nine demonstrated sensitivity of 81% suggesting the shortened version has clinical utility though as found by Sappok et al. (2015a, who used the original version) specificity was low (62%). A strength of the study was the international recruitment of participants; however, the authors noted some differences in diagnostic process across sites. Further independent evaluation of this new measure is needed.
The Diagnostic Behavioural Assessment for ASD–Revised
When the Diagnostic Behavioural Assessment for ASD–Revised (DiBAS-R) was completed by a relative or staff member supporting an adult accessing an intellectual disability service, rates of 81% sensitivity and specificity were found when comparing those with and without ASD (Sappok et al., 2014, 2015b). These findings using this new measure are encouraging, and a strength of the study is that diagnoses were made contemporaneously therefore replicating circumstances from clinical settings. Further evaluation in other populations of adults with intellectual disability is required.
In a study of consecutive referrals to a specialist intellectual disability psychiatric clinic in Germany, DiBAS-R sensitivity was 82% and specificity 67%. Diagnostic accuracy was better in adults with mild/moderate intellectual disability than those with severe intellectual disability (for whom specificity decreased to 34%; Heinrich et al., 2017). A strength of the study was that the DiBAS-R was completed by carers, prior to a full diagnostic assessment, and was therefore representative of the clinical process.
One study used a combination of the DiBAS-R and the Autism Checklist (ACL) and is described below (Mutsaerts et al., 2016).
Autism Checklist (ACL)
In a psychiatric clinic for adults with intellectual disability, Mutsaerts et al. (2016) reported that combined use of the ACL and the DiBAS-R led to improved sensitivity of 95% (when there was a positive screen on at least one measure) compared to when each measure was used alone (91%/75%, respectively; Sipes and Matson, 2014). Combined use also led to an increase in specificity to 88% (when there were positive screens on both measures) compared to using each measure separately (75%; Mutsaerts et al., 2016). The inclusion of data collected from people referred to clinic was a study strength.
Diagnostic Measures (DMs) and observational assessments
Findings from studies of DMs and observational assessments are shown in Table 5.
Findings from studies evaluating diagnostic measures and observational assessments.
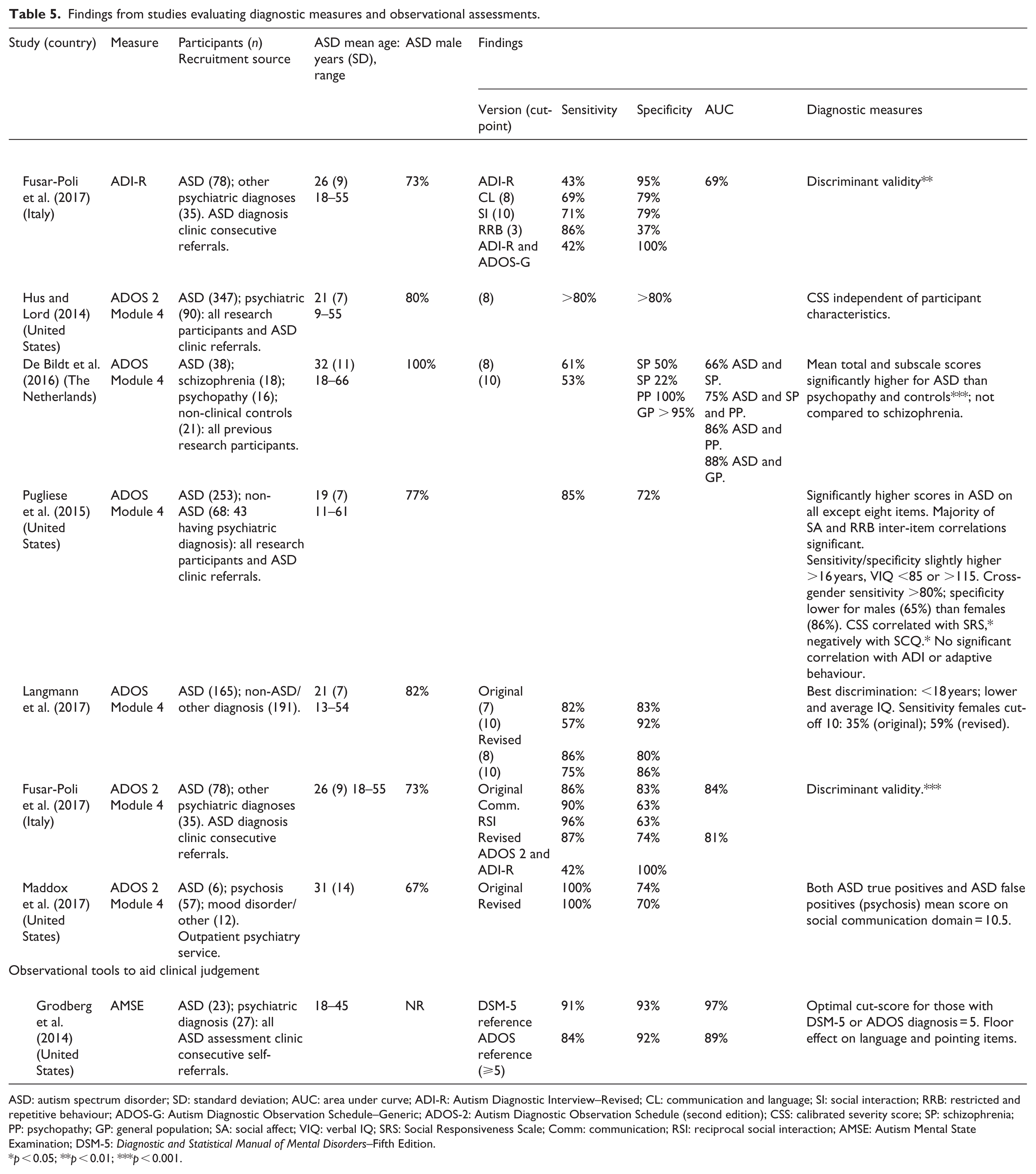
ASD: autism spectrum disorder; SD: standard deviation; AUC: area under curve; ADI-R: Autism Diagnostic Interview–Revised; CL: communication and language; SI: social interaction; RRB: restricted and repetitive behaviour; ADOS-G: Autism Diagnostic Observation Schedule–Generic; ADOS-2: Autism Diagnostic Observation Schedule (second edition); CSS: calibrated severity score; SP: schizophrenia; PP: psychopathy; GP: general population; SA: social affect; VIQ: verbal IQ; SRS: Social Responsiveness Scale; Comm: communication; RSI: reciprocal social interaction; AMSE: Autism Mental State Examination; DSM-5: Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition.
p < 0.05; **p < 0.01; ***p < 0.001.
Diagnostic Measures (DMs): interviews
Autism Diagnostic Interview-Revised (ADI-R)
The ADI-R was evaluated with adults without intellectual disability who were consecutively referred (mostly by self or a relative) to an ASD diagnosis clinic in Italy (Fusar-Poli et al., 2017; Lord et al., 1994). Overall, the ADI-R had low sensitivity (43%) but good specificity (95%). In contrast, across the subscale domains sensitivity was acceptable (more than 60%) and specificity was good (more than 79%), with the exception of the restricted, repetitive and stereotyped behaviours domain (just 37%).
When the ADI-R and ADOS-G were combined, sensitivity was still low (42%). The authors noted that the ADI-R may work less well with higher-functioning adults because a significant number of items rely on developmental history, and so more subtle presentations later in life may be missed (Fusar-Poli et al., 2017). It was a strength of the study that those administering the ADI-R were blind to DSM-5-based clinical consensus and that a third of participants already had a psychiatric diagnosis.
Diagnostic Measures (DMs): observational
Autism Diagnostic Observation Schedule (second edition) Module 4 revised algorithm
Hus and Lord (2014) reported sensitivity and specificity of the new revised Module 4 algorithm to be above 80% in a study including previous research participants and individuals presenting to a developmental disabilities clinic (the control group comprised individuals with a variety of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; text rev.; DSM-IV-TR disorders (Lord et al., 1999, 2012). The severity scores were mostly independent of verbal IQ and race. A limitation of the study was the retrospective design, and exclusion of some individuals with a relative with ASD, so these new algorithms do require replication in other groups.
In a Dutch study of individuals with ASD and three different control groups, De Bildt et al. (2016) reported a sensitivity of 61% for the ADOS Module 4. However, specificity varied according to the comparator group: 95%–100% for individuals recruited from non-clinical or forensic settings, compared to 22%–50% for individuals with schizophrenia (De Bildt et al., 2016). Items that were endorsed by the ASD group but not by individuals with schizophrenia included ‘quality of rapport’, ‘conversation’, ‘quality of social responses’ and ‘highly specific topics’. Limitations in the study design included the small sample size and the use of archival video data with individuals being diagnosed prior to the study.
In the third study, Pugliese et al. (2015) investigated individuals referred for an ASD assessment and previous research participants (many of whom met criteria for a range of diagnoses) using the Autism Diagnostic Observation Schedule (second edition) (ADOS-2) Module 4 and a cut-point of 8. The study found that while sensitivity was 85% (80%–89% across research sites), specificity was somewhat lower at 72% (62%–91%). The results were best for women and those with above or below average verbal IQ. Limitations in the study design included variability in the reference standards used to confirm a diagnosis of ASD and omission of any description of blinding during administration of the tests.
Langmann et al. (2017) investigated the performance of the original and revised ADOS-2 Module 4 algorithms using retrospective data. Participants were adults and adolescents with suspected ASD who had been referred to specialist ASD diagnostic clinics in psychiatry services. The revised algorithm demonstrated slightly better performance overall (sensitivity 86% and specificity 80% at cut-point 8) compared to the original algorithm. However, specificity for adults with a diagnosis of personality disorder compared to ASD was poor (individuals with personality disorder comprised 58% of false-positive cases). In addition, diagnostic accuracy was less for women and older individuals. However, a possible limitation to the generalisability of these findings was that less than a quarter of those recruited were female and only 25% were over age 24 years.
Fusar-Poli et al. (2017) evaluated the ADOS-2 Module 4 with adults whose IQ was more than 70 and who were consecutively referred to an ASD diagnosis clinic in Italy. The majority of participants were self or relative referrals. The original ADOS-2 Module 4 algorithm (Lord et al., 2012) had sensitivity of more than 86% across all domains. Sensitivity of the revised algorithm (Hus and Lord, 2014) was 87%. Specificity was 83% for the original algorithm but reduced on individual domains (63%) and was 74% on the revised algorithm. Strengths of the study included the avoidance of a case–control design, and that those administering the ADOS-2 were blind to DSM-5-based clinical consensus. In addition, and as would be expected in a clinical setting, a proportion of those recruited had existing psychiatric diagnoses (37%).
Maddox et al. (2017) found the original and revised algorithms for the ADOS-2 Module 4 (Hus and Lord, 2014; Lord et al., 2012) had a sensitivity of 100%, while specificity was 74% and 70%, respectively. A strength of the study was recruitment of participants from psychiatric settings; however, study findings indicated a high number of participants with psychosis falsely met criteria for ASD and that the social-communication domain was particularly limited in discriminating between the two.
Short observational assessments
Autism Mental State Examination
The Autism Mental State Examination (AMSE) was reported to have good sensitivity and specificity for discriminating ASD from other disorders using the ADOS-G or the ADI-R (Grodberg et al., 2012, 2014). Strengths of the study design included blinded administration of the measure and the consecutive recruitment of individuals who self-referred for assessment of ASD.
Discussion
Key findings
The two key findings of the review are that overall, there is very limited evidence to support the use of SQs (self-report or informant completed brief measures developed to screen for ASD) in the assessment and diagnosis of ASD in adults. Furthermore, the evidence regarding the use of DMs (more in-depth assessment tools involving semi-structured interviews and interactive tasks) suggests some utility in identifying ASD among clinic referrals, although specificity for eventual diagnosis of ASD was still relatively low. For both types of assessment tools, more evidence is required regarding their use in diagnostic assessments. We consider that tools are useful, but only as an aid to diagnostic decision-making within a broader multidisciplinary team ASD assessment. These conclusions are in keeping with the NICE (2014) guidelines that suggest using a battery of tools to support the diagnostic process.
Structured Questionnaires (SQs)
The new information reported compliments the overall NICE (2014) recommendations regarding SQs. Most SQs show limited utility in identifying those who did not have ASD (Ashwood et al., 2016). This finding was evident in studies recruiting participants in clinically realistic settings (e.g. Ashwood et al., 2016) compared to studies using a case–control design with a general population comparator (e.g. Booth et al., 2013). There were particular problems differentiating ASD from schizophrenia, which may be in part a consequence of the potential overlap in symptoms (e.g. flattened affect and aspects of social communication) and/or underlying genetic phenotype (Cross-Disorder Group of the Psychiatric Genomics, 2013). Given the low specificity, the AQ and the RAADS-R should not in our opinion be used on their own for screening and case recognition in clinical settings. Based on published data, this would apply to all versions of the AQ including the abbreviated 10-item version recommended by NICE (2014). Regarding the SRS, at the time of the NICE (2014) recommendations there were no diagnostic accuracy studies that met guideline inclusion criteria. New evidence suggests that the accuracy of the SRS (Japanese translation) for adults may be limited in women, and in the presence of symptoms of psychoticism or distress as measured using screening tools (Nishiyama et al., 2014; Takei et al., 2014). Evidence for the diagnostic accuracy of the SCQ with adults was not available previously. In this review, the SCQ was found to be more effective when using a higher cut-off score in a German cohort (Sappok et al., 2015a). However, when an international cohort was recruited (Germany, United States and the United Kingdom), a lower cut-score improved diagnostic accuracy (Sappok et al., 2017). Where professional carers completed the current SCQ (without reference to developmental history) for adults with intellectual disability in a clinical setting, this showed better sensitivity and specificity than the lifetime version (Sappok et al., 2015a). This highlights the potential difficulty of gathering a developmental history to support the diagnosis of ASD in adults, which has implications for the choice of diagnostic tools used. A new and shortened version (the SCQ-AID) used in an international study had good sensitivity but low specificity; however, the authors note some variation in diagnostic rates and processes across countries (Derks et al., 2017). This review found no new evidence regarding the Asperger Syndrome Diagnostic Interview (ASDI) or the Adult Asperger Assessment (AAA).
Diagnostic Measures (DMs)
Studies assessing the psychometric properties of DMs (such as the ADOS-2 Module 4) reported some success identifying ASD among clinic referrals though limitations remained. The ADOS-G and ADI were recommended by NICE for use with adults with and without intellectual disability. New evidence shows that the new ADOS-G algorithms had good sensitivity and specificity in a study with a case–control design (Hus and Lord, 2014). This was to a certain extent replicated (specificity was acceptable) in individuals consecutively referred to a psychiatric clinic with a variety of diagnoses (Fusar-Poli et al., 2017). However, new studies also indicated that in clinical groups, specificity was reduced for schizophrenia, personality disorder and psychosis (De Bildt et al., 2016; Langmann et al., 2017; Maddox et al., 2017). Scores were additionally found to interact with gender and IQ although further studies are required to replicate these findings before definite conclusions can be made (Langmann et al., 2017; Pugliese et al., 2015). The ADI-R demonstrated mixed results in adult ASD clinic referrals, having good specificity but low sensitivity (Fusar-Poli et al., 2017). The AMSE showed promising evidence as a new measure; further studies in other settings and by teams independent of the authors are required (Grodberg et al., 2014).
Combinations of tools
NICE (2014) recommended using a battery of tools to support the diagnostic process. This was based on evidence from studies using SQs and DMs in isolation, and at the time the guidelines were published there were no diagnostic accuracy studies regarding use of tools in combination. In this review, only two studies evaluated the use of a combination of tools. In adults with ASD and intellectual disability, using the ACL and the DiBAS-R improved the sensitivity and specificity of these tools (Mutsaerts et al., 2016). For adults without an intellectual disability, combining the ADI-R and the ADOS-G improved specificity but reduced sensitivity (Fusar-Poli et al., 2017). Sensitivity of the combined measures was lower than to using the ADOS-G alone; the authors suggest that the ADI-R may be less sensitive to the more subtle presentation of ASDs diagnosed in adulthood (Fusar-Poli et al., 2017). This new evidence whereby combined use of these measures improved diagnostic effectiveness is in accordance with NICE (2014) recommendations regarding a battery of measures (Mutsaerts et al., 2016).
Strengths and limitations of the review
A strength of this review is that it includes new evidence about measures for which at the time of the NICE (2014) review publication there was no or limited evidence available (the SCQ, DiBAS-R, ACL, SRS and the AMSE). A further strength was that only studies reporting sensitivity and specificity, or receiver operating characteristics (ROC) analysis were included. A limitation was that the number of studies and the sample sizes reported were relatively small, and heterogeneity in the design of studies was considerable. In addition, case–control design was highlighted as a potential source of bias for the existing evidence on tools when the NICE (2014) guidelines were published; this design limitation was also present in a number of the studies included in this review. However, the studies reported here that used more ecologically valid designs (e.g. consecutive clinic referrals) also reported poor psychometric properties of most measures, particularly around specificity.
Implications
The diagnosis of ASD during adulthood is likely to pose challenges to clinicians and researchers as people’s presentation may be more subtle (Brugha et al., 2015; Rogers et al., 2015). The presence of other mental health conditions, which is highly likely in individuals presenting to a specialist mental health service, challenges the accuracy of case recognition of ASD and complicates the ability of clinicians and researchers to identify the core symptoms of ASD (Underwood et al., 2015). The risk of diagnostic overshadowing (i.e. misattributing behaviours to an existing diagnosis leading to a failure in identifying other diagnoses) as a consequence of the presence of associated psychiatric disorders may be increased (Cross-Disorder Group of the Psychiatric Genomics Consortium, 2013; Ford and Crewther, 2014). For many seeking a diagnostic assessment for suspected ASD in adulthood, the likely scenario will be an assessment in the context of co-occurring mental health needs, additional neurodevelopmental difficulties, social/relationship difficulties and/or problems with employment or education (NICE, 2012; Russell et al., 2016). This review highlights the limitations of the psychometric properties of existing diagnostic tools (SQs and DMs) to aid the accuracy of diagnostic practice, in adults particularly in the presence of co-occurring mental health diagnoses. The use of SQs that do not require a trained assessor may be useful particularly in community primary and secondary healthcare settings (e.g. general practitioners (GPs) and mental health services), to gather information about a possible neurodevelopmental disability (Allison et al., 2012; Booth et al., 2013). However, as already described, SQs alone should not be used to exclude further ASD assessment other than if the scores are extremely low (Brugha et al., 2012).
The studies included highlight that performance of SQs and DMs depends on the circumstances (countries, cultures and clinical setting) in which they are used and evaluated. For example, using ASD measures to identify individuals with ASD within the general population is a very different task to using the same measures in mental health and intellectual disability services, where ASD prevalence would be expected to be higher (Brugha et al., 2016). The interpretation of data derived from SQs and DMs including the values for sensitivity and specificity will be affected by both the prevalence of ASD in particular populations and the presence of co-existing conditions including intellectual disability and mental health conditions (Campbell et al., 2015; Leeflang et al., 2009). In addition, deciding how best to interpret the significance of particular SQ and DM scores is not without problems given the possibility that there may be cultural and/or country differences in scores (Sappok et al., 2015a, 2017) in addition to the existing reported different clinical and research cut-off scores for many measures (Pugliese et al., 2015). Sappok et al. (2017) note that variations regarding the SCQ scores across countries may relate to differences in measure administration practices, ASD reference standards and referral processes. This has implications for international multi-site studies when researchers should agree cut-offs in advance (Sappok et al., 2017).
An inclusion criterion for the review was that study participants had completed an SQ or DM as part of a comprehensive ASD diagnostic assessment. However, in some studies, participants were diagnosed prior to the study and in others participants were consecutive new referrals to a diagnostic clinic. Where participants were diagnosed prior to the study, it was not always clear whether the ASD diagnosis was made in childhood or adulthood. This is important for several reasons: first, the presentation of adults diagnosed in childhood may be different to that of people referred for a first diagnosis in adulthood. Second, selecting adults with an existing diagnosis for studies of SQs and DM rather than adults referred for a suspected diagnosis may influence the sensitivity and specificity values (Campbell et al., 2015; Leeflang et al., 2009). Therefore, the findings from studies in which individuals were first time referrals for an ASD assessment might arguably have more validity for real-life clinical settings.
Future research
Further research is needed to investigate the accuracy, efficiency and comparative utility of all the tools identified in this review. Tools may require modification for use in adult ASD diagnosis services with individuals with or without intellectual disability whose neurodevelopmental conditions were not recognised in childhood, and for whom the risk of additional mental health comorbidities is high. Research should compare the sensitivity and specificity between tools when appropriately used in the diagnostic pathway with ecologically valid populations, such as individuals presenting to adult mental health settings. Only then can the clinical utility of individual SQs and DMs be directly compared. The strongest tools can then be developed further as needed – and others redeveloped, or discarded. New tools that have robust psychometric properties and that have been constructed specifically for use in adult diagnostic health services may be more useful than those adapted from childhood measures. In addition, clinicians and researchers should examine the utility of the combined use of measures to aid the assessment, differential diagnosis of ASD and recognition of co-occurring neurodevelopmental and mental health conditions in the context of an overall clinical formulation. An important next step will be investigating consensus views of adults with ASD and clinicians in different clinical contexts on the most effective, efficient and acceptable combinations of DMs. Whether SQs and DMs are sensitive to clinical change in response to interventions and/or progress over time is an area for future research (Bolte and Diehl, 2013; Brugha et al., 2015), as is the impact of gender and also culture on the psychometric properties of SQs and DMs – particularly as international collaborations are increasingly used to gather data from different settings (Pinto et al., 2014).
Regarding specific measures, no studies published since 2014 were found to have evaluated the ADOS Modules 1–3 for adults with intellectual disability. No studies investigating the psychometric properties of the DISCO (Leekam et al., 2002; Wing et al., 2002) or peer-reviewed publications evaluating the 3DI (Santosh et al., 2009; Skuse et al., 2004) were identified that met the inclusion criteria for this review. Research on the clinical utility of these DMs that are used in a number of UK and European clinical settings is required.
This review did not include any existing interview measures of the more subtle presentation of the broader autism phenotype (BAP) (Parr et al., 2015). Given the possibility that presentations of ASD in adulthood may be more subtle, the potential value of interviews originally designed to identify the BAP for use as ASD diagnostic tools needs to be explored.
In conclusion, the findings of this review compliment the NICE (2014) guidelines’ recommendations on the use of SQs and DMs in combination rather than in isolation. This review suggests that SQs have limitations when used alone as screening measures and are unlikely to be reliable indicators of who should go on to have a full ASD diagnostic assessment. Future studies should examine the combined use of SQs alongside DMs for case recognition within the multidisciplinary diagnostic assessment in order to identify the most efficient and effective (clinical and cost) ways to ‘streamline’ diagnostic practice and intervention planning in different settings for adults with suspected ASD. Research should also focus on which SQs and DMs both separately and in combination might be most appropriate for particular client groups – for example those with co-existing mental health conditions and those with intellectual disability.
Supplemental Material
AUT748245_Lay_Abstract – Supplemental material for Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review
Supplemental material, AUT748245_Lay_Abstract for Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review by Sarah Wigham, Jacqui Rodgers, Tom Berney, Ann Le Couteur, Barry Ingham and Jeremy R Parr in Autism
Supplemental Material
AUT748245_Supplementary_Material_PRISMA_2009_Checklist – Supplemental material for Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review
Supplemental material, AUT748245_Supplementary_Material_PRISMA_2009_Checklist for Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review by Sarah Wigham, Jacqui Rodgers, Tom Berney, Ann Le Couteur, Barry Ingham and Jeremy R Parr in Autism
Supplemental Material
AUT748245_Supplementary_Table_DS1 – Supplemental material for Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review
Supplemental material, AUT748245_Supplementary_Table_DS1 for Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review by Sarah Wigham, Jacqui Rodgers, Tom Berney, Ann Le Couteur, Barry Ingham and Jeremy R Parr in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the UK autism research charity Autistica (![]() ) for funding this study as part of the Autism Life Course and Ageing research programme. In addition, the authors are grateful to Northumberland Tyne and Wear NHS Foundation Trust for sponsoring the research and for Research Capability Funding.
) for funding this study as part of the Autism Life Course and Ageing research programme. In addition, the authors are grateful to Northumberland Tyne and Wear NHS Foundation Trust for sponsoring the research and for Research Capability Funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.