
Abstract
As prevalence of autism spectrum disorder continues to increase, so too does the need for timely, accessible diagnostic consultation. The present work extends from a previous study which provided preliminary evidence for the feasibility of expert clinicians to utilize telemedicine to triage autism spectrum disorder risk in young children. However, it did not examine whether a telediagnostic model had a demonstrable impact on tertiary care center referrals and usage. We therefore examined whether the introduction of telemedicine-based diagnostic consultation for families served by a rural medical facility affected referrals overall as well as to a metropolitan tertiary care diagnostic center. Results suggest that telemedicine diagnostic consultation in partnership with a referring early intervention system may positively impact referrals for diagnostic evaluation as well as the ability of families to schedule and attend appointments.
Introduction
As prevalence of autism spectrum disorder (ASD) increases, so too does the need for timely, accessible diagnostic consultation. With a prevalence of 1 in 59 (Baio et al., 2018), demand for diagnostic expertise has grown exponentially, with ongoing disparities regarding geographic, socioeconomic, and racial/ethnic factors (Christensen et al., 2016; Durkin et al., 2010; Fountain et al., 2011; Liptak et al., 2008; Zuckerman et al., 2013). Clinic waitlists can be extensive; families may see multiple professionals before receiving a diagnosis (Christensen et al., 2016; Hyman and Johnson, 2012; Wiggins et al., 2006). This leaves thousands of families waiting for answers who, in the interim, may lack access to crucial early intervention for their children (Pierce et al., 2011; Stahmer and Mandell, 2007).
In recent work, we partnered with the Tennessee Department of Education’s Part C system (a statewide early intervention program for children 0–36 months) to develop and implement a telemedicine-based ASD diagnostic consultation service in a rural region of the state (Juárez et al., 2018). Although it offered preliminary evidence of diagnostic accuracy as well as family satisfaction, the larger aim of this work is to shift outcomes on a systems level. Understanding how systems of care respond to telemedicine implementation is crucial to determining its generalizability, sustainability, and impact.
The present study investigates whether the introduction of a telemedicine-based diagnostic consultation service (“telemedicine service”) impacts systems of care by affecting referrals to a metropolitan tertiary care diagnostic center (“tertiary center”) for families served by a rural medical facility. To examine this question, (1) referrals from the rural target region to the tertiary center were examined before and after the introduction of the telemedicine service; and (2) referrals from the targeted rural region were compared to a comparable rural region without the telemedicine service.
Methods
Participating systems and families
Participating families were served at a rural medical facility approximately 130 miles from the tertiary center where the remote assessor was located. Families were recruited from a target region of 23 counties immediately west of the tertiary center’s home region. This region was selected based on its identification as “under resourced” by the state Department of Education as well as its number of referrals to the tertiary center. According to the most recent US Census estimates, the mean population of represented counties was 34,408; median household income, $40,541.20 (range: 29,893–55,972), and percentage of persons living in poverty was 20.25 (range: 16–42.7) (Juárez et al., 2018).
For comparison, we analyzed patterns of tertiary center referral rates from a second rural region of the state with Part C support. The comparison region (17 counties) is immediately east of the tertiary center. It was selected based on its comparable distance, history of referrals, and demographic similarities.
Identification of appropriate referrals
In contrast to a comprehensive evaluation model (i.e. Autism Diagnostic Observation Schedule-Second Edition (Lord et al., 2012), cognitive assessment, adaptive skill interview), the telemedicine service relies on a singular assessment and a caregiver interview regarding developmental history and Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) diagnostic criteria. As such, the evaluating team worked with referring providers to identify children and families most likely to be served well by this model. Referred families were enrolled in the state Part C system, whose service coordinators identified children showing ASD characteristics based upon parental report and/or direct observation.
Because ASD presentation in young children varies and early intervention providers have inconsistent expertise, a standardized pre-screening decision tree was developed for determining the appropriateness of the telemedicine service for families, and distributed among referring service coordinators. It included the following description:
The program is designed to help rapidly and accurately identify ASD (or clearly rule-out ASD) when this is a clear and pressing issue for families. The program is not intended to replace more in-depth assessments for families where complex issues require more substantial evaluation over time.
Guidelines were provided (Figure 1) for determining appropriate referral routes. Exclusion criteria necessitating referral for comprehensive evaluation at the tertiary center included complicating medical conditions (e.g. prenatal substance exposure), psychosocial factors (e.g. history of abuse), significant sensory impairment, or limited English proficiency. All referrals were then reviewed by the in-person assessor for appropriateness.
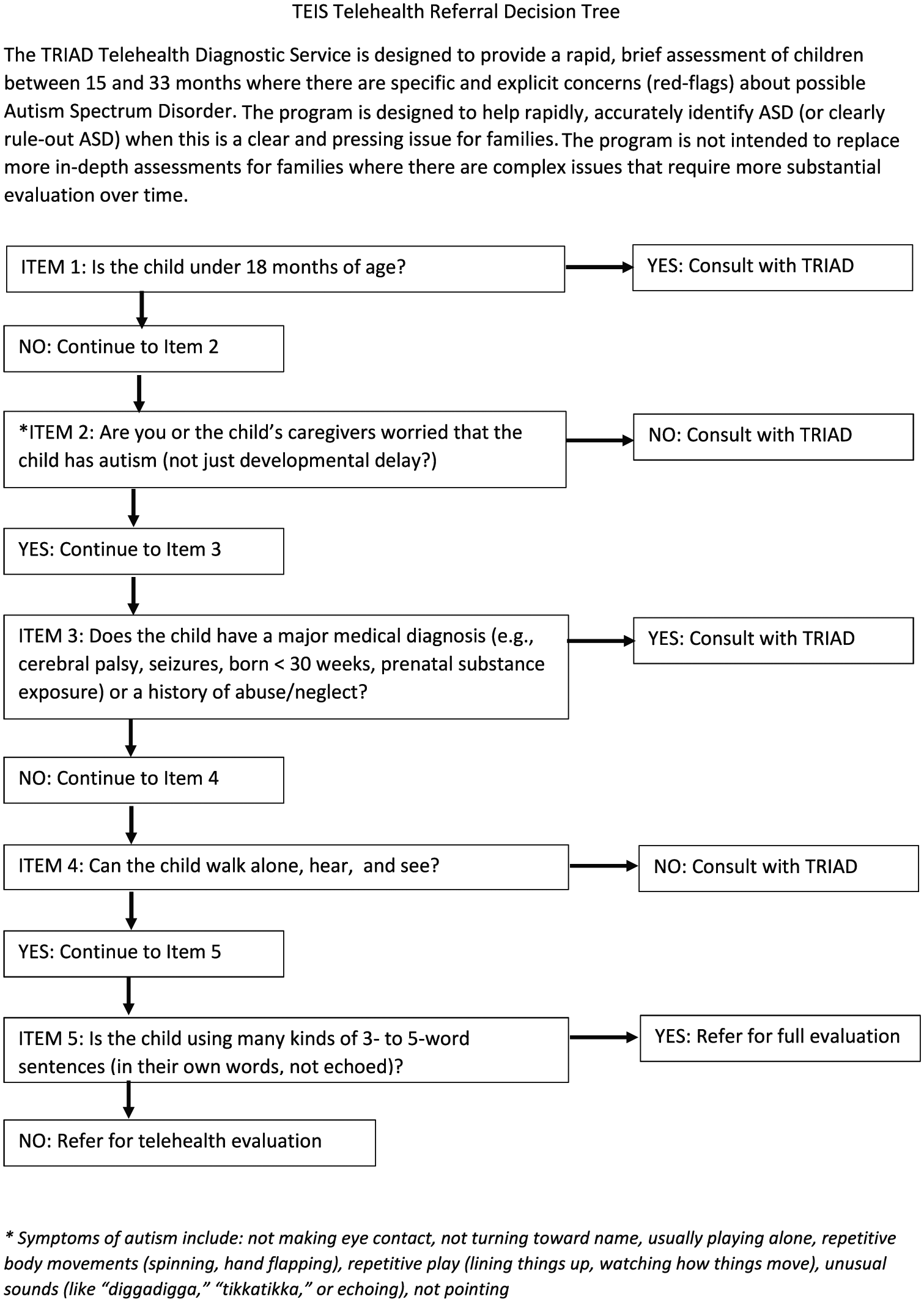
Telemedicine referral decision tree.
We established regular meetings with the Part C system as part of an iterative program evaluation procedure to maintain ongoing communication about how this decision-making process functioned. This included discussing case examples of appropriate referrals as well as referrals of families not adequately served by this abbreviated model. This formalized check-in procedure between referring providers, in-person testers, and remote assessors was critical in assuring the telemedicine service was useful and positive for these rural families, for whom the Part C system was their first and primary point of continued contact.
Overview of the telemedicine diagnostic consultation model
At the rural medical facility, visits were conducted in an exam room outfitted with Health Insurance Portability and Accountability Act (HIPAA) compliant technology. In-person testers had college degrees in child development, experience working with families in homes, and training on the Screening Tool for Autism in Toddlers & Young Children (STAT, Stone et al., 2000). The STAT, a Level 2 ASD screener for use with children ages 24–36 months, was selected because it is well-validated and easily implemented in community settings (Stone et al., 2004). The remote assessor, a licensed clinical psychologist with extensive ASD expertise, observed and interviewed caregivers. At the conclusion of the 60-minute appointment, the remote assessor discussed diagnostic impressions with the family, which included making an ASD diagnosis, ruling ASD out, or recommending further evaluation (Juárez et al., 2018).
Results
Impact of the telemedicine diagnostic consultation on regional referrals
From 2012 to 2016, the target region referred an average of 33.2 children per year (2.76 per month) to the tertiary center. After telemedicine services started in August 2016, the average total referral rate for 2016 (tertiary center, 38 + 5 months of telemedicine service, 20) rose to 4.8 per month (see Figure 2). This represents a 56.76% total increase in referrals for evaluations from 2015 (tertiary center only, 37) to 2016 (tertiary center + 5 months of telemedicine service, total of 58), and an 81.25% increase over the average of referrals made over the previous four years, 2012–2015 (average of 32).
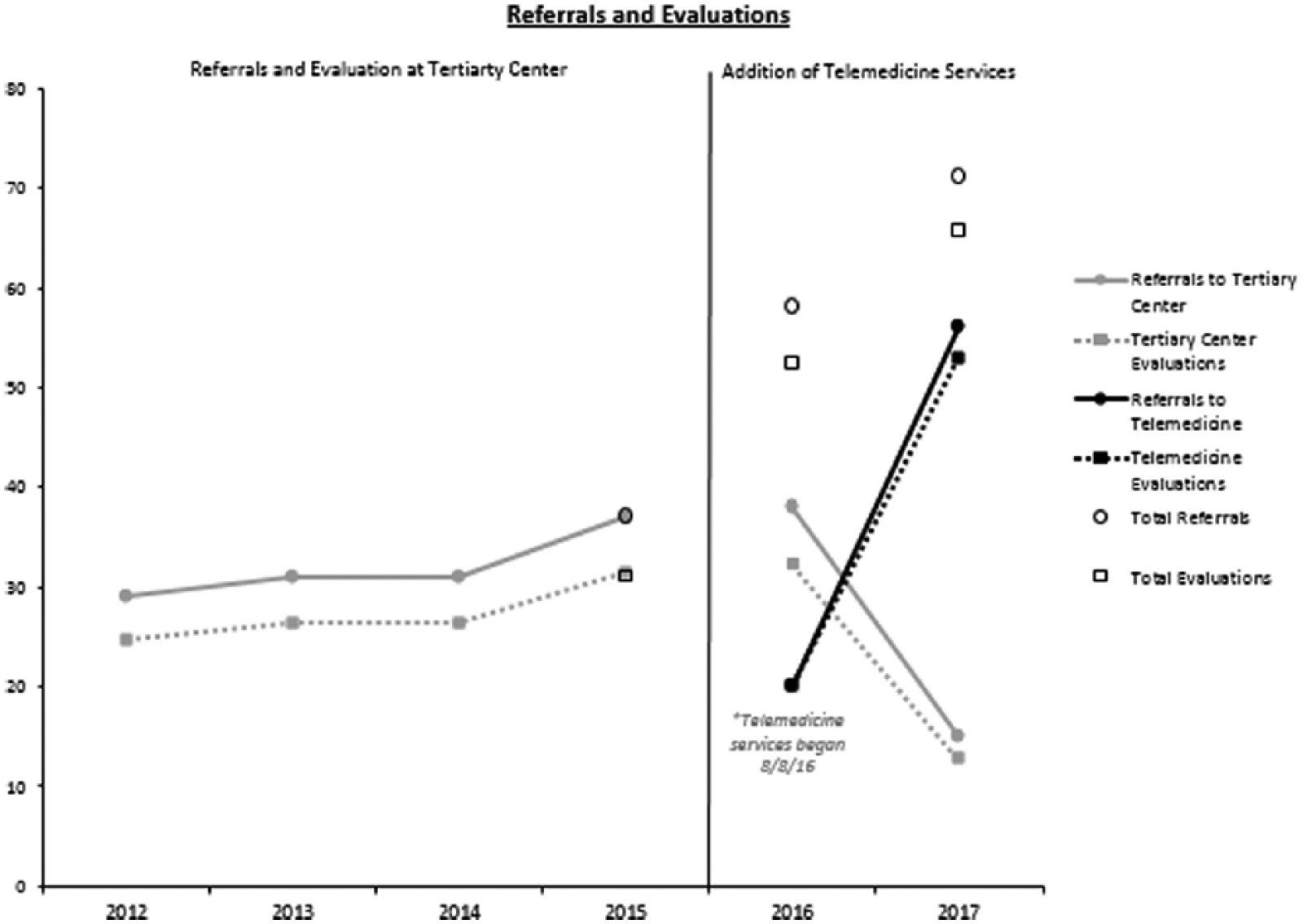
Target region referrals and evaluations.
We next compared referral rates across the first full telemedicine year (2017) to the last full year without telemedicine (2015). As seen in Figure 2, in 2017, the Part C system made 69 referrals for any type of evaluation, representing an 89.19% increase over 2015. Fifty-six of these referrals were for telemedicine evaluations; 13 were for the tertiary center, representing a 64.86% decrease in referrals for tertiary center evaluation. Of the 12 families then completing tertiary evaluations, 7 chose to do so rather than accessing telemedicine services, an option offered to every participating family. The remaining five children were medically complex, which made telemedicine services less appropriate. Information on the child who did not complete any evaluation was not available.
Importantly, the telemedicine service sped access to diagnostic consultation relative to waits at the tertiary center. In 2017, the statewide early intervention system referred 323 children under the age of 3 years for comprehensive evaluation, resulting in a 15-month wait time by January 2018. In contrast, families waited an average of 11.01 weeks for telemedicine visits from time of intake to time of evaluation (standard deviation (SD) = 8.83). This wait time has slowly increased (August-December 2016: mean = 8.17 weeks; August-December 2017: mean = 15.03 weeks) but still remains far below that of the tertiary center to which children would otherwise have been referred. Families are also keeping more appointments. Show rates from the target region to the tertiary center were 85% from 2012–2016; show rates for the telemedicine service were 100% in 2016 and 94.64% in 2017. Of families referred to the tertiary center rather than the telemedicine service in 2017, the show rate was 92.30%.
Comparison across rural geographies with versus without telemedicine service access
To determine whether differences in referral rates were attributable to telemedicine services versus statewide changes in Part C referral patterns, we compared the number of referrals from the target region with the number of referrals from the comparison region. From 2015–2017, referrals to the tertiary center from the target region decreased by 64.86% (from 37 to 13), whereas referrals from the comparison region increased by 114.71% (from 34 to 73).
Discussion
Our preliminary work provided convincing data on the accuracy and feasibility of a telemedicine diagnostic consultation model. However, we had yet to examine whether implementing this type of care model actually affected service system outcomes, including families’ abilities to access recommended care.
Results suggest implementing a telemedicine diagnostic consultation service for ASD in partnership with the early intervention system may positively impact referrals for diagnostic evaluation as well as the ability of families to schedule and attend appointments. We examined the impact of the telemedicine service on both families and systems. Most potentially participating families (56 out of 63) opted for this type of visit over travel to the tertiary center, with referrals to that center becoming more focused on children with diagnostic complexity or family preference. At a system level, a collaborative process of communication between diagnostic and early intervention teams allowed for more targeted screening of children and facilitated faster access to expert consultation, making a difference of up to a year in the time between referral and consultation with an expert in ASD. In turn, children from eligible regions referred by early intervention service coordinators to the tertiary center presented with added layers of potential diagnostic complexity (or, just as importantly, family preference) necessitating wait time and potential financial hardship of the travel.
There are a number of potential hypotheses for the increase in referrals and show rates. Data from caregivers and providers (Juárez et al., 2018) suggest the addition of telemedicine services facilitated access for families who would not have otherwise been referred due to the financial resources and time required for traveling to the tertiary center. Given the geography of the state, families in the target region could travel a minimum of 140-miles or as much as 400-miles roundtrip to access the tertiary center. As such, 12.50% of families receiving telemedicine services reported they would not have made the trip. We also discovered families referred by Part C providers to the tertiary center presented with diagnostic, developmental, or family preference factors, which reinforced the need for time, expense, and travel involved in this type of evaluation. Importantly, no family completing a telemedicine evaluation was denied further follow-up testing if they expressed a preference for such (Juárez et al., 2018). This service was not designed to impede access to care, rather to facilitate rapid, timely diagnostic triage to meet family and child needs within their community.
The telemedicine service described in this article was funded by the Tennessee Department of Education. Although not developed as a billable model, it could potentially facilitate insurance and private pay billing. Financial reimbursement of telemedicine services from insurance companies has been reported across a variety of medical and psychiatric fields (Antoniotti et al., 2014). Translating the telemedicine service into a billable model would further ease access to early identification by reducing geographic and financial barriers.
A primary challenge of the telemedicine service is localization. While technology, protocol, and validation of the model support replication across other regions, initiation of the service requires identification of ideal partner sites to accommodate the technology as well as in-person testers. These partners have personnel on-site with knowledge of child development and ASD assessments who facilitate discussions with families regarding results and next steps (i.e. local early intervention resource agencies or pediatric medical centers/clinics), and are located in facilities already providing pediatric services to simplify access and scheduling for families. An additional barrier to replication of this model is financial support. However, as telemedicine becomes increasingly commonplace and insurance companies begin to provide reliable reimbursement for behavioral services, this should become less of a barrier.
Supplemental Material
AUT787797_Lay_Abstract – Supplemental material for Measuring the service system impact of a novel telediagnostic service program for young children with autism spectrum disorder
Supplemental material, AUT787797_Lay_Abstract for Measuring the service system impact of a novel telediagnostic service program for young children with autism spectrum disorder by J Alacia Stainbrook, Amy S Weitlauf, A Pablo Juárez, Julie Lounds Taylor, Jeffrey Hine, Neill Broderick, Amy Nicholson and Zachary Warren in Autism
Footnotes
Acknowledgements
J.A.S., A.W. and A.P.J. conceived of the study and crafted the experimental design. A.P.J. and A.S. provided oversight of study implementation across Vanderbilt sites. A.W., N.B., A.N., J.H., and J.A.S. helped design and implement the rapid diagnostic procedure and methods for capturing diagnostic agreement. A.P. and J.A.S. assisted with data collection and analysis for manuscript preparation. J.A.S., A.W., and A.P.J. significantly participated in drafting the article, revising it critically, and providing final approval of the manuscript. All authors are in agreement with accountability for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.