
Abstract
The present study examined how stress reactions after traumatic events influence subjective well-being (SWB) via the indirect effect of posttraumatic growth (PTG) in two samples of Palestinian professional helpers from the Gaza Strip and West Bank (n = 201). Using the General Health Questionnaire (GHQ-12) as a dependent measure of well-being, and PTGI-10, PANAS-20, WHO-5 BREF, and IES-13 questionnaires as independent variables, structural equation modelling (SEM) was used to examine whether: (a) cumulative trauma was negatively and directly related to subjective well-being; (b) levels of trauma were positively and directly related to posttraumatic growth; and (c) PTG was positively and directly related to subjective well-being. The findings suggest that posttraumatic growth contributes to mitigating and buffering (on the order of approximately 10%) the effect of trauma on subjective well-being. PTG seems to be a resource that can help aid workers deal with the consequences of stressful life events. Clinical implications and directions for supervision and training are discussed.
Introduction
Professional health workers (e.g., social workers, helpers, practitioners) operating in war-like conditions are an occupational group at risk of experiencing feelings of stress, exhaustion, and burnout due to their direct and indirect involvement in traumatic events (Gilbar, 1998; Veronese & Pepe, 2014). Indeed, health professionals working with traumatized populations in war-like environments display higher levels of vicarious traumatization and compassion fatigue than other professionals (Al-Krenawi, Graham, Dean, & Eltaiba, 2004; Baum, 2016; McCann & Pearlman, 1990; Nimmo & Huggard, 2013; Ray, Wong, White, & Heaslip, 2013). In relation to Palestinian aid workers specifically, this group has faced increased levels of poverty and unemployment since the beginning of the second intifada in 2000 (Blome & Safadi, 2015; Veronese, Pepe, & Afana, 2016; Veronese, Said, & Castiglioni, 2011). The barrier between Israel and the occupied Palestinian territories (OPT) of the West Bank and Gaza restricts the movement of Palestinians within and between these regions (Cohen et al., 2005; Giacaman et al., 2009; Vitullo et al., 2012). In the West Bank, ambulances and medical personnel are required to go through checkpoints on their way to health services, resulting in delays and increased travel costs. Many commuters report moderate levels of harassment by the Israeli army at the checkpoints and say that stressful working conditions impede their ability to provide health care effectively (Sousa & Hagopian, 2011). In such contexts, professional helpers are frequently impacted by a similar type of cumulative and continuous trauma to that found in their clients. An additional factor to be considered is the concept of shared traumatic reality or shared trauma (Dekel & Baum, 2009), which is characterized by a deep sense of loss and which can impair the effectiveness of emergency workers’ interventions during the exercise of their professional duties (Bauwens & Tosone, 2010).
These extremely challenging living conditions as well as a demanding workload represent risk factors for the development of symptoms such as anxiety and depression (Ager & Loughry, 2004). Further symptoms include short- and long-term mental health issues such as posttraumatic syndromes (de Jong, Komproe, & van Ommeren, 2003; Neria et al., 2010; Shiri, Wexler, Alkalay, Meiner, & Kreitler, 2008). The political situation in Palestine is one of the major risk factors for mental health distress among the population (Al-Krenawi, Lev-Wiesel, & Sehwail, 2007; Giacaman, 2004; Punamaki et al., 2008; Qouta, Punamaki, & El Sarraj, 2008). Specifically, the ongoing conditions of chronic uncertainty, military violence, unemployment, incarceration, and poverty are likely to increase stress and mental health problems (Giacaman, 2004; Punamaki et al., 2008; Salo, Punamaki, & Qouta, 2004). The health providers themselves report that, as a result of the occupation and military violence, they have already experienced considerable stress, which in turn affects their work (Lindsay, 2007; Shamia, Thabet, & Vostanis, 2015). The consequences of the military occupation have been one of the primary concerns driving the development of mental health care in Palestine, which is focused mainly on intervention aimed at reducing posttraumatic stress symptoms (PTSS) (for a critique see, e.g., Afana, 2012; Afana, Dalgard, Bjertness, Grunfeld, & Hauff, 2002; Giacaman et al., 2011). However, from a chronic stress perspective, in light of Palestinians’ ongoing exposure to war and political violence, it has been argued that mainstream diagnoses related to traumatic stress, such as PTSD and complex PTSD, are not applicable—or only marginally so—to the Palestinian context, in which trauma consists of continuous threat to life and human insecurity (Stevens, Eagle, Kaminer, & Higson-Smith, 2013). The main concern here is that “posttraumatic” constructs frame trauma exposure as temporally situated in the past, failing to adequately intercept the daily experiences of extreme trauma or realistic expectations of ongoing threat and danger of the Palestinian population (Afana, 2012; Afana, Pedersen, Rønsbo, & Kirmayer, 2010). The concept of continuous traumatic stress (CTS) fits better with the Palestinian experience of ongoing trauma and social suffering (Barber et al., 2014; Barron & Abdallah, 2015). CTS has been theorized in contexts of political violence and encompasses both the social and individual conditions affecting those who live in conflict-affected zones with low-intensity warfare (e.g., Kosovo and Sudan), in which the civil population lives under threat and is exposed to the constant violation of human rights (Straker, 2013).
Aid workers are particularly vulnerable to the risk of developing primary and vicarious trauma from working with victims of political violence (Cohen & Collens, 2013). However, despite the heavy psychological burden, a growing body of literature shows that positive personal change after traumatic exposure is possible for this group (Baum & Ramon, 2010; Paton, 2005). A recent study by Veronese and Pepe (2014) in the occupied Palestinian territories shows that aid workers often demonstrate high levels of sense of coherence and psychological resources when it comes to their ability to attribute meaning to and psychologically manage the traumatic events experienced. Similarly, Britt, Adler, and Bartone (2001) in a study on emergency professions reported that finding meaning in one’s work is a key prerequisite for benefitting from potentially traumatic experiences.
The literature on trauma shows that it is possible for traumatic events to trigger positive psychological change in individuals exposed to them (Calhoun & Tedeschi, 1989–1990; Taylor, 1983). Tedeschi and Calhoun (2004) were the first to introduce the concept of posttraumatic growth (PTG) to describe positive psychological change after highly challenging life circumstances. A body of literature provides evidence for psychological growth in a variety of populations such as children, adolescents, and adults who have been exposed to diverse kinds of traumatic events. PTG has been identified in adult civilians exposed to war (Kimhi, Eshel, Zysberg, Hantman, & Enosh, 2010), war veterans (Kaler, Erbes, Tedeschi, Arbisi, & Polusny, 2011; Pietrzak et al., 2010), former prisoners of war (S. Dekel, Ein-Dor, & Solomon, 2012; Erbes et al., 2005; Feder et al., 2008; Solomon & Dekel, 2007), and victims of interpersonal violence (Cobb, Tedeschi, Calhoun, & Cann, 2006; Kleim & Ehlers, 2009; Kunst, Winkel, & Bogaerts, 2010; Updegraff, 2005).
Both resilience and posttraumatic growth are salutogenic constructs associated with the aftermath of traumatic events, including war and violence (Helgeson, Reynolds, & Tomich, 2006). In the majority of cases, posttraumatic growth and resilience are treated as similar in the scientific literature (Tedeschi, Calhoun, & Cann, 2007). For instance, it has been debated whether or not resilience overlaps with the construct of growth, or whether growth is superior to resilience (Johnson et al., 2007; Lepore & Revenson, 2006; Tedeschi et al., 2007; Westphal & Bonanno, 2007).
In contrast, other authors have argued that is highly unlikely that resilient individuals will engage in the meaning-making behaviors associated with PTG, for the simple reason that they tend not to struggle to the same extent as other, more traumatized individuals (Westphal & Bonanno, 2007). Given that Palestinians in general are required to deal with severe social suffering and extreme cumulative trauma in a context of ongoing occupation and violence, we believe that aid workers are likely to be constantly engaged in psychological processes functional to attributing sense and coherence to these highly adverse conditions (Veronese & Pepe, 2017). It follows that their recovery is more likely to involve PTG than resilience (Shamia et al., 2015). This does not mean that we share the common but empirically unfounded assumption that PTG generates better outcomes than resilience. Rather, we are interested in the idea that having to continuously cope with uncertainty and life threat could lead aid workers to experience PTG, particularly in terms of action-focused growth (Westphal & Bonanno, 2007).
Furthermore, while on the one hand many authors have questioned the nature of the growth factor measured given that it is often found to correlate positively with indicators of posttraumatic stress (Hobfoll, Hall, et al., 2007; Hobfoll, Watson, et al., 2007; McMillen, 2004; Zoellner & Maercker, 2006), on the other hand, to our knowledge, no studies have measured aspects of subjective well-being as a means of independently assessing the relationship between stress and growth. If PTG is found to influence other areas of well-being, it may reflect real growth after a traumatic experience (Bitsch, Elklit, & Christiansen, 2011; Clay, Knibbs, & Joseph, 2009).
The construct of subjective well-being (SWB) is a multifaceted concept that may be explored by assessing multiple and diverse dimensions. The construct was introduced by Diener, Suh, Lucas, and Smith (1999) to describe a “broad category of phenomena that includes people’s emotional responses, domain satisfactions and global judgments of life satisfaction” (p. 277). As such, SWB is thought to stimulate processes of meaning-making via enhanced cognitive functioning (Fredrickson, 2001). In this respect, Diener shares Tedeschi and Calhoun’s (2004) assumption that people adapt to a traumatic event via processes of meaning-making. Furthermore, the revised adaptation theory (Diener et al., 1999) argues that the set point of a person’s subjective well-being varies within a given range and can be subject to dramatic change after a significant life event. In the words of Tedeschi and Calhoun (2004), a positive change after a traumatic event represents posttraumatic growth.
Recently the Organization for Economic Co-operation and Development (OECD, 2013) has issued guidelines suggesting that subjective well-being should be measured as a three-factor model that includes life evaluation, affect, and eudaimonia or a sense of meaning and purpose in life. With regard to the latter factor, contemporary psychology holds that the pursuit of that which is worthwhile is accompanied by a distinctive set of subjective experiences (and aspects of functioning) that are distinguishable from pleasure in the hedonic meaning of that term (Huta & Waterman, 2014).
Life evaluation can be measured using a personal well-being index such as that developed by the World Health Organization—WHO-5, a five-item well-being scale (WHO, 1998)—whereas affect is typically measured using the Positive and Negative Affect Scale (PANAS; Watson & Clark, 1994). Kahneman, Diener, and Schwarz (1999) and Diener et al. (1999) describe positive affect as a unidimensional, single-axis concept that captures positive emotions such as joy and contentment. Negative affect, however, is seen as a multidimensional concept that can reflect a range of emotional states such as anger, sadness, or anxiety. Unlike positive emotions, these negative feelings are not always present at the same time, hence the multidimensionality of this axis (OECD, 2013). Finally, eudaimonia as psychological flourishing is reflected in interest in learning, autonomy, sense of purpose, or social engagement (OECD, 2013). For the purposes of the present research, we adopted a well-known and widely used instrument, the General Health Questionnaire (GHQ; Goldberg & Williams, 1988)—a context-free measure of syndromes that may be used to measure psychological well-being by testing for a range of psychological states including unhappiness, nervousness, and social inadequacy—to tap into the construct of eudaimonic well-being (Veronese & Pepe, 2014). This was in line with existing studies in which the GHQ was used to measure subjective well-being as a form of “psychological wealth,” in which lasting satisfaction is derived from meaningful values and goals within a process of positive character development (Cloninger & Zohar, 2011; Gravensteen, Helgadottir, Jacobsen, Sandset, & Ekeberg, 2012; Linna et al., 2013; Wyller, Holmen, Laake, & Laake, 1998). However, the General Health Questionnaire was developed to evaluate psychiatric morbidity rather than psychological well-being, and therefore focuses on poor mental health, rather than on the positive factors emphasized within a philosophical framework advocating eudaimonic perspectives on happiness (Ben-Shahar, 2007; Seligman, 2002; Warr, 2012).
The study
The aim of the present study was to model how stress reactions after traumatic events influenced subjective well-being (SWB) via the indirect effect of posttraumatic growth (PTG) in a sample of Palestinian professional helpers from the Gaza Strip and West Bank (n = 201). Many studies indicate that the dimensions of trauma have a direct negative impact on multiple indicators of individual well-being and health (Erbes, 2011; Gellis, Mavandadi, & Oslin, 2010; Renshaw, Rodrigues, & Jones, 2008; Schnurr, Lunney, Bovin, & Marx, 2009; Sledjeski, Speisman, & Dierker, 2008). In the model hypothesized here, SWB was operationalized as a latent construct measured by different indicators: affect balance (Watson & Clark, 1994), psychological distress (Goldberg & Williams, 1988), and general well-being (Bech, Olsen, Kjoller, & Rasmussen, 2003). The outcomes of being involved in traumatic events were measured in terms of avoidance, intrusion, and hyperarousal (Veronese & Pepe, 2013).
While the direct relationship between exposure to traumatic events and SWB has been clearly established, the study of the indirect effect of trauma on SWB via posttraumatic growth (i.e., the positive changes experienced by an individual as a consequence of the psychological effort made to deal with a challenging situation; Tedeschi & Calhoun, 2004) is a relatively new focus of interest for the enquiry into the role played by psychological resources in adverse situations. On the one hand, posttraumatic stress is conceptualized as a catalyst for PTG: greater avoidant and intrusive posttraumatic reactions are generally related to stronger PTG (Helgeson et al., 2006). In a similar fashion, when low levels of posttraumatic stress are found it is expected that individuals will report low levels of PTG (Carroll, 2014). On the other hand, PTG has been reported to be a predictor of SWB (McDonough, Sabiston, & Wrosch, 2014) and it appears to be a key mechanism protecting the individual from the effects of posttraumatic stress (Shakespeare-Finch, Rees, & Armstrong, 2014; Veronese, Castiglioni, Barola, & Said, 2012).
Although professional helpers may be seen as dealing with challenging and distressing life experiences, to our knowledge, the effects of posttraumatic growth on their subjective well-being remain largely unexplored. In this area, studies investigating how posttraumatic growth, in interaction with trauma, affects subjective well-being make a key contribution to the health of professional helpers, especially in contexts of low-intensity warfare (Hamber et al., 2015; Veronese et al., 2012). The present study used a structural equation approach to model the direct effect of reactions to traumatic events on subjective well-being. In addition, the proposed model evaluated both the direct effect of trauma on posttraumatic growth and the indirect effect of trauma on well-being via posttraumatic growth (the conceptual model is represented in Figure 1). In light of existing findings, we expected that: H1. Levels of trauma would be negatively and directly related to subjective well-being.
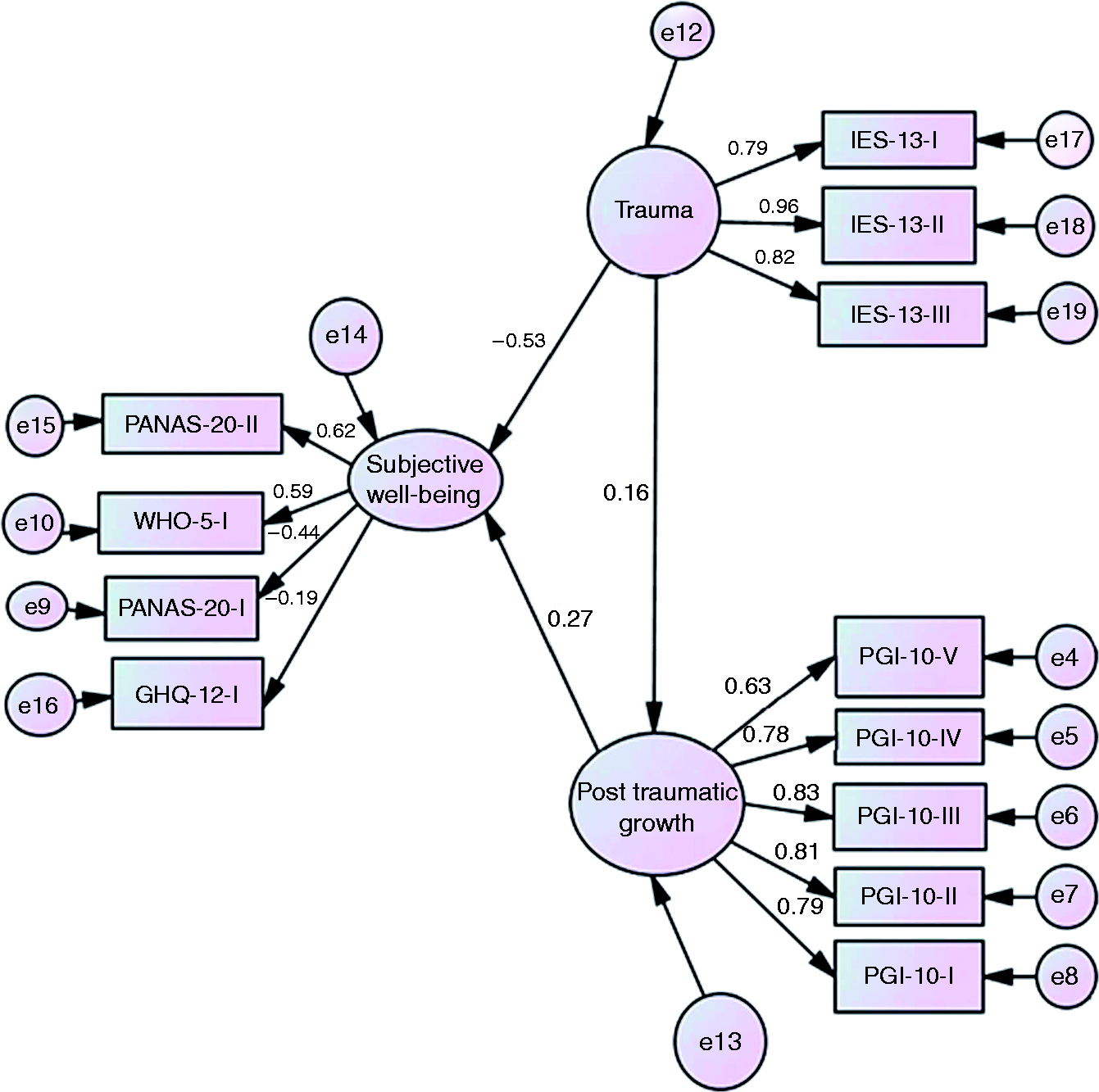
Conceptual model of trauma, subjective well-being, and posttraumatic growth. Results for the structural equation model (direct and indirect effects). H2. Levels of trauma would be positively and directly related to posttraumatic growth. H3. Posttraumatic growth would be positively and directly related to subjective well-being.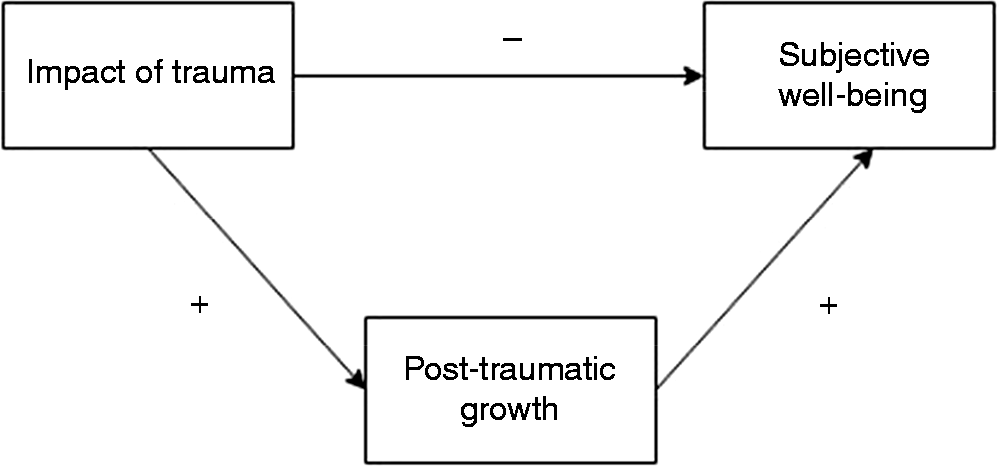
Method
Sample
Participants in the study were professional helpers (i.e., medical doctors, nurses, psychologists, counsellors, and social workers) working in public health organizations in the Gaza Strip and West Bank (n = 201). We applied the maximum variation method of purposive sampling (Teddie & Yu, 2007). In the category of professional helpers, we included those health practitioners who had received specific academic training in working with populations affected by disasters in emergency settings. We adopted Durlak’s (1979, p. 80) definition of professional helpers as “individuals who have received post-baccalaureate formal clinical training, professional programs of psychology, psychiatry, social work, and psychiatric nursing … Those who have not received this training are paraprofessionals” (Hattie, Sharpley, & Rogers, 1984). Gender distribution was 42.8% male (n = 86) and 57.2% female. All participants were of Palestinian ethnicity, Arabic native speakers, and Muslim. Participants’ mean age was 34.3 years (SD = 8.46), and their ages ranged from 20 to 62 years. Mean length of professional experience was 9.09 years (SD = 7.02), with years’ experience ranging from 1 to 33 years. Participants’ professional categories (as defined in the Standard Occupational Classification System [SOCS]; U.S. Bureau of Labor Statistics, 2010) were as follows: professional nurses (21.9%, SOCS code 29-1071), physicians (8.1%, 29-1060), psychologists (15.4%, 19-3030), social workers (16.4%, 21-1020), counsellors (11.4%, 21-1010), other (13.9%), missing values (12.9%).
Ethical issues, inclusion criteria, and data collection method
The research was conducted with the involvement of local organizations operating in the health sector. It was carried out for scientific purposes related to exploring the dynamics of health among professional helpers. In order to take part in the study, helpers were required to have completed at least 1 year of professional experience, be Palestinian, be 25 to 65 years old, and work in direct contact with patients in hospitals or other healthcare contexts. In keeping with the maximum variation sampling paradigm informing the research design, participants were selected with a view to covering the full range of helper roles in the Palestinian care system and obtaining representative proportions of the listed professions. Another criterion for inclusion in the sample was having witnessed at least one episode of war or armed fighting in the occupied Palestine territories (OPT) over the 3 years prior to the study. Participants were fully and clearly briefed about the measures in place to protect their privacy and anonymity before the data was gathered. All the participants provided explicit verbal consent and confirmed their understanding that their anonymity and confidentiality would be protected throughout dissemination of the research findings. The study received the ethical approval of the Psychiatry, Nursing, and Midwifery Research Ethics Committee (PNM RESC) of King’s College London Research Ethics Committee (Protocol Number: 2PNM 13 14-121). Ethical clearance was also obtained from the boards of the hosting organizations. Participants’ identities were kept confidential. The database was password-protected and encrypted. All files will be deleted within 5 years of first storage.
The resulting sample was composed of Palestinian helpers from two Palestinian areas (Gaza Strip, West Bank). Both contexts are characterized by ongoing political and military violence.
The self-report instruments were administered to the participants using a paper-and-pencil method over the period April–June 2014 by local Arab-speaking personnel trained in social research. All the measures had been translated into standard Arabic, which was readily understood by the participants, all of whom were native Arabic speakers.
Measures
Traumatic Events Checklist (TEC)
The Traumatic Events Checklist (TEC) is based on the checklist developed in Arabic by Abu Laila, Thabet, and Vostanis (2009). It consists of questions about exposure to traumatic events that can arise in the context of the occupied territories. These questions can be grouped into three categories: (a) war-related trauma, including being shot at, seeing someone being killed or shot, suffering from witnessing rocket fire and shootings, and witnessing the demolition of properties by tanks or rocket fire; (b) detention, either being detained or having a family member or close friend in prison; and (c) economic loss, with just one item: having lost one’s home as a result of bombing or rocket fire. There is no existing scoring protocol or cut-off score for this measure.
Impact of Event Scale (IES-13)
The Impact of Event Scale (IES-13), the Arabic version (Veronese & Pepe, 2013) of the Impact of Event Scale (Horowitz, Wilner, & Alvarez, 1979) is a self-report screening tool measuring traumatic reactions in people who have experienced traumatic events in contexts of violence or low-intensity warfare. Participants rated 13 items on a 4-point scale (not at all, rarely, sometimes, often; scores: 0, 1, 3, and 5) with specific reference to the previous 2-week period. No reversed items were included in the measurement model. Earlier empirical evidence from the Palestinian context (Veronese & Pepe, 2013) prompted the adoption of a tri-partite measurement model composed of intrusion, avoidance, and hyperarousal subscales. It should be noted that intrusion and hyperarousal were so highly correlated as almost to be considered overlapping. High scores on the IES-13 reflect high levels of vicarious trauma. In the present study, reliability coefficients were .83 for intrusion, .88 for avoidance, and .81 for hyperarousal respectively.
General Health Questionnaire (GHQ)
The General Health Questionnaire (GHQ) is an instrument aimed at “detecting psychiatric disorders among respondents in community settings and non-psychiatric clinical settings” (Goldberg, 1972, p. 1). It is widely used in clinical practice to measure changes in patients’ symptomatology over time (Ormel, Koeter, van den Brink, & Giel, 1989) and in psychology and the social sciences for research purposes. In general, the GHQ asks respondents to describe their global health status as perceived over the previous few weeks. Participants are instructed to rate each item (some items are negatively worded) on a 4-point Likert scale. A generally accepted way of interpreting GHQ scores is to sum all the individual item scores to obtain a global cumulate measure of psychological distress ranging from 0 to 36 (Goldberg & Williams, 1988), with high scores indicating a state of psychological distress. The present study adopted the Arabic version of the GHQ, which comprises 12 items (Daradkeh, Ghubash, & el-Rufaie, 2001); for this unidimensional scale, Cronbach’s alpha reliability coefficient was .79 in the present study.
World Health Organization Well-Being Index (WHO-5)
The World Health Organization Well-Being Index (WHO-5) is a self-report questionnaire composed of five positively worded questions related to mood, vitality, and general life interests. Given that it takes very little time to administer this measure (2–3 minutes), it is routinely adopted in clinical practice as a reliable measure of psychological functioning (Heun, Burkart, Maier, & Bech, 1999). The global score for the index is calculated by summing the scores (Likert-type response scale) for each of the five items and it ranges from 0 to 25, with higher scores indicating greater well-being. The present study adopted the Arabic version of the WHO-5 (Sibai, Chaaya, Tohme, Mahfoud, & Al-Amin, 2009); for this unidimensional scale, the Cronbach’s alpha reliability coefficient was .87.
20-item Positive and Negative Affect Schedule
The 20-item Positive and Negative Affect Schedule (PANAS-20; Watson, Clark, & Tellegen, 1988) is a group of self-report questionnaires aimed at evaluating affect balance as a crucial facet of subjective well-being (Diener, 2008). The questionnaire is composed of 20 different items rated on a Likert-type scale measuring respondents’ experience of positive affect (PA) and negative affect (NA) over the previous weeks. The two scales are usually found to be weakly correlated. In the current study, the extent to which each emotion had been experienced over the previous 2 weeks was rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (very much). Overall scores ranged from 10 to 50, with low scores indicating low levels of positive and negative affect and high scores suggesting high levels of positive and negative affect.
An adapted Arabic language version of the instrument was used. Cronbach’s alpha reliability coefficients were .81 and .73 for negative and positive affect, respectively.
Post Traumatic Growth Inventory (PTGI-10)
The Palestinian version of the Post Traumatic Growth Inventory (PTGI-10; Kira et al., 2013) evaluates perceived positive changes in life (e.g., greater appreciation of life) following traumatic experiences and it has been applied across a variety of studies and populations (Calhoun & Tedeschi, 2006). The questionnaire comprises 21 items loading on factors mapping five different domains: personal strength, spiritual change, relating to others, new possibilities, appreciation of life. The response scale ranges from 0 (I did not experience this change to a very great degree) to 5 (I experienced this change to a very great degree). High scores on the PTGI indicate stronger posttraumatic growth. The present study adopted a shortened form of the PTGI composed of 10 items loading on five factors (Cann et al., 2010). Given that the measurement model needed to be tested, confirmatory factor analysis was applied to the current data. The results confirmed the robustness in the Palestinian context of the abbreviated form of the PTGI: χ2 (25) = 52.66, p = .01; normed chi-square (NC) = 2.26; root mean square error of approximation (RMSEA) = .059, 95% CI [0.039, 0.080], normed fit index (NFI) = .97, nonnormed fit index (NNFI) = .96, comparative fit index (CFI) = .983. Reliability coefficients (Cronbach’s alpha) for the individual subscales were: personal strength (.81), spiritual change (.73), relating to others (.77), new possibilities (.75), appreciation of life (.65). Respondents were given the following instruction: “Consider the 10 areas listed below that are sometimes reported to have changed after traumatic events. Please mark the appropriate box beside each description indicating how much you feel you have experienced change in the area described” (Tedeschi, 1996, pp. 458–459). This more general instruction was preferred to focusing on a specific “event” or crisis, with a view to capturing the outcomes of cumulative traumatic experience, which is the most common in health providers working in crisis settings (Pigni, 2014).
Data analysis
The proposed model was analyzed via structural equation modelling (SEM) computed using the AMOS 21.0 software package. First, descriptive data were calculated in order to evaluate the measures’ psychometric properties. To identify outliers, all variables were first checked by computing Mahalanobis’ distance (p < .001). There were no extreme multivariate values. Next, the data were assessed to verify whether the scores were normally distributed. None of the variables under study displayed kurtosis or skewness values outside of the recommended ranges (−1, +1), indicating that it was appropriate to use maximum likelihood as a method of parameter estimation in the subsequent SEM phase of data analysis (Gath & Hayes, 2006; Pepe & Addimando, 2014). Second, the hypothesized theoretical model was assessed using covariance-based structural equation modelling (SEM) an approach to inferential data analysis (Joreskog & Sorbom, 1989), which enables the pattern of interrelationships among a set of constructs and latent variables under study to be tested. The logic underpinning the SEM technique is that of comparing the covariance matrix (Σ) obtained by specifying model parameters, with the empirical matrix obtained from the observed data (S). By evaluating the degree to which Σ resembles the structure of S, the appropriateness of a given structural model may be determined. The modelled data is assessed based on multiple goodness-of-fit indexes (Bagozzi & Yi, 1988; Brown, 2006; Hair, Black, Babin, & Anderson, 2010; Hu & Bentler, 1999). The following were used in the present study: χ2 (nonstatistically significant values indicate a good fit; Schumacker & Lomax, 2004), RMSEA < .05 (Hu & Bentler, 1999), standardized root mean square residual (SRMR < .08; Hu & Bentler, 1999), NFI > .95 (Marsh, Hau, & Wen, 2004), Tucker–Lewis Index (TLI > .95; Tucker & Lewis, 1973), CFI > .95 (Vandenberg & Lance, 2000).
Results
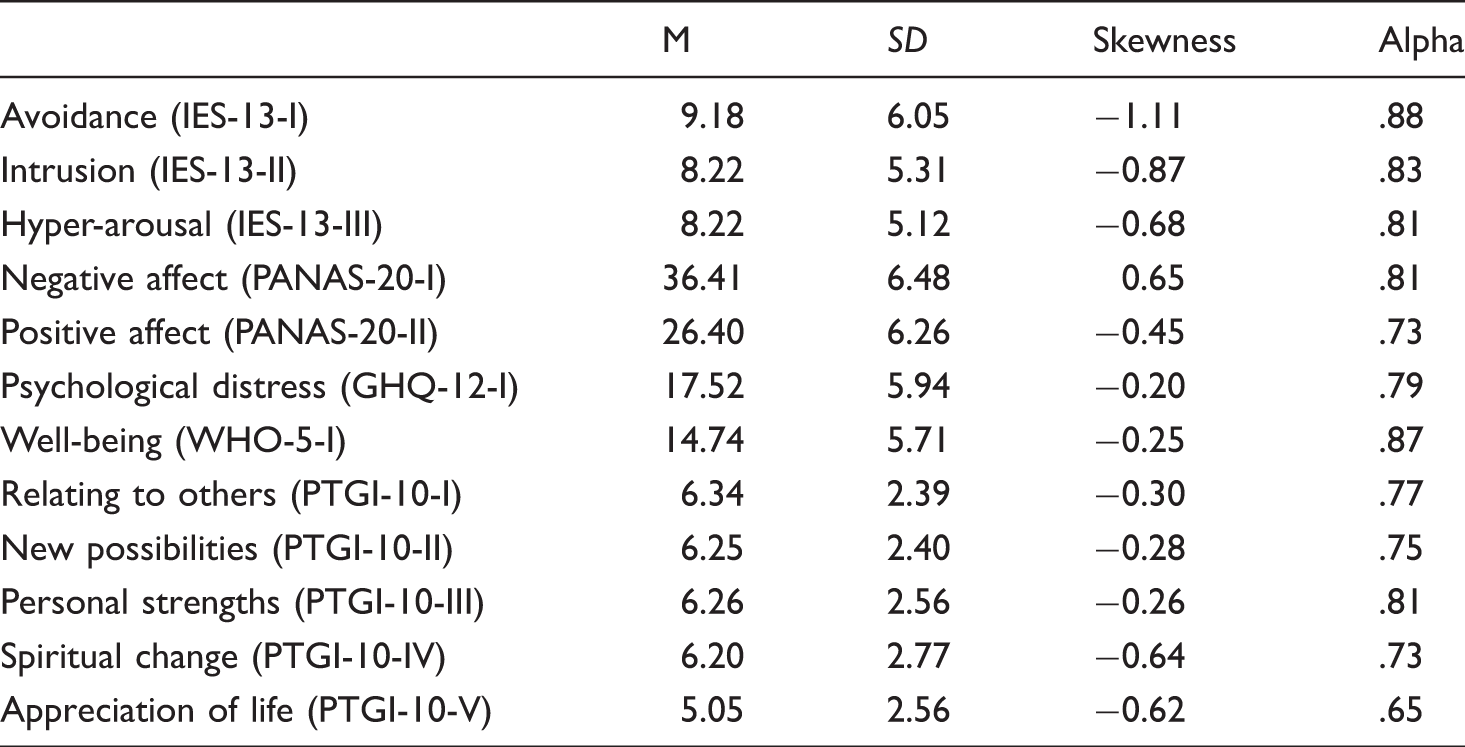
Summary of descriptive statistics for the overall sample of helpers (N = 201)
Concerning the nature of the trauma exposure reported by our respondents via compilation of the Traumatic Event Checklist, almost all participants (98%) had experienced or witnessed at least two traumatic events over the 3 years prior to the study. Approximately half of the participants (39%) had experienced or witnessed more than 10 traumatic events. The most common were “Witnessing bombardment of other people’s houses by airplanes and helicopters” (92.5%), “Witnessing firing at neighbor’s houses by tanks and heavy artillery” (91%), “Body searched” (58%), “Shot at or hit” (69%), and “Saw friend/neighbor humiliated” (67%).
With regard to the outcomes of being exposed to traumatic events, the data confirmed the moderate levels of traumatization in helpers already identified in previous studies with different samples of health professionals working in Palestinian refugee camps (Veronese, Fiore, Castiglioni, & Natour, 2014; Veronese & Pepe, 2013, 2014).
The majority of health workers assessed in the present study were affected by medium to high levels of psychological distress. When the conventional thresholds (0–10, “low psychological distress”; 11–12, “typical value”; 13–15, “more than typical”; 16–20, “high psychological distress”; 21–36, “severe psychological distress”) suggested by Goldberg et al. (1997) were applied, 84.6% of Palestinian helpers reported “more than typical” (19.9%), “high” (30.4%), and “severe” (35.3%) psychological distress, whereas only 6.1% fell within the category “low psychological distress.” In comparison with data gathered in different contexts but with similar samples, Palestinian helpers’ GHQ-12 scores (M = 14.74, SD = 5.77) were found to be uncommonly high. For instance, lower scores (M = 10.7) were found in Australian ambulance officers (Mayhew & Chappell, 2003), in British mental health nurses (M = 9.7, SD = 4.5; Snelgrove, 1998), in Swedish practitioner nurses (M = 9.81, SD = 3.47) and physiotherapists (M = 9.75, SD = 3.47; Nerdum & Ostertun-Geirdal, 2014), and in a multisample of human service workers (M = 11.53, SD = 5.81; Dollard, Winefield, & Winefield, 2001, p. 106). Concerning well-being (WHO-5), it may be concluded that 48.8% of helpers obtained a raw score of less than 50 indicating a state of “poor well-being,” while 9.7% appeared to be in need of further investigation for depression symptoms under the ICD-10 criteria. Compared with the GHQ-12 scores, it would seem that the well-being scores reflected a less “problematic” picture than what might reasonably be expected in light of the psychological distress scores alone. A similar outcome was obtained when the professional helpers’ affect balance scores were analyzed. In fact, compared to normative data for the PANAS-20 (Crawford & Henry, 2004), we surprisingly found that the levels of positive affect (M = 26.4, SD = 6.26) experienced by these Palestinian helpers were similar to those of a British nonclinical sample (M = 31.3, SD = 7.65). This suggested the presence of some kind of mechanism mitigating the effect of trauma on subjective well-being. In line with recent developments in the literature on the relationship between trauma and posttraumatic growth (S. Dekel et al., 2012), we hypothesized that this buffering role was played by individuals’ levels of posttraumatic growth. Consequently, we set out to evaluate the plausibility of a structural model in which the direct effect of trauma on subjective well-being was evaluated via posttraumatic growth. In line with current practice (e.g., Lyubomirsky & Lepper, 1999), the latent variable “subjective well-being” specified in the model was represented by multiple observed indicators, whereas the effect of trauma and posttraumatic growth were represented by their corresponding measurement models. Consequently, the parameters to estimate were: (a)
Analysis of both absolute and relative fit indexes revealed an excellent fit, 1 supporting full acceptance of the model, χ2 = 67.68, p = ns, NC = 1.32, RMSEA = .040 (pclose = .75), SRMR = .058, NFI = .951, TLI = .976, CFI = .982.
All of the direct effects were statistically significant. In particular, the standardized direct effect of trauma on subjective well-being (β1,3 = −.52, p < .001) bore out the first hypothesis, implying that exposure to traumatic events had a negative effect on helpers’ subjective well-being. The direct effect of trauma on posttraumatic growth (β2,3 = .19, p < .001) was in line with the second hypothesis, in that posttraumatic growth was positively influenced by levels of trauma. The direct effect of posttraumatic growth on subjective well-being was .34, supporting the third hypothesis. In particular, analysis of the standardized total effects revealed that trauma negatively influenced positive affect (−.21) and well-being (−.36). In addition, exposure to trauma seemed to increase negative affect scores (.26) and psychological distress (.08). Explained variance (R2) in subjective well-being was 31.1%. All in all, the findings supported the idea that posttraumatic growth contributes to mitigating and buffering (in the order of approximately 10%) the effect of trauma on subjective well-being. It therefore seemed to be a key resource that assists helpers in dealing with the consequences of stressful life events.
Discussion
The primary aim of this study was to model, via a structural equation approach, how stress reactions after traumatic events influenced SWB via the indirect effect of posttraumatic growth in two samples of Palestinian professional helpers from the Gaza Strip and West-Bank. SWB was operationalized in terms of three different indicators: affect balance (Watson & Clark, 1994), psychological distress (Goldberg & Williams, 1988), and general well-being (Bech et al., 2003). The results confirmed all three hypotheses tested.
We found that levels of trauma were directly and negatively correlated to subjective well-being (H1). The more Palestinian practitioners are exposed to violent trauma, the more their psychological well-being is at risk of being undermined (Karamouzian & Carmichael, 2014; Veronese et al., 2014). This finding is confirmed by previous studies documenting the extreme sense of insecurity and threat that Palestinian helpers have to cope with, due to the ongoing military occupation and its consequences for the health system in the OPT (Giacaman et al., 2009; Veronese, 2013; Veronese et al., 2016). On the other hand, in accordance with recent studies investigating similar constructs (Magruder, Kılıç, & Koryürek, 2015; Taku, Tedeschi, & Cann, 2015), the results obtained with our sample of Palestinian helpers showed a direct and positive relation between traumatic stress and posttraumatic growth (H2). The more Palestinian helpers are affected by traumatic sequelae, the more they are likely to experience a subjective sense of growth after trauma. These results appear to fit with previous studies conducted with Palestinian samples, in which helpers operating on the front line were shown to be able to cope with severe trauma thanks to personal resources, spirituality, and activism, and to experience positive feelings as situated political actors in a community at risk of social, physical, and political disruption (Makkawi, 2014; McNeely et al., 2015; Veronese, 2013; Veronese et al., 2016).
The findings confirm the positive relationship between posttraumatic growth and subjective well-being. The more Palestinian helpers benefit from a sense of growth after trauma, the more they conserve a self-perception of feeling subjectively well, despite the risky conditions they are working in. During their working life span, these helpers are likely to be exposed to life threat and to personally experience episodes of violence and humiliation as Palestinians in the front line when violence and conflict escalate or terror attacks occur (Giacaman, Abu-Rmeileh, Husseini, Saab, & Boyce, 2007). The ability to attribute meaning to their lives via relational networks, spirituality, and appreciation of their personal resources appears to help these care professionals to strategically maintain a sense of integrity and to enact resilience (Veronese & Pepe, 2014; Veronese et al., 2016).
In sum, the construct of posttraumatic growth may contribute to explaining how helpers working in extremely dangerous conditions can continue to maintain good psychological functioning and ability to adjust to trauma in terms of perceived psychological wealth and well-being (Vindevogel, Ager, Schiltz, Broekaert, & Derluyn, 2015). These findings provide us with valuable evidence regarding the importance of promoting PTG in emergency service contexts in order to enhance well-being and prevent psychological suffering in helpers exposed to war and violence (Shakespeare-Finch et al., 2014). Specifically, helpers in this category require targeted training focused on self-experience to raise their awareness of their own personal and interpersonal skills and of the survival resources to be drawn on in order to reduce the risk of burnout or psychological impairment. Supervision should be aimed at helping these workers to access those aspects of their lives that provide a sense of meaningfulness and personal strength connected with a sense of community—at the political and spiritual level—so that they will be better equipped to deal with suffering and violence, attacks in conflict zones, and unstable environments (Karamouzian & Carmichael, 2014). Finally, the current research findings might inform the development of broader community resilience programs relevant to and appropriate for the ongoing Palestinian condition, which is characterized by a lack of resources and underdeveloped health system in both the West Bank and the Gaza Strip (Makkawi, 2014).
Palestinians share a master narrative of social suffering and political injustice. This suggests that healthcare for the Palestinian population in general and for helpers in particular, should not be exclusively focused on medical symptoms, but should also contemplate quality of life and the political domains of overall well-being (Giacaman, Mataria, et al., 2007; Mataria et al., 2009). PTG, as a psychological process related to the experience of growth in presence of traumatic suffering, is a construct that oscillates along the continuum between ease and disease, between mental well-being and mental disease. In fact, the majority of ordinary Palestinians experience severe and chronic distress as they endure the suffering and trauma of ongoing warlike conditions (Giacaman, Mataria, et al., 2007). Social dimensions, such as family and community support, nurture their connectedness with others, sustaining their sense of coherence and growth despite the chronic human insecurity and human rights violations experienced in their daily lives.
Limitations
As in other studies, a number of limitations affecting this work deserve to be addressed. The first main caveat concerns the cross-sectional nature of our research design, which does not allow us to capture the longitudinal relationships between trauma, posttraumatic growth, and subjective well-being. A truly longitudinal study, ideally conducted at multiple levels, would allow the relationships among variables of interest to be tracked dynamically and at a deeper level of complexity. However, it should be noted that in contexts of low-intensity warfare and crisis, longitudinal research designs are difficult to implement due to the probability of unconventionally high attrition rates. The study’s second limitation concerns the nature of the mechanism linking trauma and posttraumatic growth. Our data analysis strategy was essentially based on linear mathematical models and relationships. Recent developments in the field suggest that the relationship between trauma and posttraumatic growth may be also represented by curvilinear models (Shakespeare-Finch & Lurie-Beck, 2013; Taku et al., 2015). In this regard, the selection criteria adopted in the present study (professional helpers characterized by low-medium and medium levels of trauma only) might compensate for this potential source of bias.
Finally, another limitation of this study concerns the uniqueness of the sample, drawn from the Palestinian context in which helpers identify political experiences as playing a key role in determining their overall quality of life (Barber et al., 2014). Palestinian aid workers, in both Gaza and the West Bank, seem to benefit from the so-called political dimension of well-being, identified as a key domain of functioning (McNeely et al., 2015; Sousa & Hagopian, 2011; Veronese, 2013; Veronese et al., 2016). In fact, their personal growth includes active participation in civil resistance to the military occupation. In assisting the population at a time of crisis, Palestinian helpers take on the role of human right defenders in a context of ongoing political violence and discrimination. In this sense, it may not be possible to generalize the current findings to workers operating in different settings. On the other hand, the social and political dimensions of growth, in term of professional perseverance and persistence, may also be an asset for helpers living and working in war-like conditions and ongoing crisis contexts elsewhere (Sousa & Hagopian, 2011). Future research extended to other countries experiencing ongoing political violence, especially in the Middle East, will serve to explore similarities and differences in the dimensions of personal growth displayed by aid workers exposed to traumatic experiences across different cultural and political contexts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.