
Abstract
Background
No large-scale characterizations of neurofilament light chain (NfL) and cognitive outcomes have been conducted in community-dwelling non-Hispanic Blacks.
Objective
This study aims to enhance the application of blood biomarkers, in particular NfL, to ethno-racially diverse communities. We assess the association of NfL with cognitive outcomes, hypothesizing that NfL can identify cognitive changes regardless of diagnostic category.
Methods
Baseline data were analyzed among n = 283 non-Hispanic Blacks (NHB) from the multi-ethnic Health and Aging Brain Study- Health Disparities (HABS-HD). Plasma NfL was measured on the Simoa platform. Linear regression models were conducted, covarying for age, gender, and education.
Results
The majority of study participants (72%) were cognitively unimpaired (CU), with 21% having mild cognitive impairment (MCI), and 6.7% with Alzheimer's disease (AD). In adjusted models among the entire sample, significant associations existed between NfL and Trails A (p < 0.0001), Trails B (p < 0.0001), phonemic (FAS) and semantic (Animals) fluency (p = 0.03), and Symbol Digit Substitution (p < 0.001). When separated by diagnostic classification, significant associations were removed for functions involving executive functions for all diagnostic groups. Higher levels of NfL were positively associated with cognitive diagnosis, older age, and less education.
Conclusions
Plasma NfL levels are significantly associated with measures of executive functioning, which elucidate NfL as a non-specific marker of neurodegeneration associated with efficiency of brain functions involving attention, processing, and generativity. NfL may be a sensitive measure for the detection of alterations in cognitive processing before the onset of phenotypic functional changes of neurodegeneration.
Introduction
There has been increased interest in the utility of blood-based biomarkers as a quick, cost-effective method to learn valuable information about diseases, with blood-based biomarkers being a potential first step in early identification and intervention of disease pathology.1,2 The exploration of blood-based biomarkers, particularly neurofilament light (NfL), holds promise in various neurological disorders, including Alzheimer's disease (AD), multiple sclerosis (MS), amyotrophic lateral sclerosis, traumatic brain injury (TBI), and others.3–7 NfL, a cytoplasmic polypeptide in myelinated neurons, reflects axonal damage and is associated with various Central Nervous System (CNS) pathologies8,9 Although NfL is predominantly released within cerebrospinal fluid (CSF), both CSF and plasma (P) NfL levels exhibit a high correlation.10–12 In MS and TBI, NfL is associated with worse long-term clinical outcomes and brain atrophy. 13 In the context of AD, NfL levels have been implicated in cognitive decline and mild cognitive impairment (MCI), though its specificity to AD pathology is limited due to its association with various CNS disorders. 14 Overall, integration of NfL into the AT(N) diagnostic framework for AD, alongside other biomarkers like amyloid and tau, provides a comprehensive approach to characterizing the disease course. 15
Studies have shown that elevated NfL levels correlate with changes in established measures of neurodegeneration and AD diagnostic states.16–20 However, there is some concern of the consistency of NfL as a biomarker for AD. For example, Nyberg and colleagues 21 longitudinal analyses suggest age-related NfL increase is highly variable, and while AD cases demonstrated elevated NfL levels, NfL could not predict cognitive decline or AD incidence. Mielke and colleagues 4 reported that NfL levels were associated with changes in attention and global cognitive scores in cognitively normal adults and those with MCI (average age = 76) after a 30-month follow-up, while Mattsson and colleagues 19 demonstrated that NfL was correlated with a faster decline in global cognition in individuals with MCI and dementia but not in those without cognitive impairment. A limitation in evaluating neurofilament light (NfL) is the absence of age-related cutoff scores, non-standardized immunoassay methods, the inability to precisely identify focal atrophy using NfL, and the lack of investigation of NfL values and cognitive outcomes in diverse populations. The aim of the present study is to characterize plasma NfL values and cognitive outcomes in a population of community-dwelling non-Hispanic Blacks (NHB).
Methods
Participants
Data was analyzed from n = 283 non-Hispanic Black (NHB) participants from the Health & Aging Brain Study – Health Disparities (HABS-HD). HABS-HD is an ongoing, longitudinal, community-based study of health disparities in brain health in underrepresented populations, with specific recruitment of Hispanic, Mexican Americans (MA), non-Hispanic whites (NHW), and most recently, non-Hispanic Blacks. Methods of the HABS-HD are published elsewhere, and are briefly described below.
Recruitment, protocol, and inclusion
Participant recruitment for the HABS-HD study is community-based participatory research approach.22,23 This approach involves collaborating with local communities through culturally sensitive outreach methods. The HABS-HD protocol includes interviews, functional exams, blood draws for clinical labs and biobanking, neuropsychological testing, and 3 T MRI scans of the brain. Additionally, amyloid and tau positron emission topography (PET) scans are ongoing for the full cohort. The study protocol can be conducted in Spanish or English. All procedures are conducted under IRB-approved protocols, and participants (or their legal representatives) provide written informed consent. Data from the study is accessible to the scientific community through the UNTHSC Institute for Translational Research website.
The current study focuses on data from NHB participants enrolled in the HABS-HD study as of January 2024 (data release 5). These individuals self-reported Black/African American ethnicity and met study inclusion criteria of (1) willingness to provide blood samples, (2) capable of undergoing neuroimaging studies, (3) age 50 and above, and (4) fluent in English or Spanish. Exclusion criteria includes (1) Type 1 diabetes, (2) presence of active infection, (3) current/recent (12 month) cancer (other than skin cancer), (4) current severe mental illness that could impact cognition (other than depression), (5) recent (12 months) traumatic brain injury with loss of consciousness, (6) current/recent alcohol/substance abuse, and (7) active severe medical condition that could impact cognition (e.g., self-reported end stage renal failure, chronic heart failure, chronic obstructive pulmonary disease). Education was defined as years of self-reported education.
Clinical
The HABS-HD protocol 24 includes the following cognitive assessments: Mini-Mental Status Exam (MMSE), 25 Wechsler Memory Scale-Third Edition (WMS-III) Digit Span and Logical Memory, 25 Digit Symbol Substitution, Trail Making Test Parts A and B, 25 Spanish-English Verbal Learning Test (SEVLT), 26 Animal Naming (semantic fluency), 25 phonemic verbal fluency (FAS), 25 as well as the American National Adult Reading Test (English-speakers), 25 and Word Accentuation Test (Spanish-speakers). 27 Z-scores are calculated using normative references from the HABS-HD cohort classified by education (i.e., 0–7 years, 8–12 years, and 13 + years), primary language (English or Spanish) and age (median split ≤65 and ≥66). 24 An informant interview is also conducted for completion of the Clinical Dementia Rating Scale 28 by clinicians with expertise in dementia to evaluate for functional declines.
Diagnostic classification
Classification of cognition were measured independent of biomarker profiles. Cognitive diagnoses were assigned using an algorithmic process map (decision tree) and verified with consensus review into the following broad categories: 1) Cognitively unimpaired (CU) with no cognitive complaints, MCI with cognitive complaints made by the individual or an informant and at least one cognitive test score falling ≤1.5 standard deviations below the normative ranges, and Dementia, with both cognitive complaints and at least two cognitive test scores falling ≤2 standard deviations below accepted normative ranges.29,30
Biomarkers
Fasting blood samples were collected, processed within 120 min of draw, clotted in a vertical position at room temperature before centrifugation and inverted 5–10 times. Samples were stored at −80° and stored in aliquots no larger than 0.5 ml; consistent with previously published international guidelines.2,24 Assay preparation was completed using custom automated StarPlus system from Hamilton Robotics. Plasma markers of neurodegeneration (neurofilament light chain [NfL]) were assayed using the ultra-sensitive single molecule array (SIMOA) technology platform on the HD-X (Quanterix.com). A total of 500 µL of plasma was utilized to measure biomarker levels. Sample and control concentrations were calculated from a 4PL fit. Coefficient of Value (CV) for NfL were (Avg CV = 0.038; Avg lowest level of detection [LLOD] = 0.038; Avg highest level of detection [HLOD] = 1800; concentration = pg/µL).
Statistical analysis
Analyses were conducted in R (V4.3.2) and SPSS(v28). Descriptive statistics were captured using mean (M) and standard deviation (SD) for demographic and clinical variables. Multivariate analysis of variance (MANOVA) was used to determine the association of NfL with cognitive performance, with all predictors entered into multi-variate models. Age (in years), gender, and years education were entered as covariates across models. Statistical significance was set at p < 0. 05.
Results
Demographics
As of January 2024, there were a total of n = 828 participants of non-Hispanic Blacks enrolled in the HABS-HD study. All individuals included in the analysis are English-speakers. Cases (n = 545) containing insufficient NfL level (below the threshold of 0.038 pg/µL) were removed from analysis. Sufficient power was retained and (n = 283) participants were included in the analysis. The demographic characteristics for n = 283 participants included in the analysis are represented in Table 1. All other clinical variables had a mean within the average value of the z score and are summarized along with corresponding SDs in Table 1.
Demographic characteristics of the study population.
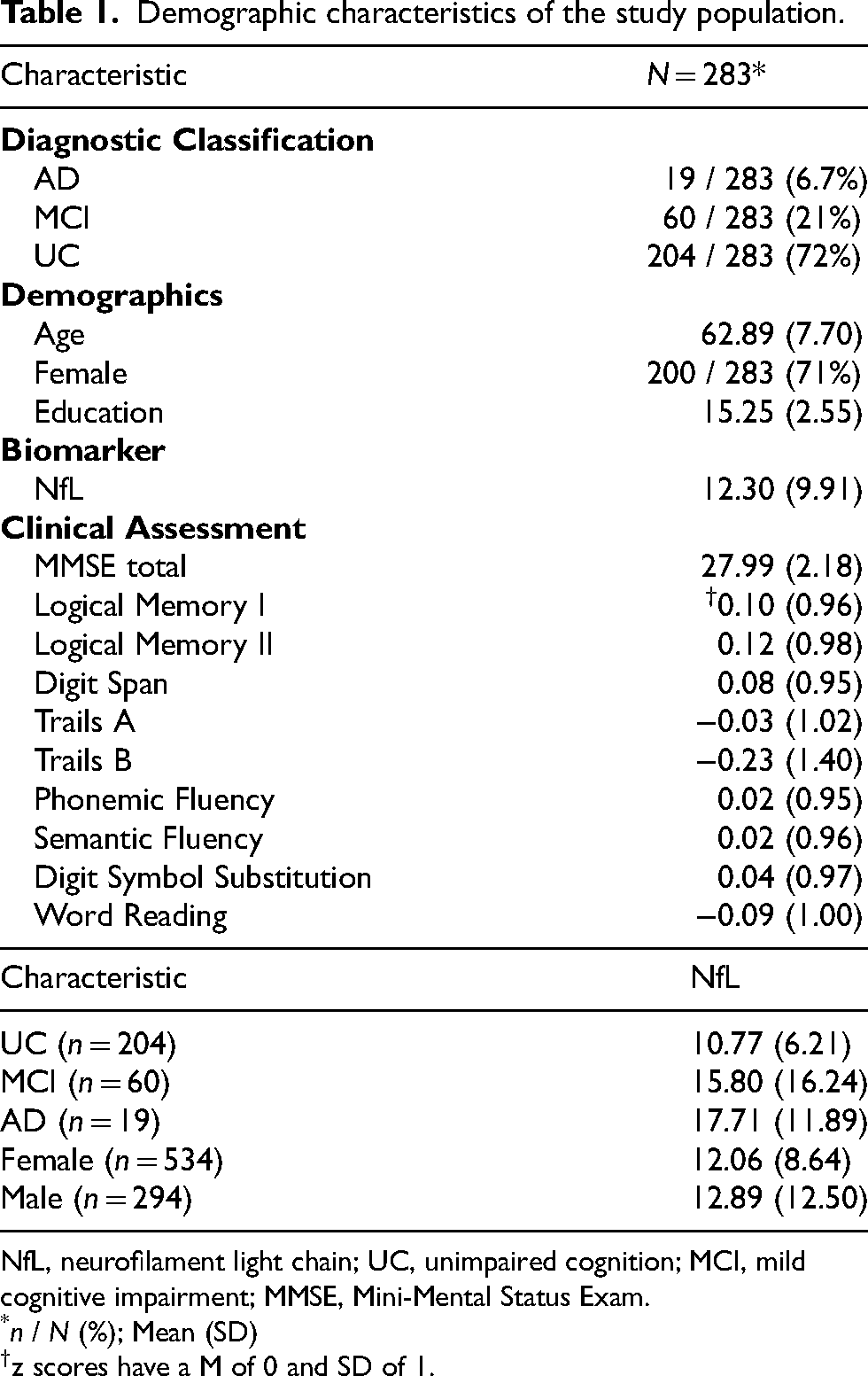
NfL, neurofilament light chain; UC, unimpaired cognition; MCI, mild cognitive impairment; MMSE, Mini-Mental Status Exam.
n / N (%); Mean (SD)
z scores have a M of 0 and SD of 1.
Nfl levels in relation to demographic variables
NfL level was weakly associated with age and education. Older individuals had higher values of NfL (r = 0.25), and those with higher education are associated with lower values of NfL (r = −0.23). There were no significant sex differences in mean NfL level. When separated by diagnostic group, NfL levels were highest for those classified as AD, followed by MCI, and UC; these group differences were significant (Table 2).
Association of neurofilament light (NfL) with demographic characteristics.
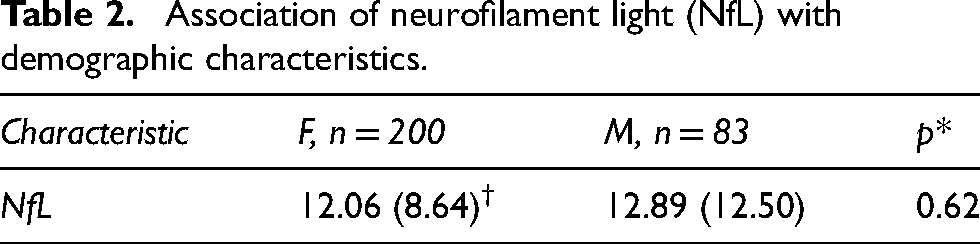

F, female; M, male; NfL, neurofilament light chain; UC, unimpaired cognition; MCI, mild cognitive impairment.
Wilcoxon rank sum test
Mean (SD)
Kruskal-Wallis rank sum test
Mean (SD)
Nfl levels in relation to neuropsychological test performance
Across the entire sample, after covarying for age, sex, and years of education, plasma NfL was significantly associated with Trails A, Trails B, FAS, Animals, and Digit symbol substitution (Table 3).
Association of neurofilament light (NfL) with cognitive test performance.
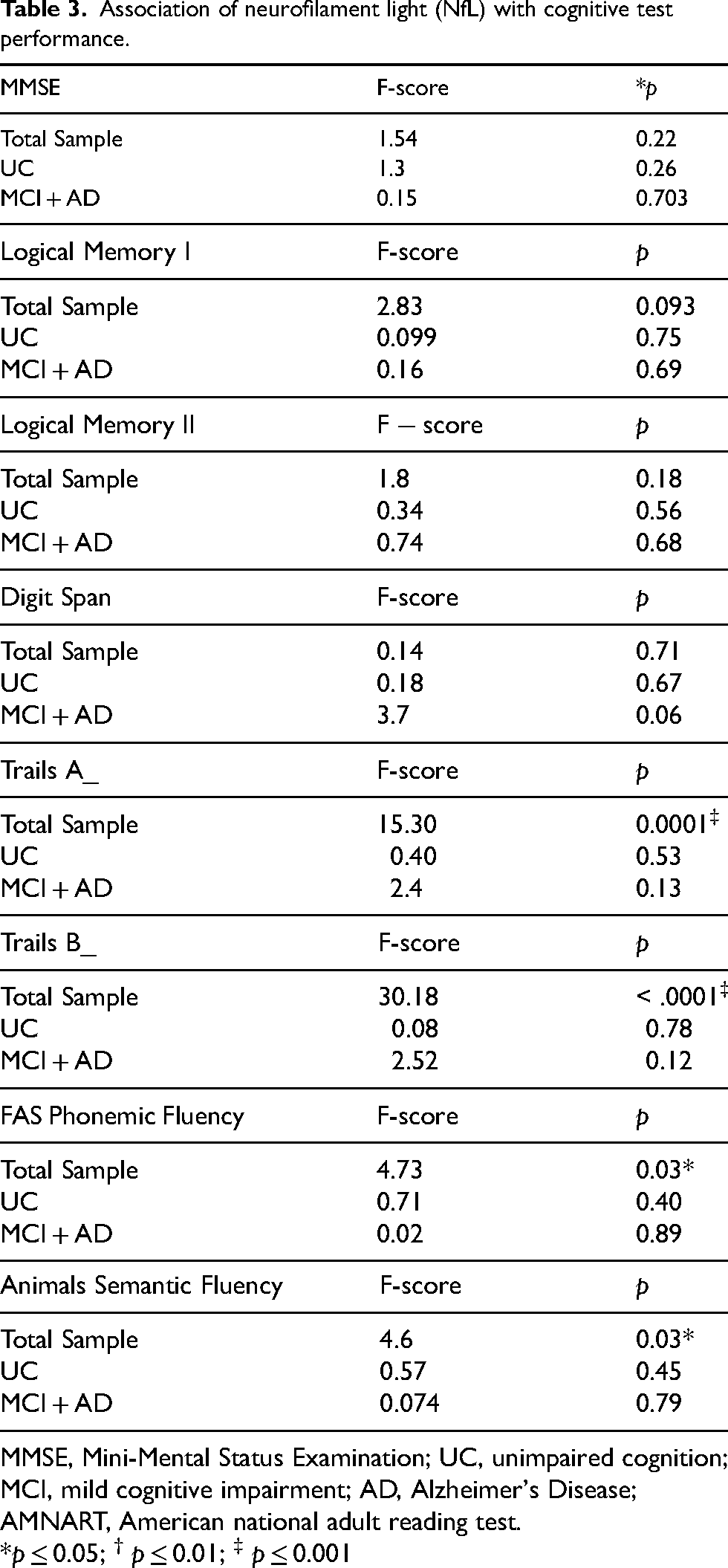
MMSE, Mini-Mental Status Examination; UC, unimpaired cognition; MCI, mild cognitive impairment; AD, Alzheimer's Disease; AMNART, American national adult reading test.
*p ≤ 0.05; † p ≤ 0.01; ‡ p ≤ 0.001

MMSE, Mini-Mental Status Examination; UC, unimpaired cognition; MCI, mild cognitive impairment; AD, Alzheimer's Disease; AMNART, American national adult reading test.
p ≤ 0.05
Nfl levels in relation to neuropsychological test performance by diagnostic group
Once separated by diagnostic groups, UC and MCI + AD, most significant associations were removed. There was a singular significant association of NfL with word reading for those classified as UC (p < 0.05).
Discussion
The present work reflects a study of the link between plasma NfL values and cognitive outcomes among a community-dwelling, cross-sectional cohort of non-Hispanic Blacks (NHB). The NfL values reported in the current study are similar to previously published reports on a smaller sample (n = 142) of NHB from the HAB-HD cohort. 31 The results support previous findings that show different racial/ethnic groups have various average values of NfL, and that NHB may experience lower levels of NfL on average when compared to non-Hispanic Whites (NHW).19,32 Emerging research supports that ethno-racial diversity may influence biomarker outcomes. In a study examining annualized rate of change over a 5-year follow-up, NfL was associated with a faster decline in normed mental status scores among White participants only. 32 Additionally, recent studies indicate that models predicting brain amyloidosis using NfL may yield inconsistent results across ethno-racial groups, potentially leading to disproportionate misdiagnosis in African Americans (AA). 33
Possible explanations for ethno-racial variation in biomarker values may be partially explained by medical comorbidities. A previous report leveraging HABS-HD data on NHW and HW participants, demonstrated that ethnicity and diabetes was associated with higher Aβ40 (p < 0.001), Aβ42 (p < 0.001), total tau (p < 0.001), and NfL (p < 0.001). 34 This relationship has not been explored in NHB populations, necessitating further investigation into other plasma AD biomarkers and clinical utility among diverse groups. Racial/ethnic differences in social determinants of health may also explain biomarker differences. In a longitudinal analysis of every day functioning in NHB and NHW older adults, lower levels of economic stability and social context in NHB was related to accelerated decline in every day functioning when compared to NHW. 35 The researchers also note that within-group heterogeneity of social determinants of health (SDOH) in NHB communities contributes to differences in plasma NfL, where low resource/high stress phenotypes are positively associated with NfL. This relationship has been similarly elucidated in HD patients, where higher NfL was associated with smaller social network size and diversity. 36
To date, this is the largest cross-sectional examination of biomarkers and cognitive outcomes among community-dwelling non-Hispanic Blacks. Across the entire sample, plasma NfL showed associations with executive functions of processing speed, attention, working memory, and verbal fluency and generativity. These findings align with previous work demonstrating a link between plasma NfL and neuropsychological functioning.37,38 Specifically, O’Bryant and colleagues 37 identified an inverse association of NfL with global cognitive functioning, working memory, attention, processing speed, verbal fluency, and learning and memory across Mexican American (MA) and non-Hispanic whites (NHW) ethnic groups. When examining NfL associations with neuropsychological across diagnostic classifications and ethnicity, however, O’Bryant and colleagues observed differences, wherein associations diminished for NHW with dementia. In contrast, MA with dementia observed several significant associations. Similarly, Osbourn and colleagues 38 identified negative associations between plasma NfL and cognitive testing of language, executive functioning, visual spatial, and memory for community-dwelling NHW older adults with MCI, with significant associations going away for participants classified as cognitively normal. The current study similarly identified diminished associations when participants were separated by diagnostic group, adding to the breadth of literature supporting the inconsistency of NfL as a specific biomarker of AD.
The lack of association of NfL with cognitive outcomes amongst those with cognitive impairment may be partially explained by sampling, with a large proportion of the participants being CU and having higher education which may buffer against the cognitive effects of NfL. In a cross-sectional examination of cognitive reserve (CR) and brain reserve (BR) on cognition across the AD continuum, it was found that CR, as measured by years of education, had a positive independent effect on attention and executive functioning that was greater for those in predementia than in dementia (β = 0.39 versus β = 0.21 [Welch t = 2.40, p < 0.01] and β = 0.46 versus β = 0.26 [t = 2.83, p < 0.01]). Both high CR and BR were associated with improved cognitive performance. 39 Similarly, Beyer and colleagues (2019), found that higher education buffered against neuronal injury markers, CSF t tau, but that higher reserve resulted in increased accumulation of more pathology and a steeper cognitive decline. 40 The current findings may demonstrate evidence of accumulation of axonal injury and prodromal changes related to AD or non-AD pathogenesis. Taken together, use of NfL as a diagnostic marker is not straightforward due to its differential associations with ethnicity and other factors such as medical comorbidity. 34 The largely executive nature of how NfL associates with cognitive testing in the current analysis may suggest that changes in the larger memory architecture and the coordination of multiple cognitive domains that direct attention and aid in memory retrieval. Further work to identify longitudinally, which baseline NfL levels can predict developmental dementia, and including MRI outcomes of neurodegeneration in NHB is warranted. Such work would facilitate commentary on the utility of NfL diagnostically. Additionally, other markers of neurodegeneration, such as t tau, may be more related to cognitive outcomes in NHB due to the interrelated impact of AD and medical comorbidities (e.g., hypertension) that increase neuroinflammation and risk of progression to AD.41,42
There were no sex effects with NfL. This is consistent with previous studies 43 examining NHW and MA individuals from the HABS-HD, where across the entire sample, differences were noted between men and women for Aβ40 and total tau, while no significant differences were found for NfL. Stratified analysis, however, revealed that MA men (n = 292) exhibited significantly higher NfL values than MA women (n = 561) (p ≤ 0.05). Similar findings regarding the absence of sex differences in plasma NfL levels have been reported in other studies19,44 which predominantly involved homogenous NHW populations. Contrasting results emerge in studies with a larger representation of NHB individuals (56.3% African American, 27.8% below the poverty line), indicating that men, on average, experience a heightened rate of annualized NfL change over 5 years compared to women. 32 This suggests that the demographic composition of cohorts may moderate the association between NfL levels and sex.
Limitations and future directions
Limitations of the current findings include the cross-sectional design precluding inferences about causality. Generalizability is also restricted, with a large percentage of participants having post-secondary education and unimpaired cognition. Moreover, diagnostic classifications are based on clinical criteria rather than imaging biomarkers. Lastly, the effect of specific medical co-morbidities on plasma NfL levels was unexplored. Despite these limitations, the current work offers an initial understanding of the relationship of AD biomarkers with cognitive outcomes in community-dwelling non-Hispanic Blacks. Further research, utilizing longitudinal models, imaging biomarker data, and considering sociocultural impacts on biological factors could further clarify how plasma biomarkers, like NfL, relate to the cognitive trajectory in AD among Black Americans. Examining specific sub-populations within this racial/ethnic group, such as those with intellectual disabilities, and those with varying levels of support resources and distress is crucial for inclusive medical research and for understanding how variations in baseline functioning impact AD biomarker presentation and disease progression.
Footnotes
Acknowledgments
Research reported here was supported by the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The research team thanks the local Fort Worth community and participants of the HABS-HD study.
Author contributions
Lubnaa Abdullah (Conceptualization; Writing—original draft; Writing—review & editing); Fan Zhang (Formal analysis; Writing—review & editing); James Hall (Conceptualization; Writing—review & editing); Sid O'Bryant (Conceptualization; Funding acquisition; Investigation; Methodology).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HABS-HD project is funded by grants from the National Institute on Aging (NIA): R01AG054073, R01AG058533.
Declaration of conflicting interests
Sid O'Bryant is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review. All other authors have no conflict of interest to report.