
Abstract
Background:
Examination of Alzheimer’s disease (AD) related biomarkers among diverse communities has remained limited.
Objective:
The aim of this study was to expand on prior work to provide a characterization of ptau181 among a diverse community sample. Consideration was taken regarding the impact of comorbidities on ptau181 levels including medical.
Methods:
3,228 (n = 770 African American [AA], n = 1,231 Hispanic, and n = 1,227 non-Hispanic white [NHW]) Health and Aging Brain Study- Health Disparities (HABS-HD) participants were included in this study. ANCOVAs were conducted to examine differences in ptau181 levels across race and ethnic groups. Violin plots were also generated stratified by APOE ɛ4 carrier status, Amyloid PET positivity status, medical comorbidity (hypertension, dyslipidemia, chronic kidney disease [CKD], and diabetes) and by cognitive diagnosis.
Results:
Ptau181 levels were found to differ between Hispanics and NHW after covarying for age, sex, and APOE ɛ4 status. Amyloid PET positivity was associated with higher ptau181 levels across all groups. APOE ɛ4 positivity status was only significantly associated with ptau181 levels among AAs. Across all race and ethnic groups, those with a diagnosis of CKD had higher levels of ptau181. When stratified by cognitive diagnosis, cognitively unimpaired Hispanics had higher ptau181 if they also had a diagnosis of CKD or diabetes. p-values ≤0.01.
Conclusions:
Differences in ptau181 levels were shown in a diverse community sample. Medical comorbidities had a differing effect on ptau181 levels particularly among Hispanics even without cognitive impairment. Findings support the need for future work to consider comorbid conditions when examining the utility of ptau181.
INTRODUCTION
The field of blood-based biomarkers has continued to advance at an incredible pace, partly to meet the growing demands of the aging field and provide reliable, cost-effective, and minimally invasive diagnostic options. The commercialization of particular proteins, including phosphorylated tau, has allowed researchers across the globe to examine the effectiveness of such biomarkers in the application of disease detection. Several studies have investigated the utility of particular phosphorylated tau isoforms, including phosphorylated tau at threonine 181 (ptau181).1 –6 However, as has been the case across many studies examining blood-based biomarkers, this work has primarily been conducted on samples reflective of the population’s non-Hispanic white (NHW) segment.
Among the studies on ptau181, a consensus of findings supports its higher levels among individuals with Alzheimer’s disease (AD) as compared to those cognitively unimpaired (CU),4,6,7 , 4,6,7 as well as between those with mild cognitive impairment (MCI) as compared again to those diagnosed as CU.6,7, 6,7 Research also supports ptau181 as an informative biomarker for disease progression from MCI to AD. 1 Moreover, elevations in ptau181 have been linked to amyloid-β (Aβ) PET status across diagnostic groups, including CU, MCI, and AD. 7 In several studies, individuals identified as Aβ PET positive (as compared to negative) had higher ptau181 levels.1,3,5,7–10 , 1,3,5,7–10 Even after adjusting for demographic factors (i.e., age, sex, and APOE ɛ4 status), ptau181 levels were found to be over 50% higher among Aβ PET positive cases than negative. 1 This highlights the potential for ptau181 to serve as a biomarker for AD disease progression and its relevance in clinical settings.
Recent work has examined several demographic and medical factors in their relationship with ptau181. One study investigating sex differences found ptau181 levels to be significantly higher among males than females. 11 APOE ɛ4 carriers also had higher ptau181 levels than non-carriers.5,12, 5,12 Several studies have also found differences in ptau181 levels among those with the medical condition of chronic kidney disease (CKD), with higher levels found among those with the condition.1,11, 1,11 Other medical conditions reported in the literature, such as hypertension and diabetes, were not found to have a relationship with ptau181, despite higher rates reported in the sample for African Americans (AA) as compared to NHWs. 11
As stated previously, most of the work examining the application of ptau181 has been conducted among NHWs, with only a few studies examining this biomarker among racial and ethnically diverse populations. The findings varied; some indicated differences, 8 while others reported no difference in ptau181 levels across race and ethnic groups.5,11,13 , 5,11,13 In some cases, while no significant interaction was found for ethnicity, differences in odds were still reported, as was the case with Asken and colleagues, 6 who saw in their sample (57% Hispanic) that those who self-identified as Hispanic with a diagnosis of MCI (amnestic subtype) had a lower odds (odds ratio = 0.41) of elevated ptau181 levels as compared to NHWs of the same diagnostic group. Additionally, Windon and colleagues 13 also found a trend toward significance with lower levels of ptau181 among Latinos (n = 43) compared to NHWs (n = 129). Ramanan and colleagues in their study 11 found that despite finding no overall difference in plasma AD biomarkers (including ptau181) between their sample of AAs (n = 267) and NHWs (n = 268), a moderate interaction was found between ptau181 and cognition with a stronger association among NHWs as compared to AAs; however, this effect did not hold once the medical condition of CKD was accounted for.
One study with focused community recruitment seeking to reflect a representative clinical trial cohort (Bio-Hermes Study) found ptau181 levels to be lower among those who self-identified as AA as compared to NHW. 8 A finding that held, including with the covariates of age, sex, education, and Mini-Mental State Examination performance. 8 Interestingly, no difference in ptau181 levels was observed in their sample between those who self-identified as Hispanic ethnicity as compared to NHW. Given the discrepancy in findings and minimal work conducted among diverse communities, this study sought to expand on prior work and provide a characterization of ptau181 among a community-dwelling sample of AAs, Hispanics, and NHWs to enhance the understanding and potential interplay between ptau181 and comorbidities. We hypothesize that differences in ptau181 levels exist across certain race and ethnic groups and that comorbid factors impact this relationship.
METHODS
Participants
Participants in this study included those enrolled in the Health and Aging Brain Study- Health Disparities (HABS-HD) with available requisite data. HABS-HD is a community-based study of aging focused on the diverse recruitment of AA, Hispanic, and NHW participants. Inclusion criteria for the study involve individuals who self-report as AA, Hispanic, or NHW race and ethnicity, age 30 and above, able to undergo study procedures including clinical interview, neuropsychological testing, neuroimaging, and blood draw, and fluent in English or Spanish. Study exclusion criteria include having type 1 diabetes, presence of an active infection, recent/current diagnosis of cancer (12 months), current severe mental illness, recent traumatic brain injury with loss of consciousness, current or recent alcohol or substance abuse, an active severe medical condition that could impact cognitive functioning, and current diagnosis of non-AD related dementia.
The HABS-HD clinical interview includes the collection of demographic information such as age, sex, education, self-report of race and ethnicity, and medical history. An informant interview is also collected as part of the study protocol, and the Clinical Dementia Rating (CDR) scale is utilized.14,15, 14,15 Participants complete a neuropsychological test battery, previously published, 16 which is used along with the CDR to assist with diagnostic determination. Regarding the determination of medical comorbid conditions (such as CKD, dyslipidemia, hypertension, and diabetes), a medical professional affiliated with the HABS-HD study takes into consideration 1) self-reported medical history (derived through the clinical interview), 2) information obtained during the HABS-HD medical examination, 3) clinical labs, 4) medication list, and 5) objective measures. A research medical diagnosis decision tree was used to assist in determining medical conditions, including conditions such as dyslipidemia, hypertension, and diabetes (see Supplementary Table 1). CKD for this study was determined based on clinical labs and defined as eGFR levels < 60. Of note, only the medical comorbid conditions of CKD, dyslipidemia, hypertension, and diabetes were selected for evaluation in this study as 1) these represent the most prevalent medical conditions among the sample population and 2) based on prior research that indicated associated findings with select conditions (such as CKD). All components of the study protocol are conducted under Institutional Review Board approval, and each participant (and/or legal guardian) provided written informed consent for study participation.
Cognitive diagnosis
A diagnosis of CU, MCI, and dementia is completed through a consensus review process as previously published. 16 Briefly, data derived from self and informant reports of daily functioning and results from neuropsychological testing were considered. Of note, neuroimaging data was not utilized to determine cognitive diagnosis. All diagnostic determinations were made by a dementia expert associated with the HABS-HD study. A diagnosis of CU is made when there is no complaint of cognitive change by self or others, a CDR sum of boxes score of 0, and neuropsychological test performance that falls broadly within normal ranges. A diagnosis of MCI is made when there is a report of cognitive change either by self or informant, a CDR sum of boxes score of 0.5–2.0, and having at least one neuropsychological test performance that falls at or below one and a half standard deviations from the mean. A diagnosis of dementia is made when there is a complaint of cognitive change by self or others, a CDR sum of boxes score of≥2.5, and neuropsychological test performance that falls at or below two standard deviations from the mean on two or more tests.
Neuroimaging
The HABS-HD neuroimaging protocol is aligned with that of ADNI3 (available at https://adni.loni.usc.edu/methods/pet-analysis-method/pet-analysis/). Amyloid positron emission tomography (PET) scans were obtained using Siemens Biograph Vision 450 whole-body PET/computed tomography (CT) scanners. The amyloid scans were completed using the florbetaben (FBB) tracer (8.1 mCi, 4 x 5 min frames, 90 min post-injection) with standardized uptake value ratios (SUVR) determined at the University of Southern California Stevens Neuroimaging and Informative Institute using ROIs derived from FreeSurfer with the cerebellum as a reference. Amyloid PET positivity was determined based on a global SUVR > 1.08.16,17, 16,17
Ptau181
Fasting blood samples were collected as part of the HABS-HD protocol and processed in accordance with the international guidelines for AD biomarker studies. 18 The Single Molecule Array (Simoa) Human ptau181 V2 kit was used to quantitatively determine the amount of ptau181 in human plasma. Several tests were performed to optimize dilution factors and centrifugation. Based on these tests, it was found that the suggested dilution factor of 4× for plasma was suitable for the samples. After thawing, the samples were vortexed and spun at ∼2,500 for 15 min; the supernatant was directly transferred to a clean 96 deep well plate. From the materials provided, a recombinant ptau181 calibration curve was constructed and transferred to the 96 well plate (240μL per well). Calibration range was 0–106 pg/mL and the dynamic range was 0–424 pg/mL. Analog (high control) of 89.3–134 pg/mL and digital (low control) of 2.5–3.82 pg/mL were made and added to control wells. An inter-assay control of normal pooled plasma was included. All controls were run in duplicate (125μL per well).
The neat samples (65μL for singlet or 90μL for duplicate) were then diluted onboard by the Simoa HD-X analyzer. Utilizing a 2-step procedure in a reaction cuvette samples were incubated with antibody coated paramagnetic beads and the biotinylated detector antibody simultaneously. After a wash, streptavidin-conjugated β-galactosidase (SBG) reagent was added. SBG binds the biotinylated antibodies leading to enzyme labeling of ptau181. After a final wash, the beads are re-suspended in resorufin β–D-galactopyranoside (RGP) reagent. The beads were then transferred to a Simoa disc array and sealed with oil for imaging. If ptau181 is present in the sample, it will be captured and labeled on the bead; the SBG reagent hydrolyzed the RGP substrate to produce a signal. The fluorescent signal values from prepared calibration curve are fit using a 4-parameter logistic curve and 1/y2 weighting. The sample and control concentrations were calculated from 4PL curve fit. Lower Limit of Detection was reported at 0.028 pg/mL, Analytical Lower Limit of Quantification at 0.085 pg/mL and Functional (plasma) Lower Limit of Quantification at 0.338 pg/mL.
APOE genotyping
APOE genotyping was performed using commercially available TaqMan Genotyping kits for the two determining SNPs, rs429158 and rs7412. Amplification was conducted using TaqMan GTXpress Master Mix (ThermoFisher). The individual SNP genotypes were assessed using the 7500 Real-Time PCR System (Applied Biosystems) under the manufacturer’s suggested thermal cycling parameters. APOE genotypes were called according to combined of allele amplification results at the two SNPs as follows (rs429358, rs7412): ɛ2/ɛ2–T,T; ɛ2/ɛ3–T,CT; ɛ2/ɛ4–CT,CT; ɛ3/ɛ3–T,C; ɛ3/ɛ4–CT,C; ɛ4/ɛ4–C,C. Positive controls (individuals of known, independently typed APOE genotypes) and negative controls were included on all runs.
Statistical analysis
Statistical analyses were conducted using R (V4.3.3). A total of n = 3,228 participants from HABS-HD were included with available data (n = 770 AA, n = 1,231 Hispanic, n = 1,227 NHW). Percentages as well as means and standard deviations were derived for the sample demographic characteristics, including age, sex, education, APOE ɛ4 status, cognitive diagnosis, and select medical comorbid conditions for the overall sample and by race and ethnic group. A two-sample Student’s t-test was performed to compare the means of each pair of groups. ANCOVAs were conducted to examine group differences. Covariates included age, sex, and APOE ɛ4 in models as indicated. Violin plots (with noted significance levels) were derived to examine differences in ptau181 levels across race and ethnic groups. Additional violin plots were generated by race and ethnic group to examine differences in Aβ PET positivity status (yes/no), APOE ɛ4 positivity status (yes/no), APOE ɛ4 positivity status stratified by cognitive diagnosis (CU, MCI, dementia), medical condition (CKD, dyslipidemia, hypertension, and diabetes), and medical condition stratified by cognitive diagnosis. The resulting p-values were adjusted using Bonferroni correction to account for multiple comparisons. Support vector machine (SVM) models were further conducted to see how well ptau181 could distinguish cognitive diagnosis (i.e., CU versus MCI and dementia) for the total sample and by race and ethnic group. Significance was set at p < 0.05.
RESULTS
When examining the demographic characteristics of the sample (see Table 1), NHWs were shown to be older and have higher levels of education than AAs and Hispanics. No difference was found in APOE ɛ4 positivity rates between Hispanics and NHWs in the sample, while a difference was found between AAs (39%) and both Hispanics (24%) and NHWs (25%). Regarding medical conditions, rates were higher among AAs across conditions examined (dyslipidemia, hypertension, and diabetes) as compared to Hispanics and NHWs. A medical condition of CKD was also found to differ in rates across race and ethnic groups, with NHWs presenting with a higher percentage (15%) as compared to either AAs (13%) or Hispanics (8%). Cognitive diagnosis was also found to be significantly different across groups, with AAs having higher rates of MCI (31% AA, 20% Hispanic, 13% NHW) and dementia (8.2% AA, 6.7% Hispanic, 5.9% NHW) as compared to Hispanics and NHWs.
Demographic characteristics
CKD, chronic kidney disease; Significance group difference between racial/ethnic groups: aAA versus Hispanic; bAA versus NHW, cHispanic versus NHW; Significance is set at p < 0.05.
Age was found to be significantly associated with ptau181 levels (p < 0.001). After adjusting for age, sex, and APOE ɛ4 status, a significant difference was found in ptau181 levels between Hispanics and NHWs (see Fig. 1). Of note, Cohen’s d was 0.339, indicating a small effect size. When stratified by Aβ PET positivity status (yes/no) and adjusting for age and sex, a significant difference was found within each race and ethnic group between those classified as Aβ PET positive as compared to Aβ PET negative (see Fig. 2). Interestingly, no significant difference was found in ptau181 levels across race and ethnic groups in those who were Aβ PET positive as compared to Aβ PET negative (p = 0.81 between AA and Hispanic; p = 0.92 between AA and NHW; p = 0.77 between Hispanic and NHW).
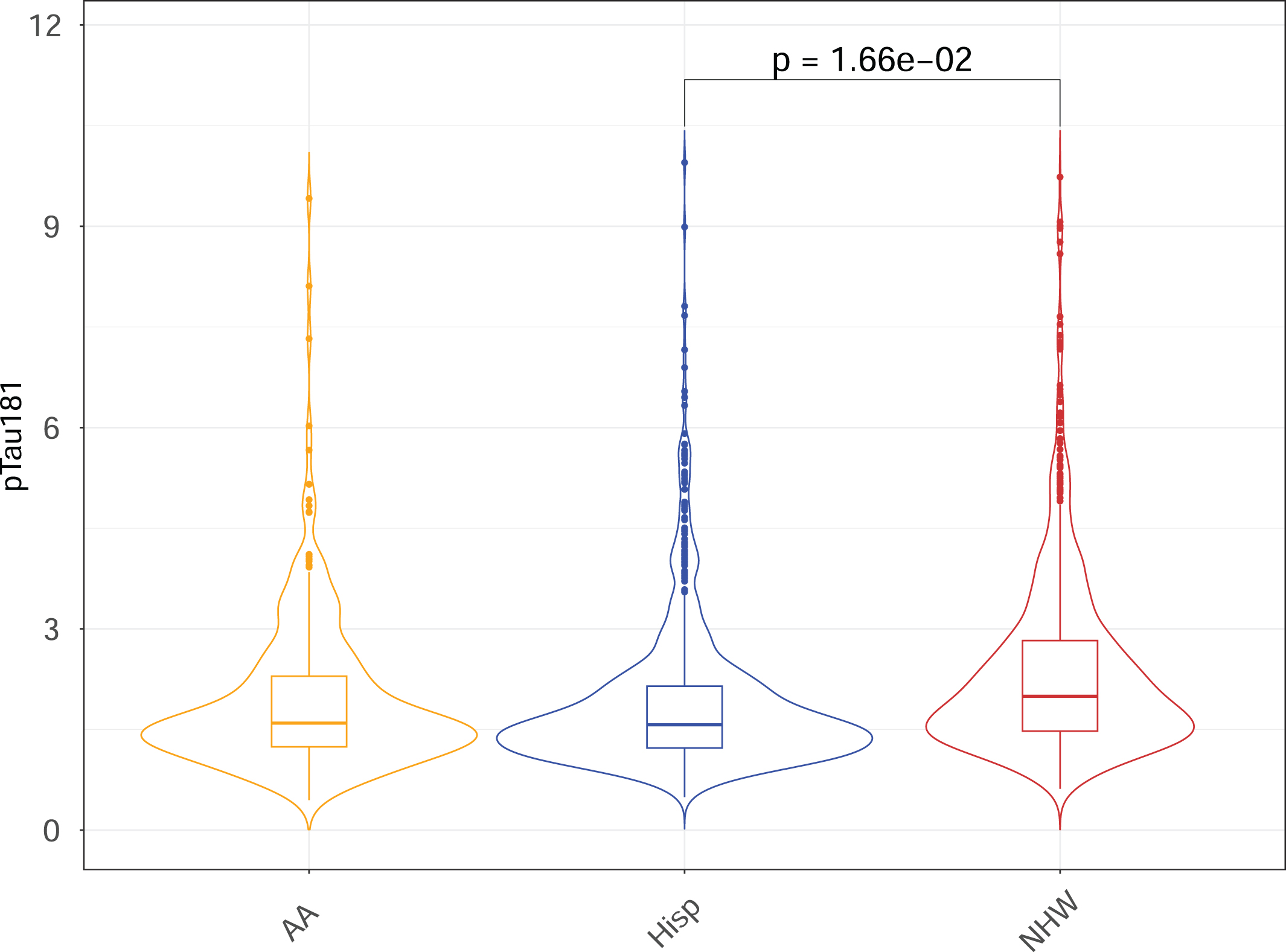
Violin plot for plasma ptau181 levels across racial and ethnic groups with age, sex, and APOE4 as covariates.
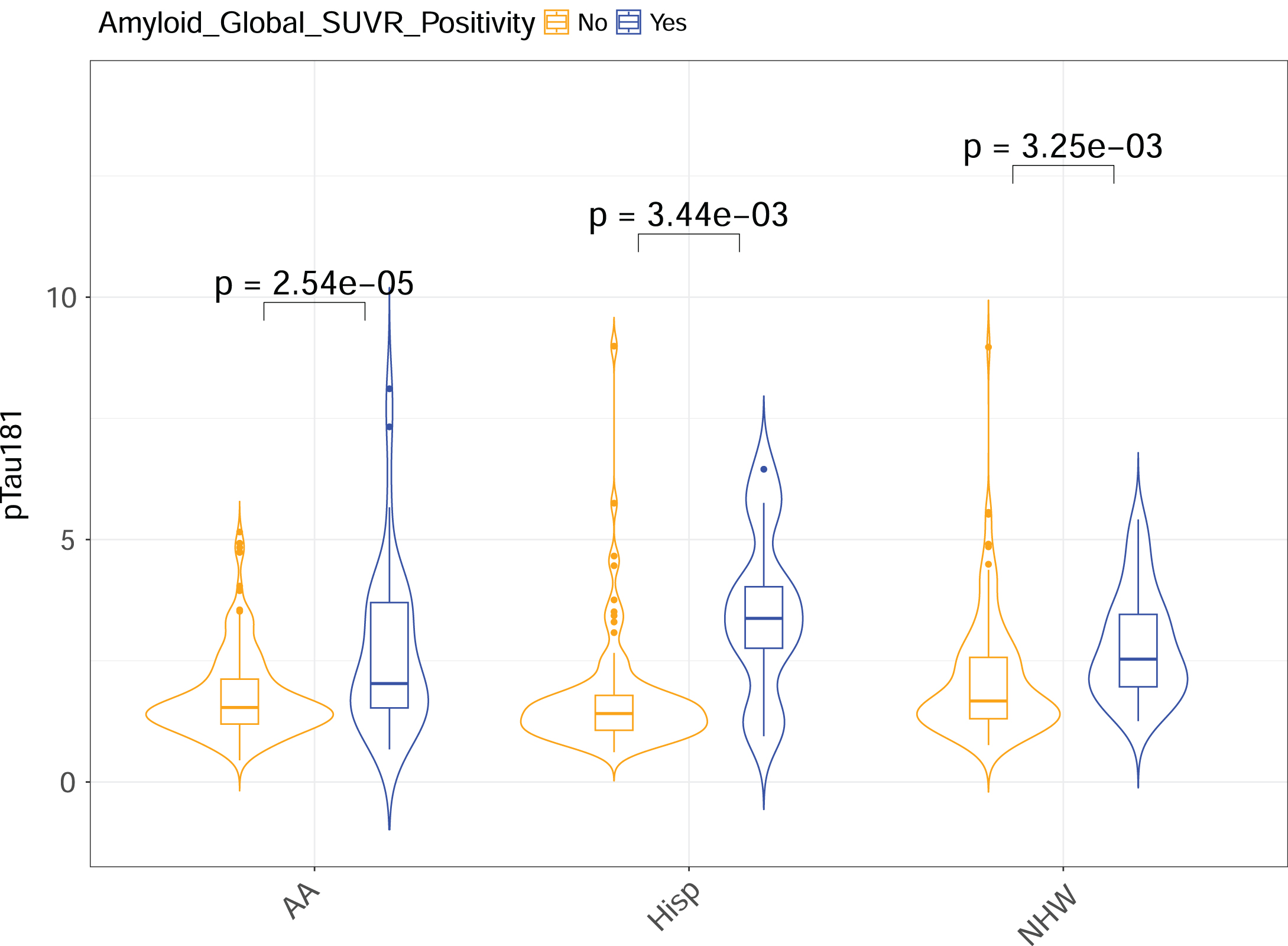
Violin plot for plasma ptau181 levels between Amyloid-Beta (Aβ) PET positivity status (yes/no) (with age and sex as covariates) split by race and ethnic group.
When separated by APOE ɛ4 status (adjusting for age and sex), the only significant difference in ptau181 levels was found between AAs who were APOE ɛ4 positive (ɛ4/ɛ4 or ɛ3/ɛ4) versus negative. Once further stratified by cognitive diagnosis (again adjusting for age and sex), the observed difference was shown for AAs who were diagnosed as MCI. Interestingly, a similar significant difference stratified by APOE ɛ4 status was also shown for Hispanics with the same diagnosis (See Fig. 3).
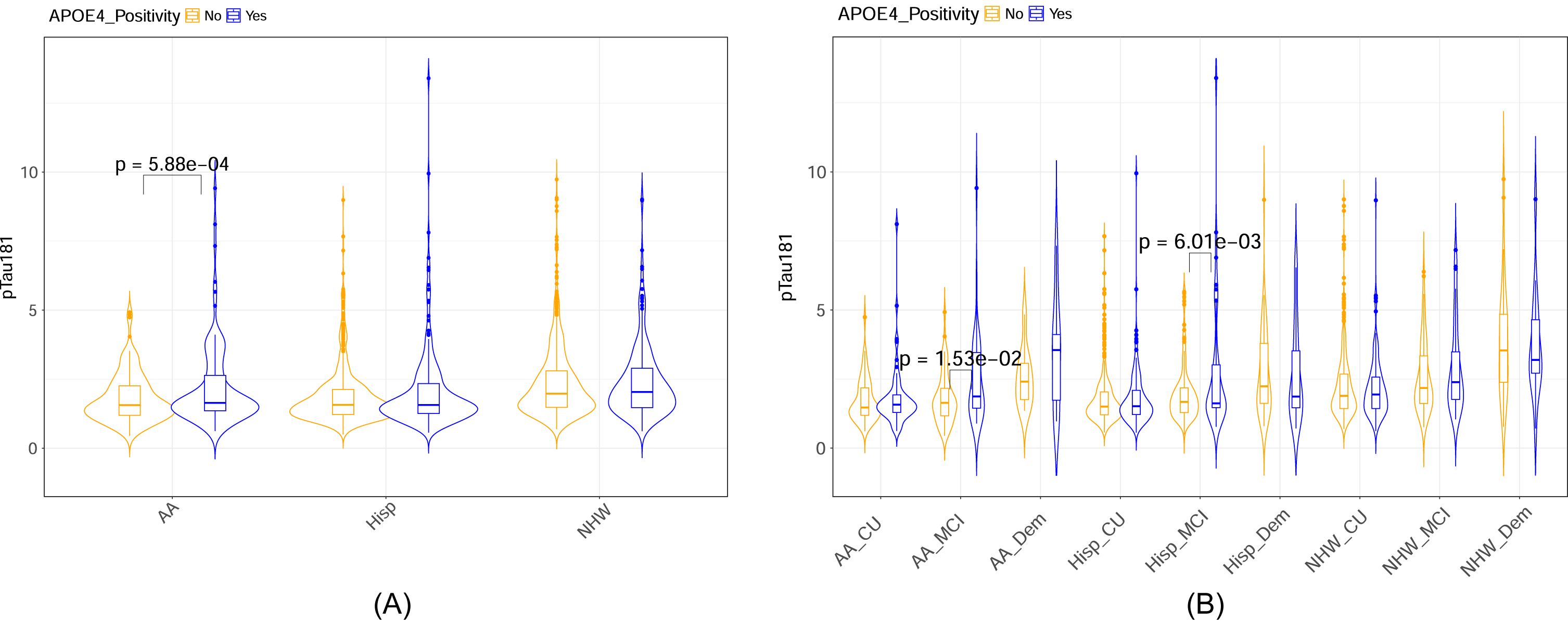
Violin plot for plasma ptau181 levels between APOE ɛ4 positivity status (yes/no) (with age and sex as covariates) split by a) race and ethnic group and b) race and ethnic group and cognitive diagnosis.
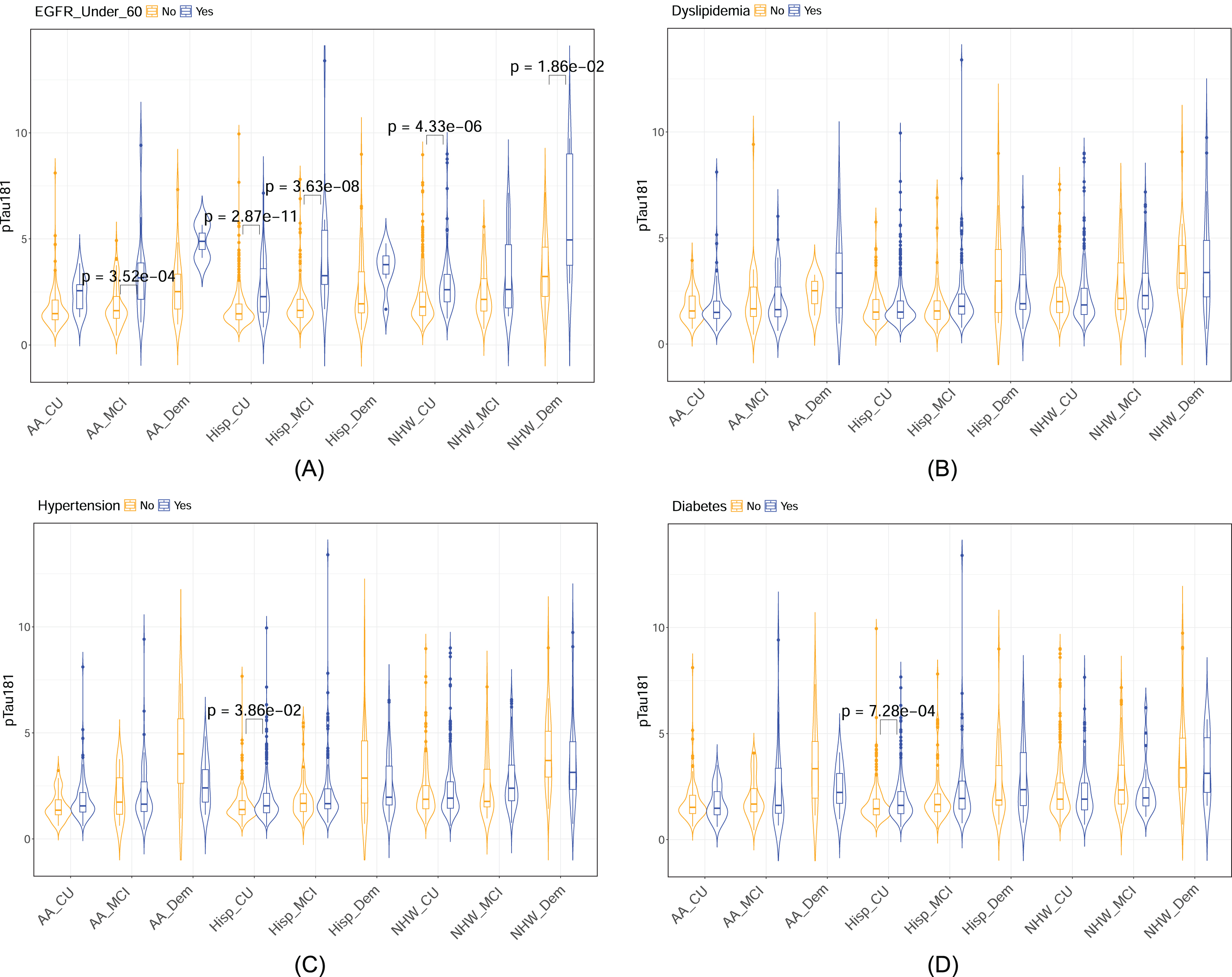
The medical conditions of CKD, dyslipidemia, hypertension, and diabetes revealed condition-specific findings after adjusting for age and sex (see Fig. 4). When examining those with CKD, significant differences were found in ptau181 levels across all race and ethnic groups, with higher levels found among those with the condition versus those without. For diabetes, the only significant difference found was among Hispanics with higher levels of ptau181 identified for those with the medical condition. No significant finding was revealed for the medical conditions of hypertension or dyslipidemia.
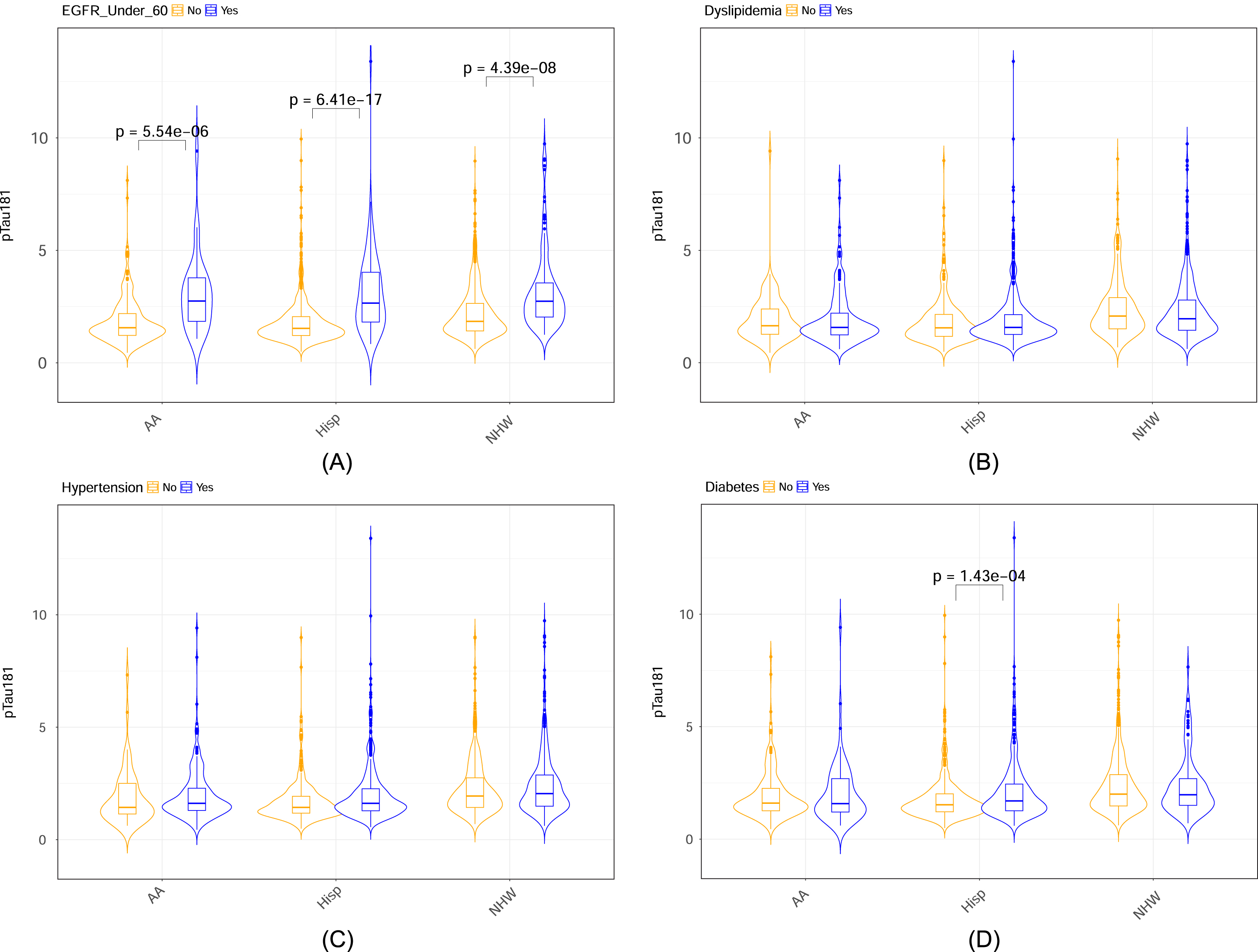
Violin plot for plasma ptau181 levels separated by medical condition a) chronic kidney disease (defined as eGFR < 60), b) dyslipidemia, c) hypertension, d) diabetes and racial and ethnic group (with age and sex as covariates).
When separated by both medical condition and cognitive diagnosis (CU, MCI, dementia), specific findings were revealed per race and ethnic group additionally once adjusting for age and sex (see Fig. 5). The stratified analyses indicated that Hispanics with either a diagnosis of CU or MCI had higher ptau181 levels if they also had CKD. A similar finding was revealed among NHWs with a diagnosis of CU as well as those with a diagnosis of dementia, with higher ptau181 levels found among those also with CKD. Among AAs, the only diagnostic stratified finding was among MCI, with higher ptau181 levels found among those with CKD. Regarding the medical conditions of hypertension and diabetes, the only significant finding was identified again among Hispanics with a diagnosis of CU, as higher ptau181 levels were found among those with the medical conditions.
Violin plot for plasma ptau181 levels separated by medical condition a) chronic kidney disease (defined as eGFR > 60), b) dyslipidemia, c) hypertension, and d) diabetes as well as by cognitive diagnosis (Cognitively Unimpaired [CU], Mild Cognitive Impairment [MCI], Dementia) and race and ethnic group (with age and sex as covariates).
Additional analyses were conducted to examine the application of ptau181 in distinguishing between cognitive diagnostic status for the total sample and by race and ethnic group. In the total sample, ptau181 (along with age and sex) produced an area under the curve (AUC) of 0.66, sensitivity (SN) of 0.59, and specificity (SP) of 0.66 in distinguishing CU from MCI/Dementia. When split by race and ethnic group, the model was relatively similar for AAs and Hispanics with AUCs of 0.69 (AAs SN = 0.62, SP = 0.70; Hispanics SN = 0.84, SP = 0.38), while the AUC was higher for NHWs and reached 0.72 with a SN of 0.68 and SP of 0.66.
DISCUSSION
Results of this study revealed that differences in the AD biomarker of ptau181 did exist across the race and ethnic groups examined as hypothesized. NHWs were found to have higher ptau181 levels than Hispanics, while no differences were observed between the diverse segments of the HABS-HD cohort (AAs and Hispanics) in their mean levels (once adjusting for factors such as age, sex, and APOE ɛ4 status). This work also revealed that ptau181 could distinguish Aβ PET positivity status across race and ethnic groups. While differences existed in rates of APOE ɛ4 positivity across groups, a significant relationship between ptau181 and APOE ɛ4 was only found among AAs. This finding held, including once stratified by cognitive diagnosis, which revealed a significant relationship for AAs diagnosed as MCI.
Our study found that the link between ptau181 and certain medical conditions was more impactful, primarily among diverse communities. When stratified by cognitive diagnostic status, we found a similar indication when examining the link between ptau181 and medical comorbidities. An example of this was shown for Hispanics with a CU diagnosis, as a significant difference was found in ptau181 levels for those with versus without medical conditions of hypertension, diabetes, and CKD, thus pointing toward potential points of therapeutic consideration. Although Hispanics presented overall in our study with the most relationships between ptau181 and medical conditions, CKD was shown to be the one condition that impacted all race and ethnic groups alike, with higher levels of ptau181 found for those with versus without the condition. Interestingly, once stratified by cognitive diagnosis, race and ethnic findings were revealed, with Hispanics diagnosed as either CU or MCI showing significant differences in ptau181 levels between those with and without CKD as well as for NHWs with a cognitive diagnosis of CU or dementia. For AAs, the only difference was found for those with an MCI diagnosis.
When placing this into the context of prior work, our findings are consistent with other research conducted among a biracial cohort of AAs and NHWs, which found medical conditions such as CKD to impact ptau181 levels. 11 This work supported that once CKD was included in the modeling, the relationship between ptau181 and cognition was no longer significant. 11 Other work conducted by Lehmann and colleagues 1 found in their sample that CKD, creatinine, and eGFR were all independently associated with ptau181 levels in their Biomarker of AmyLoid pepTide and AlZheimer’s diseAse Risk (BALT-AZAR) cohort. From this work, examining their sample of MCI who converted to dementia, the suggestion was made that renal function should be taken into consideration when utilizing ptau181 in diagnostic models. 1
Our study also found a similar link between CKD and ptau181 levels and that certain stages in the AD disease progression were more impacted by whether you did or did not have this medical condition. Mainly, our findings support a more significant impact among those still in the CU stage for medical conditions for certain race and ethnic groups such as Hispanics and NHWs. Models that utilize ptau181 to predict diagnostic states have found that ptau181 levels are higher among those with AD Dementia who are Aβ PET positive and even those in the preclinical stage of AD (CU who are Aβ PET positive). 7 Studies applying ptau181 in the detection of Aβ PET positivity have reached a detection range of 0.825,6,8 , 5,6,8 to 0.93. 9 One study conducted by Janelidze and colleagues to examine different ptau181 assays found a similar range in AUCs from 0.83–0.84 in predicting both Aβ PET status (positive/negative) and in predicting progression from MCI to AD between both the Mass Spec Lilly Research Laboratory (Lilly-WashU) ptau181 and ADxNeuroscience ptau181. 2 Of note, SVM analyses from this study (utilizing a Quanterix ptau181 assay kit) produced slightly lower AUCs than previously reported with findings ranging from 0.72 for NHW to 0.69 for both Hispanic and AAs, with the covariates of age and sex. Although other ptau isoforms (ex. ptau217) have, in general, shown higher diagnostic accuracy in this work with AUCs reaching as high as 0.93–0.94 (for predicting Aβ PET positivity and disease progression), 2 the relatively close range of AUCs for ptau181 suggests that it is a viable marker even across differing commercially available vendors.
Work conducted with expanded models that included ptau181 and other AD biomarkers, demographics, and APOE ɛ4 status revealed higher AUCs in predicting Aβ PET positivity (AUC 0.86–0.88 10 ; AUC 0.84 1 ). However, none of this work further stratified by medical comorbidities despite this same work 1 implicating that conditions such as CKD can impact AD biomarkers and thus could lead to potential diagnostic errors if not modeled accordingly. Additionally, limited work has examined ptau181 and its diagnostic capabilities across race and ethnic groups, including AAs, Hispanics, and NHWs. Our work suggests that models examining biomarkers, such as ptau181, should further consider medical comorbidities, particularly when applied to diverse communities.
There are several limitations to this study. One is the cross-sectional nature of the analyses that limits the implications of looking at the long-term effect of medical conditions on ptau181 levels. In addition, sample size per race and ethnic group did not allow for further stratified analyses to be conducted at this time (i.e., medical condition by amyloid status); however, future work is planned to examine the interplay of multiple comorbid factors/conditions once sample sizes are appropriate to do so. Additionally, this study utilized self-reports of race and ethnic groups compared to genetically determined ancestry. Of note, a vast majority of Hispanic participants self-reported as being of Mexican American origin, which limits generalizability when applying these findings to other Hispanic subgroups. This study’s strengths include a robust community-derived sample of AAs, Hispanics, and NHWs with available AD biomarker data. This work contributes to our understanding of potential factors that impact AD biomarkers among diverse communities and how consideration should be provided for factors such as comorbid medical conditions. Future work is planned to model the implications that conditions have for diverse communities on disease detection and progression, in addition to how sociocultural differences such as socioeconomic status could impact the identified relationship and findings from this work.
Lastly, while ongoing efforts are underway to characterize additional AD biomarkers in the HABS-HD study, this study sought to investigate ptau181 and provide an initial step in the characterization of this biomarker across different race and ethnic groups. Findings from this study highlight important considerations for applying and using ptau181 among diverse populations. The impact of factors such as APOE ɛ4 status, cognitive diagnosis, and medical conditions reflect the complexity of the AD disease process and implicates several modifiable targets for future consideration.
AUTHOR CONTRIBUTIONS
Melissa Petersen (Conceptualization; Formal analysis; Methodology; Writing – original draft); Fan Zhang (Conceptualization; Formal analysis; Methodology; Writing – original draft); James R. Hall (Conceptualization; Formal analysis; Methodology; Writing – original draft); David Julovich (Formal analysis; Methodology; Writing – review & editing); Robert A. Rissman (Conceptualization; Formal analysis; Methodology; Writing – review & editing); Karin L. Meeker (Conceptualization; Formal analysis; Methodology; Writing – review & editing); Nicole Phillips (Formal analysis; Methodology; Writing – review & editing); Stephanie Large (Formal analysis; Methodology; Writing – review & editing); Beau M. Ances (Conceptualization; Formal analysis; Methodology; Writing – review & editing); Sid E. O’Bryant (Conceptualization; Formal analysis; Funding acquisition; Methodology; Supervision; Writing – original draft).
Footnotes
ACKNOWLEDGMENTS
HABS-HD MPI Team: Sid O’Bryant, Kristine Yaffe, Arthur Toga, Leigh Johnson, and Robert Rissman. HABS-HD Investigators: Meredith Braskie, Kevin King, James R. Hall, Melissa Petersen, Raymond Palmer, Robert Barber, Yonggang Shi, Fan Zhang, Rajesh Nandy, Roderick McColl, David Mason, Bradley Christian, Nicole Phillips, Stephanie Large, and Rocky Vig.
FUNDING
Research reported in this presentation was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers R01AG054073 and R01AG058533, P41EB015922 and U19AG078109. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors would like to thank the Health and Aging Brain Study- Health Disparities (HABS-HD) research team and participants.
CONFLICT OF INTEREST
Sid E. O’Bryant has multiple patents pending related to precision medicine technologies for neurodegenerative diseases. He is the founding scientist of Cx Precision Medicine and has served on an Advisory Board for Roche Diagnostics. All other authors have nothing to disclose. Fan Zhang, Robert A. Rissman, Nicole Phillips, and Sid E. O’Bryant are all Associate Editors of this journal; however, none of the authors listed were involved in the peer-review process of this article nor had access to any information regarding its peer-review.