
Abstract
Background
Addressing modifiable risk factors such as physical inactivity and social isolation could reduce risk of Alzheimer's disease and all-cause dementia, but little is known about which factors individuals are most willing to address or how they prefer to address them.
Objective
To examine and describe behavior change goals set by participants during the Systematic Multi-domain Alzheimer's Risk Reduction Trial (SMARRT).
Methods
In SMARRT, older adults worked with a health coach and nurse over 2 years to set incremental, personalized goals to reduce dementia risk. We performed quantitative analyses to summarize the numbers of goals per risk factor and qualitative content analyses of health coach and nurse notes to describe types of goals and useful strategies.
Results
82 dementia-free adults (70 to 89 years) with at least two dementia risk factors participated in the SMARRT intervention arm (mean age, 76 ± 5 years; 72% women; 11% Black/African American, 4% Asian, 3% Hispanic, 7% another non-White race). Participants set a median of 12 health coach goals and 1 nurse goals. The risk factors participants chose to work on most frequently were physical activity (95%), hypertension (72%), and cognitive activity (60%). Participants reported that the most useful strategies included support and accountability from the health coach/nurse, setting small goals, and learning to manage setbacks.
Conclusions
When given support, older adults at increased risk for dementia set a wide range of goals to reduce dementia risk. A flexible, personalized approach that focuses on setting feasible goals and managing setbacks provides a useful framework for dementia risk reduction.
Keywords
Introduction
There are currently nearly 7 million people in the U.S. and 55 million people worldwide who are living with Alzheimer's disease and related dementias (ADRD), and prevalence is projected to more than double by 2060.1,2 Although several new Alzheimer's disease medications have recently been approved by the U.S. Food and Drug Administration (FDA), they have relatively small effects on cognitive and functional decline, are costly, sometimes have serious side effects, and do not cure the disease.3–5 Therefore, it remains important to study interventions to prevent or delay onset of symptoms.6–8
Several studies have estimated that approximately 40% of ADRD cases may be attributable to modifiable and treatable risk factors, including physical inactivity, low education, hypertension, obesity, diabetes, depression, smoking, head injury, social isolation, hearing loss, high alcohol consumption, and air pollution.7,9,10 However, clinical trials aiming to address modifiable risk factors have had mixed results,11,12 with some studies finding improvements in cognitive function13–21 and others finding no evidence of cognitive benefit.22–29 There remains an overarching question of why some interventions show evidence of effectiveness and others do not.
Most multidomain trials to date have used a highly structured intervention schedule, requiring a uniform set of activities at prescribed times and locations for all participants. While this approach maximizes internal validity, it may be challenging to scale for widespread implementation. In contrast, the Systematic Multidomain Alzheimer's Risk Reduction Trial (SMARRT) study was designed to study a personalized approach to ADRD risk reduction, in which participants chose what they wanted to work on and how, aided by health coaches with expertise in behavior change and medical professionals focused on management of chronic conditions. 30 Our recently completed randomized, controlled trial found that participants in the intervention arm experienced significantly better cognitive function, had improvement in dementia risk factors, and reported better quality of life compared to a health education control group. 21 Therefore, this trial provides “proof of concept” for a personalized approach to ADRD risk reduction that may inform larger trials and provide guidance for patients and professionals seeking to improve cognitive outcomes in older adults.
Given the positive outcomes of the SMARRT study and the flexible, personalized intervention, SMARRT provides a unique opportunity to understand participants’ priorities related to dementia risk reduction. The primary goal of this manuscript is to provide a detailed description of the risk factors participants chose to work on, types of goals set, and barriers and facilitators to behavior change. This in-depth analysis may help guide the development of future interventions by providing insights into participants’ motivations and their perceptions of which behavior change strategies were most helpful.
Methods
Setting
This study took place at Kaiser Permanente Washington (KPWA), an integrated healthcare delivery system that provides members with health insurance and medical care. This study recruited patient participants from 9 clinics in the greater Seattle area between September 2018 and March 2020.
Study participants
Detailed eligibility criteria have been previously published. 30 Inclusion criteria were age 70 to 89 years, English language fluency, enrollment in KPWA for at least 12 months, and two or more risk factors targeted by the intervention. Risk factors counted towards eligibility were poorly controlled hypertension, diabetes with evidence of hyper- or hypoglycemia, depressive symptoms, poor sleep quality, medications potentially harmful to cognition, physical inactivity, social isolation, and current smoking. Poor diet and low cognitive activity were not specifically assessed for enrollment purposes but were included in the intervention as potential risk reduction targets. We excluded individuals who would have limited ability to participate for two years (e.g., receiving hospice care) or evidence of dementia (based on diagnosis codes, medications, or telephone Cognitive Abilities Screening Instrument (CASI) 31 score ≤ 25). Racial and ethnic minority groups (American Indian/Alaska Native, Asian, Black/African American, Hispanic, Native Hawaiian/Pacific Islander) were oversampled during recruitment. Those who enrolled were randomly assigned to the SMARRT intervention group or health education control group. This manuscript focuses on the intervention group.
All study procedures were approved by Institutional Review Boards (IRBs) at KPWA and the University of California, San Francisco (UCSF), and are in accord with the Helsinki Declaration of 1975. The study is registered on ClinicalTrials.gov (NCT03683394). All participants provided written informed consent.
Intervention activities
The SMARRT intervention team included behavioral interventionists (health coaches) and a nurse care manager led by a clinical psychologist (BHB) and supported by an additional clinical psychologist (DER), intervention physician (KA) and other study physicians (EBL, SD). Health coaches had master's degrees in social work or other related fields. The nurse care manager was a registered nurse.
All health coaches and the study nurse were trained in motivational interviewing. 32 The intervention team provided additional risk-factor specific training (e.g., brief cognitive behavioral therapy for insomnia (CBT-I), 33 Problem Solving Therapy (PST) for depression) 34 as well as general refresher training for motivational interviewing. Training boosters were provided as needed. Coaches were also provided with a detailed coaching manual, participant-facing handouts, and recommended resources for each risk factor. The nurse care manager worked closely with the intervention physician to review cases and determine appropriate care responses. The intervention team met weekly initially and later biweekly throughout the study period to present cases and receive feedback and support. A summary of training activities and recommended resources for each risk factor is included in the Supplemental Table 1.
After randomization, initial in-person visits were scheduled with both the assigned health coach and the nurse. Health coaches shared a personalized risk factor profile with each participant and then worked with them to develop an initial personalized risk reduction action plan. Health coaches elicited participants’ values and motivations to reduce dementia risk and used a decisional balance process informed by motivational interviewing and confidence ratings to help participants choose one to three specific, achievable risk reduction steps. Coaches provided participants with tools (e.g., wrist-worn activity monitor, insomnia workbook, etc.; see Supplemental Table 1) to track their progress as needed. At each subsequent visit, coaches reviewed and reinforced participant progress, problem-solved to address barriers, provided additional relevant education and tools, and helped participants set new goals as needed.
At the initial nurse visit, participants were asked to bring all current medications (prescription and over-the-counter [OTC]), and the nurse reviewed them to identify any that were potentially harmful to cognition according to the 2015 Beers criteria 35 (e.g., anticholinergic medications, benzodiazepines). The nurse also worked with participants who had hypertension or diabetes to help ensure their conditions were being well-managed. She reviewed participants’ medical record to screen for recent blood pressure (BP) and hemoglobin A1c (HbA1c) values and provided education regarding risks of high or low values. When appropriate, she taught proper technique for home BP monitoring and reviewed home BP values and antihypertensive medication adherence. She also provided education and cooperative goal setting tailored to where a participant was on the continuum of diabetes management. If participants agreed, the nurse or study physician sometimes made recommendations to the participant's primary care physician (PCP) via staff message in the electronic health record (EHR).
In general, health coaches focused on behavioral risk factors and strategies, while the study nurse focused on medical conditions (hypertension, diabetes) and medications. Participants chose which risk factor(s) they wanted to address at each visit. They were free to set goals on any of the risk factors, even if they were never in the “high risk” zone.
The frequency and duration of visits were tailored to participants’ needs and preferences. A suggested visit cadence was biweekly health coaching visits for the first three months, monthly visits for the next six months, and visits approximately every six to eight weeks for the remaining 15 months to maintain behavior change. Nurse visits were scheduled quarterly to check-in on management of medical risk factors but could include additional contacts as needed to facilitate changes such as communication with the PCP or follow-up on lab results. Prior to the COVID-19 pandemic, initial health coaching and nurse visits were conducted in-person, and patients had the option for subsequent visits to be in-person or by phone. Beginning in March 2020, all visits were conducted by phone.
Intervention data collection
Health coaches and the study nurse documented each encounter with participants in a visit note. The first health coach visit note described participant motivations for joining the study, questions and concerns expressed about memory loss, prior experiences related to risk factors (e.g., efforts to exercise more), which risk factor(s) participants were most motivated to work on and why, one specific and actionable goal, and participants’ confidence to meet that goal. The first nurse visit note described medical risk factors (e.g., diabetes) and medications with attention to those that might affect cognition, patient education related to these factors, and goals set. Subsequent visit notes described participants’ progress toward their goals, including adjustments to goals, barriers, facilitators, and motivators, and whether technology was used to help achieve the goal. Due to the nature of how goals were tracked and the dynamic nature of goal setting and progression, it was not possible to summarize goal progression within the context of this paper.
The final health coach visit note summarized which risk factors the participant worked on; participant reflections on progress toward their goals, overall observations, and “lessons learned” from the study; and a final goal and plan to work on after the intervention period. The final nurse visit note included a description of progress made managing medical risk factors and medication changes addressed during the study.
Data analysis
We extracted the following data elements for analysis: demographic data (self-reported during screening); baseline risk factors (based on EHR and screening data); numbers of health coach and nurse visits; numbers of health coach and nurse goals set; risk factors addressed at each visit; risk factors addressed for each goal; free text notes from first and last visits with health coaches and the study nurse; and free text for all health coach and nurse goals.
Quantitative data were summarized using descriptive statistics (means, standard deviations [SDs], medians, ranges, numbers, and percentages) (Statistical Analysis Software 9.4 or Microsoft Access 2016). Qualitative data were uploaded into Atlas.ti Windows version 9.1.7.0, and four sub-projects were created: 1) health coach goal notes; 2) nurse goal notes; 3) health coach first and last visit notes; and 4) nurse first and last visit notes. We used a primarily deductive content analysis approach for the qualitative data. 36 An initial code list was developed based on the risk factors addressed in the SMARRT study and by consulting members of the study team. New codes were added as they emerged using an inductive coding process. All qualitative data were initially coded by a primary coder (LS) with regular review and discussion to clarify code definitions (LS and BHB). A secondary coder (BHB, TEM, KDM, or DK) then reviewed all of the coded transcripts and flagged any areas of disagreement. The primary coder was a master's-level social worker with prior experience conducting qualitative analyses who was external to the SMARRT intervention team. Secondary coders were members of the SMARRT study team who provided intervention supervision, health coaching, or operational support. In this way, secondary coders provided a form of “member-checking” by verifying notes were interpreted accurately by the primary coder. Discrepancies were reviewed (LS and BHB) and, if necessary, discussed with the study team until consensus was reached.
All of the quotations associated with each code were extracted into separate Excel spreadsheets. Different team members then wrote narrative summaries for different codes (DEB: cognitive activity, barriers, facilitators, progress, takeaways, great quotes; BHH: hypertension, diabetes, sleep, depression; LS: diet, social engagement, smoking, COVID-19; DER: physical activity; SD: medications potentially harmful to cognition). DEB integrated narratives into the manuscript and made final edits to ensure consistency across the different sections based on co-author feedback.
Results
Participant characteristics
Of the 172 participants enrolled in SMARRT, 21 82 were randomized to the intervention group. Thirteen of the 82 (16%) withdrew, including two deaths unrelated to the intervention.
Baseline characteristics of intervention group participants are shown in Table 1. Participants had a mean ± SD age of 76 ± 5 years; 72% were women; 46% were married or living with a partner; and 36% reported living alone. Most participants (80%) had education beyond high school. The race distribution was 78% white, 11% Black, 4% Asian, and 5% other/unknown; 3% had Hispanic ethnicity.
Baseline characteristics (n = 82).

Values are N (%) unless indicated otherwise.
The “another race” category includes Native Hawaiian or Other Pacific Islander (very small sample size) and self-reported other or unknown race and those who preferred not to answer.
Risk factors worked on, number of goals set, and tools used
The prevalence of each risk factor and the proportions of participants who worked on each risk factor during the 2-year study period are shown in Table 2. At enrollment, the most common risk factors were physical inactivity (n = 64, 78%), hypertension (n = 49, 50%), and poor sleep (n = 40, 49%). As noted in the Methods section describing study participants, we did not gather data on prevalence of poor diet or low cognitive activity at enrollment and therefore do not know the baseline prevalence of these risk factors. The three risk factors worked on most commonly with health coaches were physical activity (95.1%), cognitive activity (59.8%), and sleep (52.4%). The three risk factors worked on most commonly with the study nurse were hypertension (72.0%), medications potentially harmful to cognition (22.0%), and diabetes (12.2%).
Risk factors participants chose to work on with health coach or nurse.*
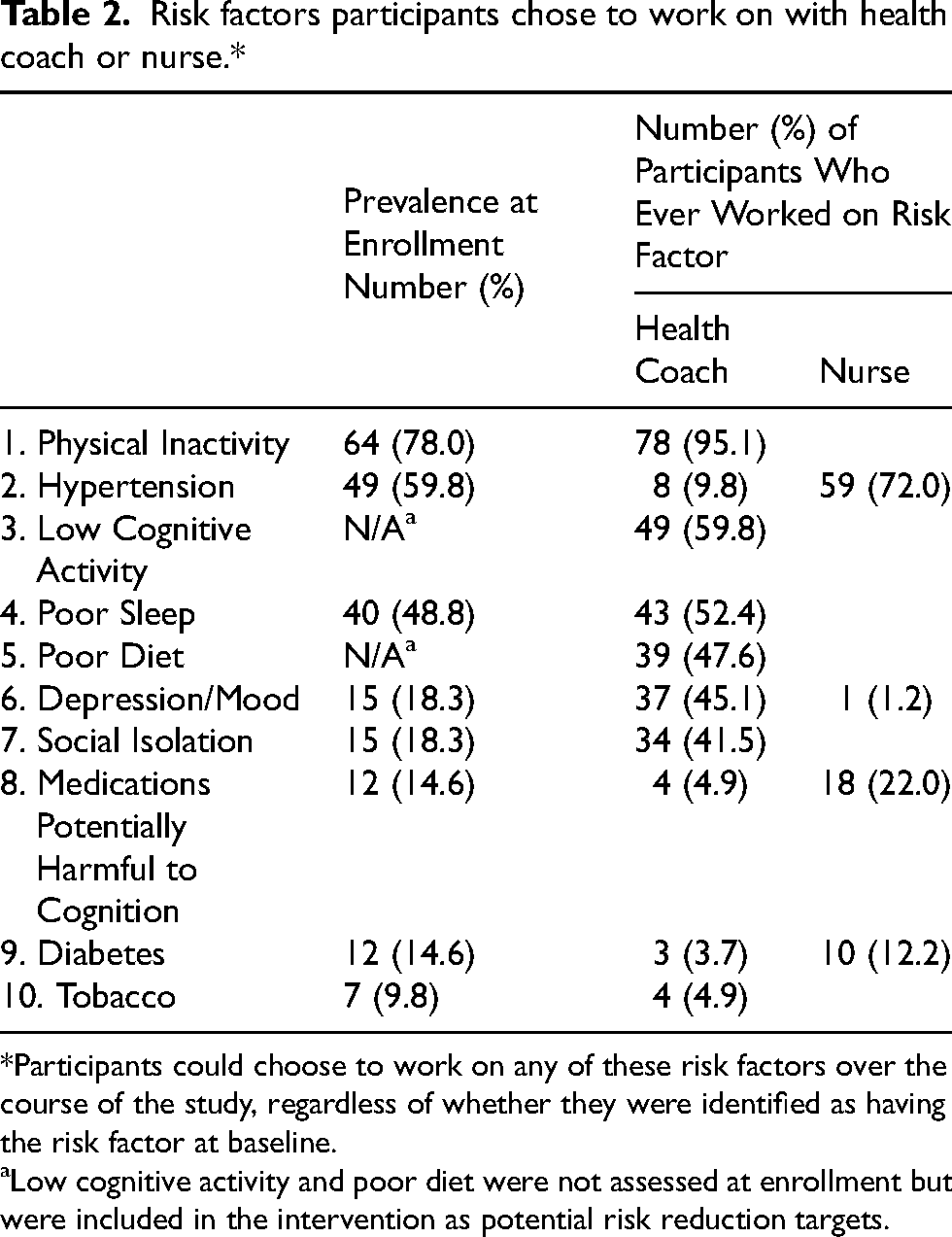
Participants could choose to work on any of these risk factors over the course of the study, regardless of whether they were identified as having the risk factor at baseline.
Low cognitive activity and poor diet were not assessed at enrollment but were included in the intervention as potential risk reduction targets.
The 82 participants set a total of 1225 health coach goals and 113 nurse goals over two years. The median (range) number of goals per participant was 12 (1, 38) health coach goals and 1 (0, 4) nurse goals. The primary paid resources or technology supplied by the study were Garmin VivoFit devices to track physical activity (n = 42, $96/device), home BP monitoring kits (n = 24, $61/kit), and insomnia workbooks (n = 22, $36/workbook). The average cost of supplies per participant was $77. In addition to paid resources, we provided many free resources such as handouts.
Types of goals set
Physical activity
Although 78% of participants were identified as being physically inactive at enrollment (<150 min/week of moderate/vigorous physical activity), 30 nearly all participants (95%) worked with their health coach on physical activity at some point during the two-year intervention period. Participants who worked on physical activity set a median (range) of 8 (1, 24) goals (Table 3).
Numbers of goals set per participant.*
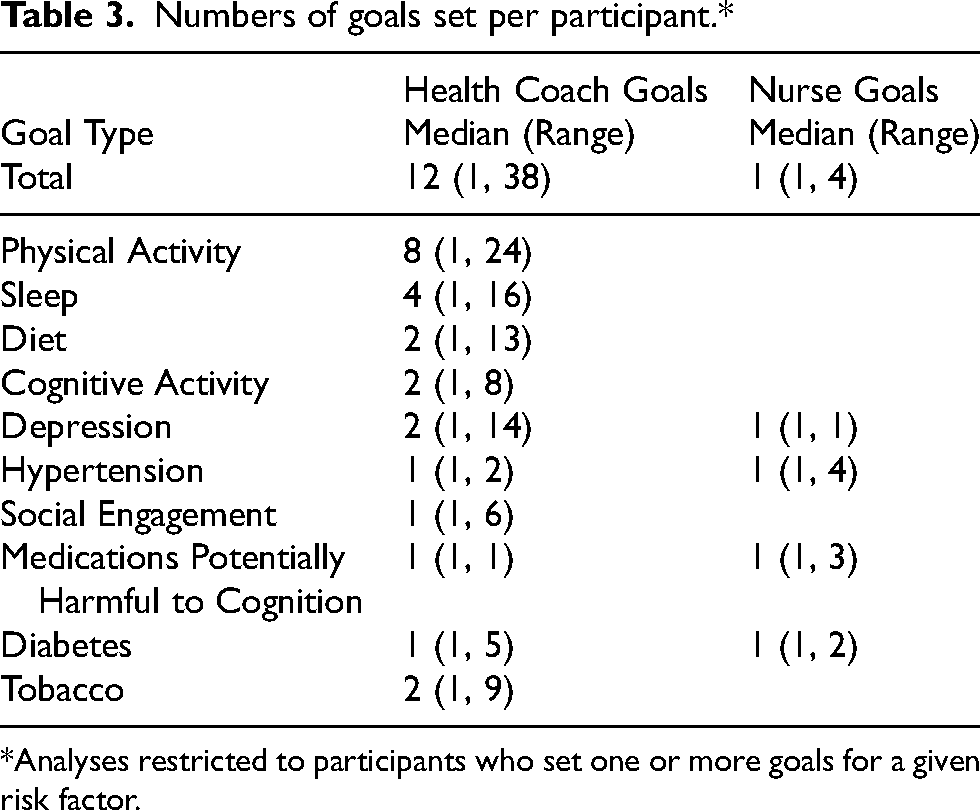
Analyses restricted to participants who set one or more goals for a given risk factor.
The most common physical activity goals were related to increasing walking or step counts. Walking goals included daily life activities (e.g., using the stairs, walking through museums/galleries/zoo, walking the dog) as well as more structured walking goals (e.g., using a treadmill, walking a mile a day). Most walking goals involved relatively brief periods of movement (e.g., walk 1 block, 5 laps around the house, 10 min of walking near home). Some participants set goals to increase steps by a certain amount each week, typically 100 to 200 steps/day each week. Other participants set goals to increase steps to a certain level, ranging from 2000 to more than 10,000 steps/day. Participants were often quite creative in their efforts to get extra steps (e.g., walking while waiting for coffee).
Many people reported using tracking devices to monitor step counts or activity levels. The Garmin VivoFit provided by the study was the most common device used. One health coach note stated that a participant had been given the Garmin band and used it for the entire length of the study to track her steps, averaging 8 to 10 thousand per day, which she did not do before the study. According to the health coach note, this participant said, “The band helped me see how much I'm doing and understand how to make small changes add up over time.”
Participants also set goals related to a wide range of other types of physical activity, including upper body exercises, stretching, balance, fitness classes, bowling, golfing, dancing, yoga, rowing, cardiac rehabilitation, and reducing sedentary time. Participants often reported that being more physically active led to a sense of accomplishment and greater energy. For example, one participant told their health coach, “Finding more ways to move has helped me feel better.” Another health coach note stated that a participant regularly used the National Institute on Aging (NIA) Go4Life materials 37 and reported that “she feels more energized after she does them and she can tell they are ‘stimulating my body.’”
Hypertension
Hypertension was the second most common risk factor that participants chose to work on. Sixty percent of participants were identified as having hypertension at enrollment, including 50% with poorly controlled hypertension 30 (Table 2). All of these individuals worked with the study nurse on hypertension management during the intervention. In addition, some participants who were not initially identified as having hypertension set goals related to blood pressure management. The total proportion of participants who set hypertension-related goals during the 2-year intervention period was 72% with the study nurse and 10% with health coaches (Table 2). Participants who worked on hypertension set a median (range) of 1 (1, 2) nurse goals and 1 (1, 4) health coach goals (Table 3).
The most common hypertension-related goal was home BP monitoring. Many participants were unsure how often to check BP. For example, one participant stated their PCP had instructed them to check their BP daily, but they thought this was just for one week. Participants responded well to encouragement to check BP; however, many set low or less clear goals (e.g., to check weekly or “occasionally”). Most participants set goals of checking BP two to three times a week. The study nurse often taught participants how to do BP self-monitoring. Many goals were related to setting reminders to check BP and involving others such as family members or their PCP.
Nurse notes suggested that regular BP checking appeared to help some participants increase confidence for home monitoring and provide a better understanding of BP variability and risk. For example, according to one nurse note, a participant said: “I think it's been really helpful for me – you got me to start checking my BP again, and my health coach has helped me with planning and strategies.”
Cognitive activity
Cognitive activity (i.e., intellectually stimulating or educational activity) was the third most common risk factor addressed by participants. Although low cognitive activity was not one of the risk factors used for eligibility, 60% of participants set at least one cognitive activity goal with their health coach (Table 2). Among those who worked on cognitive activity, the median (range) was 2 (1, 8) health coach goals set (Table 3).
The most common types of cognitive activity goals were related to puzzles and games, such as crossword puzzles, jigsaw puzzles, Sudoku, and bridge. Patients did puzzles and games using hard copy versions (e.g., game books, newspaper crosswords) and online (e.g., crossword on tablet, computer brain games). In some cases, participants appeared to lose interest in these types of activities over time. For example, one coach noted that a participant “commented that she is easily bored with the [cognitive activity] that she previously enjoyed. She is still doing them but ‘less enthusiastically’ and ‘less intensely.’” Other participants, however, engaged consistently in these activities throughout the study.
Many participants set cognitive activity goals related to reading. Specific activities included going to the bookstore or library, ordering new books, reading a specific number of books each month, and making reading part of their daily routine. Several participants combined reading goals with social goals, such as participating in book clubs or reading the same book as a friend and meeting by phone to discuss.
Other common cognitive activity goals were related to learning or practicing language skills, particularly using the Duolingo app. Several participants reported long-term success with language-related goals.
Less common cognitive activity goals related to music (e.g., learning or practicing a musical instrument, taking music classes) or crafts (e.g., ceramics, sewing). Several participants set goals related to mindfulness practice or taking continuing education classes.
Sleep
Sleep was the fourth most common risk factor chosen by participants. Nearly half (49%) of participants had poor sleep at enrollment (defined as self-reported problems with sleep ≥ 3 nights a week and bothered “somewhat” or more),30,38 and slightly more than half (52%) worked with their health coach on sleep during the intervention period (Table 2), with a median (range) of 4 (1, 16) goals set per participant (Table 3). The most common sleep complaints were irregular sleep, poor quality sleep, sleeping too little, and waking in the middle of the night.
Participants’ sleep-related goals included keeping sleep logs, reducing screen time, establishing a bedtime routine, practicing relaxation techniques, creating a regular sleep schedule, altering the bedroom environment, reducing time in bed awake, exercising to help with sleep, reducing daytime napping, and managing stress and worry.
Several participants reported highly impactful changes related to improved sleep. One health coach note stated, “Sleep: Per her self-report, this is her biggest area of improvement. She used our CBT-I book for sleep. We walked through it together. When talking today she noted, ‘I used to feel physically sick from lack of sleep (some days) and that never happens anymore.’ She found the sleep hygiene and constructive worry content most helpful.” There were frequent goals around improving utilization of continuous positive airway pressure (CPAP) machines for participants with sleep apnea who had been prescribed one.
Relaxation techniques were among the most frequent sleep-related goals. Specific relaxation technique goals included diaphragmatic breathing, progressive muscle relaxation, meditation, guided imagery, and listening to relaxing music. Relaxation techniques were often paired with a pre-bedtime ritual for managing stress/anxiety. Participants particularly identified learning how to manage stress and having more acceptance regarding sleep changes as being a great help. The most used resources were the Overcoming Insomnia workbook, 33 sleep logs, and apps such as Sleepio (http://www.sleepio.com) and Calm (http://www.calm.com).
Diet
Diet was the fifth most common risk factor that participants chose to work on. Although poor diet was not one of the risk factors used for eligibility, nearly half (48%) of participants worked on diet with their health coaches during the study (Table 2), with a median (range) of 2 (1, 13) goals set per participant (Table 3).
Health coaches were trained to encourage participants to increase adherence to the MIND diet, which combines the Mediterranean and DASH (Dietary Approaches to Stop Hypertension) diets. 39 The most common dietary goals included learning more about the MIND diet by reviewing study handouts or trying to increase consumption of food items from the MIND diet, such as leafy green vegetables, whole grains, nuts, and berries. A related goal was to replace less healthy items with more healthy items from the MIND diet, such as using olive oil over butter or eating fish or poultry instead of red meat.
Other diet goals included tracking daily food intake. Most people used the food logs provided by the study. Another frequent goal was trying to reduce sugar and dairy consumption. A few participants preferred to try different diet regimens, like the keto or Atkins diets. Several participants reported weight loss as a motivator, although this was not an explicit goal of the intervention.
One participant shared that her diet goals were the most helpful part of the SMARRT Study. One health coach note stated: “[S]he dropped her membership in Weight Watchers because she didn’t feel she was getting anything from it above and beyond what she was getting from MIND diet goal setting.” She reported having lost 8 lbs. and attributed this change to her MIND diet goals of eating more spinach salads and fish.
Depression
Depression was the sixth most common risk factor participants selected to work on. Relatively few participants (n = 15, 18%) screened positive for depression at enrollment (score ≥10 on the PHQ-8 40 ); however, 45% worked with their health coaches on depression or mood during the intervention period (Table 2) with a median (range) of 2 (1, 14) goals set among these participants (Table 3).
Although PST was initially intended as the primary offering for depression management, only six participants engaged in formal PST treatment. Participants who engaged in PST primarily used problem solving work sheets to explore and create action plans to resolve problems. Common problems addressed included physical health and medical care concerns and interpersonal challenges.
More commonly, participants set broader depression management goals without formal PST. Goals focused on participating in pleasant events, tracking mood, using relaxation skills, exercising, increasing social activity, and connecting to medical or mental health services. The most frequent pleasant event goals were related to using a pleasant event schedule worksheet to select frequent and new activities. Common pleasant events included relaxation, increasing social contact, and exercise.
Fifteen participants set goals to connect with their PCP or a therapist for depression or mental health care, with approximately half of these being new episodes of care. Depression also was sometimes addressed in nursing visits, with a focus on medication adherence and changing antidepressants to avoid those potentially harmful to cognition.
Several participants highlighted depression as something that had been positively affected by the study. As one health coach noted about a participant, “He feels his mental health has significantly improved over the course of the study; he is happier and doing more. He completed PST with me and found that helpful.”
Social engagement
Social engagement was the seventh most addressed risk factor. Although only 15% of participants were identified as being socially isolated at enrollment (score ≥6 on the UCLA 3-Item Loneliness Scale 41 ), 42% of participants set at least one goal related to social engagement (Table 2), with a median (range) of 1 (1, 6) goals set per participant (Table 3).
Many goals combined social engagement with physical activity. The most common of these goals was to walk with a friend. Many participants set goals to attend classes at their local senior center or gym, volunteer, or see friends and family. Another participant joined daily Zoom group exercise activities, including yoga, Zumba, and Pilates, demonstrating the important intersection between physical activity and social activity goals.
Social engagement became especially important after the COVID-19 pandemic began. When gathering in public spaces was no longer an option, health coaches worked with study participants to create goals around social activities that were virtual or took place outside. Popular goals included attending virtual classes or video chatting with friends and family.
Some participants struggled to set social engagement goals during the pandemic. One health coach wrote that a participant “feels very socially isolated and would like to work on that, but her confidence and readiness were at a 0. Her daily activity consists of preparing meals and taking care of the house.”
Other participants highlighted the importance of the health coach visits for supporting social connection during the pandemic. A health coach visit note said that a “surprising aspect of this study and the timing of the COVID pandemic was the realization of how important social engagement was to her. She said that the lack of social engagement through usual avenues was really hard. She has found ways of connecting through church and more frequent phone calls with friends and family.”
Medications potentially harmful to cognition
At baseline, the medication inventory with the study nurse found that 43% of participants were taking medications potentially harmful to cognition, more than double the proportion identified through the EHR (18%). The main reason was frequent use of OTC medications containing diphenhydramine, which were often used as sleep aids. Diphenhydramine was the most frequently used potentially harmful medication, with use reported by 16 individuals (20%) at baseline. Many participants (n = 11) were on more than one potentially harmful medication.
In some cases, participants had been on a potentially harmful medication for many years and were not aware of potential risks. One woman taking paroxetine reported, “[The nurse] told me that the antidepressant I’ve been on since 1996 is one of the drugs that is a risky med . . . No primary care physician has ever mentioned that to me even though they knew [my husband] had dementia.”
Over the 2-year follow-up, 18 (22%) of participants set formal goals with the study nurse related to potentially harmful medications (Table 2) with a median (range) of 1 (1, 3) per participant (Table 3). Detailed review of nursing notes showed that 27 individuals discontinued a total of 34 risky medications, constituting 69% of those who ever reported using a risky medication (n = 39), or 33% of the intervention group. Another six participants were able to reduce their dose of one or more medications.
Results also highlighted the importance of repeated medication inventory and discussion of cognitive risks over time. During the 2-year follow up, eight participants (10% of the cohort) reported starting 10 new potentially harmful medications. Five of these individuals had not reported any use of potentially harmful medications at baseline. Four participants (50% of those with new starts) ultimately discontinued the new medication during the study period.
Diabetes
Diabetes was the nineth most common risk factor participants worked on (Table 2). Only 15% (n = 12) participants reported having diabetes at baseline, and one person developed diabetes during the study. All these individuals set at least one goal related to diabetes, with a median (range) of 1 (1, 2) nurse goals and 1 (1, 5) health coach goals (Table 3).
About half of the diabetes goals were related to working with the study nurse to monitor blood glucose and HbA1c values. The nurse provided education around the importance of monitoring, medication adherence, healthy diet, and exercise; setting goals for home monitoring of blood glucose; and communication with their PCP around HbA1c labs and medications. Many from this group learned to monitor their blood glucose at home and worked with their PCP to complete regular lab work. However, many chose to set home monitoring goals that were lower than recommended by the study nurse given their disease stage, with a small minority not conducting any blood glucose or HbA1c monitoring.
Another group of participants were already monitoring their blood glucose and taking medications as recommended and were focused on setting goals with health coaches around diet and exercise to improve diabetes and decrease insulin utilization. In this group, there were reports of improved lab values and decreased need for insulin over the course of the study that were very exciting and motivating for those participants. For example, a 24-month nursing visit note stated: “I reviewed with her the positives over the length of the study: had never used any [potentially inappropriate medications], and A1c had decreased from 8.3 to 6.4.”
Smoking
Smoking was relatively uncommon among study participants at baseline (n = 7, 8.5%) and was the least common risk factor worked on. Four participants set goals related to smoking (Table 2) with a median (range) of 2 (1, 9) per participant (Table 3). Two participants set goals around tapering the amount they smoked. This included only taking three puffs per cigarette, not smoking in the house, and extending the time between cigarettes. A third had already quit smoking before joining the study and worked on remaining tobacco free. The fourth participant was motivated to quit smoking in preparation for joint replacement surgery. She created a “cigarette calendar” to track her smoking, gradually reduced the number of cigarettes smoked per day, signed up for the “Quit for Life” smoking cessation program (covered for KPWA members), and used nicotine patches. Ultimately, she was able to quit in preparation for her surgery.
Impact of the COVID-19 pandemic on the intervention and types of goals set
The COVID-19 pandemic began as the SMARRT study was nearing the end of the recruitment period. Many participants had already enrolled and begun working with the health coach and nurse. The transition to exclusively telephone visits had both positive and negative consequences for the intervention.
The health coach visits were relatively easy to conduct by telephone, although many participants reported they preferred in-person visits. The nurse visits were more difficult to translate into phone visits, which made it more difficult to conduct activities including measuring BP and teaching proper cuff use. The impact on medication review was mixed: it was more difficult to do a full medication review without visual inspection of pill bottles, but completing the visit while the participant was in their home allowed for potentially more thorough assessments.
As described above in the social engagement section, the pandemic had a strong impact on both opportunities for social engagement and awareness of the importance of social engagement. In addition, many other aspects of the intervention were affected. Many goals that were planned to be completed in public spaces had to be modified. Some participants noticed that their motivation for completing goals decreased, especially for physical activity, diet, and social connectedness. For example, participants noted less motivation to exercise without group classes, outside rather than indoors, or without a companion. Some participants were concerned about potential infection risk from outdoor physical activity if people were not masked. Some diet goals were also impacted due to less grocery shopping, different meal routines, and less access to fresh produce.
Most participants appreciated being able to continue the intervention over the phone. They noted that telephone visits addressed several barriers including challenges with transportation, mobility, and time. In addition, many participants reported that outreach during the height of the pandemic was very appreciated, providing social contact during a time of heightened isolation. One participant shared “how important those health coaching calls were to me.” Another participant helped to make masks and was proud of this as an activity promoting cognitive activity and social connectedness goals.
Barriers, facilitators, and takeaways
Additional themes were primarily related to barriers and facilitators to achieving goals and “takeaways” highlighted by participants. These often cut across the different risk factors and goals and provide additional context to inform future work.
The most cited barriers to achieving goals were pain, illness, injury, and other health-related issues, usually unrelated to the intervention. Many participants reported pain that made it difficult to exercise. Others reported experiencing illness or injury, including falls, that resulted in lower activity levels and, in some cases, increased fear or anxiety. These issues also impacted participants’ ability to accomplish other goals that required mobility (e.g., meeting a friend, going grocery shopping). Health coaches addressed these barriers by helping participants identify personally meaningful goals and take small, achievable steps to support feelings of success and build confidence.
The second most cited barrier was lack of motivation. Health coaches used motivational interviewing to address this barrier, meeting participants where they were in the context of behavior change stage and supporting them to increase their intrinsic motivation to engage in specific activities. Other barriers noted included weather, the built environment, distractions or difficulty prioritizing, lack of support, the COVID pandemic, and safety concerns.
When participants were asked what they felt were the most important aspects of the intervention, they highlighted the supportive role of the health coach and nurse and being held accountable. For example, one health coach note said that a participant “really appreciated the encouragement and reinforcement from this study. She said that sometimes she just needs someone to tell her that she is on the right track or doing good things. She said she liked ‘reinforcement from people I trust and respect—that's what you guys gave me.’” According to another health coach note, a participant said, “I had to be accountable to you every month, and that was a big motivator.”
Equally important was learning how to set small, achievable goals, particularly when dealing with setbacks. For example, one participant told her health coach, “My biggest change here is understanding setbacks are ok and I can start small.” Another health coach note stated, “She says her main take-aways from the study are to set smaller goals, or steps toward her larger goals, to make change manageable. Also motivate herself with small steps, so she can see the success or adjust if something doesn’t work.”
Participants also reported that an important benefit of the study was increased knowledge and awareness of dementia risk factors. One health coach note said, “She said she previously did not know much of anything about dementia because ‘it's not something you talk about in polite company.’ She appreciates increased awareness about [risk factors] for dementia, which she very nicely summarized back to me.” Participants also reported on the usefulness of supportive tools provided by the study such as goal tracking, journaling, the Garmin fitness tracker, and the insomnia workbook.
Many participants reported experiencing improvements in dementia risk factors over the course of the study—including increased physical, cognitive, and social activity; better sleep; improved diet; improved mood; and reduced smoking—as well as improved ability to maintain positive achievements and manage setbacks. These changes were often accompanied by positive feelings such as motivation, pride, gratitude, hopefulness, enjoyment, confidence, and resilience.
Although a few participants reported feeling disappointed with their progress, most reported feelings of gratitude or appreciation for being part of the study. Several were especially appreciative that the study had been performed within their healthcare system (KPWA). One health coach note stated, “The [participant] reports things are going well. He has maintained his diet changes, made progress on incorporating leafy greens more, and has a new, specific physical activity goal. He says he found the health coaching helpful. ‘I know how I can avoid some of the pitfalls of aging and improve my physical and mental health. I feel more in control of my destiny.’”
Discussion
SMARRT was originally designed as a pilot study to determine whether a flexible, personalized approach to dementia risk reduction would help older adults make behavioral changes over a two-year intervention period. Although the study was not originally powered to detect an effect on cognitive function, and we had to stop enrollment early and transition to fully remote delivery of the intervention due to the COVID pandemic, the main trial found statistically significant beneficial effects on measures of cognitive function, dementia risk factors, and quality of life. 21 In addition, the effect size in SMARRT was substantially larger than has been observed in other recent dementia risk reduction trials.12,14 This in-depth analysis of intervention notes found that participants chose to work on a wide range of risk factors and to set goals in a variety of ways. It is possible that the larger treatment effect observed in the main SMARRT trial may be explained in part by the flexible, personalized approach that was implemented, potentially making behavior changes more sustainable as they fit more easily into participants’ unique daily lives. 42 Allowing people to select their own risk factors and set their own goals may help those in contemplation and pre-contemplation stages of change make incremental changes and build confidence and self-efficacy over time.
In general, we found that these high-risk older adults were willing and able to make and sustain meaningful behavior change over the two-year intervention period. They appreciated having regular, long-term contact with the study team to hold them accountable. The health coaches and study nurse provided complementary expertise to support behavior change goals. Transitioning to telephone during the COVID pandemic did not appear to have a negative effect on the impact of the intervention.
Physical activity was by far the risk factor that participants chose to work on most often, suggesting that this risk factor should be prioritized in multi-domain dementia risk reduction interventions. Most participants were relatively inactive at enrollment, and goals tended to be well below current guidelines of 150 min/week of moderate to vigorous activity. We found that it was important to support participants in setting realistic goals related to physical activity, and that they reported benefits from even small changes.
It is interesting to note that many participants chose to set goals for physical activity, depression, and social isolation even if they were not identified as having these risk factors at enrollment. Some of these individuals developed these risk factors during the study period. However, others were interested in maintaining or continuing to improve on factors for which they were never in the “high risk” zone. It is possible that allowing participants to choose which factors to address, including setting goals related to factors they are already doing well on, may help them experience feelings of success that open the door to working on more challenging risk factors.
In contrast, only 4 of 7 (57%) of participants who smoked chose to set a goal related to smoking. These findings suggest that it may be less fruitful to target deeply entrenched risk factors such as smoking that are especially difficult to change.
We also observed that, although neither cognitive activity nor diet were included as eligibility criteria for the main trial, these were often selected by participants as factors they wanted to change. In addition, social engagement was often paired with goals for other risk factors and served as an important motivator for many participants. These findings indicate that multi-domain interventions may increase their success by leveraging desires related to everyday life experiences such as preparing and eating meals and engaging in cognitive and social activities.
All participants with hypertension or diabetes at enrollment set at least one goal with the study nurse related to these conditions during the study period. In many cases, the nurse found that they had not understood or were not following their doctor's instructions on condition self-management and provided support to help them be more adherent. The study nurse also found that many participants were taking OTC medications that were potentially harmful to cognition, particularly sleep medications with antihistamines, highlighting the importance of gathering information about OTC and prescription medications in multi-domain risk reduction trials.
Participants reported that the most useful aspects of the intervention included having the support of the coach and nurse, being held accountable, and learning to set small goals and recover from setbacks. These strategies resulted in self-reported improvements in dementia risk factors, increased awareness and knowledge of dementia risk factors, and positive feelings about both the intervention and the healthcare system.
The current manuscript used both quantitative and qualitative methods to gain a deep understanding of what occurred during the SMARRT intervention, when participants were given an opportunity to create personalized dementia risk reduction goals and strategies. This approach has several strengths. All visits were documented in a comprehensive research database. Qualitative coding was performed by an independent analyst not involved with the intervention, with review and confirmation/clarification provided by team members knowledgeable about the intervention. Limitations include the relatively small sample size and the study population being primarily non-Hispanic white and well-educated, which may impact generalizability. Our small sample size also did not allow us to explore potential differences based on age, gender, living arrangement, or other factors. In addition, our data sources (visit and goal notes written by health coaches and the study nurse for internal tracking and documentation purposes) were not suitable for a more detailed thematic analysis. Future studies would benefit from doing exit interviews with participants and intervention team members to capture more detailed information on barriers, facilitators, and other learnings. We also did not routinely capture data on whether goals were met in a structured way; instead, we tracked the evolution of goals over time, including strategies for maintenance and management of setbacks.
In this paper, we have provided an in-depth examination of how SMARRT study participants engaged with health coaches and the study nurse to make healthy behavior changes based on their own preferences and values. We provide detailed information about the concrete steps taken by participants and health coaches that facilitated successful behavior change. Furthermore, the behavior changes observed in SMARRT were associated with improved outcomes in the main clinical trial. 21 The findings detailed here may be helpful for researchers designing future interventions to reduce dementia risk or for teams wishing to implement an intervention like this in their own clinical setting. These results and those of other dementia risk reduction interventions around the world13–29 deepen our understanding of the best ways to support dementia risk reduction in older adults.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241296161 - Supplemental material for The Systematic Multi-domain Alzheimer's Risk Reduction Trial (SMARRT) intervention: A personalized approach to dementia risk reduction
Supplemental material, sj-docx-1-alz-10.1177_13872877241296161 for The Systematic Multi-domain Alzheimer's Risk Reduction Trial (SMARRT) intervention: A personalized approach to dementia risk reduction by Deborah E Barnes, Benjamin H Balderson, Lisa Shulman, Dori E Rosenberg, Theresa E Matson, Kayne D Mettert, Kristin Delaney, Deborah King, Kristin Adams, Lynn Fleckenstein, Carrie B Peltz, Abisola Idu, Eric B Larson, Kristine Yaffe and Sascha Dublin in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We gratefully acknowledge the study participants.
Author contributions
Deborah E Barnes (Conceptualization; Formal analysis; Methodology; Supervision; Writing – original draft; Writing – review & editing); Benjamin H Balderson (Formal analysis; Methodology; Supervision; Writing – original draft; Writing – review & editing); Lisa Shulman (Formal analysis; Writing – original draft; Writing – review & editing); Dori E Rosenberg (Conceptualization; Formal analysis; Methodology; Supervision; Writing – original draft; Writing – review & editing); Theresa E Matson (Investigation; Validation; Writing – review & editing); Kayne D Mettert (Project administration; Validation; Writing – review & editing); Kristin Delaney (Data curation; Formal analysis; Writing – review & editing); Deborah King (Investigation; Supervision; Validation; Writing – review & editing); Kristin Adams (Investigation; Writing – review & editing); Lynn Fleckenstein (Project administration; Writing – review & editing); Carrie B Peltz (Project administration; Writing – review & editing); Abisola Idu (Data curation; Writing – review & editing); Eric B Larson (Conceptualization; Funding acquisition; Methodology; Supervision; Writing – review & editing); Kristine Yaffe (Conceptualization; Funding acquisition; Methodology; Supervision; Writing – review & editing); Sascha Dublin (Conceptualization; Formal analysis; Methodology; Supervision; Writing – original draft; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was supported by the National Institute on Aging of the National Institutes of Health (R01AG057508). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Barnes is co-founder, Chief Science Advisor, and holds stock in Together Senior Health, Inc., which has created an online program for older adults with subjective cognitive decline that includes brain health education and coaching. The Conflict of Interest Advisory Committee at the University of California, San Francisco, reviewed this relationship and determined that there is no conflict with the SMARRT intervention. Dr Dublin has received grant funding from GSK and Syneos Health for work unrelated to this study. Other authors have no conflicts of interest.
Data availability
Qualitative data described in this manuscript will not be shared because they may contain identifiable patient information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.