
Abstract
Background
Apolipoprotein E (APOE) ε4 is the most significant genetic risk factor for sporadic Alzheimer's disease (AD). However, its impact on the dynamic changes in resting-state functional connectivity (FC), particularly concerning network formation, interaction, and dissolution over time, remains largely unexplored in AD.
Objective
This study aims to explore the effect of APOE ε4 on dynamic FC (dFC) variability and cognitive performance in AD.
Methods
We analyzed the dFC of AD patients, comparing APOE ε4 carriers (n = 33) with non-carriers (n = 41). The whole-brain dFC was assessed by calculating dynamic fractional amplitude of low-frequency fluctuations (dfALFF) and dynamic regional homogeneity (dReHo). To further explore the relationship between cognitive function and dFC in AD patients, we conducted a correlation analysis. Mediation analysis was also performed to determine whether dFC mediates the link between the APOE ε4 and cognitive decline in AD patients.
Results
AD patients carrying the APOE ε4 exhibited more severe cognitive impairment, along with reduced dReHo and dfALFF in both the left and right posterior cerebellar lobes. In these carriers, the dFC analysis showed lower dFC between the left posterior cerebellar lobe and the left middle temporal gyrus, which was positively correlated with executive function and information processing speed. Additionally, mediation analysis indicated that APOE ε4 influences dFC in this brain region, contributing to executive dysfunction in AD.
Conclusions
These findings offer preliminary evidence that APOE ε4 modulates fluctuating communication within the cerebellar lobe and the dFC between the cerebellar lobe and the temporal gyrus in AD.
Keywords
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disease with cognitive and functional abilities decline characterized by amyloid-β (Aβ) deposition, pathological tau, and neurodegeneration. Since the discovery of Apolipoprotein E (APOE) allele ε4 in 1993, it continues to be the strongest genetic risk factor associated with sporadic AD. 1 An interaction between race and the effect of APOE genotype on AD risk has been known that Asian (i.e., Japanese) carriers having the highest ORs. 2 Traditionally the APOE ε4 allele (APOE ε4) was thought to be a trigger of Aβ accumulation at the top of the sporadic AD amyloid cascade by regulating Aβ oligomerization and aggregation in the brain. Recent studies in mouse models expressing human APOE alleles have linked APOE pathogenesis to other AD pathologenic processes including tau neurofibrillary degeneration, microglia and astrocyte responses, and blood–brain barrier disruption. 3 Individuals who are homozygous for the ε4 allele is associated with a higher increased risk than those who are heterozygous for ε4.2,4
Studies using resting-state functional magnetic resonance imaging (rs-fMRI) showed that the disruption of functional connectivity (FC) among brain regions may be an early outcome of neurotoxic Aβ.5–7 Aberrant FC in functional hub regions, neuronal networks, and across the brain has been found in AD patients.8–11 The APOE genotype has been showed to have an effect on FC. A recent study demonstrated that subjects with APOE ε4 have lower FC of temporal default mode network (DMN) compared to those without APOE ε4. 12 Healthy individuals carrying APOE ε4 had a higher FC between the hippocampus and prefrontal, parietal, and temporal cortex. 13
However, previous literature on the APOE influence on the traditional static FC (sFC), which depicts the averaged brain connections across a full scan, only looked at the brain's time-stable features. Research indicates that variations in FC over time can reveal dynamic changes in brain function, reflecting the brain's complexity and variability. A growing number of fMRI studies have discovered that dynamic FC (dFC) which refers to brain connection within sub-intervals of the time series, captures time-sensitive information about the brain network.14,15 dFC from the rs-fMRI time series has proven valuable insights into brain connection patterns in several neurological illnesses, including schizophrenia. major depressive disorder and dementia.16–18 Therefore, brain illnesses associated with cognitive deficiencies and clinical are likely to be determined not only by the level of connectivity between any two specific brain regions, but also by the patterns of temporal variation in that connectivity of those regions. Hence, comprehensive and in-depth investigations of the specific characteristics and temporal properties of FC dynamics could provide insight into alterations in the brain function network of AD.
In the present study, we aimed to explore how the temporal variability of dynamic spontaneous activity fluctuations and dFC differ among individuals with different APOE genotype for AD. To model the FC dynamics alteration of each participant, we utilized a sliding window approach to estimate a set of connection states. Next, we investigated the local and large-scale dFC differences between APOE ε4 carriers and APOE ε4 non-carriers. In addition, the correlation analyses between the aforesaid indices of dFC, AD cognitive performances, and APOE genotype were performed. Then we explored the relationships between these characteristics in AD subjects.
Methods
Subjects
As shown in Figure 1A, a total of 74 AD patients (All right-handed) were recruited at the outpatient and inpatient departments of Affiliated Drum Tower Hospital of Nanjing University Medical School between from September 2022 to January 2024, including 41 non APOE ε4 gene carriers and 33 APOE ε4 gene carriers. All AD patients were diagnosed with AD for the first time. Each subject underwent a series of standardized clinical assessments including blood test, a battery of neuropsychological examinations, and a whole brain MRI scan. In addition, all patients’ blood tests met the AD diagnostic criteria recommended by the National Institute on Aging and Alzheimer's Association (NIA-AA) (Aβ42/40 positive, P-tau181 positive). 19 According to the Declaration of Helsinki, this study has been approved by the ethics committee of Affiliated Drum Tower Hospital of Nanjing University Medical School. Written informed consent was obtained from all subjects.
Participants were excluded based on the following criteria: (1) individuals with cognitive impairment under 50 years of age or with a disease duration of less than one year; (2) Head MRI examination indicated that there were new cerebrovascular diseases in the past month; (3) Cognitive dysfunction caused by severe depression, schizophrenia or other mental disorders, syphilis, acquired immune deficiency syndrome, reduced vitamin B12, thyroid dysfunction, infection, alcoholism, etc.; (4) participants unable to cooperate to complete neuropsychological tests or have contraindications for MRI examination; (5) participants who cannot accept or refuse blood tests.
Data acquisition
MRI data were obtained using a 3.0 Tesla Philips Achieva scanner (Philips, Netherlands) equipped with an 8-channel phased-array coil and fitted with a foam pad to reduce head movement. During the scan, soft pads and headphones were used to hold the subject's head and reduce scanner noise. Conventional three-dimensional T1-weighted images served as anatomical references, obtained using a fast gradient echo sequence with the following parameters: repetition time/echo time = 8.2/3.8 ms, inversion angle = 8°, matrix = 256 × 256, and slice thickness = 1 mm. For diffusion-weighted imaging, a spin-echo sequence was employed with parameters: repetition time/echo time = 8662/71 ms, matrix size = 112 × 112, voxel size = 2 × 2 × 2 mm³, slice thickness = 2.5 mm, and 32 diffusion encoding directions (b = 1000 s/mm²) alongside a non-diffusion encoding (b = 0 s/mm²). Additionally, resting-state BOLD fMRI data were collected using gradient echo single-planar imaging sequences with the following parameters: repetition time/echo time = 2000/30 ms, flip angle = 90°, matrix size = 64 × 64, slice thickness = 4 mm, number of slices = 35, and a total of 240 volumes of functional images.
Cognitive tests
The Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) were conducted to evaluate global cognition. In addition, cognitive domains and each raw test were (1) episodic memory: Rey Auditory – verbal Learning Test (RAVLT) 20 ; (2) visuospatial ability: The Clock Drawing Test (CDT) 21 ; (3) Language functions: the Boston Naming Test (BNT) 22 and verbal fluency tests (VFT) 23 ; (4) Executive function: parts A and B of the Trail Making Test (TMT) 24 ; (5) Attention: the Stroop Color and Word Test (SCWT) 25 and the Digit Span Test (DST). 26
The determination of Aβ40, Aβ42, Aβ42/40, and P-tau181 in plasma
Peripheral venous blood was collected from the subject's arm using EDTA anticoagulant tubes. After a resting period of 20 min, the samples were centrifuged at 2000 RPM for 10 min at 4°C. The supernatant plasma was then transferred into 0.5 ml EP tubes and stored at −80°C. Aβ40, Aβ42, Aβ42/40, and P-tau181 levels were measured using the Quanterix SIMOA-HD1 platform (Simoa; Quanterix, Lexington, MA, USA). The Neurology 3-Plex A combination panel, which includes Aβ40, Aβ42, and P-tau181, was employed for the analysis. To minimize confounding factors such as assay variability, all samples from the same subject were tested three times under the same conditions. Any samples with a coefficient of variation greater than 20% were re-evaluated. All measurements were conducted by professionally trained technicians who were blinded to the subjects’ statuses and clinical data.
Data preprocessing
The resting-state fMRI data were preprocessed using Data Processing Assistant for Resting State fMRI (DPARSF https://restfmri.net/forum/DPARSF) in Matlab platform (Matlab R2013b). The following steps were performed for data pre-processing: (1) removal of the first ten volumes; (2) slice timing; (3) head motion correction, subjects were excluded as head motion exceeded 3 mm of translation or >3 degrees of rotation during the scan, no subjects was eliminated; The average function image after motion correction was co-registered with the structure T1 image; (4) The brain structure image from T1 image was segmented into gray matter, white matter and CSF, and the total brain volume of each subject was obtained; (5) Regress out the white matter, CSF and Friston-24 motion parameters; (6) normalization to the Montreal Neurological Institute (MNI) space, and resampled into 3 mm × 3 mm × 3 mm; (7) band-pass filtering (0.01 Hz <f < 0.1 Hz); (8) smoothing with an isotropic Gaussian kernel (full width at half-maximum = 6 mm).
fMRI processing
Dynamic fractional amplitude of low frequency fluctuations (dfALFF) and dynamic regional homogeneity (dReHo)
As shown in Figure 1B, the temporal dynamic analysis (TDA) toolkit based on DPARSF V6.1 software was used for dfALFF analysis. Using the sliding window method, a window length of 30 TRs and a step length of 1 TR were selected, resulting in each subject's time series being divided into 191 windows. The dfALFF was estimated by calculating the standard deviation (SD) of the ALFF across the windows for each voxel, resulting in a set of fALFF maps for each participant. A two-sample t-test, controlling for education, age, and sex as covariates, was conducted to assess the differences in dfALFF maps between the two groups at each voxel. Multiple comparisons correction was performed with Gaussian random field (GRF) theory (voxel level, p < 0.01; Cluster level, p < 0.05, two-tailed GRF corrected). The process of dReHo is the same as that of dfALFF, but the functional data after band-pass filtering is selected for dReHo analysis.
Dynamic FC
Voxel-wise seed-based FC analyses were performed using the DPARSF 6.1. We utilized the aberrant dfALFF and dReHo regions, which we calculated above, as seed regions. We applied the sliding window approach, similar to that used in the dfALFF and dReHo calculations. The time course was divided into 30 TR Hamming windows, with each window shifted by 1 TR, resulting in a total of 191 overlapping windows for the first-level analysis. Within each sliding window, whole-brain functional connectivity (FC) maps for the seed region were computed by calculating the Fisher z-transformed Pearson correlation coefficient between the averaged time course of all voxels in the seed and the time course of all other voxels in the brain. This process generated a set of sliding window zFC maps for each participant. The dFC was estimated by calculating the standard deviation of zFC values across the windows for each voxel. A two-sample t-test, controlling for age and sex as covariates, was conducted to examine differences in dFC values between APOE ε4 carriers and non-carriers in each region. Multiple comparisons were performed with GRF correction (voxel level, p < 0.01; Cluster level, p < 0.05, two-tailed GRF corrected). To verify the results in this study, Hamming Windows of 50TRs and 80TRs were selected for analysis.
Statistical analysis
As shown in Figure 1C, statistical analyses were performed using SPSS Statistics 25, as well as correlation analyses and mediation analyses. Measurement data were reported as mean ± standard deviation or median (interquartile range) based on normality. Independent sample t-tests or Mann-Whitney U tests were used for group comparisons. Categorical data were expressed as counts (percentages), with chi-square tests applied for analysis. When comparing cognitive differences between the two groups, variables known to be associated with cognitive function, such as age, gender, and education, were included as covariates. For normally distributed data, Pearson correlation analysis was employed to examine the relationship between the data and cognitive domains. In cases where the data were not normally distributed, Spearman correlation analysis was used. A p-value of less than 0.05 was considered statistically significant. a mediation analysis model was utilized to investigate whether the relationship between the APOE ε4 gene and cognitive function is mediated by brain dFC. Bootstrap analysis was conducted to assess the reliability of the mediation model. In this study, APOE ε4 was treated as the independent variable, cognitive function as the dependent variable, and brain dFC as the mediating variable. Evaluate the corresponding 95% Confidence Interval (CI), if the 95% CI contains 0, it means that the mediating effect is not significant at the significance level of 5%.
Results
Demographic and clinical characteristics
The demographic and clinical characteristics of the two groups are summarized in Table 1. A total of 74 AD patients participated in the study, with 41 patients (18 males, age: 71.93 ± 8.06) in the APOE ε4 non-carrier group and 33 patients (14 males, age: 72.64 ± 8.97) in the APOE ε4 carrier group. No significant differences were observed between the two groups in terms of age, sex, education, or plasma pathological markers (p > 0.05).
Demographic and clinical data for participants of the two groups.
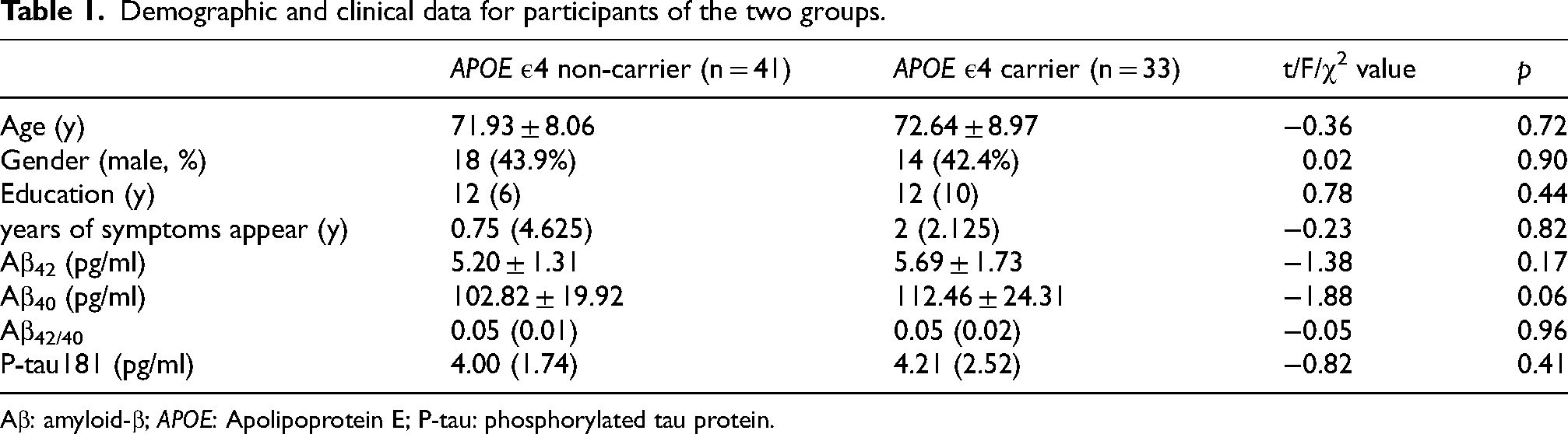
Aβ: amyloid-β; APOE: Apolipoprotein E; P-tau: phosphorylated tau protein.
Cognitive differences between APOE ε4 non-carrier and APOE ε4 carrier group
Regarding cognitive assessment, as detailed in Table 2, the results indicated that participants in the APOE ε4 carrier group performed worse than participants in another group on assessments of global cognition (MMSE: p = 0.03, MoCA: p = 0.02). In addition, the scores of RAVLT_ IR (p = 0.02) and RAVLT_ R (p = 0.02) in the APOE ε4 carrier group were lower, indicating a significant impairment in episodic memory compared to the non-carrier group. No significant differences were found in other indices (p > 0.05).
Cognitive data for participants of the two groups.
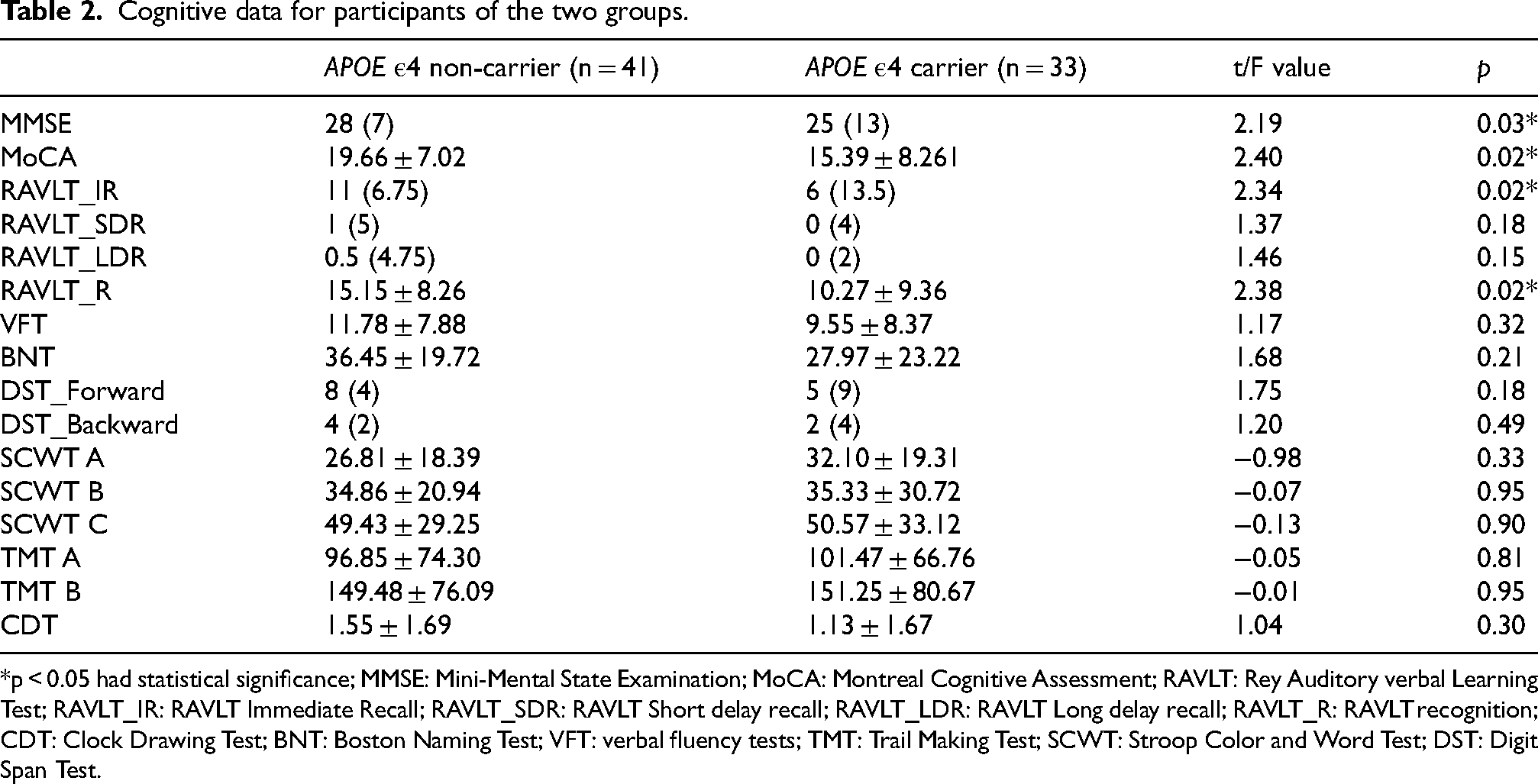
*p < 0.05 had statistical significance; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; RAVLT: Rey Auditory verbal Learning Test; RAVLT_IR: RAVLT Immediate Recall; RAVLT_SDR: RAVLT Short delay recall; RAVLT_LDR: RAVLT Long delay recall; RAVLT_R: RAVLT recognition; CDT: Clock Drawing Test; BNT: Boston Naming Test; VFT: verbal fluency tests; TMT: Trail Making Test; SCWT: Stroop Color and Word Test; DST: Digit Span Test.
Differences in dynamic functional image markers between two groups
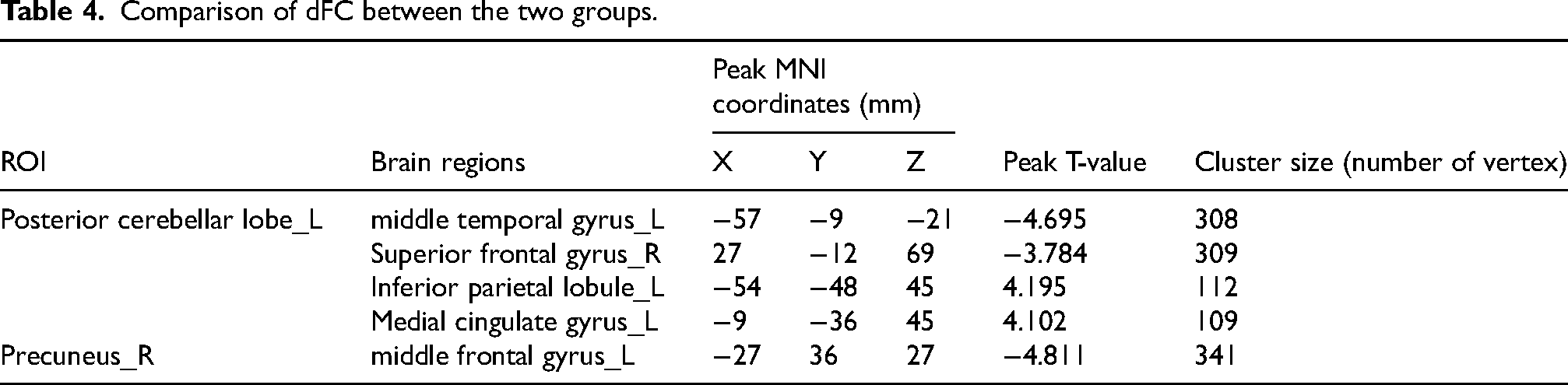
The APOE ε4 carrier group exhibited lower dReHo and dfALFF in the left posterior cerebellar lobe and lower dfALFF in the right posterior cerebellar lobe compared to the non-carrier group. However, dfALFF in the right precuneus was higher in the APOE ε4 carriers. (Table 3 and Figure 2). the brain areas that exhibited differences in dynamic brain activity between the two groups were selected as seed points for dFC in subsequent analyses. As shown in Table 4 and Figure 3, for the left posterior cerebellum, compared with the group of APOE ε4 non-carrier, APOE ε4 carrier shows that the lower dFC of left medial temporal gyrus and right superior frontal gyrus, but a higher dFC of left inferior parietal lobule and middle cingulate gyrus. For the right precuneus, the APOE ε4 carrier group showed a lower dFC of the left middle frontal gyrus.
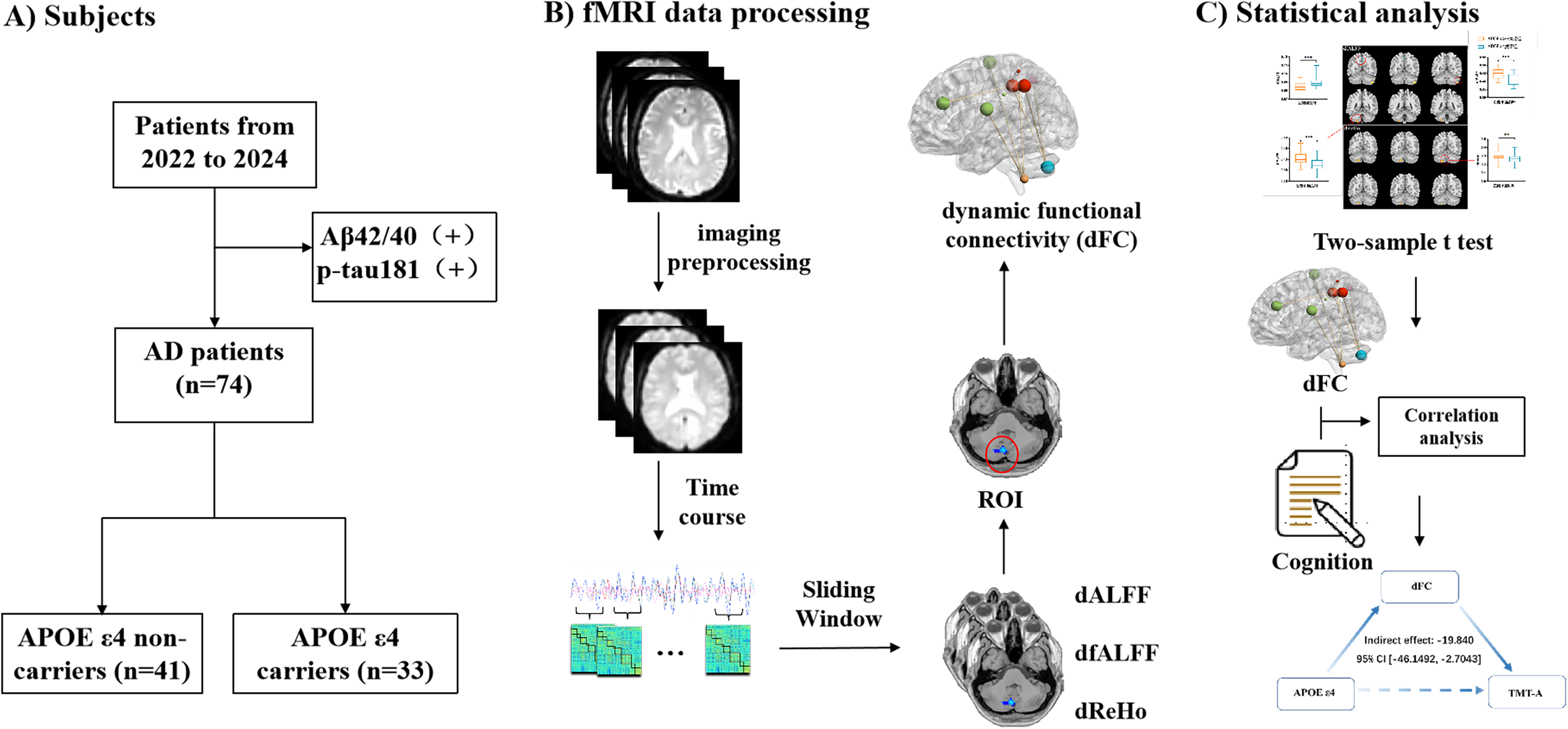
A schematic illustration of the analysis approach. (A) Subject selection; (B) Functional MRI processing; (C) Statistical analysis: including inter-group difference analysis, correlation analysis and mediation analysis. dFC: dynamic functional connectivity; dfALFF: dynamic fractional amplitude of low frequency fluctuations; dReHo: dynamic regional homogeneity, ROI: region of interest.
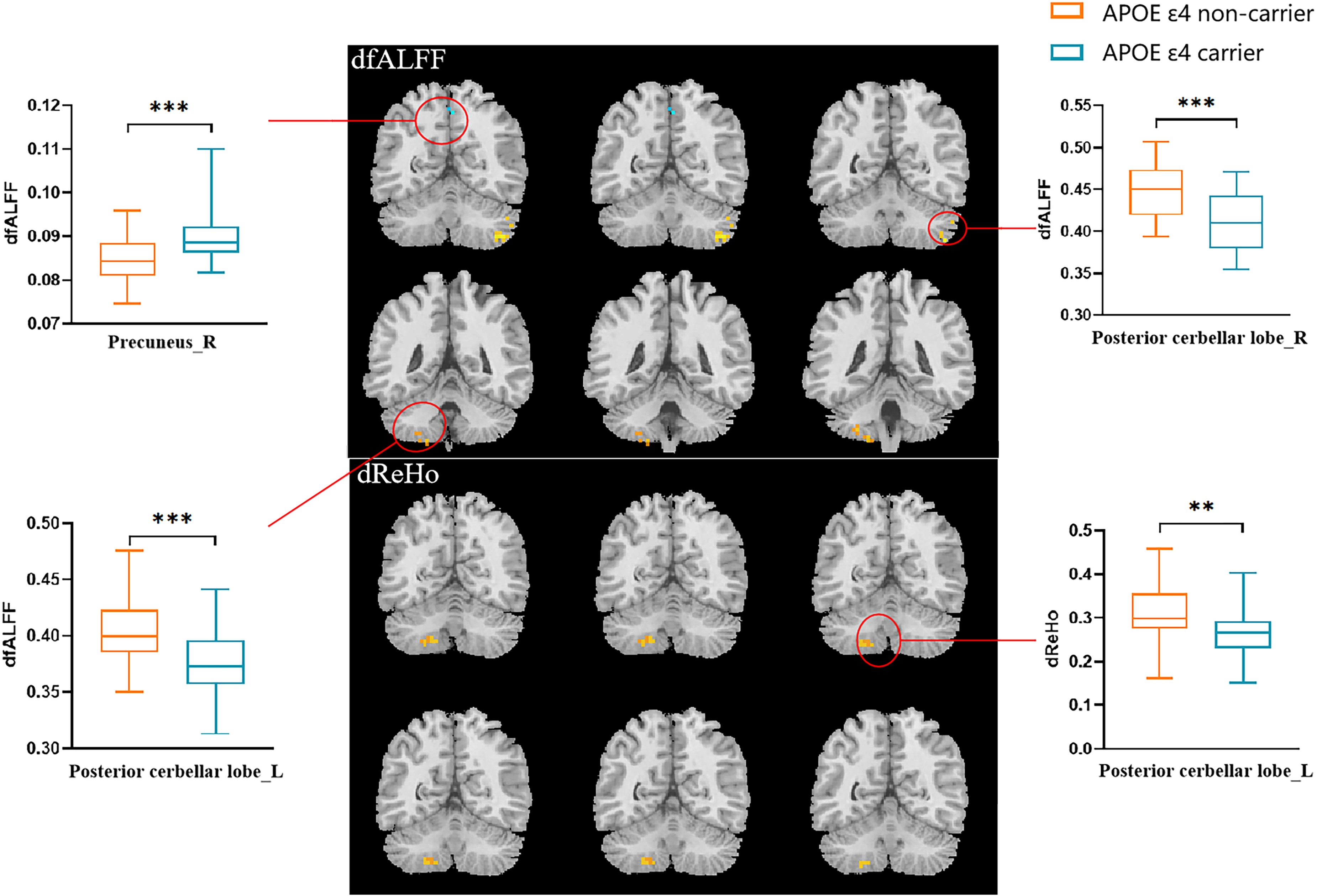
Comparison of dfALFF and dReHo between the two groups. **p < 0.01, ***p < 0.001, had statistical significance. dfALFF: the dynamic fractional amplitude of low frequency fluctuations; dReHo: dynamic regional homogeneity.
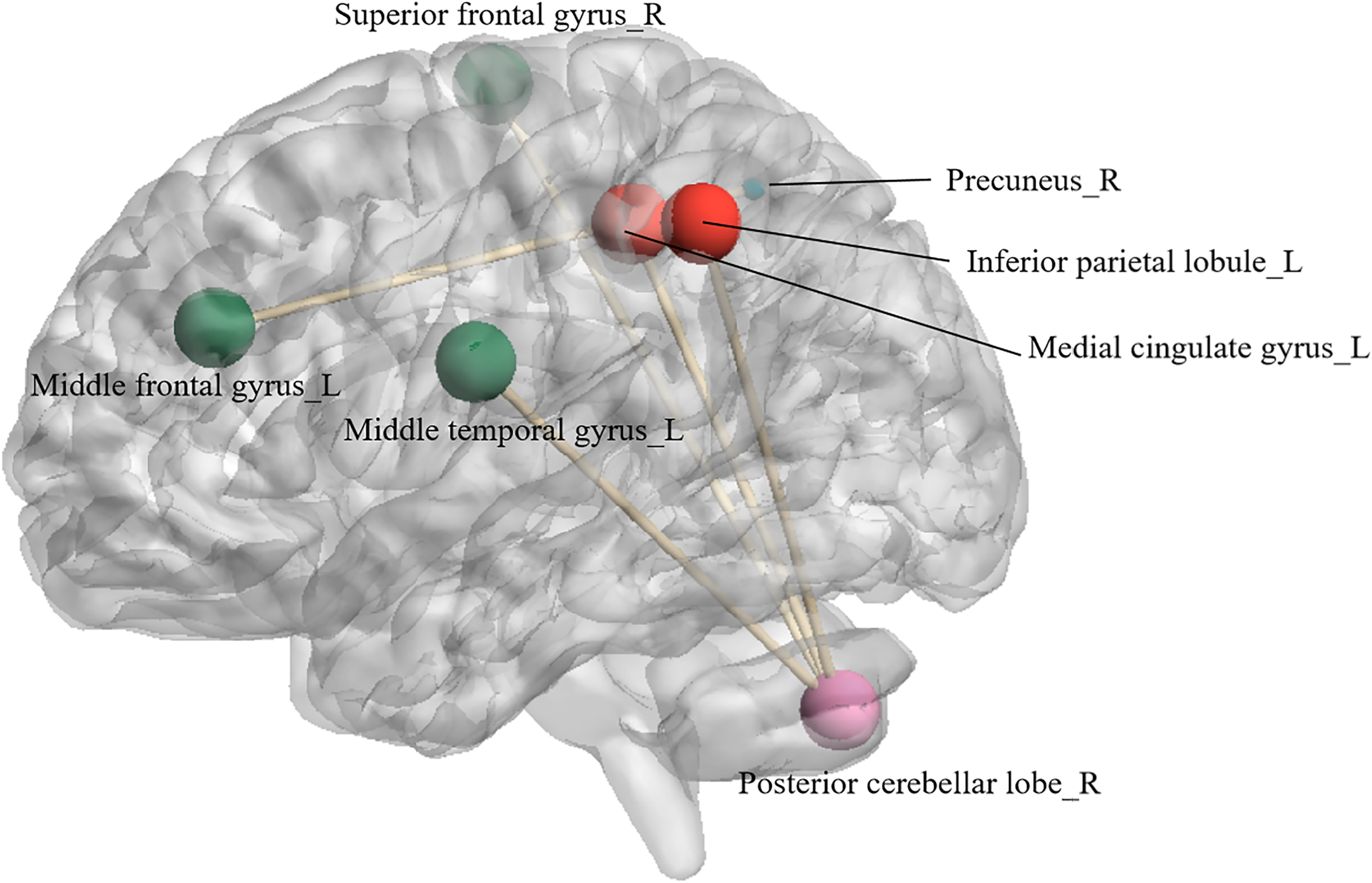
Seed-based dFC between the left posterior cerebellar lobe and right precuneus with other brain regions. Each node represents a brain region. The pink node is the left posterior cerebellar lobe, the blue node is the right anterior cuneiform lobe, linking with red nodes indicate a higher dFC with this brain region, linking with green nodes indicate a lower dFC with this brain region.
Comparison of dfALFF and dReHo between the two groups.
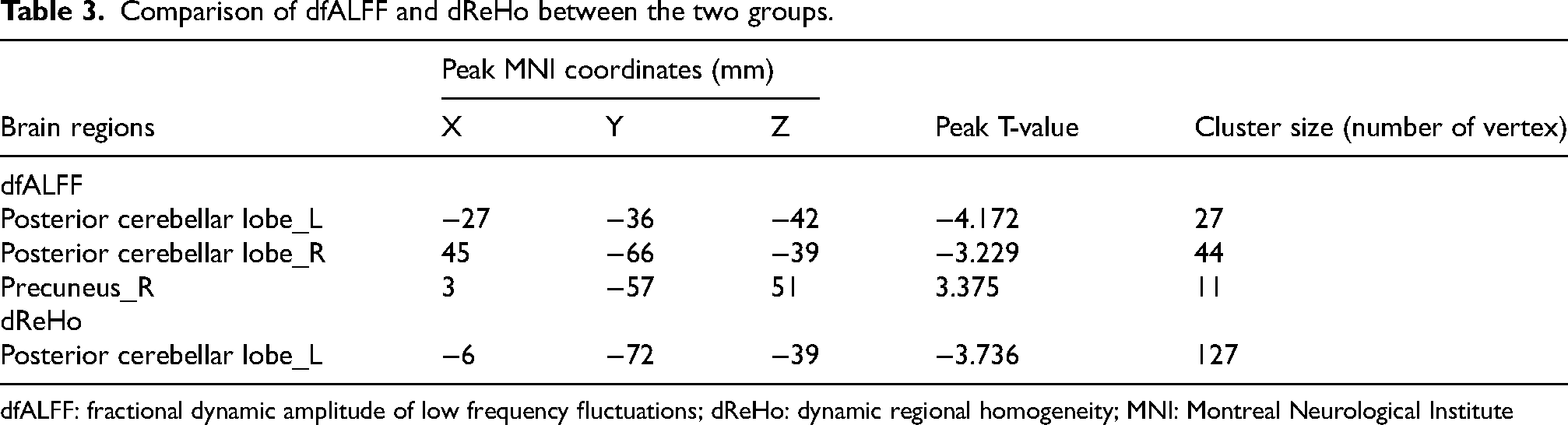
dfALFF: fractional dynamic amplitude of low frequency fluctuations; dReHo: dynamic regional homogeneity; MNI: Montreal Neurological Institute
Comparison of dFC between the two groups.
The relationship between dFC and cognition
By controlling for age, sex and education, the data presented in Table 5 indicate that among APOE ε4 carrier AD patients, the dFC of the left posterior cerebellar lobe with the left middle temporal gyrus was positively correlated with executive function (TMT A: p = 0.001, TMT B: p = 0.005). The dFC of right precuneus with left medial frontal gyrus was negatively correlated with information processing speed (TMT A: p = 0.036). In APOE ε4 non-carriers, the dFC of the left posterior cerebellar lobe with the left middle temporal gyrus showed positive correlations with language (BNT: p = 0.016), attention (SCWT B: p = 0.005, SCWT C: p = 0.014), and executive function (TMT A: p = 0.026, TMT B: p = 0.001). Additionally, the dFC with the left medial cingulate gyrus was positively correlated with information processing speed (TMT A: p = 0.036) (Table 6).
Correlation between dFC and cognitive in APOE ε4 carrie
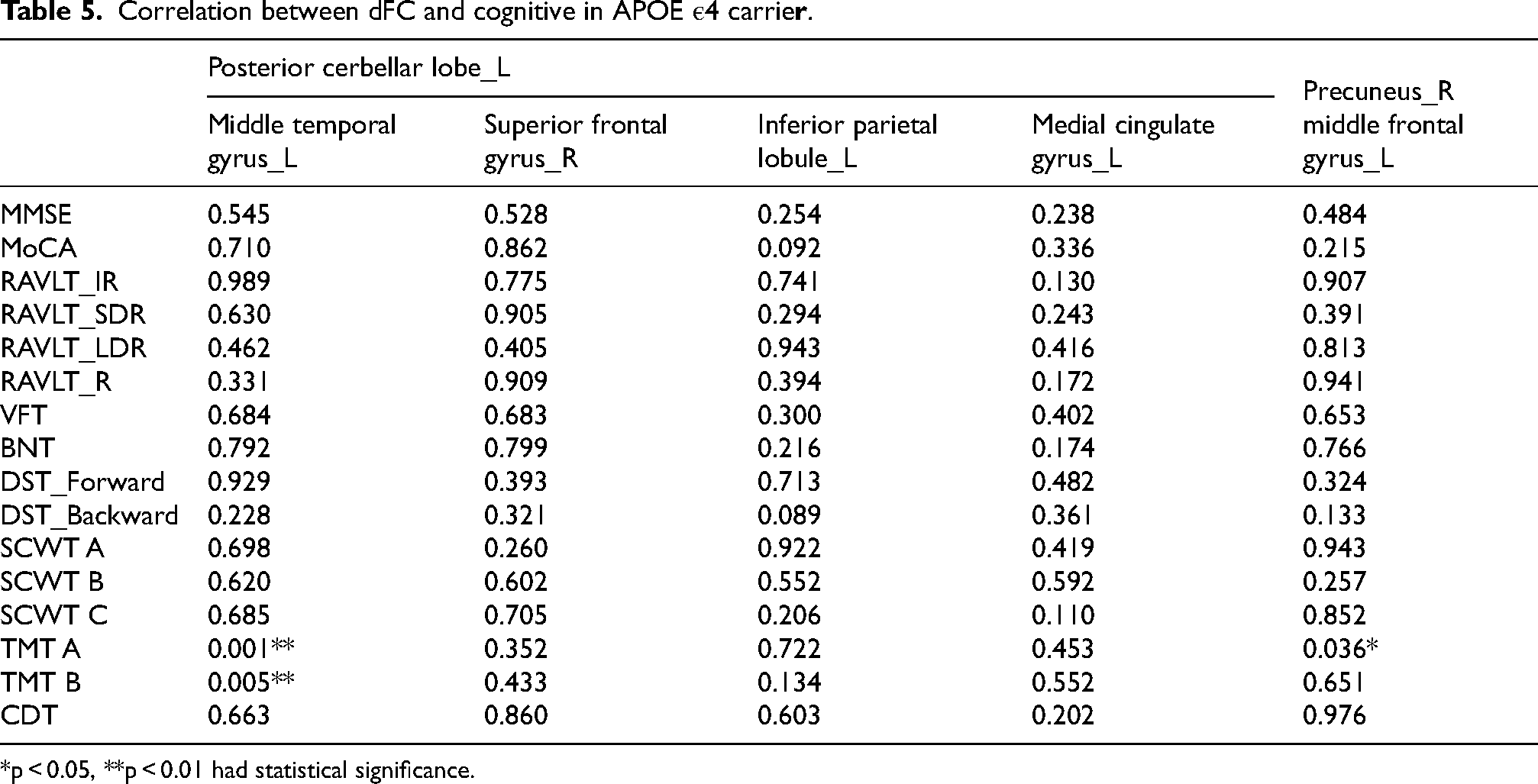
*p < 0.05, **p < 0.01 had statistical significance.
Correlation between dFC and cognitive in APOE ε4 non-carrier.
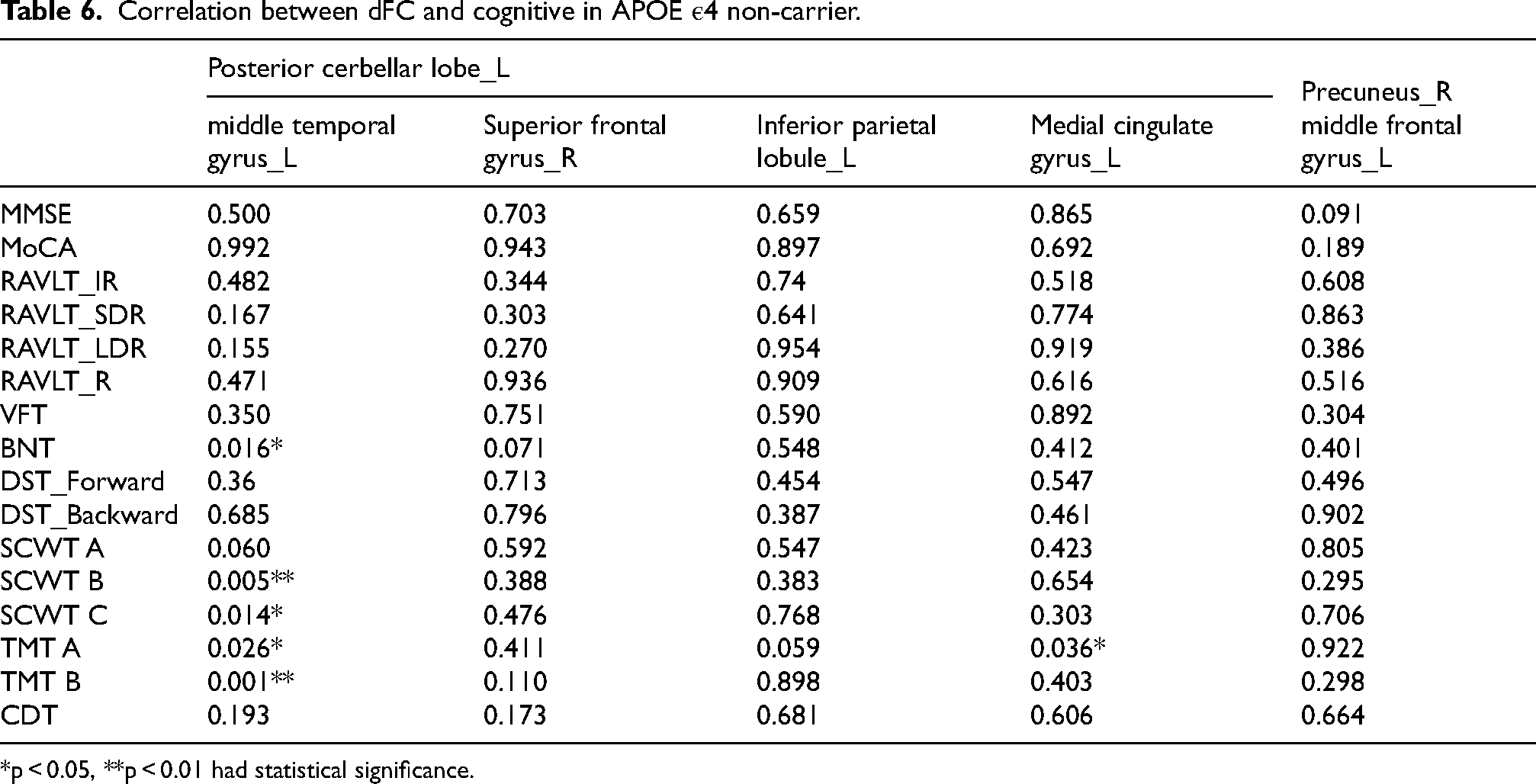
*p < 0.05, **p < 0.01 had statistical significance.
The relationships among the APOE ε4 gene, cognitive function, and dFC
Mediation analysis was conducted to examine the relationships among the APOE ε4 gene, cognitive function, and dFC. The dFC of left posterior cerebellar and left medial temporal gyrus served as the mediating variable, the APOE ε4 genotype as the independent variable, and cognitive scores as the dependent variable. This study found that the APOE genotype negatively impacted TMT and SCWT test scores in AD patients by influencing dFC in the left posterior cerebellar lobe and the left middle temporal gyrus, primarily relating to executive function (Figure 4).
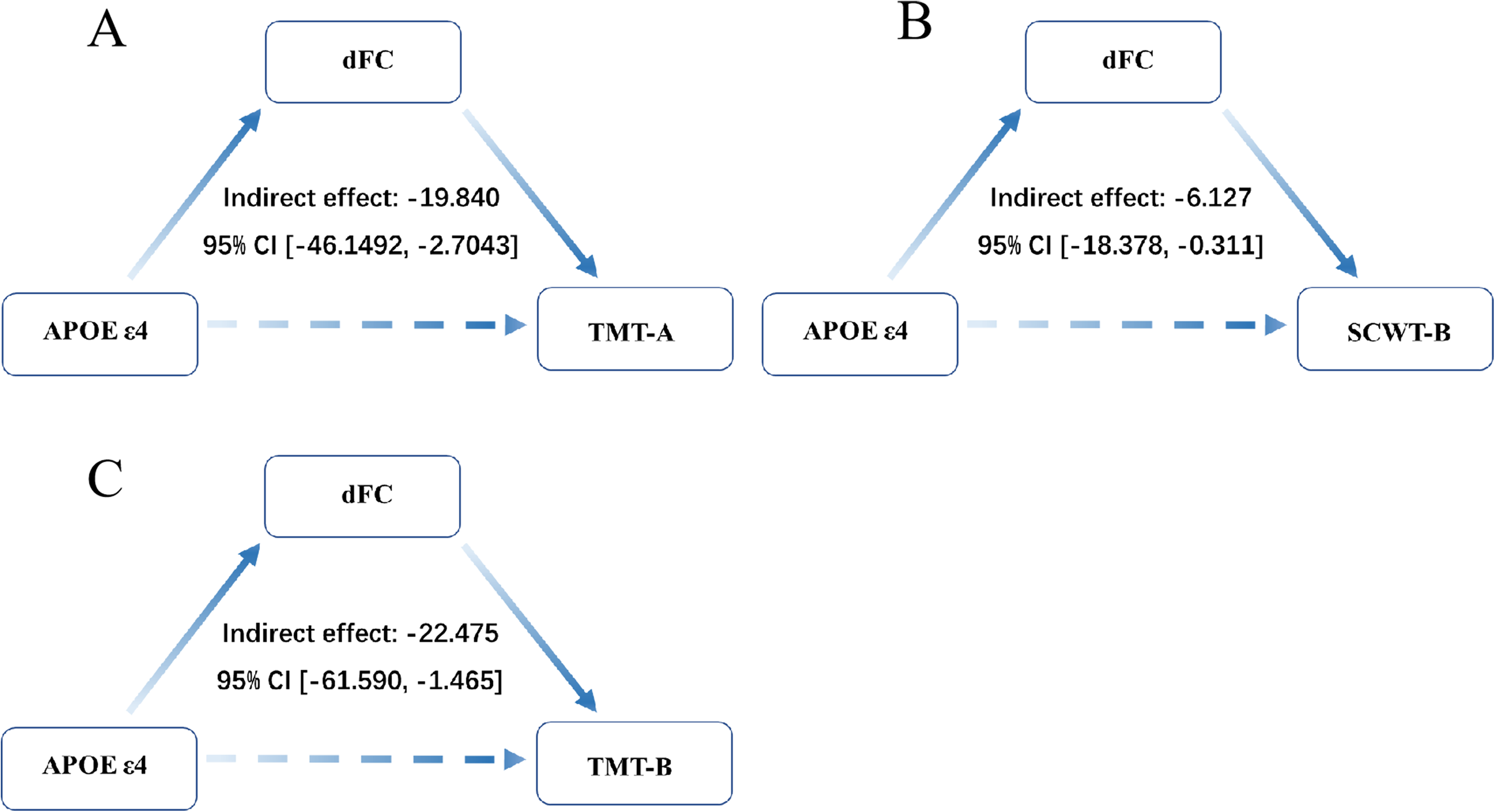
Mediation analysis. TMT: Trail Making Test. SCWT: Stroop color word test. dFC: the dFC of left posterior cerebellar and left medial temporal gyrus.
Discussion
In the current study, we employed dFC analysis to investigate the time-varying network connection patterns of the local aberrant variability in AD individuals with different APOE genotypes, and its correlation with cognitive function. Our main findings are as follows. First, the overall cognitive impairment in APOE ε4 carriers was more severe in the APOE ε4 carriers. Second, compared to the APOE ε4 noncarrier group, the APOE ε4 carrier group showed different patterns of abnormalities in dfALFF, dReHo, and dFC variability. Finally, the APOE ε4 allele affects the dFC between the left posterior cerebellar lobe and the left middle temporal gyrus, which is linked to executive dysfunction in AD.
Consistent with previous studies we observed more severe cognitive decline in APOE ε4 carriers than in APOE ε4 non-carriers. 27 APOE ε4 has a gene-dosage effect that affects the severity of hippocampus deformation and linked to accelerated cognitive decline. 28 Given the modest number of APOEs, we did not identify variations in AD plasma markers between the APOE ε4 carriers and noncarrier group. In our work, among 33 APOE ε4 carriers, most were homozygote (ε3/ε4) and only one heterozygote (ε4/ε4). In China, the frequency of homozygote (ε3/ε4) and heterozygote (ε3/ε4) in sporadic AD (SAD) was 28.82% and 5.72%, respectively. Although China did not have the lowest prevalence of SAD, it did have the lowest prevalence of APOE (36.23%), compared to South Korea (46.25%), Japan (48.92%), Brazil (49%), Colombia (49.37%), Spain (51.15%), Germany (53.04%), America (55.84%), the United Kingdom (56.16%), France (56.36%), Australia (62.44%), and Canada (64.20%). 29 A research from the ADNI database indicated that compared with APOE ε4 noncarriers, APOE ε4 carriers had higher baseline levels and quicker rates of rise in Aβ PET, CSF P-Tau18 and cognitive decline. 30 Larger sample numbers in the Chinese population are necessary for research to validate the link between APOE and AD plasma pathology biomarkers, as well as the effect of the dFC states of different APOE genotype in AD.
Resting-state dfALFF, and dReHo analysis revealed abnormal variability in AD with APOE ε4 carriers in the posterior cerebellar lobe and the precuneus. Large-scale dFC analysis revealed abnormal resting-state temporal dynamics in specific brain areas, primarily between the cerebellar and the DMN, the central executive network (CEN).
Based on previous studies, the dFCs of the brain would have better predictive power than sFC in distinguishing AD and non-AD, and that this would be associated with overall cognitive ability. 31 Significant abnormalities in dFC variability in the brain region might predict declines in cognitive ability during AD progression. 32 Combining the genetic risk factors of AD with dFC analysis may increase our knowledge of cognitive differences and pathological heterogeneity between APOE ε4 carriers and noncarriers patients. In our study, AD with APOE ε4 carriers had significantly lower levels of dfALFF, and dReHo in the left posterior cerebellar lobe. Lower dfALFF values indicate poorer regional blood oxygenation signal strength. The sliding-window approach discovered that brain regions with high dReHo fluctuation are functional hubs in the brain system, whereas lower dReHo indicates the delineation of local FC, 33 suggesting that APOE ε4carriers with AD may experience unstable neurofluctuation in the left posterior cerebellar lobe during the resting state.
For decades, the cerebellum was thought to only be responsible for controlling motor tasks.
Nowadays its role in cognitive and affective disorders is well established. 34 The cerebellum consists of 10 lobules: anterior (lobules I-V), posterior (lobules VI-IX), and flocculonodular (lobule X). Various cerebellar areas handle sensory, cognitive, and emotional information. Sensorimotor homunculi have been found in lobules III-VI and lobule VIII. 35 The posterior lobe of the cerebellum has been related to the so called ‘cerebellar cognitive affective syndrome’, previous studies have found that the hemispheric portion of the posterior lobe was primarily involved in AD. 36 We also discovered aberrant local connection abnormalities in the left cerebellar posterior lobe of AD APOE carriers, the evidence for the influence on global brain functional connectivity in AD patients is not conclusive. To investigate the dynamic interactions between the left posterior cerebellar lobe and other brain networks, we used it as the seed area and performed a dFC of the entire brain.
In our work, seed-based dFC revealed reduced connectivity between the posterior cerebellar lobe and various brain regions in APOE ε4 carriers and non-carriers. This included decreased variability in the left posterior cerebellar lobe and left middle temporal gyrus, which is positively correlated with executive function. An intermediary investigation discovered that the APOE genotype affects executive function in AD patients via affecting the left posterior cerebellar lobe, which is related to dFC in the left middle temporal gyrus. Functional MRI studies in humans shows cerebellar activity during many cognitive activities, including linguistic, visual-spatial, executive, and working memory. Different regions of the cerebellum participate in these “cognitive” networks with prefrontal and parietal association cortices. 37 There is evidence that the cerebellum influences memory function through the executive aspects of memory rather than directly affecting memory operations, the differences in cerebellar FC between MCI and AD patients were linked to impaired cognitive performance, particularly in executive functions. 38 Regions such as the middle temporal gyrus and the superior frontal gyrus are mainly thought to be associated with the CEN. They are involved in higher cognitive functions such as decision making, planning, working memory, attention and task switching. 39 Consistent with previous studies, the current analysis suggests that disparities in dFC between cerebellar seeds (the posterior cerebellar lobe) and the rest of the brain may contribute to the observed executive functions performance gap between APOE ε4 carriers and non-carriers AD patients, rather than other cognitive domains.
Our results indicate that an increase in dfALFF in the right precuneus and a lower dFC in the right precuneus and left middle frontal gyrus among APOE ε4 carrier AD patients, which was negatively linked with information processing speed. The DMN is an important network connected to cognitive function, and the functional connectivity of the DMN network is damaged in the brains of AD patients, with the precuneus being one of the most vulnerable locations, which could be an early predictor of memory loss. 40 In the current study, APOE ε4 carrier AD patients demonstrated elevated dfALFF in the right precuneus. This modification may be related to compensation associated with reduced functional connectivity across the AD brain.
Our study found that the APOE ε4 gene affects cerebellar FC and is associated with cognitive deficits in AD. Previous studies have also demonstrated that the APOE ε4 gene affects grey matter volume and cerebellar volume in the cerebellum of AD patients with superimposed effects. 41 The APOE ε4 allele was formerly thought to initiate Aβ accumulation at the top of the SAD amyloid cascade. However, new research indicates that the APOE alleles have varied downstream impacts on several pathophysiological processes beyond Aβ metabolism. It is unclear whether the pathogenic consequences of the APOE ε4 gene result in loss of protective activity or the emergence of detrimental function. Although in this work there is no difference in plasma Aβ42/40 and P-tau181 between APOE ε4 carriers and non-carriers AD patients, we detected changes in dFC. This conclusion can be explained by a number of non-exclusive mechanisms by which APOE may be involved in AD. Due to the multiple roles of APOE in AD pathophysiology, other plasma, CSF, and PET biomarkers which have been linked to other aspects of AD such as tau-induced neurodegeneration, neuroinflammation (microglial and astrocyte reactions), synapse failure, and disruption of the blood-brain barrier should be used to investigate the mechanism of APOE.
Although this investigation discovered the characteristics of cerebellar functional connectivity abnormalities among APOE ε4 carrier AD patients and their relationship with executive abilities. However, it has some limitations and can provide insights for future research. First, this study evaluated a limited number of subjects, we exclusively investigated the impact of APOE ε4 on brain functional activity in AD patients, include the APOE ε4 carrier without cognitive impairment is challenging. Future work is encouraged to assess a larger sample size and verify our current findings. Secondly, APOE ε4, the risk gene for AD, is dosage dependent. In this work, the genotype of APOE ε4 carriers is generally heterozygous, with very few homozygotes, making it impossible to further investigate the pathogenic mechanism of functional connection between the cerebellum and brain influenced by the APOE ε4 gene in Chinese AD patients. Future research should investigate the role of genes in AD progression by combining biomarkers related to core pathologies and non-specific tissue reactions, such as Aβ42/40, P-tau181, P-tau1217, microtubule-binding region 243, neurofilament light chain, glial fibrillary acidic protein, and others.
Limitations
This study has a few limitations that need to be taken into account. First, we only analyzed the effect of APOE ε4 on brain functional activity in AD patients and did not include the normal population. Second, APOE ε4 is dose dependent. The genotypes of APOE ε4 carriers in this study are basically heterozygous, and the sample size of ε4/ε4 homozygous patients is small, so it is impossible to further analyze the influence of ε4 dose on the study. Because of the relatively small sample size in the present study, large-sample, longitudinal studies are needed to further validate our results and uncover more details regarding AD pathology. Furthermore, due to the limited sample size of participants, the study did not analyze the effect of different stages of disease progression among participants.
Conclusions
In conclusion, our study demonstrated that APOE ε4 carriers experience more severe cognitive deterioration in AD patients. The APOE ε4 gene may impair cognitive function particularly executive function in AD patients by weakening the connection between the cerebellum and brain. This study contributes to a better understanding of the role of the APOE ε4 gene in the degenerative process of AD. Based on the status of APOE ε4 alleles carried by individuals, the FC variability of brain regions can be personalized monitored for early identification of AD. It also allows more targeted interventions and therapy approaches for APOE ε4 carriers AD patients.
Footnotes
Acknowledgments
We wish to thank all of the participants, their relatives, and all individuals who helped with data collection, for their fundamental contributions to the study.
Ethical considerations
The studies involving human participants were reviewed and approved by the Drum Tower Hospital Research Ethics Committee.
Consent to participate
The participants provided their written informed consent to participate in this study.
Consent for publication
Not applicable.
Author contributions
Chengbing Gong (Formal analysis; Writing – original draft); Wenting Song (Writing – original draft); ZhengYang Zhu (Data curation); Dan Yang (Methodology); Xiang Zhao (Funding acquisition); Yun Xu (Conceptualization; Writing – review & editing); Hui Zhao (Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Nanjing Medical Science and Technology Development Key Projects (ZKX23026).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.