
Abstract
Background
The recent approval of anti-amyloid therapies (AATs) for Alzheimer's disease (AD) has introduced new complexities into clinical care. While offering therapeutic promise, AATs necessitate changes in practice models, infrastructure, and team responsibilities. Understanding clinician and system-level adaptations is critical to guide implementation.
Objective
To explore how clinicians adjust clinical workflows and care processes when integrating anti-amyloid treatments into AD management.
Methods
We conducted semi-structured interviews with neurology and geriatrics clinicians across seven academic medical centers to explore perspectives on AAT implementation. An interdisciplinary team used hybrid deductive-inductive coding and thematic analysis to identify themes.
Results
Twenty-seven clinicians (17 neurology, 10 geriatrics) participated. Three themes emerged: (1) Structural adaptations: Sites developed governance committees, eligibility protocols, and workflows for referrals, administration, and monitoring. Some hired new staff, and protocols evolved with experience. (2) Diagnostic shifts: Clinicians reported heightened pressure for earlier, more precise diagnoses, prompting greater biomarker use and structured disclosure visits incorporating treatment discussions. (3) Cultural change: While clinicians described optimism about disease-modifying therapies, they expressed ethical concerns about resource allocation, over-medicalization of early dementia, and diversion of resources from broader dementia care.
Conclusions
The findings reflect evolving institutional protocols, clinical roles and responsibilities, and ethical tensions within the clinical workforce in response to AAT administration and access to early diagnosis and treatment.
Introduction
The anti-amyloid monoclonal antibodies (mAbs) lecanemab and donanemab are the first disease-modifying therapies to receive full FDA approval, and the first approved therapy of any kind in more than 20 years, for the treatment of mild cognitive impairment and mild dementia due to Alzheimer's disease (AD). 1 These therapies slow progression of cognitive decline in early-stage AD, offering a new avenue for therapeutic intervention.1–4 However, they are associated with significant adverse effects, including infusion reactions as well as amyloid-related imaging abnormalities with edema/effusion (ARIA-E) and hemorrhage (ARIA-H), which are often asymptomatic but can occasionally be disabling or fatal. 5 Furthermore, treatment requires substantial logistical coordination, including infusion administration, intensive monitoring with serial MRIs, side effect surveillance, and multidisciplinary care, requiring significant changes to clinical practice. 6
Prior studies of implementing new treatments, such as targeted cancer therapies and immune checkpoint inhibitors, have demonstrated that successful implementation requires changes to clinician workflows, practice personnel and resource infrastructure, and clinical management processes.7,8 These challenges are amplified when treatments carry complex risk profiles, require specialized diagnoses and treatment monitoring, or demand new care coordination pathways, as is the case with anti-amyloid therapies. Failure to anticipate these changes can lead to suboptimal patient outcomes, inequitable access, and clinician burnout. 9 Therefore, systematically describing how anti-amyloid therapies are impacting clinical practice—from logistics and resource demands, workflow adjustments, and clinicians’ experience—presents multiple opportunities. These learnings can provide a deeper understanding of how health systems might achieve sustainable, accessible, and high-quality implementation strategies for anti-amyloid therapies presently, and can inform the future implementation of novel therapies in other fields that change traditional care models. Furthermore, unpacking the experiences in the dementia care specialties are particularly interesting given that novel anti-amyloid therapies are the first treatments of their type to be widely used.
To date, limited research has examined how clinician perceptions about AD diagnoses and treatment may be changing and how clinicians adapt their workflows as they incorporate anti-amyloid therapy into clinical practice. We conducted a qualitative study to characterize the structural changes and practice adaptations that clinicians navigate as they implement anti-amyloid therapies into the care of individuals with AD.
Methods
Study design and data collection
This qualitative study used semi-structured interviews of health professionals and 10 adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 11 The study protocol was approved by the Mass General Brigham Institutional Review Board (2023P002711). All participants provided verbal informed consent and completed a demographic survey.
Qualitative data collection
Between August and October 2024, we conducted 27 semi-structured interviews of a purposive sample of physicians and advanced practice providers from neurology and geriatrics clinics at seven academic medical centers in the U.S. Five participants declined interview participation (84% response rate). We did not record reasons for refusal. Participants were deemed eligible if they worked in specialty memory care clinics and evaluated patients for lecanemab eligibility, prescribed lecanemab, or supported implementation efforts. This study had two primary aims. The first aim (reported previously) 12 explored clinician experiences communicating with patients and caregivers about lecanemab, including discussions of benefits, risks, and shared decision-making processes. The second aim (reported in this paper) explores lecanemab implementation, such as clinic infrastructure, interdisciplinary coordination, and practice changes. These interviews focused on lecanemab since they were conducted before donanemab availability. 13 Interviews were digitally recorded, transcribed verbatim, and de-identified. Participants were recruited from seven U.S. academic medical centers in the Southeast, Northeast, West, and Midwest via direct email outreach and snowball sampling. We recruited clinician participants at each site through professional networks of the research team and subsequently used snowball sampling, whereby initial participants recommended additional clinicians for invitation. AP (female MD hematology physician researcher with extensive qualitative research experience) or AT (male BS clinical research coordinator with extensive qualitative coding experience) emailed each potential participant directly with an invitation to participate, including a study fact sheet describing the purpose and procedures of the interview. Interviews were scheduled with those who agreed to participate. At the beginning of the video conference or telephone call, AP or AT conducted verbal informed consent and completed the demographic survey with each participant. Upon completion of these components, the interview began. Interviews were conducted remotely and recorded via Zoom or telephone for 40–60 min by trained study personnel (AP, AT, DD (male PhD sociologist with extensive qualitative research experience)) using a semi-structured interview guide (Supplemental Material). No repeat interviews were conducted. We used ‘information saturation’ to determine when to cease data collection, or the point at which the interviews produced no novel insights or new information. 14 Transcripts were not returned to participants for comment and/or correction.
Data analysis
We used thematic analysis for this study. The primary qualitative research team included three authors: AP, AT and JP (female MD palliative care physician researcher with extensive qualitative research experience). AP, AT, and JP coded an initial five transcripts independently using inductive coding. They then met to discuss codes and resolve differences by consensus to create an initial codebook before individual coding of remaining transcripts. Using constant comparative analysis, AP, AT, and JP met regularly to reconcile differences, refine definitions, and ensure a consistent and focused interpretation, ensuring the codebook aligned with the pre-specified aims of the analysis. The final codebook was then systematically applied to the full dataset. AP, AT, and JP, the three initial team members, then met regularly with DD, SS (male MD hospitalist), and SG (male MD neurologist) to synthesize the coded data into themes and sub-themes, which were iterated and refined until the final themes were reached. While we did not maintain formal analytic memos for each interview, we systematically recorded analytic reflections through debrief discussions after interviews, larger study team meeting notes, and documentation of coding decisions in line with the consensus-building approach we have described. We incorporated these reflections into codebook refinement and thematic development to make sure that interpretations were transparent and systematically applied. The team also engaged in reflexive discussions to acknowledge and mitigate potential bias. 15 We did not conduct formal member checking of the findings due to logistical constraints since we interviewed busy clinicians with limited availability across multiple academic centers. Instead, we ensured rigor through multiple coders, iterative codebook development, and regular analytic consensus meetings and reflexive discussions. 16
Results
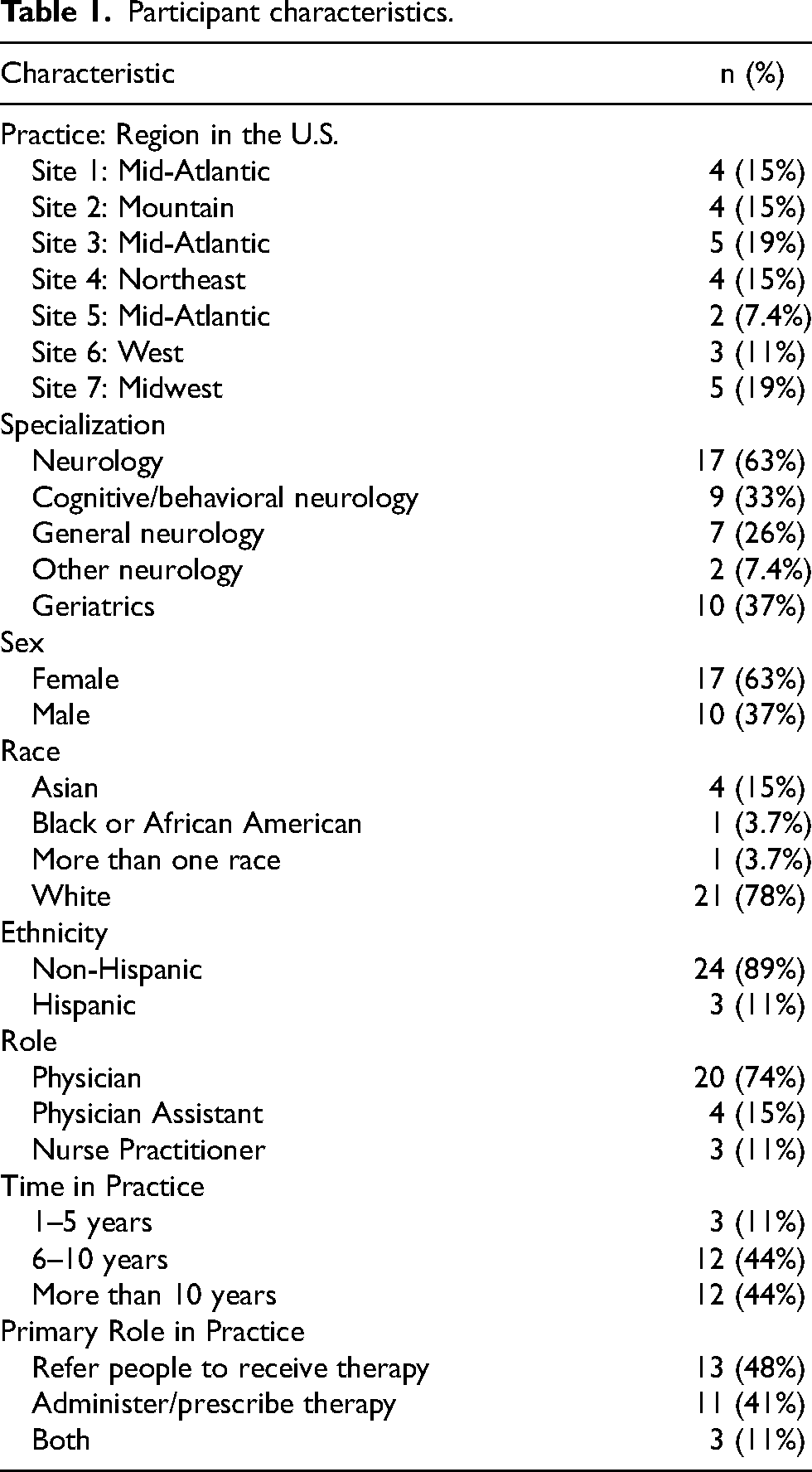
Characteristics of the 27 participants in Table 1. Most clinicians were Women (63%), White (78%) and physicians (74%) trained in Neurology (63%).
Participant characteristics.
The analysis revealed 3 major themes and associated subthemes: (1) Structural changes to support implementation of lecanemab; (2) Practice transformation around dementia diagnosis; (3) Shifts in clinical culture and practice with both benefits and burdens. Representative quotations are presented in the manuscript text. Table 2 provides additional supportive quotations.
Illustrative quotes categorized by theme and sub-theme.

Theme 1: structural changes to support implementation of lecanemab
Clinicians across all institutions noted that they implemented structural changes to support the delivery of lecanemab. First, institutions established clear protocols to guide patient eligibility that initially adhered closely to enrollment criteria (inclusion/exclusion) from the lecanemab Phase 3 trial (CLARITY AD) and/or published, expert consensus-based appropriate use recommendations. However, clinicians noted changes to aspects of their protocols over time, such as allowing patients taking certain other immunotherapies concurrently to be treated. “We started with the Clarity AD protocol. The other sources have been the appropriate use recommendation paper. We all started really rigidly around this…because we’re all scared of hurting somebody, understandably. We’ve seen some relaxations of particular points along the way. Everybody [initially thought]- you can’t be on another monoclonal [antibody]. We’re still insisting people not take Prolia, but other places are saying “It's probably fine”. Those are the things that I’ve seen really start to shift over the last six months.” (Site 3, ID 10, Neurologist, MD) “We have a multidisciplinary committee that includes neurologists and other clinicians, but also neuropsychology, radiology, nuclear medicine, ethics, and we meet twice a month and review all the individual referrals from the practice and discuss the clinical criteria. We review the biomarker results. We review the safety results, the APOE genotype, and then the committee discusses the case. I think in all but one instance we’ve reached consensus about whether to offer therapy. There was one instance where it went to a vote because we weren’t able to have full consensus. As a practice, we felt that it would be most fair to patients, and probably offer them the best care if we had a more uniform approach.” (Site 6, ID 21, Neurologist, MD) “Things keep changing, and the limitations that we had set up before may not completely apply as some groups are being more free with …different anti-platelet medications and blood thinners. But for the most part, I do tell patients that TPA, if they were to need TPA or similar medications to that, that they would not be able to have those treatments, which I think is a harder stop than some other medications.” (Site 3, ID 11, Geriatrician, MD) “We decided not to offer it to people who are APOE4 [homozygous]. We do offer it for people on anticoagulation, which is a little bit different than some places just because there has been some data…..Of course you inform people about those things, but it seemed to us that the APOE4 s were more high risk that we thought maybe the benefit wouldn’t necessarily outweigh the risk if we aren’t even sure how much benefit there is.” (Site 5, ID19, Neurologist, MD) “How this has impacted my job is I would say that there's more uncompensated navigational work because the healthcare systems frankly don’t care that we’re doing this on our backs without support and would like for us to demonstrate to them that it's effective, all the while, generally, providing benign neglect for support staff.” (Site 3, ID 10, Neurologist, MD) “We have a nurse navigator that was, part of my agreement with the health center… I told them that I couldn’t do this in my division without additional support. The nurse navigator has to keep careful track of everybody who's going through the process from insurance authorization to the timing of MRI scans.” (Site 5, ID 18, Neurologist, MD)
“We hired a bunch of nurse practitioners and a P.A. to manage a lot of this stuff. We’ve had to hire several office staff to help with all the coordinating the MRIs and ordering things and dealing with insurance. The whole clinic has expanded into a much bigger operation…For the actual providers—we’re fortunate enough here that we have some support from our healthcare system and from our [Alzheimer's Disease Research Center] that we can actually hire more people to help.” (Site 7, ID 23, Neurologist, MD)
Theme 2: practice transformation around dementia diagnosis
Clinicians emphasized that the implementation of anti-amyloid therapy has shifted clinical practice norms around dementia diagnosis compared to before their availability, including an increased perceived pressure for timely and accurate diagnoses. The steps to determine patient eligibility, combined with the short time window for anti-amyloid treatment for only early symptoms, drive processes to evaluate and confirm the specific cause of patients’ mild cognitive impairment or dementia syndrome more quickly than before. Clinicians noted their increased use of, and insurance coverage for, biomarker-based diagnostic modalities in clinical practice, such as amyloid PET scans or other biomarker testing. These tests are both required by widely accepted anti-amyloid treatment eligibility criteria but also add the specificity needed to diagnose AD independent of treatment. “Now we have pressure that we didn’t have before, the pressure of making accurate diagnosis. Before, it was like, “Okay. This looks like probably Alzheimer's disease. Here's this pill for…your memory.” If it was not Alzheimer's disease, it didn’t matter that much….The negative consequences of misdiagnoses, it was not that grave….Now we need to be more accurate. We have to use all these biomarkers to confirm the diagnosis. We need that—to do that in a timely fashion, because there's a time window for this treatment. Once you pass that time window, then it's not approved.” (Site 4, ID 17, Neurologist, MD) “Actually, for me, it really has changed the outlook of the treatment that we do for Alzheimer's disease because the diagnosis has changed. Now, we have new modalities that Medicare is paying for, like PET scans that before we only did in research and now we can do it in clinical practice. For me actually, that's been great to have that availability of new resources that we can use for diagnosis because it adds a specificity.” (Site 4, ID 14, Neurologist, MD)
Now that it's approved and that we have more biomarkers, the work about diagnosis and biomarkers, you can’t really not talk about the disease modifying therapy these days. They have to be in the background. Why would we disclose this to a patient? What will we do when we do? How we make decisions, how lecanemab gets used in the community, is an important part of the assessment process now. (Site 6, ID 22, Neurologist, MD)
When I see a new patient, and I’m doing my assessment, if at the conclusion of that assessment, we are discussing Alzheimer's disease because I’m concerned that that could be contributing to their symptoms, then when I’m discussing the option of testing, I will first ask if they’ve heard about the drug. I’ll briefly just mention that say, you know, the testing is consistent with Alzheimer's, and I’ve already kind of reviewed to see if they would meet eligibility criteria based on the appropriate use guidelines already. (Site 1, ID 1, Geriatrician, MD)
“I’ve seen the patient three or four times, because there's an initial evaluation, and then we, order testing, and then I do a lumbar puncture, and so usually when we’re having this discussion after the lumbar puncture….then… we’ve looked at the MRI…and the PET scan, and we have biomarkers which can say yes or no, this is Alzheimer's disease. Then I can talk about the risks and benefits of treatment.” (Site 2, ID 6, Neurologist, MD) “There's a three-step process before they get the drug… There's an initial one, and then there's one that happens with our head nurse. Then, there's another one that happens with the physician and with our coordinator that we’ve hired to do the antibody treatments….At one point, the health system was pushing on us and saying, “Couldn’t you reduce some of these.” The doctors that set this up said, “Nope. That's a feature, not a bug, of our process. We want people to have three different opportunities. These are cognitively impaired people. Repetition is important. We wanna make sure that people hear it every single time.” (Site 1, ID 3, Neurologist, MD)
“And I intentionally space this out because on average I’m having three or four visits with people before we consent to start treatment because I really want to make sure that they understand what this involves, what the risks are, the logistical considerations, and that's something they really want to pursue. We can have as many of these sessions as-as you need to feel confident that this is the right decision for you.” (Site 1, ID 1, Geriatrician, MD)
Theme 3: shifts in clinical culture and practice with both benefits and burdens
Clinicians in this study described the ways in which the discovery and implementation of disease-modifying therapies in AD care brings a new sense of hope and fulfillment for clinicians and patients due to the ability to intervene and potentially slow cognitive decline, counteracting longstanding feelings of nihilism in AD care. Clinicians’ expressions of hope reflect both the new treatments that are available now for patients as well as potential for future treatments down the line. In addition, clinicians cited recent historical parallels of treatment advances, such as in stroke and oncology care, that illustrate the sense of hopefulness that these AD therapies have created. Clinicians also described that the availability of anti-amyloid therapy has increased public awareness of the disease and potentially motivated individuals to seek an earlier diagnosis and adopt lifestyle changes to preserve brain health. “I think it being in the most general sense, just having these drugs available is helpful and hopeful for patients. I certainly tell all my patients, whether they’re eligible or not, that this is the first disease-modifying therapy we’ve had, and there's more to come. I think it does imbue a sense of hope that we have been lacking for a while.” (Site 7, ID 23, Neurologist, MD) “This reminds me a lot…[of] the transition from, “Okay. You have stroke-like symptoms. This is a stroke….we’ll do a CAT scan today, but MRI we’ll do in two days. Here's your aspirin. We’ll transfer you to rehab,” to the era of intravenous TPA, where you have to three or four hours. Then, from that era to the thrombectomy…You apply the protocols, the guidelines, and a lot of disability has been prevented. Hopefully, with these treatments for Alzheimer's, we’ll be able to slow down the progression. That's the hope that I have, personally.” (Site 4, ID 17, Neurologist, MD) “For my patients, it's definitely changed the relationship in the sense for a tertiary care expert like me, even though I provide care, it's fairly light touch, except when big things come up….Even then, it's often best for primary care to deal with that in terms of doing additional assessment. That used to be what it was. “Hopefully, things’ll go great, but if they don’t, I’m here. Meanwhile, we’ll check on you in a year.” That was a very standard thing to say with somebody with MCI.” (Site 6, ID 22, Neurologist, MD) “Behavioral Neurology never had urgencies. We were a place where you could be referred and it's nine-month wait, no big deal. There was no treatment anyway, which I’m being facetious about a bit ‘cause I do think that we palliatively help people significantly but there is no urgency really. All of a sudden, there is a sense with some people that this is like a cancer diagnosis, and you have a cancer treatment that you can’t even offer me for nine months. There's a perception of this really important ability to intervene.” (Site 3, ID 10, Neurologist, MD)
“I would say that there are times I worry that we don’t have enough time or bandwidth now for dementia management. We used to do so much….for a disease that doesn’t have a pharmacological cure, we do an awful lot—we do a really good job taking care of patients and families because a lot of visits were spent with what a lot of times is what the family is craving, which is just, “Give me a trick or a tool or the suggestions of how I can make bath time less of a battle,” or “how I can make—how we can have a conversation about driving,” or, “what do we think about in the future in terms of financial planning and home planning.” (Site 1, ID 3, Neurologist, MD)
- You kind of lose a little bit the soul of the field. A lot of it is neuro-palliative care. It's building a therapeutic alliance, preparing somebody for the process of having a chronic disease, building support structures, healthy coping strategies, all of those things. It's careful clinical phenomenology, this observation of behavior and localization of these complex cortical behaviors like language and appetite and all these other things that we had, that we’ve built up because we’re trying to understand the disease. I’ve had this conversation where I hope we don’t kind of lose our soul as a field. Now, just ‘cause we have a handful of partially effective treatments, I hope we don’t lose that completely, but I feel myself being pushed in that direction, 100 percent. I don’t see a lot of new patients anymore because most of my time is actually just managing patients that are referred in and are getting the Lecanemab therapy.” (Site 6, ID 21, Neurologist, MD)
Discussion
The availability and implementation of anti-amyloid therapies have significant implications for dementia care. Our findings demonstrate that institutions have started to implement structural and workflow changes to support anti-amyloid referrals and treatment programs. Clinicians also experience changing roles and norms around dementia diagnosis as well as shifts in clinical culture and practices. Clinicians compared these changes in early dementia care to an oncology-like care model, characterized by biomarker-driven diagnoses, subspecialty consultation, structured referral and treatment pathways, and intensive monitoring for therapy-related risks.
The study identified key structures and processes to support anti-amyloid therapy implementation across seven academic institutions. Most systems developed standardized governance structures and eligibility protocols17,18 to oversee lecanemab administration, including interdisciplinary committees that are similar to ‘tumor boards’ in oncology. 19 These committees determine patient eligibility criteria for treatment and deliberate patient cases. Such structures were implemented to ensure safety and fairness in access to treatment, to enable consistency and transparency in eligibility determination, and to align with existing consensus-based clinical guidelines. 18 Prior research in oncology, for example, has demonstrated the benefits of multidisciplinary committees, including enhanced adherence to clinical guidelines, improvements in treatment outcomes, and overall improvement in decision-making processes. 19 Most clinicians also noted that their healthcare systems hired and/or redeployed administrative staff and advanced practice clinicians to manage patient referrals, implement workflows for eligibility determination and informed decision-making, and oversee lecanemab infusion-related processes and monitoring for risks longitudinally.
There are several implications of our findings. Such structural changes signal a shift to a more specialized and medically intensive model of early dementia care focused on disease modification. Furthermore, clinicians and staff in dementia therapeutics are developing and refining specialized expertise and skillsets that may help them deliver the most optimal and safe care. Gaining a real-world understanding of the infrastructure, workflows, skillsets, and evolving ‘best practices’ in delivering therapy can support ongoing cross-system learning and information exchange. 20 However, the specialized diagnostic infrastructure, staffing and resources needed to support anti-amyloid delivery will likely exacerbate disparities in access to treatment, including to individuals in rural settings and racial and ethnic minorities who already face significant disparities in dementia care.21,22 As implementation continues to mature, decision-makers in health systems needs to focus their attention on reducing these disparities to ensure access to available treatments for all.
This study demonstrates that the roles of neurology and geriatrics clinicians are actively evolving as they navigate and integrate new and complex clinical discussions in early dementia care. For example, clinicians noted that administration of lecanemab has catalyzed emerging shifts in the diagnosis of AD from a clinical-biological syndrome to a mostly biologically-defined one, increasing the use of expanded diagnostic criteria, blurring boundaries between diagnosis and treatment, and changing communication practices in routine care. These changes will be further amplified with emerging use of blood tests to detect tau and amyloid proteins in plasma, beginning with FDA's clearance of the first blood test in May 2025. 13 Corroboration of a diagnosis by blood testing promises significant scalability and, ultimately, reduced costs and burdens compared to PET scans and lumbar punctures. In addition, anti-amyloid therapies, with their modest efficacy and associated risks, generate hope and therapeutic momentum while also carrying risks and tradeoffs. Clinicians integrate nuanced discussions of the potential benefits, harms, and tradeoffs of treatment at the time of diagnostic disclosure, further changing norms around communication for these specialists.
To qualify further, the availability of disease modifying therapies have shifted clinicians’, patients’, and caregivers’ mindsets about therapeutic possibility. These changes introduce new ethical questions related to anti-amyloid decision-making due to the ‘pressure’ that clinicians can feel to discuss therapy and that patients can feel to pursue it. Prior studies show that patient wishes to start a diagnostic process for cognitive symptoms vary. 23 Patients and families may now be more willing to start down a dementia diagnostic pathway if there are desirable, expected outcomes of that process, including treatment options. It is this therapeutic possibility that is likely to bring more people with memory complaints earlier to medical attention. Furthermore, our prior study of patient experiences revealed that some patients felt compelled to pursue treatment to ‘do something’ rather than ‘nothing.’ 24 This mirrors prior studies of patients pursuing immunotherapy in cancer care which have demonstrated significant hope and the desire to ‘fight’ the cancer, sometimes at great personal risk or cost and without always having a full understanding of the benefits and risks.24–27 Clinicians in our study expressed cautious and nuanced understanding of the benefits of anti-amyloid therapies, which mirrors the recognition and serious engagement within neurology and geriatrics about the “grayness” and ethical considerations of anti-amyloid treatment. 28 One major implication of these findings is that communication practices, skills, and clinician training will have to adapt to the need for nuanced, complex shared decision-making conversations with patients and caregivers.
The availability of first(s)-in-class treatments for a progressive, fatal disease, which has never had a pharmacologic treatment that alters the disease's natural course, creates positive changes in dementia care while also introducing new challenges that clinicians and healthcare systems must navigate. The availability of new diagnostic tests and disease-modifying treatments offer hope for clinicians that such advances will have positive outcomes for patients (both now and in the future), which mirrors the hopes of patients that were described in our prior study. 24 However, implementation of anti-amyloid therapy also presents new tensions for the field related to resource allocation. Similar to sentiments expressed in recent commentary, 29 clinicians in this study shared thoughtful worries and concerns that directing clinician effort and institutional resources toward a small number of patients who are eligible for and receiving anti-amyloid therapy may potentially detract from essential efforts that would benefit the entire population living with dementia, including those focused on effective diagnosis, communication, care, and management. Notably, only a small subset of patients with dementia (8–20%) are eligible for anti-amyloid therapies. 30 Care efforts that are essential for all patients affected by dementia, for example, include careful symptom and behavioral management, promotion and facilitation of brain health and wellness, unhurried discussions about diagnosis and prognosis, and provision of personalized care planning, counseling, and support for caregivers.31,32
Clinicians in this study, while reflecting on their practice independent of and before anti-amyloid therapy, described a sense of pride in their delivery of holistic and comprehensive care for patients and caregivers who are affected by an illness that carries significant stigma and burden. Similar to other fields, the cultural narrative of disease-modifying and curative-oriented care risks overshadowing essential supportive services to meet the ongoing psychosocial and practical needs within dementia care. The disproportionate investments of dementia care resources in anti-amyloid therapy implementation (above other dementia care strategies) benefits individuals in early diseases stages and, at least initially, individuals from higher socioeconomic status, which will likely exacerbate existing disparities in dementia care access and outcomes. 33 Furthermore, health systems may prioritize AAT delivery over other critical services that may benefit larger socioeconomically diverse populations, like dementia-capable primary care, caregiver support, care coordinators, behavioral management, and community based dementia care.34–36
Strengths and limitations
While this study highlights clinician perspectives from seven geographically diverse academic medical centers across the United States, these sites are among the early adopters of anti-amyloid therapies, often benefiting from greater institutional resources, specialist expertise, and infrastructure. This concentration in well-resourced, academic settings represents a key limitation. As such, findings reported in this study may not be generalizable to other healthcare institutions or contexts, given that implementation challenges, patient selection processes, and clinician attitudes may diverge meaningfully from those described here. Furthermore, because this study used a purposive convenience sample to elicit a range of perspectives rather than a representative sample, it was not designed to compare and contract findings across sites or participant groups. Additionally, we interviewed physicians and advanced practice clinicians involved in prescribing anti-amyloid therapy, which may not reflect the full range of perspectives particularly those of nurses, social workers, care coordinators, and other frontline team members who play critical roles in patient education, monitoring, and care coordination. Similarly, the perspectives of patients and caregivers were not the focus of this analysis; however, these were explored in a related study from our group examining patient experiences with anti-amyloid therapy. 24 As this study centered on lecanemab, findings may not fully capture evolving clinician experiences with all/both anti-amyloid therapies; for example, donanemab differs in dosing schedule, risk profile, and management protocols. Furthermore, the potential approval of subcutaneous administration for donanemab, and extension of approval for lecanemab to include the first 18 months of treatment, may reduce logistical challenges. Querying clinician, patient, and care partner perceptions and experiences of these developments in future studies will be important to capturing a more complete picture of this evolving field.
Conclusion
The introduction of anti-amyloid therapies marks a transformative shift in AD care toward a more specialized, medically intensive model of early dementia care focused on disease modification. Our study demonstrates that implementation of disease-modifying therapies has already prompted changes in clinical roles and relationships with patients, the need to hire new clinicians and staff, shifts in dementia diagnosis and related discussions, the establishment of institutional structures to enact standardized protocols, and new workflows to manage referrals and patients on infusion therapy. Clinicians are navigating these shifts with both hopes and worries for current and future dementia care. As advances in disease-modifying therapies for AD and hopefully other dementias emerge, the potential for ‘cure’ must not overshadow the inveterate need for holistic care. Investments in infrastructure and workforce for disease-modifying therapies must be balanced with efforts to provide comprehensive, person-centered care for all individuals affected by dementia.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261422486 - Supplemental material for A qualitative study investigating clinician experiences with lecanemab implementation across seven academic medical centers
Supplemental material, sj-docx-1-alz-10.1177_13872877261422486 for A qualitative study investigating clinician experiences with lecanemab implementation across seven academic medical centers by Ayush Thacker, Anna L. Parks, Daniel Dohan, Liliana A. Ramirez Gomez, Christine S. Ritchie, Sachin J. Shah, Seth A. Gale and Joanna Paladino in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We appreciate the time and expertise of our study participants who contributed data.
Ethical considerations
The institutional review boards of participating institutions approved this study as exempt.
Consent to participate
Study participants completed verbal informed consent for participation.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Shah reports research funding from NIA (K76AG074919). Dr Parks reports research funding from NIA (K76AG083304). Dr Dohan reports research funding from the NIA (K07AG06681 and DP1AG069809).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.