
Abstract
Background
Amyloid-β (Aβ) pathology is a core feature of Alzheimer's disease (AD) and may be present in mild cognitive impairment (MCI). Accessible, non-invasive markers of early Aβ-related cognitive change are needed.
Objective
To investigate whether perceptual-phase eye-tracking metrics during figure copying are associated with Aβ-PET positivity in MCI.
Methods
In this cross-sectional study, 59 patients with MCI underwent 18F-flutemetamol PET and were classified as Aβ-PET positive (n = 34) or Aβ-PET negative (n = 25). Participants completed a simplified Rey-Osterrieth Complex Figure Test while wearing eye-tracking glasses. The display was then divided into perceptual and working areas of interest (AOIs), and metrics were extracted for each AOI. A matched-pair sensitivity analysis (n = 28) was performed to reduce differences in age, education, and Mini-Mental State Examination scores. Binary logistic regression was used to examine the association between Aβ-PET positivity and fixation duration in the perceptual AOI.
Results
The Aβ-PET positive group showed significantly longer fixation duration in the perceptual AOI (p = 0.027, r = 0.296), whereas no significant group differences were observed in the working AOI. Exploratory analyses showed higher fixation count, visit duration, visit count, and saccade count in the perceptual AOI of the Aβ-PET-positive group. Longer fixation duration in the perceptual AOI was independently associated with Aβ positivity (OR per second = 1.18, 95% CI 1.03–1.36, p = 0.021).
Conclusions
Aβ-PET positivity in MCI was associated with greater perceptual-phase gaze inefficiency during figure copying. Perceptual-phase eye-tracking metrics may serve as potential markers of amyloid-related visuospatial alteration in MCI.
Keywords
Introduction
Visuospatial function, one of the cognitive domains that progressively deteriorate in Alzheimer's disease (AD), is defined as the ability to perceive, integrate, and interpret spatial relationships and visual forms. Importantly, this function often declines early during the transition from mild cognitive impairment (MCI) to AD. 1 Longitudinal evidence further indicates that visuospatial deficits become evident approximately three years prior to the clinical diagnosis of AD, highlighting their potential as a sensitive early indicator of underlying AD pathology, even preceding substantial memory impairments. 2 Moreover, previous studies have shown that visuospatial deficits are not only characteristic of early AD-related cognitive decline but also closely linked to amyloid-β (Aβ) pathology.3–6 Despite this, visuospatial function remains relatively under-assessed compared with other cognitive domains, likely because conventional tests rely primarily on paper-and-pencil methods.
Compared to conventional paper-and-pencil visuospatial tests, eye-tracking has gained attention as a potential tool for assessing visuospatial dysfunction in AD.7,8 Recent studies have demonstrated that eye-tracking can differentiate individuals with MCI or AD from healthy older adults by analyzing visuospatial processing during daily activities,9–11 evaluating visual search performance, 12 and characterizing gaze patterns elicited by short movies and static images. 13 Moreover, eye-tracking metrics such as fixation duration, saccadic movements, and smooth-pursuit accuracy have been correlated with established cognitive measures, including Mini-Mental State Examination (MMSE) scores, 13 standard visuospatial test scores, 14 and cortical thickness 15 along the AD continuum. However, whether biological markers such as Aβ positivity are associated with eye-tracking metrics at comparable levels of cognitive impairment has not been fully established.
Given that eye-tracking metrics can capture visuospatial dysfunction, examining their association with Aβ pathology may provide insight into the mechanisms underlying visuospatial impairment. In our previous study integrating an eye-tracking approach with a simplified version of the Rey-Osterrieth Complex Figure Test (sRCFT),16,17 Aβ-positive AD patients demonstrated longer fixation durations and increased number of fixations, saccades, and gaze switches compared to healthy controls, suggesting higher cognitive effort during complex visuospatial tasks. In addition, an eye-tracking study in patients with AD reported medium-to-large effects in visual attention measures. 18 Building on these findings, we hypothesized that Aβ-positive individuals with MCI would require greater cognitive effort to compensate for visuospatial deficits than Aβ-negative individuals with MCI, as reflected primarily by longer fixation duration in the perceptual area of interest (AOI).
Therefore, we investigated whether Aβ-positive and Aβ-negative individuals with MCI differ in phase-specific eye-tracking metrics during the sRCFT, with a particular focus on the perceptual phase as a potential locus of early visuospatial alteration.
Methods
Study design
This cross-sectional study investigated the associations between eye-tracking metrics and Aβ-PET positivity in individuals with MCI at the Memory Disorder Clinic, Jeonbuk National University Hospital, between July 2021 and February 2024. During the study period, consecutive patients attending the Memory Disorder Clinic were screened for eligibility. Of these, 66 individuals who fulfilled the modified Petersen criteria for MCI and met the study inclusion and exclusion criteria were enrolled in the study. A priori power analysis using G*Power 3.1.9.7 indicated that at least 25 participants per group were required to achieve 80% power at α = 0.05, assuming a large effect size (d = 0.80). This assumption was based on a previous eye-tracking study in patients with AD that reported medium-to-large effects in visual attention measures. 18
Participant recruitment
Participants with MCI met the modified criteria proposed by Petersen and colleagues. 19 The inclusion criteria were: (1) subjective cognitive complaint by the patient or caregiver, (2) objective cognitive impairment below the 16th percentile of education- and age-matched norms in at least one of four domains (memory, visuospatial, language, or frontal-executive function) on the Seoul Neuropsychological Screening Battery,20,21 (3) normal daily functioning based on clinical judgment and the Seoul-Instrumental Activities of Daily Living (S-IADL) scale, 22 (4) no dementia, and (5) aged 60–89 years. Exclusion criteria were: (1) structural brain lesions on MRI (e.g., infarction, hemorrhage, tumor, hydrocephalus, and severe WMH defined as a Fazekas score of 3) or other neurological disorders that could affect cognitive function, (2) abnormal laboratory results, (3) moderate or severe vision loss (visual acuity < 0.3), (4) MMSE score < 19, and (5) education below the 6th grade.
All participants underwent diagnostic assessments including clinical interview, neuropsychological testing, MRI, and PET. Laboratory tests included a complete blood count, blood chemistry, thyroid function tests, vitamin B12 and folate levels, and syphilis serology. Aβ positivity was determined using 18F-flutemetamol PET based on a visual assessment, 23 and the final classification was established by multidisciplinary consensus among neurologists, neuropsychologists, radiologists, and nuclear medicine physicians.
All procedures were approved by the Jeonbuk National University Hospital Institutional Review Board (CUH2020-12-058), and written informed consent was obtained from all participants.
Neuropsychological assessments
All participants completed the standardized Seoul Neuropsychological Screening Battery,20,21 which comprises multiple cognitive assessments. Attention and working memory were evaluated using the forward and backward digit span tests. Language abilities were assessed with the Korean version of the Boston Naming Test (K-BNT), 24 while calculation skills were measured through three problems each in addition, subtraction, multiplication, and division. Visuospatial function was examined using the Rey-Osterrieth Complex Figure Test (RCFT). 25 Memory function was assessed through immediate and delayed recall tasks from both the Seoul Verbal Learning Test (SVLT) 26 and RCFT. Frontal-executive function was evaluated using the phonemic and semantic tasks of the Controlled Oral Word Association Test (COWAT) 27 and the Stroop word/color reading test. 28 Additionally, general cognitive status and depressive symptoms were measured using the MMSE, Clinical Dementia Rating (CDR) with CDR sum of boxes, the Geriatric Depression Scale (GDS), and the Seoul-Instrumental Activities of Daily Living (S-IADL) scale to measure instrumental daily functioning. 22
Experimental apparatus
We utilized the Tobii Pro Glasses 2 (Tobii Pro, Stockholm, Sweden), a wearable eye-tracking device designed for real-world research applications. This system records binocular eye movements at a sampling rate of 50 Hz and features a scene camera with a video resolution of 1920 × 1080 pixels at 25 frames per second (fps) in H.264 format. The 50 Hz sampling rate provides sufficient resolution for fixation-based analyses; however, it does not allow for fine-grained characterization of saccadic activity. Weighing approximately 45 grams, the glasses are lightweight and non-intrusive, allowing participants to engage naturally in tasks. For the figure-copying task, we employed a 12-inch digital tablet (Samsung Galaxy Book 12, Samsung Electronics, Suwon, Korea) with a resolution of 2160 × 1440 pixels, paired with a stylus (nib diameter = 0.7 mm, pressure sensitivity = 4096 levels, Samsung Electronics, Suwon, Republic of Korea) to accurately capture participants’ drawing performance.
Experimental design
Experimental setup and eye-tracker calibration
To minimize interference from direct sunlight and enhance the quality of eye-tracking data collection, our experiment was conducted in a traditional neuropsychological testing environment with soft, evenly distributed lighting. The eye-tracker recording unit was connected to a laptop equipped with Tobii Pro Glasses Controller software. The eye-tracking glasses were then securely fitted onto the participant, with careful adjustments made to ensure that the four integrated cameras could capture clear and accurate eye movement data. For calibration, a white calibration card (7 cm × 10 cm) with a black ring and a central black dot was positioned approximately 80 cm in front of the participant's eyes. Participants were instructed to focus on the black dot until the Tobii Pro Glasses 2 Controller confirmed successful calibration.
Simplified Rey-Osterrieth complex figure test
In our previous study, we developed a simplified version of the original Rey-Osterrieth Complex Figure Test and established its validity by comparing it with the original RCFT.16,17 The sRCFT consists of four global components (a large rectangle and diagonal, horizontal, and vertical crosses) and four local components (a square, double circles, three triangles, and four arrows). Scoring was based on both accuracy and placement, following the standardized scoring criteria proposed by Meyers. The raw scores ranged from 0.0 to 16.0. 16
In this study, participants copied the sRCFT while wearing eye-tracking glasses. The display screen was divided into two regions: the upper half was designated as the “perceptual space,” where the sample figure of the sRCFT was presented, and the lower half was defined as the “working space,” where participants reproduced the figure (Figure 1). Based on our previous studies, the perceptual space is considered to primarily reflect visuoperceptual processing, whereas the working space is regarded as indicative of visuoconstructional processes. 17
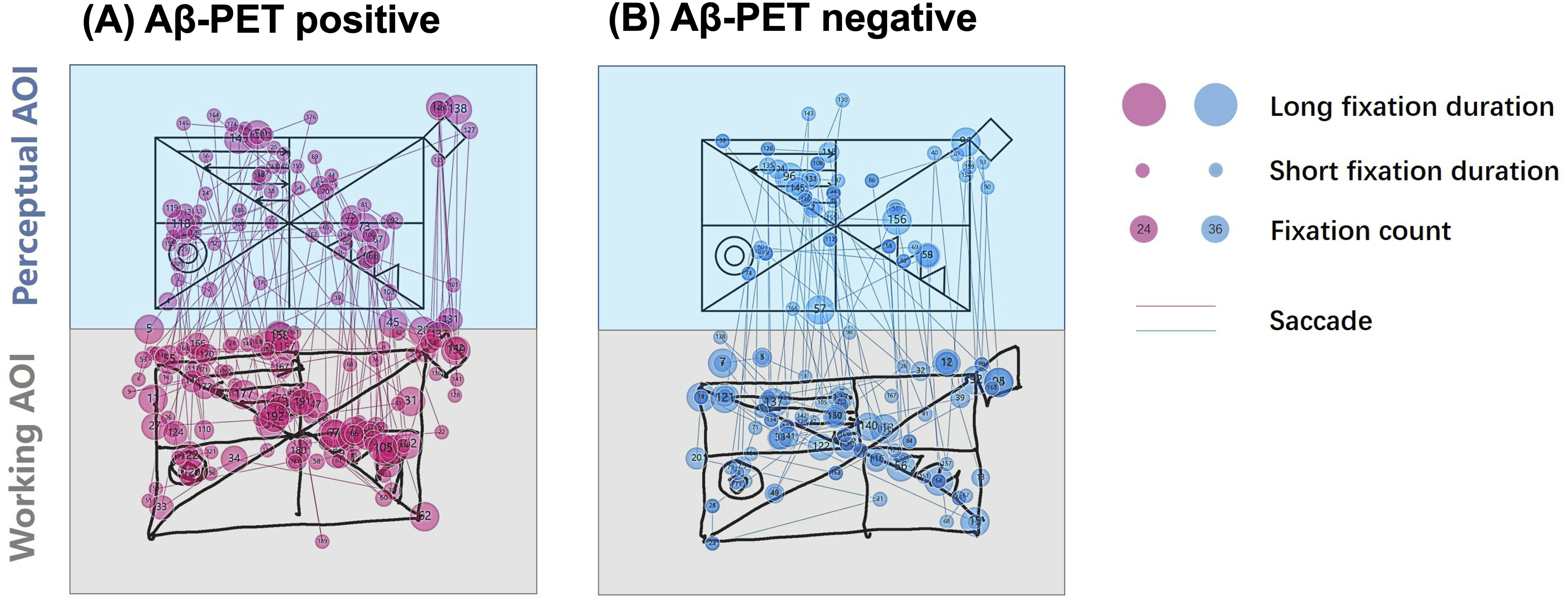
Representative gaze plots of an Aβ-PET positive (A) and an Aβ-PET negative (B) MCI participant during the sRCFT copying task.
Before the task began, participants were given the following instructions: “When the task starts, a sample figure will appear in the upper half of the tablet. Please copy the figure using this stylus, utilizing the empty space below as much as possible. The stylus does not have an eraser, and you will not be able to modify your drawing. If you make a mistake, forget about it and keep going. Take your time and let me know when you have finished.” The completion time for the sRCFT was defined as the interval between the end of the verbal instruction and the moment the participant verbally indicated that they had finished the drawing.
Eye-tracking data acquisition and preprocessing
Eye-tracking data were processed using Tobii Pro Lab software (version 1.181; Tobii AB, Stockholm, Sweden) for semantic gaze mapping, which aligned gaze coordinates with scene video recordings. Participants’ sRCFT snapshots were imported, and gaze data were automatically mapped and manually verified by the same experimenter for accuracy. Fixation, visit, and saccade metrics were extracted from two predefined areas of interest (AOIs): the perceptual and working spaces (Figure 1).
For quality control, recordings with > 10% tracking loss (fraction of samples with missing x–y coordinates) or metrics exceeding ±3 SD from the group mean were excluded. Before analysis, fixation duration in the perceptual AOI was designated as the primary endpoint based on our prior work 17 and the mechanistic focus of the present study on visuoperceptual processing, while all other metrics were considered exploratory.
Fixations, visits, and saccades were identified using the I-VT (Velocity-Threshold Identification) algorithm: fixations as gaze points with velocities below 30°/s, saccades as sequences exceeding this threshold, and visits as the time interval from the first to the last fixation within an AOI. Two fixation metrics (fixation duration and fixation count), two visit metrics (visit duration and visit count), and one saccade metric (saccade count) were extracted for each AOI.
For exploratory clinical interpretation, fixation duration in the perceptual AOI was additionally categorized into tertiles (low, middle, and high), and Aβ-PET positivity and selected neuropsychological measures were compared across tertile-defined subgroups.
Statistical analysis
Group differences in clinical characteristics, cognitive profiles, and eye-tracking metrics were analyzed using independent-samples t-test or Mann–Whitney U test for continuous variables and Chi-square test for categorical variables. To control for potential confounding effects of age, education, and MMSE score on eye-tracking metrics, a matched subgroup analysis (n = 28) was performed using paired t-tests or Wilcoxon signed-rank tests for continuous variables in the matched-pair analysis, and McNemar tests for categorical variables as appropriate. For the sensitivity analysis, Aβ-PET positive and Aβ-PET negative participants were matched 1:1 within ±2 years for age, within ±2 years for education, and within ±1 point on the MMSE score, with additional consideration of sex balance whenever possible. Matching was performed before comparing eye-tracking outcomes. Because of the limited sample size and the difficulty of identifying closely comparable pairs across multiple variables, only 14 matched pairs could be constructed from the full analytic sample.
To examine the association between eye-tracking metrics and Aβ-PET positivity, a logistic regression was performed with Aβ-PET positivity (0 = negative, 1 = positive) as the dependent variable and fixation duration in the perceptual AOI as the primary predictor. In the primary model, age, sex, education, MMSE score, and task-completion time were entered as covariates based on their clinical relevance and potential confounding effects. To assess the robustness of the findings, an additional sensitivity logistic regression analysis was performed, including APOE ε4 carrier status, SVLT delayed recall, and CDR sum of boxes, which significantly differed between groups and represented key disease-related domains. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. Model fit was evaluated using the Hosmer–Lemeshow test and Nagelkerke R2, and multicollinearity was assessed via variance inflation factors (< 5).
For exploratory clinical interpretation, participants were additionally categorized into tertiles according to fixation duration in the perceptual AOI. Trends in Aβ-PET positivity across tertiles were evaluated using Pearson chi-square test and linear-by-linear association test, whereas continuous neuropsychological measures were compared using one-way analysis of variance or the Kruskal-Wallis test, as appropriate.
All statistical analyses were performed using IBM SPSS version 29.0 (IBM Corp., Armonk, NY). Radar plots illustrating group differences in key eye-tracking parameters were generated using OriginPro, version 2025b (OriginLab Corporation, Northampton, MA, USA). Statistical significance was set at two-tailed p < 0.05.
Results
Clinical characteristics and cognitive performance
Of the 66 individuals initially screened, seven were excluded from the final statistical analysis. Three participants were excluded due to inadequate eye-tracking calibration caused by narrow palpebral fissures, two were excluded because of excessive tracking loss (>10%) based on quality-control criteria, and two withdrew from the study for personal reasons. The final analytic sample consisted of 59 participants, including 34 Aβ-positive and 25 Aβ-negative individuals.
No significant group differences were observed in age, sex distribution, and years of education. The prevalence of APOE ε4 carriers was significantly higher in the Aβ-positive MCI individuals (88.24%) than in the Aβ-negative MCI individuals (32%) (p < 0.001). In cognitive assessments, the Aβ-positive MCI individuals showed poorer performance on memory-related tests, including the Seoul Verbal Learning Test (SVLT) immediate recall (p = 0.01), delayed recall (p = 0.005), and recognition (p = 0.003), as well as RCFT immediate recall (p < 0.001), delayed recall (p < 0.001), and recognition (p = 0.002) scores. They also scored lower on the COWAT supermarket category (p = 0.004). Moreover, the MMSE scores were lower (p < 0.001), whereas CDR sum of boxes (p < 0.001) and S-IADL (p < 0.001) scores were higher in the Aβ-positive MCI individuals. Scores on tests of attention, language, and visuospatial function, including the sRCFT copy score, did not differ between the groups. Demographic and cognitive characteristics are summarized in Table 1.
Clinical and cognitive characteristics in all participants.
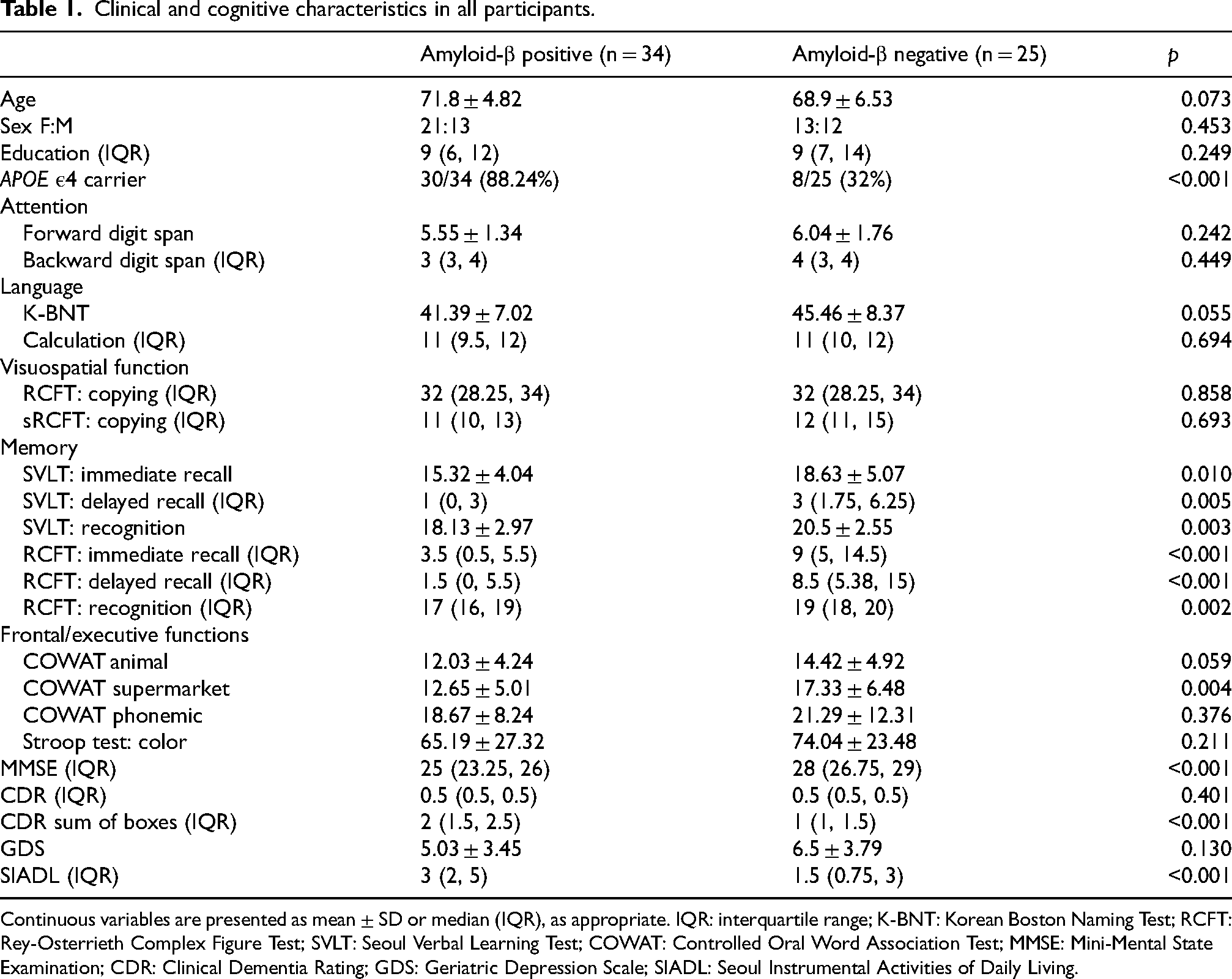
Continuous variables are presented as mean ± SD or median (IQR), as appropriate. IQR: interquartile range; K-BNT: Korean Boston Naming Test; RCFT: Rey-Osterrieth Complex Figure Test; SVLT: Seoul Verbal Learning Test; COWAT: Controlled Oral Word Association Test; MMSE: Mini-Mental State Examination; CDR: Clinical Dementia Rating; GDS: Geriatric Depression Scale; SIADL: Seoul Instrumental Activities of Daily Living.
To control for potential confounding effects of age, education, and general cognition (MMSE), we conducted a sensitivity analysis using a matched-pair design, yielding 14 matched pairs (14 Aβ-positive and 14 Aβ-negative). There were no significant differences in global cognitive or functional measures, but significant differences remained in RCFT immediate recall (p = 0.049) and RCFT delayed recall (p = 0.024) scores (Table 2).
Clinical and cognitive characteristics in the matched-pair analysis.
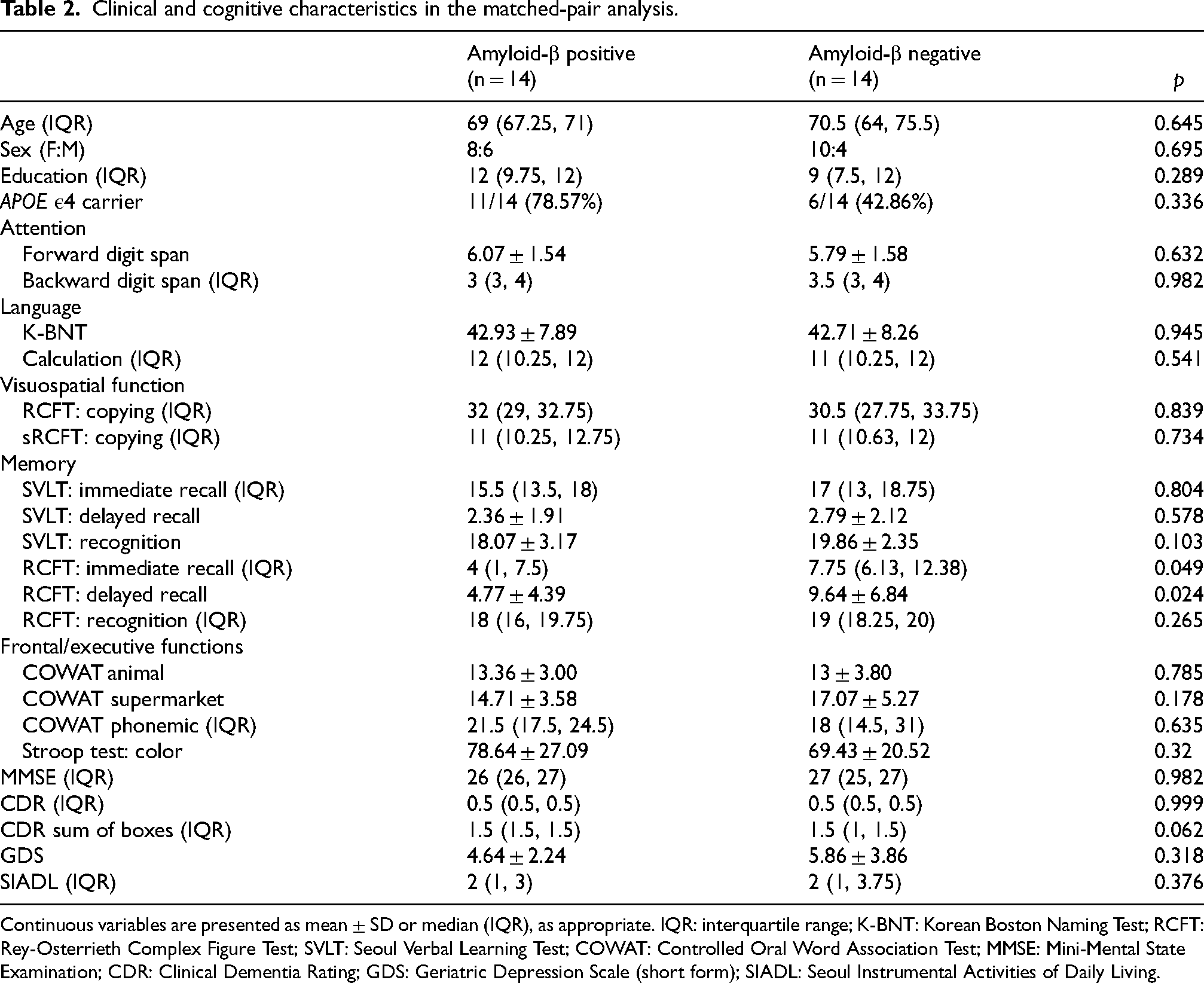
Continuous variables are presented as mean ± SD or median (IQR), as appropriate. IQR: interquartile range; K-BNT: Korean Boston Naming Test; RCFT: Rey-Osterrieth Complex Figure Test; SVLT: Seoul Verbal Learning Test; COWAT: Controlled Oral Word Association Test; MMSE: Mini-Mental State Examination; CDR: Clinical Dementia Rating; GDS: Geriatric Depression Scale (short form); SIADL: Seoul Instrumental Activities of Daily Living.
Eye-tracking metrics
Eye-tracking data were analyzed for the total, perceptual, and working AOIs. Metrics exceeding ±3 SD from the group mean were identified as outliers and excluded (1.03% of all data). No significant differences were observed between Aβ-positive and Aβ-negative MCI individuals in task completion time or in any of the eye-tracking metrics in the total AOI, including total fixation duration, total fixation count, total visit duration, total visit count, and saccade count.
When examining AOI-specific patterns, Aβ-positive MCI individuals showed significantly longer fixation duration in the perceptual AOI (p = 0.027, r = 0.296), the primary outcome measure. Exploratory analysis revealed higher fixation count (p = 0.018, r = 0.316), longer visit duration (p = 0.018, r = 0.316), increased visit count (p = 0.034, r = 0.285), and greater saccade count (p = 0.013, r = 0.322) compared with Aβ-negative MCI individuals in the perceptual AOI (Figure 2). In contrast, no significant differences were found in any eye-tracking metrics in the working AOI. The numeric results are summarized in Table 3.
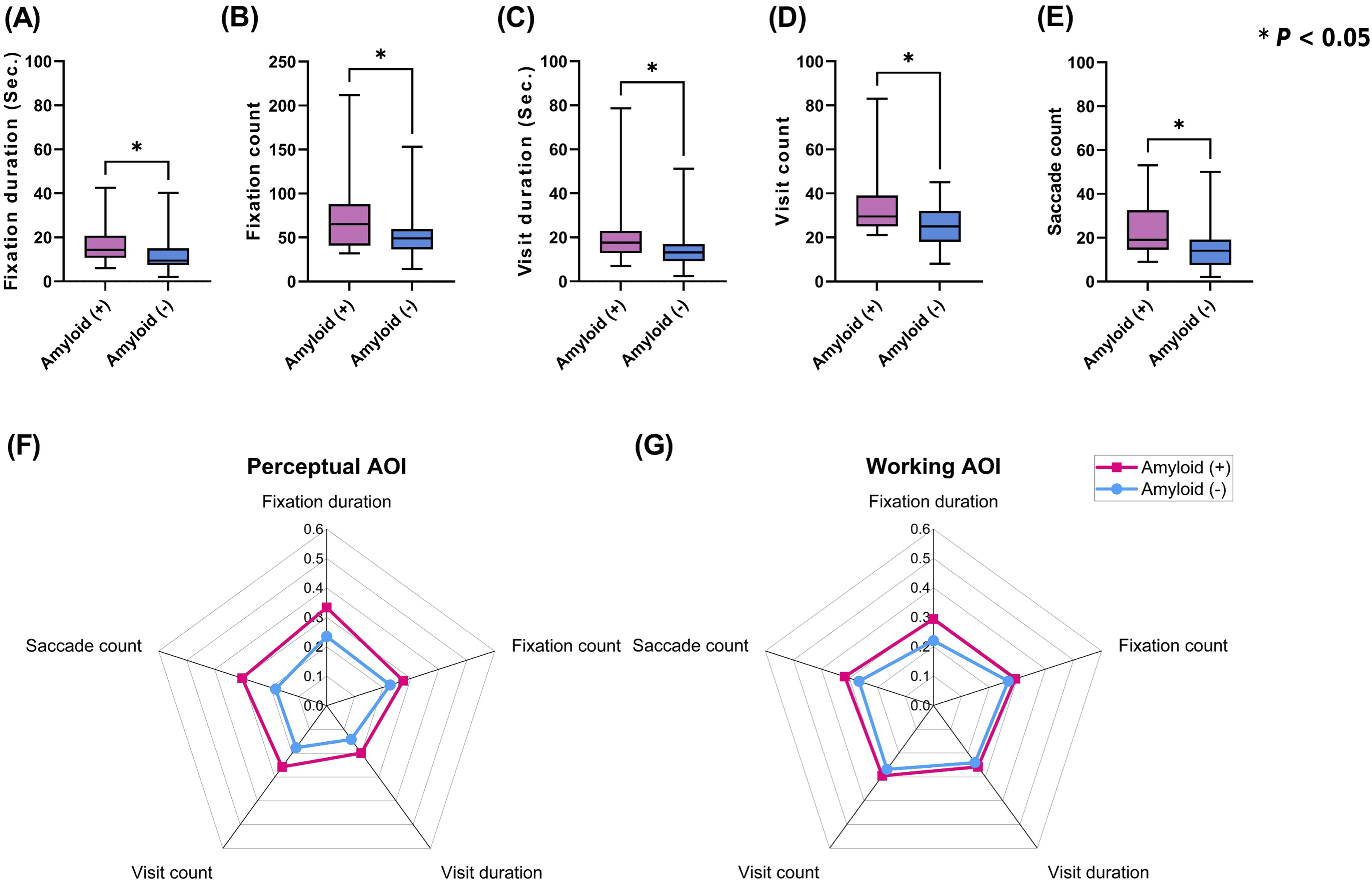
Group differences in eye-tracking metrics between Aβ-PET positive
Eye-tracking results during the sRCFT task in all participants.
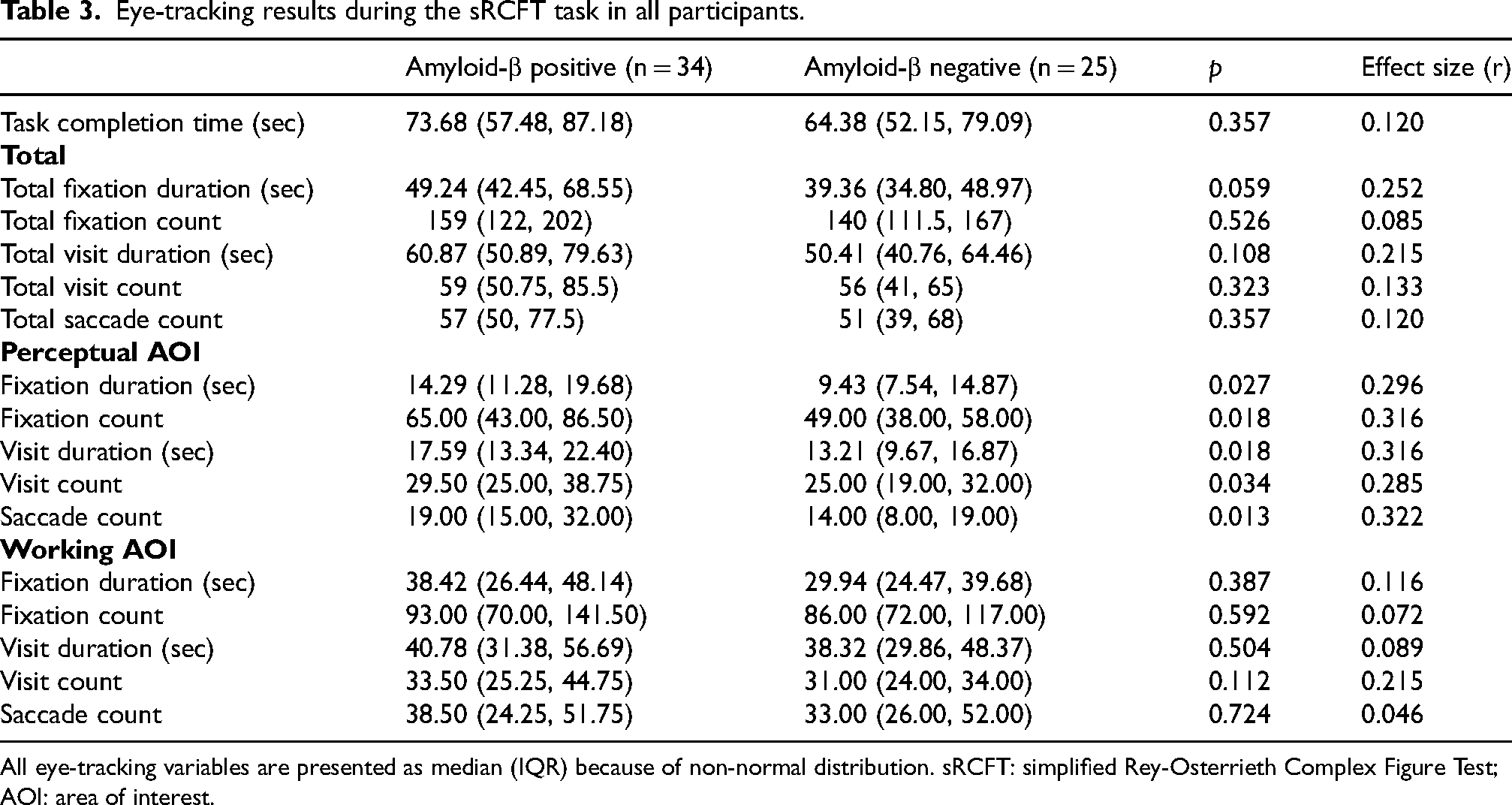
All eye-tracking variables are presented as median (IQR) because of non-normal distribution. sRCFT: simplified Rey-Osterrieth Complex Figure Test; AOI: area of interest.
A sensitivity analysis using a matched-pair design largely supported these findings. Consistent with the main analysis, Aβ-positive MCI individuals also exhibited longer fixation duration (p = 0.018, Hedges’ g = 0.678), higher fixation count (p = 0.014, Hedges’ g = 0.709), longer visit duration (p = 0.013, Hedges’ g = 0.719), increased visit count (p = 0.037, Hedges’ g = 0.586), and greater saccade count (p = 0.009, Hedges’ g = 0.657) in the perceptual AOI No significant differences were observed in any eye-tracking metrics in the working AOI (Supplemental Table 1).
Logistic regression
A logistic regression was conducted to determine whether fixation duration in the perceptual AOI predicted Aβ-PET positivity after adjusting for demographic and cognitive covariates. The model was specified as:
In the primary logistic regression model adjusting for age, sex, education, MMSE, and task completion time, longer fixation duration in the perceptual AOI was independently associated with higher odds of Aβ-PET positivity (β = 0.167; OR = 1.18, 95% CI 1.03–1.36, p = 0.021). Higher MMSE scores were inversely associated with Aβ-PET positivity (β = –0.672; OR = 0.51, p = 0.003), whereas age, sex, education, and task completion time were not significant. The model showed good calibration (Hosmer–Lemeshow χ2 = 5.84, p = 0.558) and explained approximately 50% of the variance in Aβ status (Nagelkerke R2 = 0.495). The primary logistic regression results are presented in Table 4, and Figure 3 illustrates the association between fixation duration in the perceptual AOI and Aβ-PET positivity.
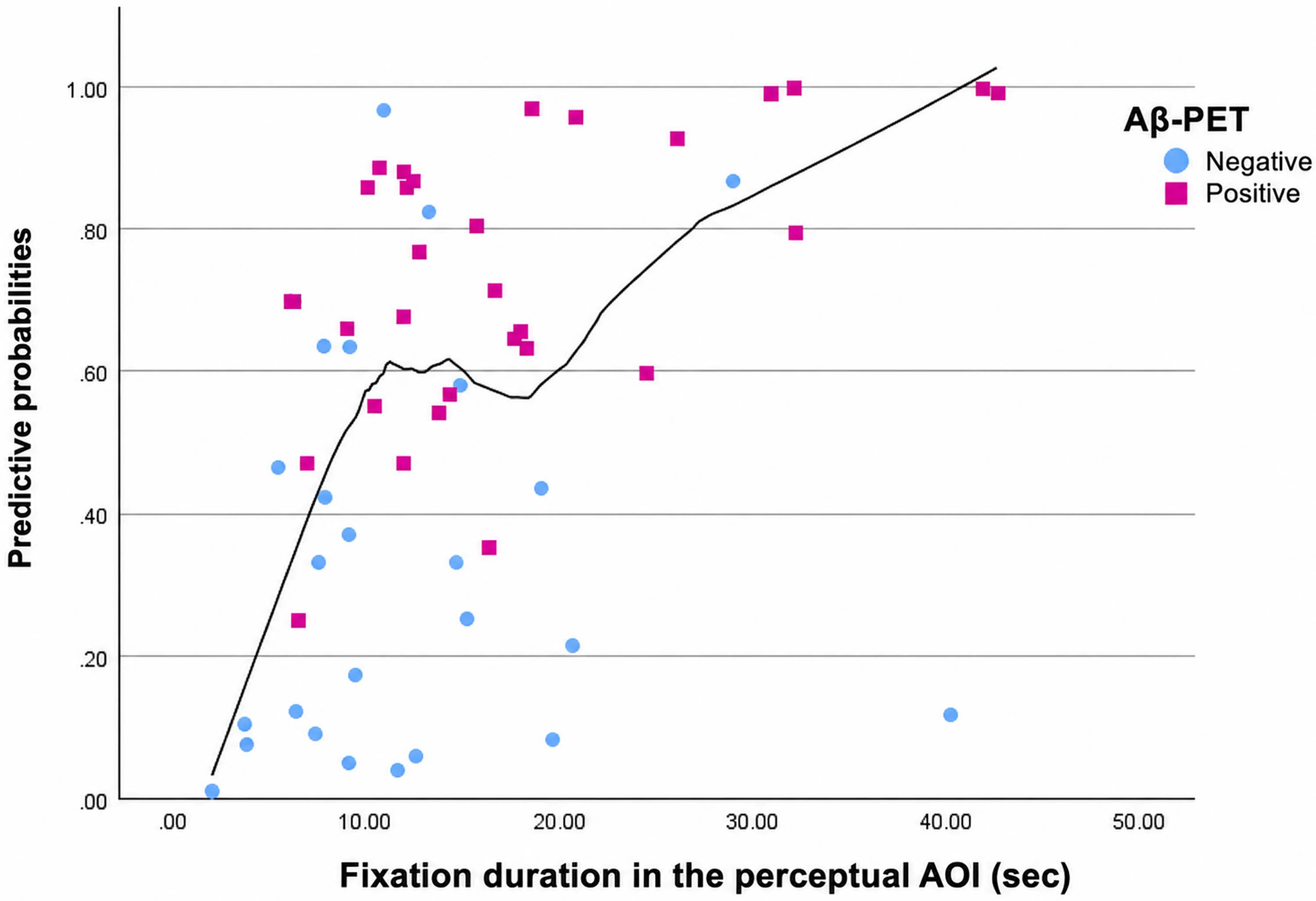
Visual relationship between fixation duration in the perceptual AOI and Aβ-PET positivity during the sRCFT copying task.
Primary logistic regression model for Aβ-PET positivity.
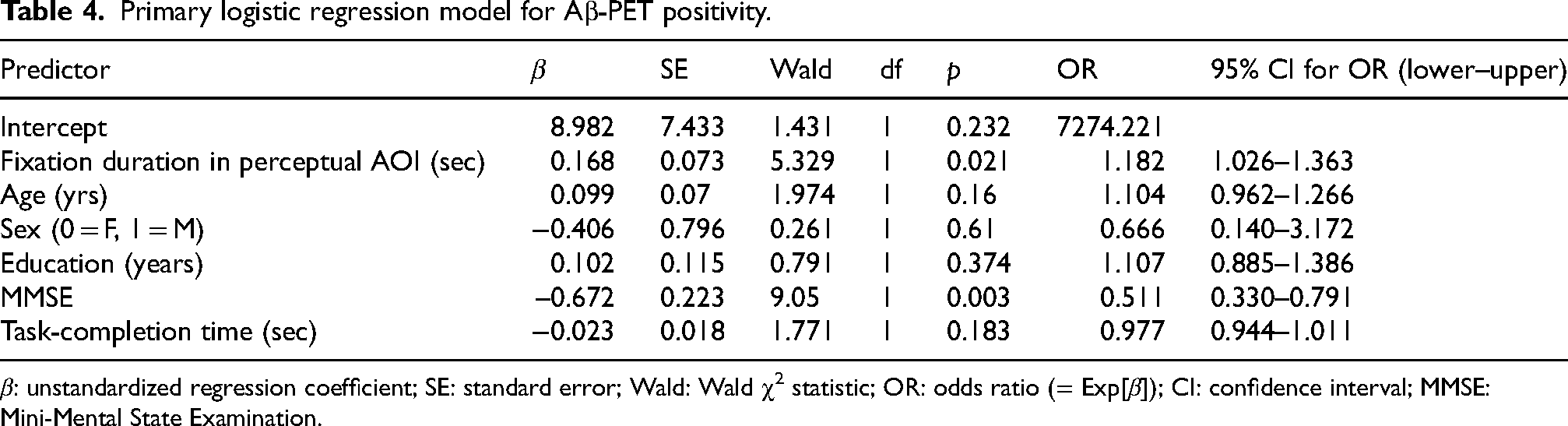
β: unstandardized regression coefficient; SE: standard error; Wald: Wald χ2 statistic; OR: odds ratio (= Exp[β]); CI: confidence interval; MMSE: Mini-Mental State Examination.
In a sensitivity model that additionally included APOE ε4 carrier status, SVLT delayed recall, and CDR sum of boxes, the association between fixation duration in the perceptual AOI and Aβ-PET positivity remained significant (OR = 1.234, 95% CI 1.039–1.467, p = 0.017). MMSE remained significant in this expanded model, whereas the additional variables were not independently significant (Supplemental Table 2).
Exploratory tertile-based subgroup analysis
For exploratory clinical interpretation, participants were additionally categorized into tertiles according to fixation duration in the perceptual AOI. The proportion of Aβ-PET positive individuals increased significantly across tertiles, from 31.6% in the low tertile to 65.0% in the middle tertile and 75.0% in the high tertile (Pearson χ2 = 8.197, p = 0.017; linear-by-linear association p = 0.007; Supplemental Table 3). In contrast, key neuropsychological measures, including MMSE, SVLT delayed recall, CDR sum of boxes, and S-IADL, did not differ significantly across tertiles.
Discussion
In this study, we compared eye-tracking metrics during the sRCFT copy task between Aβ-PET positive and Aβ-negative MCI individuals. In the perceptual AOI, Aβ-PET positive MCI individuals showed longer fixation duration—the primary endpoint—as well as longer visit durations, higher fixation and visit counts, and greater saccade counts, whereas no significant group differences were observed in the working AOI. Logistic regression analysis further demonstrated that longer fixation duration in the perceptual AOI was significantly associated with Aβ-PET positivity, independent of demographic and cognitive covariates. Exploratory tertile-based subgroup analysis further showed that longer fixation duration in the perceptual AOI was associated with a higher proportion of Aβ-PET positivity. Together, these findings suggest that Aβ-related visuospatial alterations at the MCI stage are more pronounced in perceptual processing than in visuoconstruction.
A key finding of this study is that Aβ-PET positive MCI individuals exhibited both longer fixation duration and increased fixation count in the perceptual AOI. Successful performance on the sRCFT requires repeated encoding of complex visual elements through sustained visuoperceptual processing. In this context, a prolonged fixation duration likely reflects a greater allocation of cognitive resources to perceptual encoding, whereas an increased fixation count suggests more frequent revisiting of the same regions, consistent with less efficient visual exploration. These findings are in line with our previous work in AD, in which longer fixations and higher fixation counts were similarly interpreted as reflecting increased perceptual demand and reduced processing efficiency. 17 In that study, working-AOI eye-tracking metrics did not differ significantly between individuals with late-onset AD and cognitively normal controls, whereas significant differences were observed in young-onset AD. 17 Together with the present findings, this suggests that perceptual-AOI alterations may be a more sensitive marker of early amyloid-related change at the MCI stage, whereas working-AOI abnormalities may emerge later or in specific clinical subtypes.
To minimize potential confounding effects of age, education, and global cognition, we conducted a matched-pair sensitivity analysis. Notably, the analysis largely supported the primary findings from the full sample, indicating that the observed alterations in eye-tracking metrics in the perceptual AOI are unlikely to be artifacts of sample heterogeneity. The matched-pair sensitivity analysis further suggested that the group differences in eye-tracking measures were not solely explained by differences in age, education, or global cognitive status.
An important consideration, however, is that despite matching for age, education, and MMSE, the Aβ-positive group demonstrated lower scores for RCFT immediate and delayed recall. This raises the possibility that residual confounding by visuospatial memory cannot be completely ruled out. Impaired visuospatial memory performance may increase fixation demands in the perceptual AOI. Conversely, inefficient perceptual encoding may itself lead to downstream memory deficits. These bidirectional interactions are inherently difficult to disentangle in a cross-sectional design.
Each additional second of fixation corresponded to an approximately 18% increase in the odds of Aβ-PET positivity (OR = 1.18). Importantly, this association remained significant in a sensitivity model that additionally included APOE ε4 carrier status, SVLT delayed recall, and CDR sum of boxes. In contrast to our findings, patients with clinically diagnosed AD have been reported to exhibit shorter fixations during visual target-search paradigms,12,29 likely reflecting divergent task demands: target-search tasks emphasize selective attention to a single discrete target, whereas the copying task used in our study requires broad, sustained visuoperceptual encoding. These results suggest that individuals with Aβ pathology may allocate perceptual resources to less informative visual elements, contributing to less efficient exploration strategies. In the expanded model, MMSE remained significantly associated with Aβ-PET positivity, consistent with prior literature that links global cognition to Aβ burden. 30 The logistic model showed good calibration, and the moderate Nagelkerke R2 suggests that fixation duration in the perceptual AOI captures a meaningful, though not exhaustive, proportion of the variance in Aβ status.
Exploratory outcomes revealed longer visit durations, higher fixation and visit counts, and more saccades exclusively in the perceptual AOI. Unlike fixations, which reflect moment-to-moment visual attention, visits reflect sequences of multiple fixations and saccades within a defined area, providing a broader measure of sustained visual engagement. Increased visit and saccade metrics in Aβ-PET positive individuals may therefore reflect disorganized scanning patterns, impaired top-down attentional control, 31 or a compensatory response to reduced perceptual efficiency. These alterations align with known early dysfunction in frontoparietal and visual association cortices, which are particularly vulnerable to Aβ and tau pathology. 32 Collectively, these findings suggest that eye-tracking metrics may provide a sensitive indicator of impaired perceptual encoding associated with Aβ pathology.
The tertile-based subgroup analysis supported the clinical interpretability of the main finding. Higher tertiles of fixation duration in the perceptual AOI were associated with a greater proportion of Aβ-PET positivity, whereas conventional neuropsychological measures did not differ across tertiles. This suggests that prolonged fixation duration in the perceptual AOI may reflect subtle Aβ-related visuoperceptual changes not captured by standard cognitive measures.
Although we sought to reduce potential bias through matched-pair and covariate-adjusted analyses, several limitations remain. The matched-pair analysis was based on only 14 pairs and therefore provides supportive rather than definitive evidence. In addition, residual confounding by visuospatial memory cannot be fully excluded, as lower RCFT memory scores persisted in the Aβ-positive group despite matching for age, education, and MMSE. Aβ positivity was determined by visual assessment and multidisciplinary consensus rather than quantitative centiloid-based thresholds, which may limit external validity and comparability across studies. The 50-Hz eye-tracking system may also have been less sensitive to fast or small-amplitude saccades; however, this is unlikely to have substantially influenced the primary findings, which focused mainly on fixation duration. Furthermore, the Aβ-PET negative MCI group was not further subclassified using biomarker-based or pathology-specific assessments, and some degree of etiologic heterogeneity may therefore have remained within this group. Finally, the single-center Korean design may limit generalizability to other populations.
In summary, Aβ-positive MCI individuals exhibited longer fixation and visit durations, higher fixation and visit counts, and greater saccade counts in the perceptual AOI, reflecting early differences in visuospatial processing associated with Aβ pathology. Although these findings do not establish diagnostic utility, they suggest that perceptual-AOI eye-tracking metrics may serve as a candidate mechanistic marker for future validation and multimodal integration. Larger and longitudinal studies with more rigorous control of baseline cognitive differences are warranted to confirm and extend these observations.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261461540 - Supplemental material for Perceptual-phase eye-tracking during figure copying is associated with amyloid-β PET positivity in mild cognitive impairment
Supplemental material, sj-docx-1-alz-10.1177_13872877261461540 for Perceptual-phase eye-tracking during figure copying is associated with amyloid-β PET positivity in mild cognitive impairment by Qi Wang, Yutong Bai, Byoung-Soo Shin and Ko Woon Kim in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We express our sincere gratitude to all participants in this study.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Jeonbuk National University Hospital (CUH2020-12-058). Written informed consent was obtained from all participants prior to enrollment.
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National University Development Project at Jeonbuk National University in 2023.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study will be available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.