
Abstract
Background
Social determinants of health (SDoH) are increasingly recognized as critical drivers of health outcomes, influencing care access, treatment adherence, and disease management in people with epilepsy. However, it is unclear how clinicians integrate SDoH concepts into daily practice and what needs remain unmet in the field.
Methods
A mixed-methods survey was conducted among members of the American Epilepsy Society (AES) between December 2024 and February 2025 to assess current understanding, practices, challenges, and educational needs related to SDoH. Quantitative and qualitative data analyses were conducted on the survey results.
Results
A total of 189 responses were collected, with 80% from U.S.-based healthcare professionals. Approximately 69.5% reported addressing SDoH in their practice, most frequently focusing on healthcare access and quality, followed by social and community context. Common strategies for addressing SDoH commonly involve systematic screening, telemedicine expansion, and collaboration with social workers or community organizations. Benefits from addressing SDoH-related issues were reflected in improved medication adherence, appointment attendance, and patient engagement. However, effective implementation of SDoH in epilepsy care continues to be challenged by several key barriers, including limited institutional support, lack of standardized screening tools, time constraints, and inadequate access to social work services, mental-health services, and language support.
Conclusions
While SDoH awareness among AES members is high, significant implementation gaps persist. Respondents emphasized the need for expanded education, multidisciplinary resources, and institutional alignment. These findings underscore opportunities for AES to advance advocacy, professional development, and dissemination of best practices, supporting clinicians and institutions in promoting equitable, outcomes-driven epilepsy care across diverse populations.
Introduction
In recent years, social determinants of health (SDoH) have gained increasing recognition as critical factors that influence care delivery, treatment adherence, and health outcomes in people with epilepsy (PwE). The SDoH framework emphasizes that health is shaped by the conditions in which people are born, grow, live, work, and age, such as social, economic, political, structural, and environmental conditions that extend beyond biological factors and medical treatment. 1 In epilepsy, these determinants contribute to disparities in diagnosis, treatment, and outcomes across socioeconomic and racial/ethnic groups. 2
Emerging research has demonstrated that lower socioeconomic status, public insurance, and minority race or ethnicity are associated with greater treatment delays, reduced access to epilepsy specialists, and poorer adherence to antiseizure medications.2,3 Moreover, social and structural inequities can limit opportunities for surgical evaluation and intervention, particularly in pediatric populations, where caregiver education, income, and insurance status influence referral and utilization rates. 4 Recent cohort studies also show that patients with greater cumulative SDoH needs, such as housing instability, transportation barriers, or food insecurity, experience higher emergency department utilization and worse outcomes despite similar neurological disease burden. 5 In addition, SDoH such as stigma, social isolation, unemployment, and limited access to mental-health resources significantly intensify psychosocial burden and suicidality among PwE. 6
While these studies collectively underscore the profound role of SDoH in epilepsy care and its impact on PwE, little is known about how clinicians integrate these concepts into daily practice, what strategies are effective, and where key barriers remain. To better understand current needs and gaps in SDoH education and implementation within epilepsy care, we conducted a mixed-methods, 20-question survey among members of the American Epilepsy Society (AES) between December 2024 and February 2025. Quantitative and qualitative analyses were used to characterize the current use of SDoH in epilepsy clinical practice and to identify barriers, opportunities, and future directions for enhancing SDoH integration across clinical settings.
Demographics
A total of 189 responses were collected, with ∼80% of respondents practicing in the United States (Figure 1). International participants represented a diverse range of countries, including Australia, Canada, Chile, Colombia, Cyprus, Dominican Republic, Honduras, Italy, Japan, Mexico, Montenegro, Peru, Saudi Arabia, Switzerland, and Uruguay. Most respondents (67.7%) were physicians (eg, neurologists, neurosurgeons, neuropsychiatrists, or neuropsychologists). Other participants included advanced practice providers (5%), clinical researchers (5%), patient advocates (4%), pharmacists (3%), technologists (2%), residents or fellows (2%), nurses (2%), physician assistants (1%), and social workers (1%). Regarding years in practice, 46% of respondents had 6–20 years of experience, 20% had fewer than 5 years, and 35% had more than 20 years.
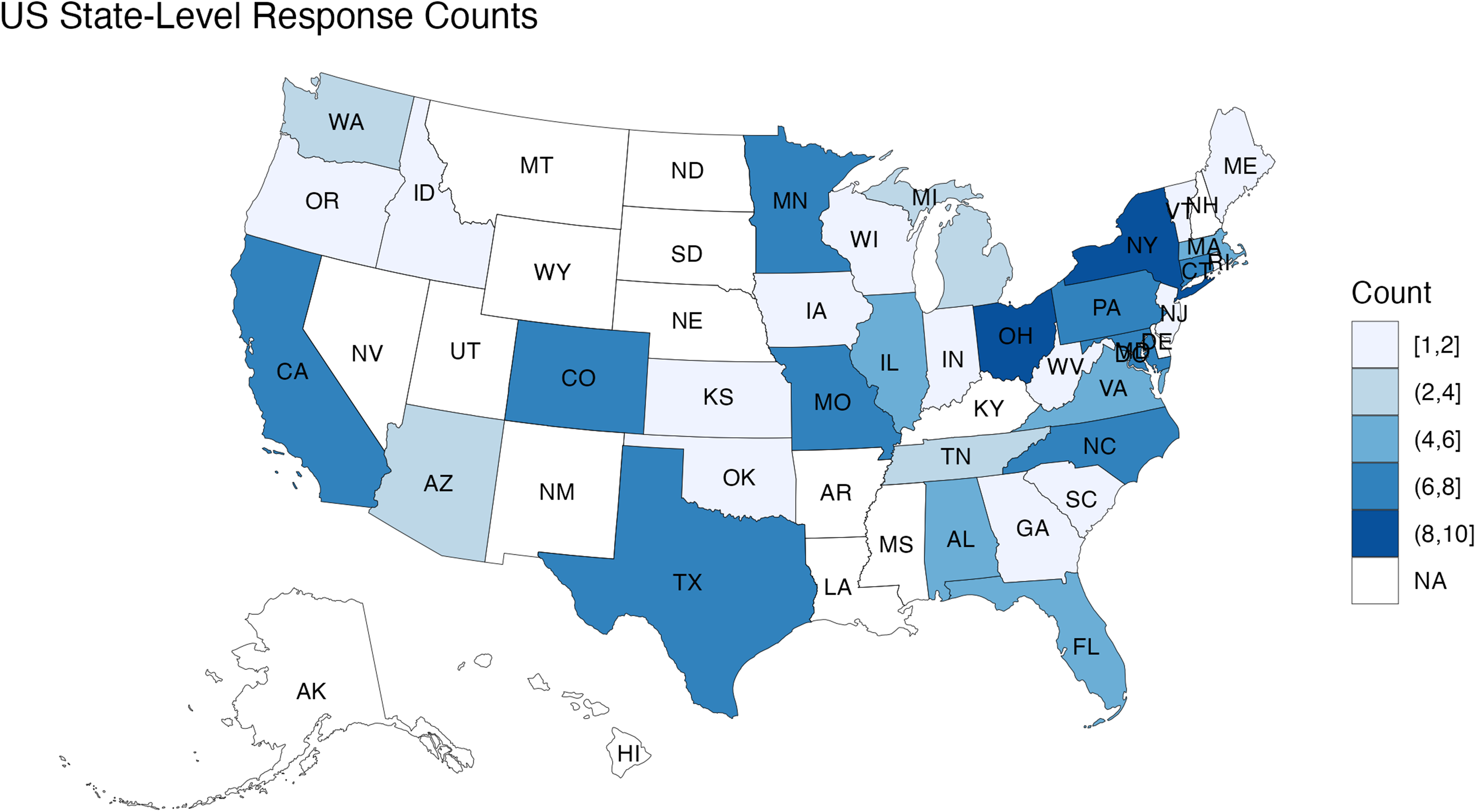
Respondents’ distribution within the United States.
Current Understanding and Integration of SDoH in Clinical Practice
About 42% of participants reported being very familiar with the concept of SDoH, while 41% were somewhat familiar. However, approximately 11.6% indicated that they were somewhat or very unfamiliar with the concept. A large majority of participants (>85%) expressed interest in learning more about SDoH. Among potential education topics, healthcare access and quality was identified as the most appealing area of interest, followed by education access and quality. Fewer participants expressed interest in topics related to economic stability, social and community context, and neighborhood and built environment.
Approximately 69.5% of respondents reported that they are currently addressing SDoH in their clinical practice. Among these, the most targeted domain was healthcare access and quality (76.5%), followed by social and community context (44.4%), education access and quality (36%), and economic stability (29.4%).
Respondents described a diverse range of strategies for addressing SDoH in epilepsy care, showing both structural and individualized approaches. A recurring theme was the incorporation of systematic screening during clinical encounters, often through standardized questionnaires or intake assessments to identify patients’ unmet social needs. Additionally, many respondents emphasized interdisciplinary collaboration with social workers and community organizations, highlighting coordinated referrals to social services, mental-health resources, or transportation support. Several respondents highlighted efforts to expand telemedicine and virtual visits, improving access for patients facing geographic or financial barriers. Beyond this, those working in rural or resource-limited settings also mentioned providing transportation assistance and financial counseling to enhance accessibility. Moreover, respondents also described educational initiatives aimed at improving health literacy and encouraging patient self-management, sometimes integrated into broader research or quality-improvement projects. Alongside this, a few respondents noted research- or foundation-supported programs that piloted innovative care models or evaluated the outcomes of SDoH-focused interventions. Collectively, these responses suggest that clinicians are addressing SDoH through a combination of screening, interprofessional collaboration, community engagement, and innovative care delivery, although implementation remains variable across clinical and geographic settings.
Among respondents who reported addressing SDoH in their clinical practice, fewer than one-third indicated that they systematically track patient outcomes related to these interventions. Nevertheless, more than 50% of them perceived the impact of their efforts as positive. Participants described a variety of examples illustrating how addressing SDoH contributed to meaningful improvements in patient care. Common outcomes included improved access to healthcare, such as financial supports from successful coordination of Medicaid coverage, transportation assistance, and timely follow-up visits. Respondents also reported improved continuity of care and treatment adherence, often facilitated through collaboration with social workers, community organizations, and patient advocacy foundations. In addition, several described improvements in psychosocial well-being and reduced patient stress following assistance for food insecurity, housing, or financial challenges. Moreover, respondents emphasized the role of multidisciplinary case discussions and integration of SDoH in care planning, which fostered a more holistic and coordinated approach among the care delivery team. Lastly, a few participants highlighted strengthened communication and trust between providers and families, particularly within pediatric and underserved populations. Together, these responses highlight that integrating SDoH into routine clinical workflows can foster multidisciplinary collaboration, improve patient access and adherence to care, strengthen trust between patients and providers, and help alleviate psychosocial stressors for PwE and their caregivers.
Gaps and Needs
Respondents identified multiple, intersecting challenges in addressing SDoH within epilepsy care. The most frequently cited barriers included limited resources, time constraints, and institutional or insurance-related obstacles that restrict comprehensive screening and follow-up. Many participants described how economic instability, transportation difficulties, and lack of insurance coverage limit patients’ access to necessary appointments and medications, particularly in rural or underserved communities. Respondents also highlighted some language-related barriers, such as shortages of bilingual providers and epilepsy-specific education in different languages. Additionally, some clinicians noted that low health literacy and occasional patient or caregiver resistance make it difficult to engage in meaningful discussions about social needs. Together, these findings reveal how structural, socioeconomic, and resource barriers converge to hinder the integration of SDoH into routine clinical workflows. Addressing these challenges will require institutional support, resource allocation, workforce development, and targeted education to help clinicians effectively translate awareness of SDoH into sustainable, patient-centered care.
In particular, respondents emphasized the importance of greater institutional support to address these gaps. Many advocated for the inclusion of social workers, psychologists, and community health workers to assist patients with nonmedical challenges. Others pointed to limited appointment time as a barrier to meaningful conversations about social needs. Moreover, participants called for increased training for clinicians and staff on how to identify and address SDoH within routine practice and stressed the value of clear referral pathways and stronger community partnerships. Overall, the responses reflect systemic constraints that require investment in multidisciplinary teams and sustained institutional backing, particularly in staffing, time, care coordination, and infrastructure.
There was also broad enthusiasm for further education and professional development on SDoH topics. Participants were especially interested in practical, skills-based training, including how to screen for social needs sensitively, implement feasible interventions, and connect patients to available resources. Topics such as implicit bias, cultural competency, and best practices for integrating SDoH into neurological care were frequently requested. Respondents favored case-based and actionable learning opportunities that move beyond theory to strengthen real-world application in epilepsy care.
Finally, many respondents expressed appreciation and support for this survey and its focus on SDoH. They viewed it as a timely and necessary effort to advance awareness and equity in epilepsy care. Some emphasized the need for continued education, standardized workflows, and institutional programs to make SDoH screening a routine part of practice. Others called for ongoing evaluation of equity and access across patient populations. Overall, the comments conveyed strong engagement and endorsement, alongside recognition that meaningful progress will depend on sustained education, organizational support, and policy-level alignment.
Discussion
Findings from our survey highlight both progress and persistent gaps in integrating SDoH into epilepsy care. Most respondents recognized the relevance of SDoH in clinical practice and reported incorporating at least some screening or counseling into patient encounters. However, barriers such as limited time, resources, and institutional support remain common, echoing prior reports of structural and operational challenges in implementing equitable care models.5,7 Our survey provides insights into clinician awareness and engagement with SDoH within the AES community. While many respondents expressed strong interest in expanding SDoH-related education and practice, fewer reported the existence of structured institutional initiatives or standardized workflows for screening and referral.
Although many respondents shared positive experiences and outcomes from integrating SDoH into their clinical practice, fewer than one-third reported systematically tracking outcomes from these efforts. This gap highlights an important opportunity for AES and its members to develop standardized approaches and guidelines for SDoH-related outcome measurement. With standardized outcome metrics and longitudinal follow-up, systematic outcome tracking can help identify persistent service gaps, support continuous quality improvement, and generate population-level or community-level insights about SDoH-related issues among PwE. In the long term, such data can also support policy advocacy efforts and provide necessary evidence to secure sustained institutional support for SDoH-related initiatives in epilepsy care.
One of the key limitations of this survey itself is the lack of data on participants’ race and ethnicity, as well as demographic information about the patient populations they serve or the geographic distribution of their clinical sites (eg, rural, suburban, or urban settings). This gap limits our ability to evaluate how racial, ethnic, and geographic factors influence current practices in epilepsy care delivery. Although some respondents mentioned challenges related to language barriers, such as limited educational materials and staffing to support non-English-speaking PwE, there were no specific responses addressing race or ethnicity. It also remains unclear in this survey how other demographic variables, including patient age, may influence care delivery in practice. In addition, the survey received relatively few responses from social workers and nurse practitioners, despite their central role in addressing SDoH in current practice. Finally, the perspectives of PwE themselves were not captured, as it was out of the scope of this survey. Overall, these limitations warrant the need for more in-depth focus group discussions within the society to better understand current practices and challenges related to these aspects of SDoH.
Building on the AES/International League Against Epilepsy (ILAE)-North America Task Force recommendations, 8 our findings reinforce several actionable priorities. AES could (1) develop standardized SDoH screening tools and promote use of ICD-10 Z-codes to systematically track social and economic barriers in clinical settings; (2) expand educational offerings that focused on health equity and culturally competent care, such as resource guides, webinars, workshop, case studies, and conference symposiums; (3) encourage inclusion of historically marginalized populations in research and quality-improvement efforts; and (4) support the development of interdisciplinary care models that integrate mental health, community health workers, and social services.
Collectively, these strategies would advance the AES's ongoing commitment to equitable epilepsy care. By promoting education, advocacy, and the dissemination of best practices, AES can help bridge the gap between awareness and action, supporting clinicians and institutions in integrating SDoH assessment and interventions into everyday practice and advancing a more equitable, outcomes-driven approach to epilepsy care across diverse populations.
Footnotes
Acknowledgements
We sincerely appreciate the outstanding support and coordination provided by our AES staff members Paige Romanello and Adam Eickmeyer.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.