
Abstract
The ideal treatment of calf vein thrombosis (CVT) remains undefined. We assessed practice patterns at a single institution for CVT. Physicians were sent an online survey with 8 multiple choice questions about management of CVT. A total of 99 physicians of varying specialties participated in the survey. A total of 48.5% anticoagulate patients with CVT and 51.5% do not. Of those who anticoagulate, 62.3% use low molecular weight heparin and 11% use IV heparin. Treatment duration is 3 months for 58% and 6 months for 30% of responders. Of those who do not anticoagulate, 71.2% reassess for clot propagation or resolution with a duplex exam. IVC filters are used by 46% when there is a contraindication to anticoagulation and 13.7% when clot propagation is noted on follow-up scan. These results suggest that there is no consensus treatment of CVT. There is a higher than expected rate of IVC filters placed for CVT.
Introduction
The ideal treatment for patients with calf vein thrombosis (CVT) remains undefined. The below-knee, or deep calf veins refer to the gastrocnemius, soleal, anterior tibial, posterior tibial and peroneal veins. 1 CVT is a separate entity from other deep vein thromboses (DVT) and must be studied independently. CVT poses a potential risk for propagation to an above-knee vessel as well as a risk of post-thrombotic syndrome. 2 However, multiple studies have differing conclusions on whether anticoagulation affects morbidity and mortality for CVT.3–8 The American College of Chest Physicians (ACCP) evidence-based guidelines for antithrombotic therapy provides recommendations for treatment of CVT. 9 Yet, practice patterns still widely vary. Treatment recommendations range from conservative management with compression stockings to full-dose anticoagulation.
At our institution, we noticed a variety of different practice patterns regarding treatment of CVT. In addition, we noticed the occasional use of inferior vena cava (IVC) filters for the treatment of CVT and questioned their use for this disease process. The purpose of this study was to examine practice patterns at our institution. These data would be useful to realize inconsistencies and attempt to change individual provider practices by encouraging evidence-based management strategies. We hypothesized that there would be no clear consensus among physicians across the institution as a whole or across each specialty.
Methods
Survey questions
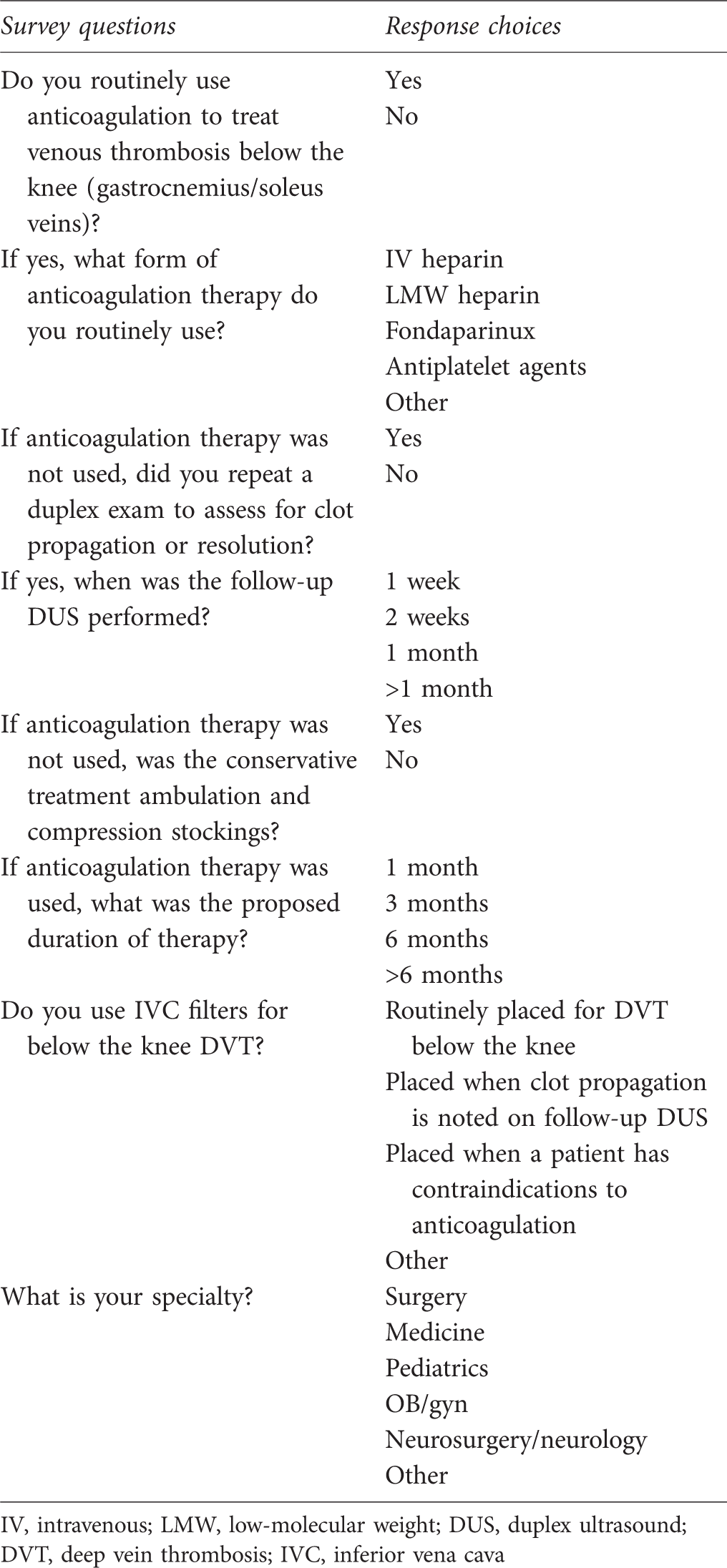
IV, intravenous; LMW, low-molecular weight; DUS, duplex ultrasound; DVT, deep vein thrombosis; IVC, inferior vena cava
Results
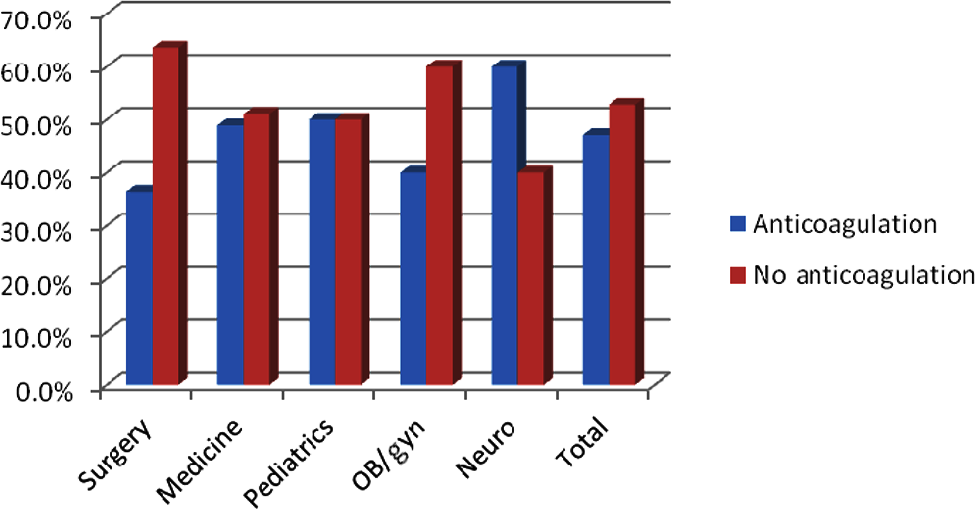
The survey was sent to all faculty physicians at our institution. A total of 99 physicians (approximately 20%) responded to the survey. Of these participants, 45.5% specialized in medicine, 11.1% surgery, 5.1% neurosurgery and 5.1% obstetrics/gynecology. Forty-eight responders (48.5%) stated that they anticoagulate patients with DVT below the knee and 51 (51.5%) stated they do not anticoagulate (Figure 1). Neurologists and neurosurgeons were most likely to anticoagulate (60%) while general surgeons were the least likely to anticoagulate (36%) (Figure 2).
Routine use of anticoagulation to treat calf vein thrombosis Routine use of anticoagulation to treat calf vein thrombosis (by specialty)
Of the 48 physicians who anticoagulate, 62.3% use low-molecular weight (LMW) heparin. Intravenous (unfractionated) heparin is used by 11% and antiplatelet agents are used by 7.5%. All of responding neurologists and neurosurgeons use intravenous heparin while all other specialties preferred LMW heparin (Figure 3).
Type of anticoagulation used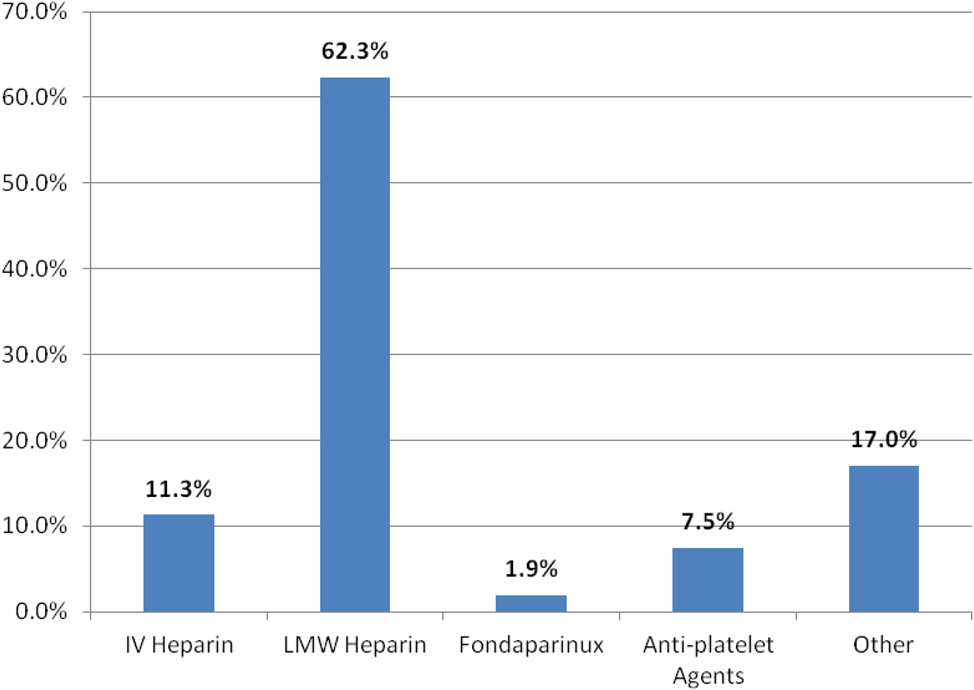
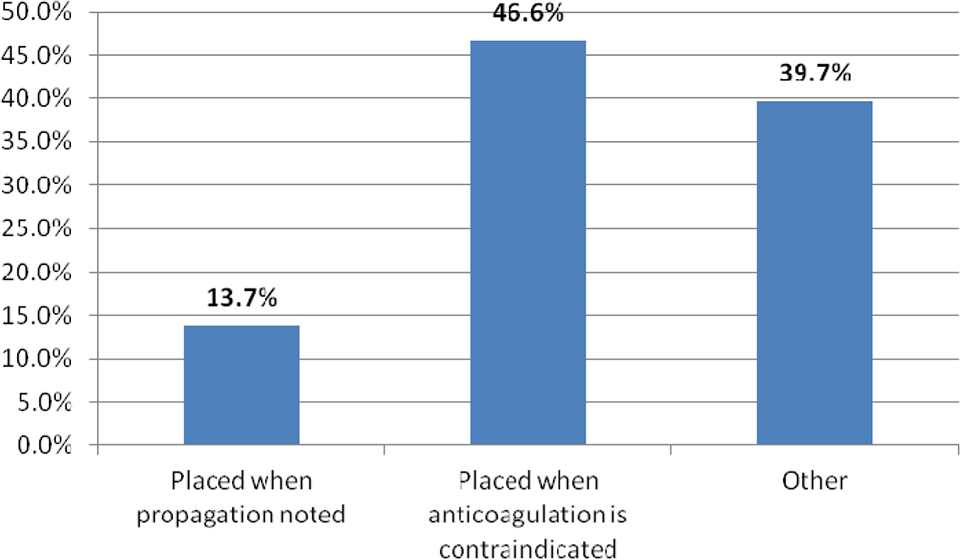
Of the 51 physicians who do not anticoagulate patients with DVT below the knee, nearly all (88.7%) use ambulation and compression stockings as treatment. A total of 71.2% reassess for clot propagation or resolution with a duplex exam. Forty-eight percent routinely obtain follow-up duplex scans at one week, 37% at two weeks and 11.1% at one month postinitial duplex scan. The usual length of anticoagulation is three months for 58% and six months for 30% of the 48 participants who anticoagulate patients (Figure 4). IVC filters are used by 46% when there is a contraindication to anticoagulation and used by 13.7% when clot propagation is noted on follow-up duplex scan (Figure 5).
Duration of anticoagulation therapy Use of inferior vena cava filter to treat calf vein thrombosis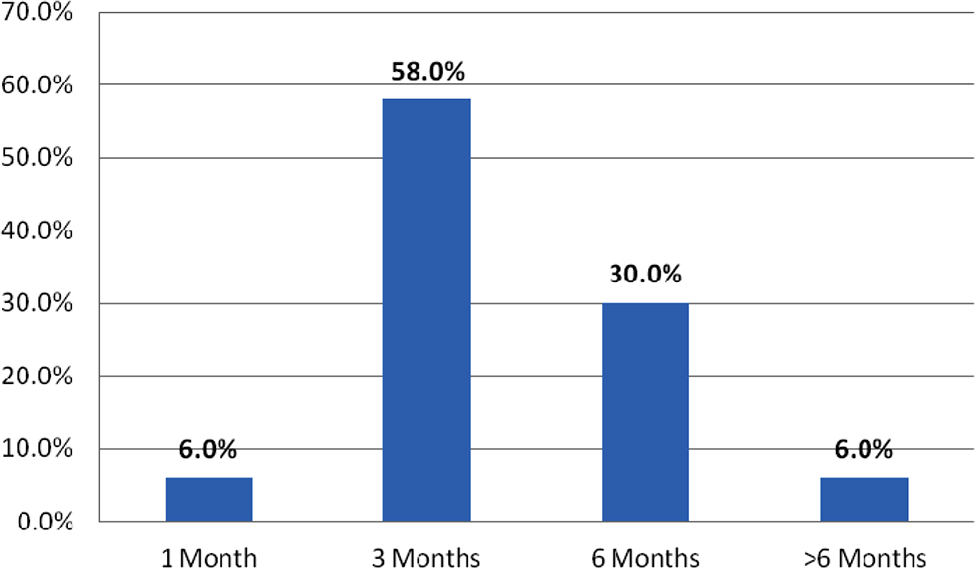
Discussion
Whether anticoagulation is necessary for CVT remains to be answered. Most studies of this topic classify the thrombus into isolated gastrocnemius and soleal vein thrombosis (IGSVT), tibial/peroneal vein thrombosis or just CVT. The difference in classification leads to further discrepancy in treatment recommendations. Risks associated with CVT include propagation and post-thrombotic syndrome, but these risks appear to be low.
The risk of propagation from a below-knee vessel to an above-knee vessel is commonly stated to be around 20%, 10 though the range reported is 3–32%.6,11 The re-thrombosis rate of all DVT after anticoagulation was found to be 24% compared with 6% for CVT after 12 years. 12 There are a group of studies suggesting minimal risk of propagation above the knee and no pulmonary embolic events.7,8,11 MacDonald, et al. in a prospective, non-randomized trial found a rate of 3% propagation of gastrocnemius and soleal thromboses. They found cancer to be the only risk factor associated with extension of the thrombus in the calf, but it was not associated with propagation beyond the calf veins. If the thrombus propagates, this will usually occur within the first two weeks, while half of these thrombi regress by three months. Gastrocnemius and soleal vein thrombosis tend to be more benign than tibial or peroneal vein thrombosis. 11 In a randomized controlled trial of 107 patients treated with either graduated compression stockings or LMW heparin for 10 days plus graduated compression stockings, progression occurred in 3.8 and 3.7% of patients in each group (P = 0.99). Thrombus recanalization was similar in both groups as well. This study's authors recommended against anticoagulation for isolated CVT without ongoing risk factors. 13 Moreover, a recent retrospective study demonstrated no difference in progression of thrombus with or without full anticoagulation. 14
Conversely, other studies contend that CVT can be associated with a high rate of propagation and serious complications.5,6,15,16 Lohr, et al. 6 quote a 32% risk of clot progression and a 5% incidence of pulmonary emboli in a prospective study. Lautz, et al. 16 in a retrospective study, found a 29% incidence of progression without therapeutic anticoagulation compared with 12% incidence with therapeutic anticoagulation.
Post-thrombotic syndrome occurs after thrombosis damages the venous valves, leading to reflux and venous hypertension. This can manifest as skin changes, pain, edema or recurrent ulcerations.17,18 Anticoagulation after DVT is thought to decrease the rate of post-thrombotic syndrome. 18 The incidence of this syndrome with proximal DVT is approximately 30% after five years. 19 Franzeck, et al. 12 report patients with calf DVT had only a 15% incidence of post-thrombotic changes and all were minor skin changes, while Meissner, et al. 3 report a 24% incidence of reflux at one month.
The high percentage of IVC filter placement is concerning given the potential morbidity associated with the device, compared with a relatively low morbidity associated with CVT. Complications of vena cava filter placement include injury to the access vessel, misplacement, filter migration, caval occlusion and increased DVT rates. 20
The eighth edition of the ACCP guidelines on antithrombotic therapy give recommendations for unprovoked CVT but do not discuss provoked CVT. 21 The just recently released ninth edition has a slightly more detailed discussion with new treatment recommendations. They state that the decision for anticoagulation should be based on the severity of symptoms and risk factors for extension (positive D-dimer, extensive thrombosis, close to proximal veins, no reversible provoking factor, active cancer, history of venous thromboembolic or inpatient status). If no anticoagulation is administered, serial ultrasound over two weeks is recommended. Yet, these recommendations are still based on poor quality data. 9
Conclusions
The results of this survey illustrate that equal numbers of physicians at our institution anticoagulate patients with CVT as compared with conservative management. There is no concordance in clinical practice at a single academic medical center, even within a specific specialty. When anticoagulation is chosen, there is substantial variability in the types of medications used. In addition, there is a higher than expected rate of IVC filters placed for CVT. These inconsistencies may represent either a lack of consensus or a lack of awareness of evidence-based guidelines. However, the evidence-based guidelines are not based on great data and many physicians who are aware of these still choose to practice differently.
This study addresses the inconsistency of treatment of CVT. There are many limitations to this survey-based study. First, there is a poor response rate of about 20%. Some of the non-responders are those who do not encounter this clinical decision, such as anesthesiology, pathology and radiology. However, this does not account for all of the non-responders, and therefore may not give an accurate representation of the entire institution. Second, our survey did not fully explain the term below-knee DVT and did not differentiate between gastrocnemius/soleal and named CVT. This could potentially skew the data as general practice patterns may differ between these two entities. Some current literature considers them separately, while other studies refer to them together.
Finally, the questions were very generalized rather than tailored to specific situations. Thus, our results discuss what physicians consider the general norm, but may not be what they do in all situations. For example, a patient who is chronically immobile with a malignancy or clotting disorder should be considered differently than an otherwise healthy patient with isolated CVT. Additionally, reasons for placing IVC filters were not clearly elucidated (i.e. contraindication to anticoagulation and propagation versus contraindication alone).
Importantly, our study is simply observational and is not meant to add new treatment evidence to the current literature. Rather, its purpose is to show that despite recommendations by the ACCP, the literature is widely varied and practice patterns are varied and inconsistent. This study was used as a launchboard for two other studies which are in process. One is a survey that has been expanded to vascular surgeons at multiple institutions throughout the country. Another is examining actual treatment practices of patients diagnosed with CVT in our institution's vascular lab, which may be more telling as it will not be subject to the biases of a survey. Yet, a multicenter, prospective randomized trial is still necessary to create better evidence-based treatment recommendations for anticoagulation of CVT.