
Abstract
Objectives
The optimal treatment of superficial vein thrombosis (SVT) of the leg has not been determined yet. The aim of this study is to evaluate the efficacy of low-molecular-weight heparin (LMWH) as compared with combined therapy of LMWH with an anti-inflammatory agent in treatment of SVT.
Methods
Fifty patients with SVT of the greater saphenous vein were randomly assigned to be treated with Ca-nadroparin 190 IUAxa/kg in a single dose or with same dose of Ca-nadroparin and 60 mg oral acemetacine twice daily for 10 days. The efficacy of the two treatments to relieve symptoms and signs was evaluated by using visual analogue scale.
Results
Significant improvements were achieved for both groups after the treatment in terms of all four symptoms (P < 0.001). Treatment scores were in favour of LMWH with anti-inflammatory agent treatment group to relieve all four symptoms. The most significant and remarkable results obtained were for the reduction of pain and local tenderness (P < 0.05). No patient experienced major complications or mortality in either group.
Conclusion
The results of this study suggest that the combined therapy of LMWH with an anti-inflammatory agent is more effective than LMWH. It may be an important option in the standard treatment of SVT.
Introduction
Superficial vein thrombosis (SVT) of lower extremities is one of the most commonly seen vascular diseases. Although the aetiology of SVT is usually not known, it may present itself as a result of the most important complication of varicose veins. It will be appropriate to look for an underlying systemic disease in patients of SVT without varicose veins. These systemic diseases may be collagen tissue disease, myeloproliferative disease, malignancy and hypercoagulability. It may occur as a result of an extremity trauma or after various intravenous treatments. Moreover, idiopathic SVT may be seen apart from all those causes as well. 1–3
Whereas SVT of lower extremity is recognized clinically as a benign disease, the thrombosis may extend towards deep venous system and may cause a pulmonary embolism. 4 Deep vein thrombosis (DVT) is seen in 3–40% of patients with SVT and pulmonary embolism in 2–13%. 5 The purpose of treatment in SVT is both to prevent thromboembolic complications and extension of thrombosis into the deep venous system, and relieve the symptoms that patient complaints of. Patients mostly complained of pain and tenderness. 1 Optimal treatment regarding this disease was not determined yet. There exist various treatment options involving medical or surgical approaches. If SVT has a history longer than one week, medical therapy is considered to be more effective than surgical therapy. 6 Antithrombotic agents that are known to be more effective than vein ligation for preventing DVT and pulmonary embolism may be better choices of SVT treatment.
Recently, low-molecular-weight heparin (LMWH) is very popular and may be acknowledged as the reference curative therapy of venous thrombosis. 5,6 Moreover, non-steroidal anti-inflammatory (NSAI) agents have been widely applied as well. It is known that only NSAI drugs may be used orally or topically in the treatment of SVT. 1,5
The present study is designed to investigate the efficacy and reliability of using together of those two effective therapies. In order to relieve the symptoms of SVT, does the combined usage of LMWH and NSAI can be more effective than single usage of LMWH? Our aim is to find the answer for this question.
Materials and methods
Fifty patients with acute SVT of the greater saphenous vein were included in this study. The patients who had SVT on both of two lower limbs were excluded. The diagnoses achieved by physical examination were confirmed with colour Doppler and duplex ultrasonography. Acute SVT of the greater saphenous vein at least 5 cm in length on duplex ultrasonography were considered for inclusion in this study. The patients, with a thrombus 5 cm closer to saphenofemoral junction, having any kind of DVT pulmonary embolism, using anticoagulants for any reason, pregnant women and patients with gastric problems were excluded from the study.
The patients were randomly assigned into two groups by consecutive alternating method. First group consisted of 25 patients, 12 women and 13 men, with a mean age of 48.6 (range 25–90). The second group again included 25 patients, 14 men and 11 women, and the mean age was 44.9 (range 28–85). The patients included in both of the groups were of comparable characteristics with regard to age, gender, weight and personal histories (Table 1).
Patients' characteristics

There was no oedema or diameter increase in the extremity showing symptoms of the disease. Pain, hyperaemia, local tenderness and palpable indurated cord were scored in all the patients. Visual analogue scale (VAS) was applied in clinical evaluation. The four significant symptoms, spontaneous pain, erythema, local tenderness and palpable cord, were assessed with points between 1 and 10 before and after the therapy. The VAS is one of the standard measuring instruments used for rating of pain. The VAS for pain is a straight horizontal line, 10 cm in length, with the left end of the line representing no pain (0) and the right end of the line representing the most pain (10). 6,7 The patients are asked to mark the number on the line that they think their current state of pain is. The VAS method could also be used to measure a variety of different subjective clinical phenomena. 8,9 In this study, the VAS has been used to rate the other symptoms and signs of SVT, such as tenderness, hyperaemia and palpable indurated cord. The patient's doctor points to the number on the scale according to the severity of symptoms and signs. For example, the severity of tenderness in the patient could be determined by the doctor, which ranges from none (0) to severe tenderness with withdrawal by gentle percussion to the cord (10). Tenderness to palpation with or without grimace and/or flinch may effect the number chosen. Complete blood count, activated partial thromboplastin time (aPTT), prothrombin time and routine blood tests were applied before the therapy.
Ca-nadroparin was applied to the patients in first group subcutaneously as 190 IUAxa/kg in a single dose. The patients in second group were given Ca-nadroparin at the same dose with the addition of 60 mg oral acemetacine twice daily. Nadroparin is available as a solution containing 19.000 AXa IU/mL for once daily regimen in the treatment of venous thrombosis. This formulation of nadroparin (0.01 mL/kg) once daily was used as the complete anticoagulation dose in both groups. Treatment duration was 10 days for both of the groups. Pantoprasol with a dose of 40 mg daily was included at the beginning of the treatment in order to protect stomach. The clinical scores of those four symptoms were assessed with VAS at the end of the treatment for both of the two groups.
Results
Before and after treatment scores in each group were evaluated by Wilcoxon signed-rank test (Table 2). Statistically significant improvements were achieved for both groups after the treatment in terms of all four symptoms (P < 0.001). The treatment methods applied for both group I and group II were shown to be considerably effective.
Statistical results of treatment groups
P* < 0.05 (Wilcoxon signed-rank test)
P** < 0.05 (Mann-Whitney U-test)
Statistical analysis
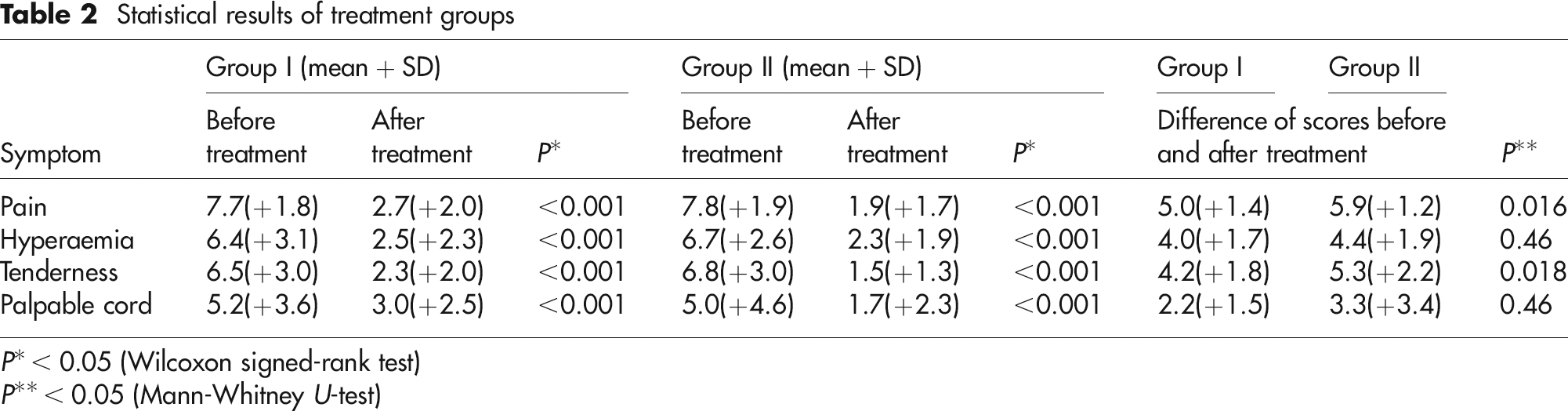
Different treatment modalities applied in two groups were compared with Mann-Whitney U-test (Table 2). Cure scores realized by VAS were in favour of group II with regard to all four symptoms. The results are shown in Figures 1–4. The most remarkable results obtained were for the reduction of pain and tenderness and those results were statistically significant (P < 0.05).
The mean pain visual analogue scale (VAS) scores of both groups

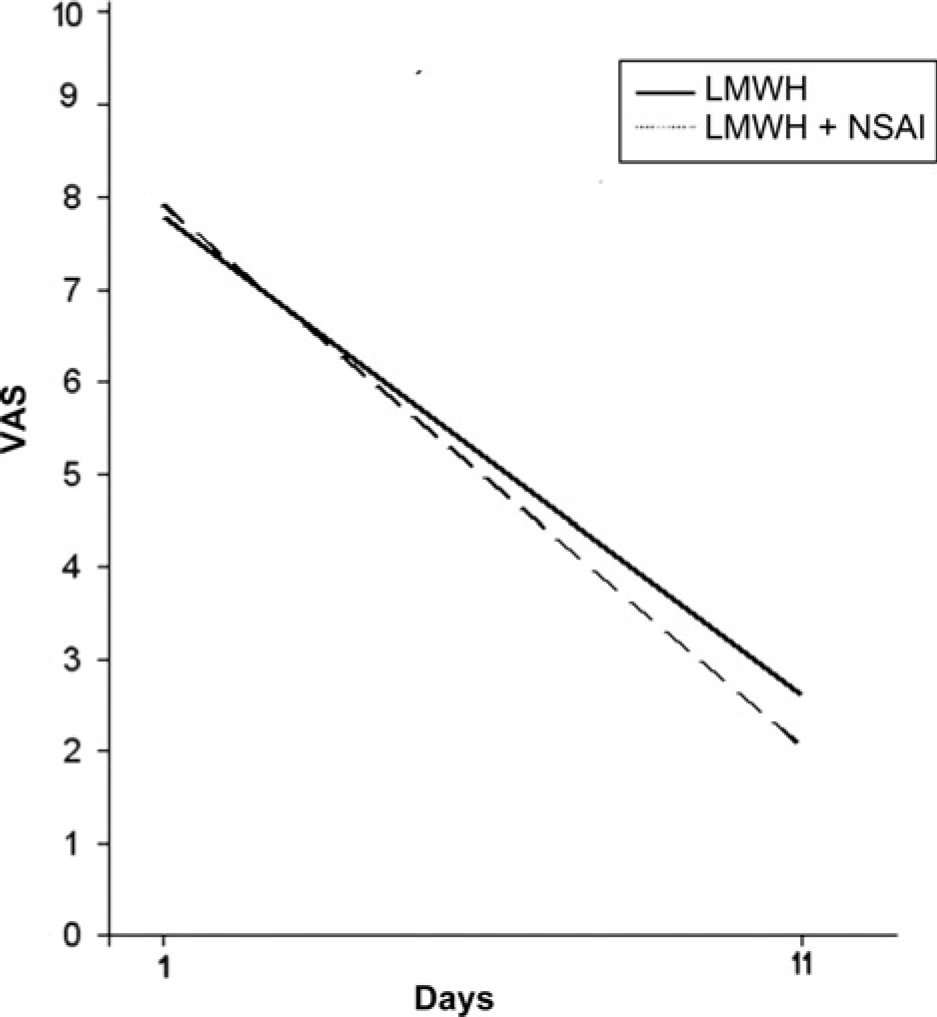
The mean hyperaemia visual analogue scale (VAS) scores of both groups
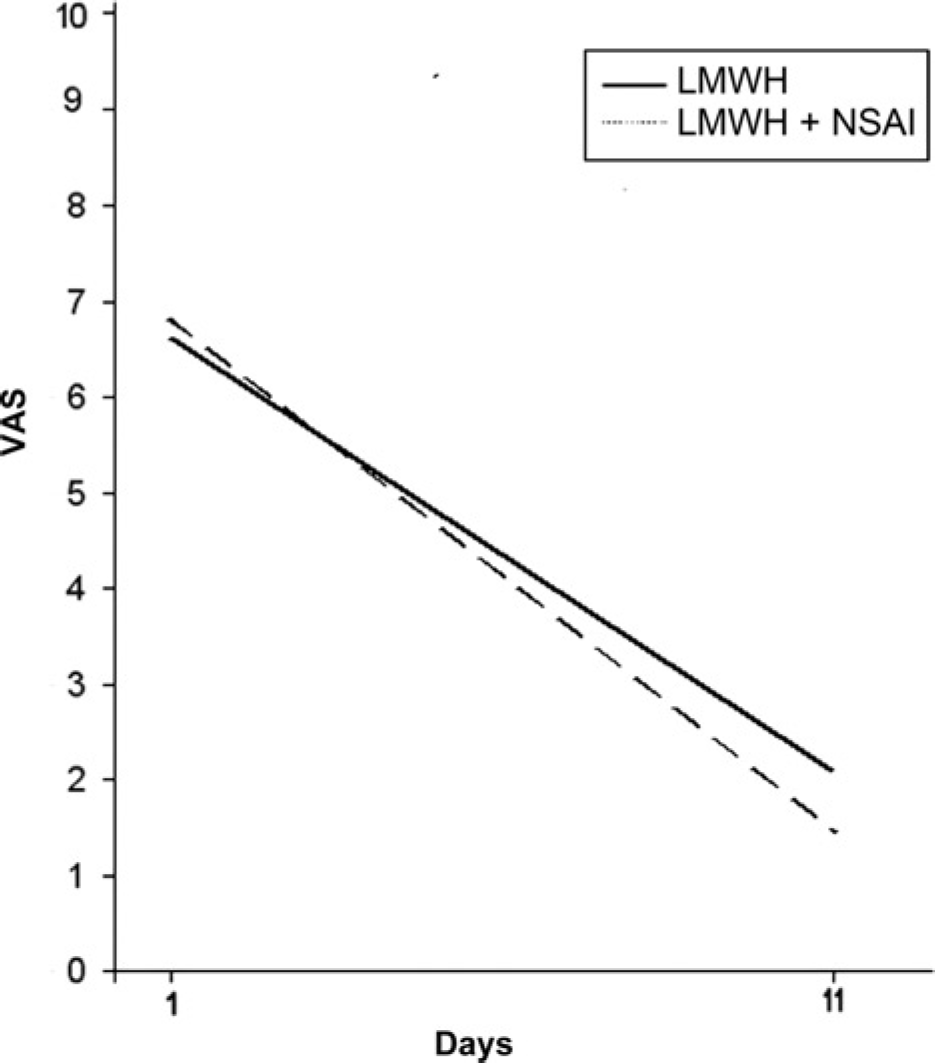
The mean tenderness visual analogue scale (VAS) scores of both groups
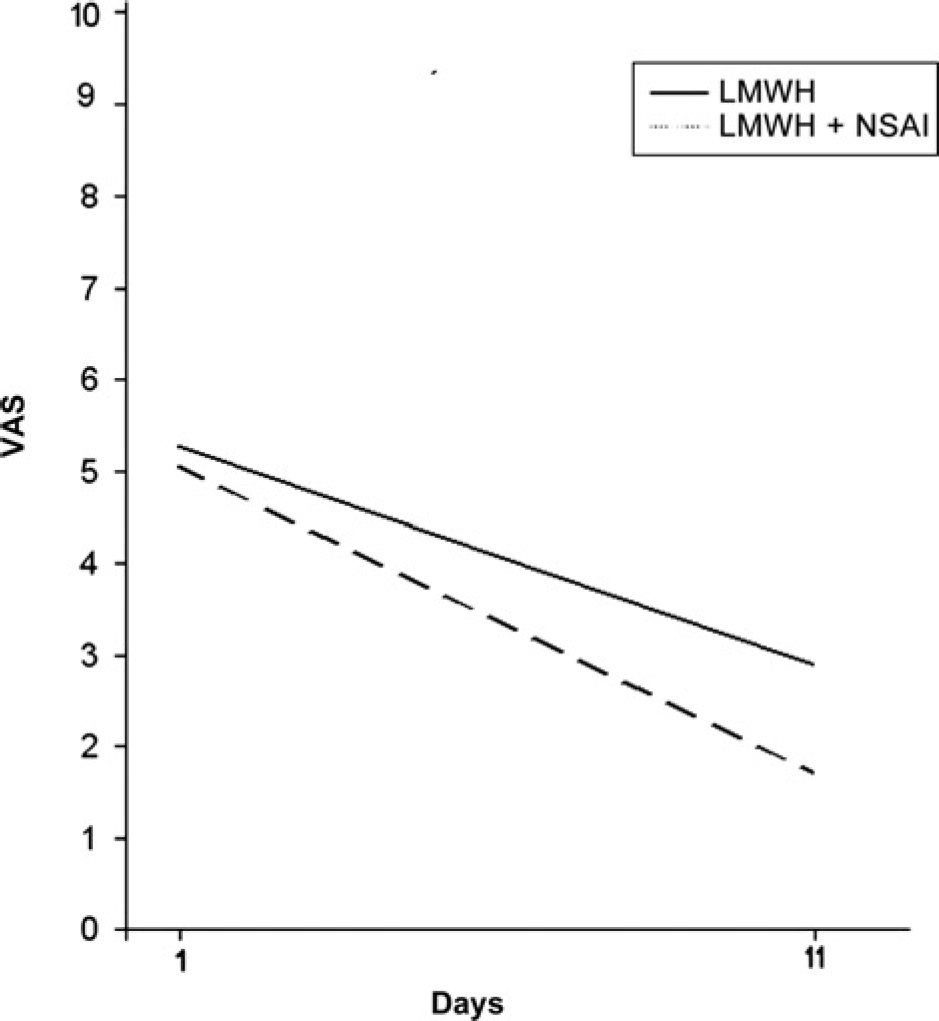
The mean palpable cord visual analogue scale (VAS) scores of both groups
Clinically, no symptomatic DVT or pulmonary embolism and extension in thrombotic process were determined in both of the groups.
No death or major haemorrhagia was observed during treatment in both of the groups. Haematuria was found in one patient included in group II.
Both of the treatment regimes were well-tolerated. No drug-related side-effects were seen.
Discussion
SVT is seen in lower extremity superficial veins with a rate of 80–90%. Seventy percent of those patients have varicose veins as well. Pain, tenderness, erythema, local hyperthermia, oedema and induration are presented at the affected veins. 10 It is not always easy to differentiate between SVT with lymphangitis, cellulitis, insect bite or erythema nodosum. 3 Thus, colour Doppler examination should be applied routinely. This examination is required for imaging deep venous system as well. Because when thrombus extends to the proximal of thigh, it may reach the deep venous system through saphenofemoral junction and lead to a pulmonary embolism risk. 4 Even if it does not extend to saphenofemoral junction, it may reach deep veins through perforator veins or through saphenopopliteal junction and cause a pulmonary embolism. 3
The earlier treatment methods for SVT were elastic compression bandages and anti-inflammatory creams. Later, local thrombectomy was started to be applied to the patients with the complaint of serious pain. 3 Today, although different treatments are applied, no standard treatment method is determined yet. Vein ligation, stripping and phlebectomy are the other surgical methods used. The success of stripping was shown to prevent extension of thrombus. 2,11 However, vein ligation do not provide the same successful results. Since the incidence of thrombus extension is higher in vein ligation compared with that of medical treatment, usually medical therapy is preferred. 3 Medical therapies applied today are unfractioned heparin, LMWH, anticoagulant drugs, fibrinolytic drugs and NSAI agents. 6,12
High and low doses of unfractionated heparin were used successfully in the treatment. 13 Thereafter, LMWHs were preferred due to their easy-to-use character and succeeded in terms of efficiency. 14 The studies showed that body-weight adjusted subcutaneous LMWH to be at least as safe and effective as standard heparin in the treatment of venous thromboembolism. In previous years it was shown that once daily regimen of LMWHs is as safe and effective as the regimen of twice daily administration. In different studies, the daily doses of LMWH in anti Xa IU/kg/day were similar: 175 for tinzaparin, 200 for dalteparin and 190 for nadroparin. 15 The study in which Ca-nadroparin was used on treatment groups in a fixed dose with regard to weight was compared and no difference was determined in terms of efficiency between the two treatment groups. 16
Nimesulid, an anti-inflammatory agent, was reported to be a successful alternative in SVT treatment. 1 Anti-inflammatory drugs exhibit significant success in preventing extension of thrombosis and relieving of symptoms such as pain and tenderness. The oral and topical use of diclofenacin, an anti-inflammatory agent, is safe and effective as well. 17 In another study, treatments with LMWH enoxiparin and NSAI agent tenoxicam have been compared and they were both found to be effective in preventing recurrences, extension of thrombosis and thromboembolic complications; however, LMWH was reported to be more effective than the anti-inflammatory agent. 5
Oral anti-inflammatory drugs may exhibit gastrointestinal side-effects. However, those effects may be precluded by using protective drugs. We applied such drugs to both of the groups in the beginning of the study as well.
Since we know LMWH and NSAI agents are effective and reliable in SVT treatment, this study was designed to see if they can be more efficient when used in combination. We believe that NSAI drugs, which are effective for relieving symptoms and are also not expensive, can be used along with LMWHs in treatment. No thrombus extension, DVT or pulmonary embolism was seen in any of the patients regarding both groups. We determined success in relief of symptoms in both of the treatment groups. However, the combined treatment in which LMWH and NSAI drugs have been used together was more effective compared with the treatment including LMWH singularly. The significant relief in pain and tenderness were remarkable. Actually, the most disturbing symptoms were pain and tenderness.
Conclusion
The results of this study suggest that the combined therapy of LMWH and an anti-inflammatory agent is more effective than LMWH in the treatment of SVT. This combined therapy as an efficient and reliable option to be remembered in the treatment of SVT. However, there is a need for further studies with larger patient groups to confirm the result of this study.