
Abstract
Objective
The purpose of this paper is to examine existing literature on physicians’ perceptions towards brand medicines, to examine the extent to which brands influence drug prescription and whether pharmaceutical industry influences the prescription of brands, as well as to examine the loyalty of physicians to a brand when prescribing drugs or willingness to switch to generic drugs.
Methods
Related articles published in different online databases from 2000 to 2017 were surveyed; 38 scientific articles indexed in Google Scholar, Science Direct, and PubMed were selected for review. Articles focused on physicians’ perceptions towards brand drugs and its effect on prescribing were extracted. The experimental design and quantitative and qualitative methods used in the studies were analyzed. The deductions made in each study were examined in tandem with the objective of the review.
Findings
The studies showed that physicians from high-income countries are inclined to prescribe generic drugs more than brand, whereas those from low-income countries heavily prescribe the brand drugs. The studies also revealed that brand influences the prescribing behavior of physicians. Five studies reported that marketing endeavors encourage the physicians to prescribe brand medicines, while three studies stated that physicians have a high loyalty toward brand medicines irrespective of country’s income. Other studies provided evidence that physicians are disposed to switching from brand to generic medicines under certain conditions. Marked differences in the prescribing generic drugs use by physicians among different age were observed. General physicians and pediatrics were more likely to suggest switching from the brand to generic drugs. The majority of physicians were familiar with biosimilars drugs.
Conclusion
Generally, the studies showed that physicians tend to have mixed views regarding prescribing brand medicines. The perceptions of physicians towards the brand drugs were found to differ in relation to the nature of healthcare system and level of development.
Introduction
Brand medicines are typically the original products that are discovered and developed by the pharmaceutical company. 1 In fact, the brand drug manufacturers must first gain approval from the Food and Drug Administration (FDA) to sell and market their medicines. Moreover, drug patents are usually valid for 20 years after the drug is invented. The patent, in fact, protects the innovator manufacturer and does not allow any other firms to make and market the drug. After the patent of the original brand is expired, other pharmaceutical companies can start to make and sell the same medicine “branded generic” to the pharmaceutical market under a different brand name.
A branded generic is an off-patented medicine that is re-issued into the market with a different brand name. Inventor’s companies create their own generic because they want to continue to profit on their customers who perceive their drug has come off patent and that there are generic drugs available. These branded generics are usually given a brand name, but the trend is that the generic name is primarily focused on a brand name. Generic medicines which may be produced by manufacturers other than the original firm are usually unbranded products with chemically identical active ingredients. 1 Theoretically, generic drugs are equivalent and might, in fact, be excess in developed countries. Actually, they are typically sold as a brand or under a proprietary name as “branded generics.” In developing countries, very few medications are patent-protected and almost all drugs are “branded generic” as per international standard.
The brand and generic medicines are differentiated based on inefficient ingredients (such as flavors and preservatives), shape, packaging, and color. 2 Because of these differences, the generic drug manufacturers are required to submit additional paperwork to the FDA to prove that their product is manufactured in accordance with good manufacturing practices and is as pure and stable as the brand name product. Brand drugs are generally more expensive compared to their generic equivalents because of its more research and development costs; hence, it is a challenge to keep it economically competitive. Brand drugs are more expensive than its generic equivalents because of its perceived higher quality and customers strongly prefer brand drugs. 3 Despite the relatively high pricing of brand medicine compared with the generic products, the branded drugs still maintained high market shares.
The majority of the big pharmaceutical firms prefer to market their drugs under brand names, which allows them to position and promote enough to fulfill the regulatory standards and product stability. 4 In fact, these companies invest heavily in marketing in order to develop strong worldwide recognition of their brand names as well as create a brand image among physicians and consumers. 5 Several theories consider the brand to be a significant factor that maximizes company’s profits and enable communication between the pharmaceutical firms and physicians. 6 Marketing managers to consider strong brands to be the cornerstone of physicians’ loyalty 7 and an influential factor in maintaining a competitive advantage for their companies. Physicians, in turn, tend to select a drug based on their preferred brand or firm in a case where no other factors such as price influence their judgment. 8 Physicians may prefer a specific brand because of its higher quality, which is promoted by advertising activities.
Studies on the prescribing behavior of physicians suggest that new brand drugs increase the interest of physicians, and thus, they are inclined to use drugs endorsed by their colleagues. 9 This implies that when given the choice between two similar products, the physicians often select the recognized brand, particularly when less qualitative information is available. This decision making can have a significant influence on the prescribing behavior when that brand name is linked with efficiency. 10 Furthermore, cognizance of one of the brands in a category will result in the repeated selection of that brand by the physician even when the generic option is available but offers quantitatively established lower quality. 11 In this line, it can be argued that several physicians opt for these brands and decline the use of substitutes (e.g., generic drugs) even though offered at relatively lower prices. 12 Therefore, related literature posits a consensus on the presence of drug brands in the prescription.
However, given the peculiar and distinct nature of brand medicine category, further studies are needed. 6 Contextually, existing reviews are narrowly focused and only partly present the perceptions of physicians towards generic drugs. For instance, Hassali et al. 13 reviewed 16 studies related to physicians’ perceptions and attitudes towards generic medicines in low- and medium-income countries. Toverud et al. 14 concluded that physicians and pharmacists are cognizant of the role played by generic drugs in improving worldwide availability of drugs. Thus, it can be deduced there is no detailed review of physicians’ perceptions towards brand drugs. To fill this gap, this study conducted a semi-systemic review that uses predefined criteria to identify studies in order to re-examine the physicians’ perceptions towards brand drugs as well as the effects of the the brand on physicians’ prescribing decisions.
What are brand drugs?
In marketing, the brand is defined as a “name, term, sign, symbol, design, or a combination of these elements, used to identify the products or services of one seller or group of sellers and to differentiate them from those of competitors.” 15 In a different study, Kapferer 16 defined a brand as the combination of name, symbol, design, and packaging by which the product differs from its competitions. Based on a consumer viewpoint, Ambler et al. 17 took an advanced approach to defining a brand as the assurance of bundles of attributes that motivate and provide satisfaction to the customer. These attributes of the brand may be physical, emotional or rational, tangible or intangible.
In the pharmaceutical field, branding is an approach to differentiating products. Drug branding is often considered as giving an attention-grabbing name to a product or drug. 18 Kumar et al. 19 defined drug branding as giving a name or a symbol to a drug in order to differentiate it from other substitutes as well as to imprint the drug in the minds of physicians as medicine with tangible (rational) and intangible (irrational or emotional) benefits. The difference based on branding is often used as an instrument for differentiation since it is easy to identify additional elements in a product, whether tangible (rational) or intangible (emotional). 8 Therefore, branding of drugs is usually perceived as an important aspect of pharmaceutical marketing, possibly due to the official designation and labeling in the drug’s profile, and the ban on direct advertising of ethical drugs to patients, and short life cycles of products. 18 Given the trust and confidence of physicians and patients in the brand drug, brands add a greater value to the medicine. 18 Prescribers are encouraged to prescribe drugs by their brand name. This is because that brand medicines have guaranteed efficiency and confidence when used by physicians for treatment.
Physicians generally have their personal list of drugs they prescribe, which are compiled based on drugs they are aware of, respective brand names, and new drugs in the market. Moreover, brand names generate awareness among several physicians and allow them to develop an opinion of the brand and its image, in terms of safety and efficacy, which are being communicated through medical representatives (MRs) of drug firms. In addition, drug branding can have a positive effect on the prescribing judgment of physicians. 9 In the context of prescription behavior, continual prescription of the same brand drug (brand loyalty) is a very important phenomenon in the pharmaceutical industry. 11 Nonetheless, while some physicians have a preference for brands manufactured by certain companies due to their loyalty, other physicians prescribe the same brand due to its efficacy confirmed by the success of previous treatments and experience as well as the impact of marketing efforts. 7
However, despite the positive effect of prescribing drug branding, the brand can be harmful to patients which pose a challenge to its success in the market. For instance, when physicians become cognizant of the side effects of one brand, they are more expected to prescribe its alternatives and thus the life cycle of the brand will become very short. Moreover, the increased focus on generic drugs as cost-effective alternatives to the expensive brand name drugs are perhaps other barriers to the use of brand medicines by physicians. Therefore, the dilemma generally still remains regarding the actual perceptions of a physician towards brand drugs and effects on prescribing.
To resolve the aforementioned dilemma, this paper extracted the perceptions of physicians towards brand drugs from the published articles for the following seven perspectives: perception of physician towards brand medicines; effects of the brand on prescribing; physician loyalty to brand medicines; physicians’ disposition to switch from brand to generic drugs or substituting a branded medication with its generic equivalent; physicians’ age and experience and their attitude towards prescribing generic drugs; switching from brand to generic among specialists especially in areas such as pediatrics and epilepsy; and physicians’ attitudes towards prescribing of generic biosimilar. Furthermore, it is pertinent to obtain a better understanding of the effects of pharmaceutical industry promotions on the prescription of brand drugs.
Methodology for the review
A systematic search was conducted for English-based scientific articles indexed in several electronic databases such as Google Scholar, Science Direct, and PubMed. To ensure the review is consistent with the current practice, this research was restricted to studies published between 2000 and 2017. The search approach combined terms for “brand,” “brand drugs,” “brand medicines,” “physician prescribing,” “factors influence prescribing,” and used free text words and medical topic heading such as branded vs. generic. The references listed in the reviewed articles were also examined and checked for additional relevant studies on brand drugs.
Once the searches had been run, articles were downloaded and entered into reference manager software (Mendeley). Articles were subsequently vetted for their eligibility to be included in the list of reviewed articles. The initial search of the electronic search of databases resulted in 529 titles and abstracts. However, 494 titles were unrelated to physicians’ perceptions towards branded medicine and effects on prescribing behavior. The remaining 52 articles were set aside for evaluation. Additional scrutiny showed that 14 of studies from 52 (per Figure 1) were excluded, while the remaining 38 were selected for review which categorically examined physicians’ perceptions towards branded medicine, but focused mainly on generic medicines, hence they were excluded from further analysis. The flow chart for the reviewed studies is shown in Figure 1.
The study flow chart of articles included in the review. *All met the inclusion criteria.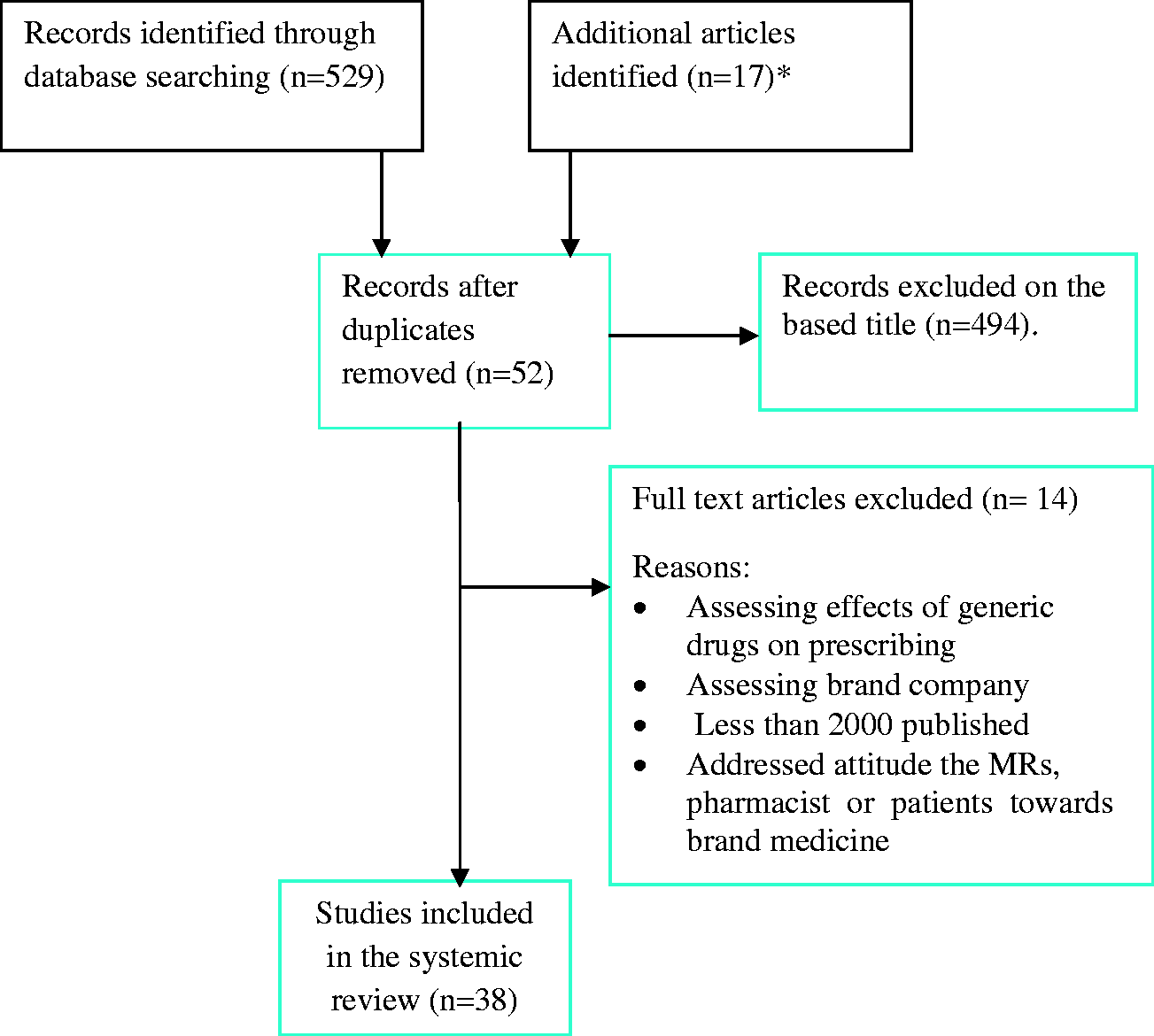
Criteria for selecting the studies
The studies selected for review were analyzed with quantitative (survey study), experimental (panel data of physicians or industry experts), and qualitative methods (interviews and focus group). Articles such as reviews, commentaries, letters to editors, and small essays were excluded. Non-English-based published articles were excluded. Articles that evaluate the physicians’ perceptions towards generic drugs, as well as the effect of generic drugs on prescribing behavior, were excluded from this review, except studies involving the switch from a brand name to a generic drug among specialists. Studies focused on physicians’ attitudes towards prescribing of generic biosimilar drugs were also included, because their results involved brand drugs. Also excluded were studies that focused on brand drug prescription by non-physicians, such as patients, nurses, pharmacists, and pharmaceutical industry. Furthermore, perceptions of a physician towards brand companies were not taken into consideration.
Methodological quality
Each article was concisely reviewed to ensure quality. The study type and characteristics comprising the author, journal, and country of origin, the number of respondents, study design, objectives, findings, and limitations were reported. Afterward, five outcomes were extracted from the articles, which include physician’s perception towards brand medicines, physician prescribing practice, physicians’ disposition to switch from brand to generic drugs, the effect of the brand on prescribing behavior, and the effects of pharmaceutical industry marketing on the decision to prescribe the brand.
However, limitations were not reported for 22 studies.11,20–30,42,44–53 One study suffered low response rate 26 while another study 31 was affected by small sample size. Twelve studies employed random sampling.10,21–23,27,28,32,38,40–43 Four studies used convenience sampling9,39,48,50, another study used purposive sampling 33 , while the study by Shamim–ul–haq et al. 30 used cluster sampling and nine studies not reported.42–47,49–52
General characteristics of the reviewed studies
Characteristics of the included studies in systematic review

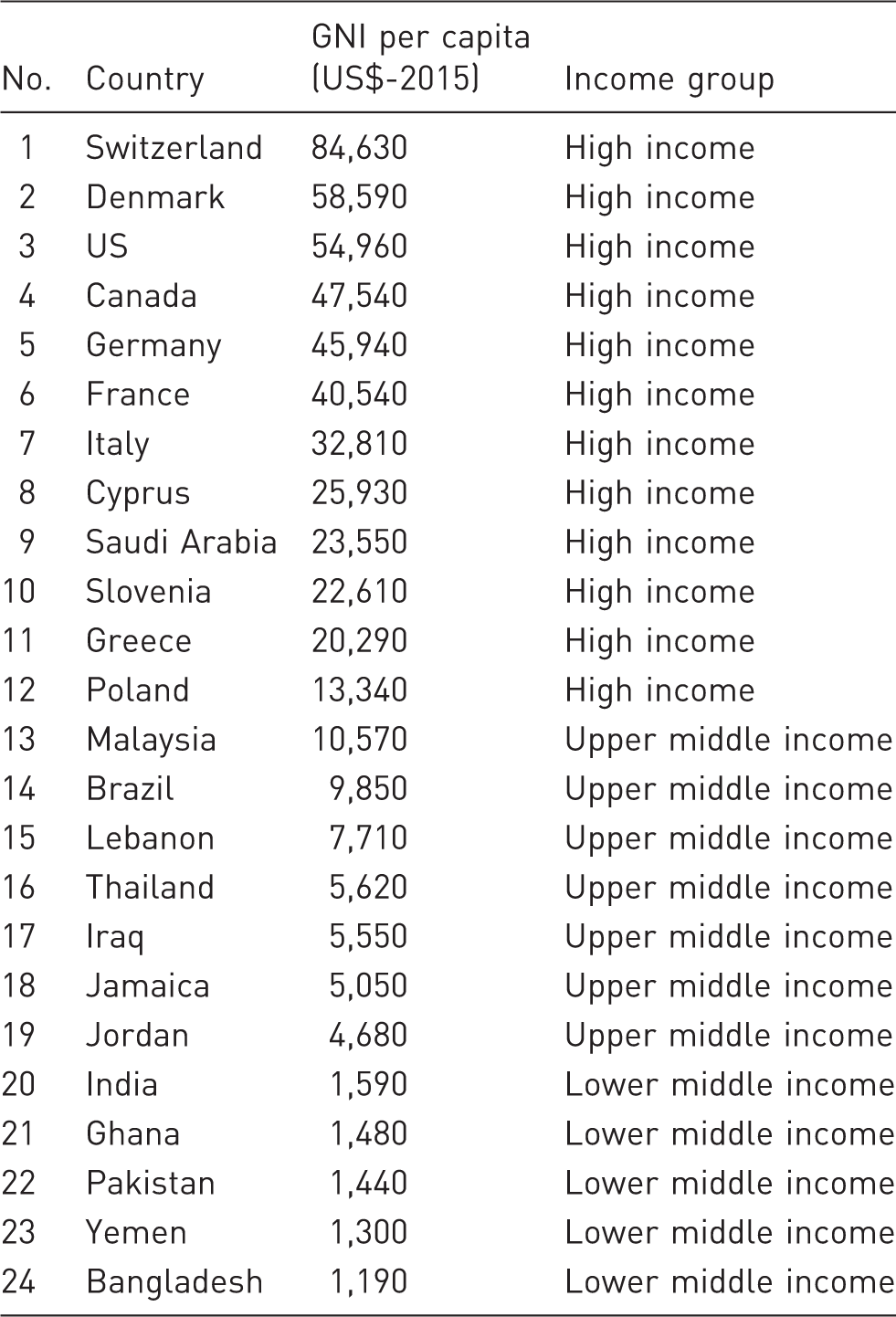
List of countries and GNI per capita. 56
Summaries of the variables that were investigated in the studies

Results
Table 1 shows the key results of the reviewed studies. A detailed and concise review of the content of each research article reveals the perceptions of physicians towards brand drugs. The findings are grouped into the following eight sections.
Perceptions of physicians towards brand medicines
Seven of the 21 studies explored the physicians’ prescribing practice of brand medicines.20,25,27,30,34,36,37 In other words, the studies simply investigated whether a physician prescribes brand drugs, rather than the influence of branding on prescribing behavior. The study carried out in Thailand by Plianbangchang et al. 20 reported that few prescriptions were written by brand name. The study found that prescribing based on brand name is focused on off-patented brand medications. In a different study carried out in the US, Joyce et al. 37 investigated the factors that affect prescribing choices and reported that physicians prescribe an average of at least three different drugs while one in six physicians prescribe the only brand drug in 8 of 10 therapeutic cases. A cross-sectional survey carried out by Theodorou et al. 34 in both Greece and Cyprus examined the attitudes and factors that influence physician prescribing decisions. The majority of the physicians surveyed in the study agreed that though the efficacy and safety of generic medicines may not be outstanding factors, they are preferred over the brand of the drugs.
Furthermore, Hossain et al. 27 carried out a cross-sectional survey in Bangladesh, which found that about 66% of physicians prefer to prescribe drugs with brand names while the other 33% are inclined to prescribe to generic drugs. Al-Shami et al. 24 and Bashrahil 25 examined physicians’ prescribing practice and the use of essential drugs in Yemen. The findings of these studies are close, with Bashrahil, 25 reporting 60.8% of prescription drugs were brand drugs, while Al-Shami et al. 24 found that 76.8% of prescribed antibiotics were brand drugs. In another study, a postal survey in Ghana conducted by Afriyie et al. 36 discovered that only 39.5% of prescriptions were brand drugs.
Effects of brand on physician prescribing behavior
Six out of the 21 reviewed studies9,23,29,30,32,33 examined the effects of the brand on the prescribing behavior of physicians. Quantitative studies carried out by Ladeira et al. 9 and Narendran and Narendranathan 29 using a self-administered questionnaire found that brand has a strong effect on prescribing behavior of physicians. Cross-sectional studies by Bamoriya 33 and Tajdar et al. 23 discussed the factors that influence drug prescribing in India and Pakistan and found that brand is an important factor capable of influencing prescribing behavior. A cross-sectional study in India 32 reported that physicians are more interested in brand names of drugs. In contrast, Shamim–ul–haq et al. 30 found that brand plays an insignificant role in influencing drug prescribing in Pakistan. Wong et al. 22 examined the physicians’ perceptions about generic medicine in Malaysia using interview data. Although the study reported a little detail into the effect of the brand on prescribing, they discovered that professionals might be inclined to prescribe original brands over generic drugs.
Effect of pharmaceutical industry on prescribing of brand medicines
Six of the reviewed studies explored the effect of different pharmaceutical promotions on physicians’ decision to prescribe brand drugs. In Greece, Karayanni 10 discovered that the brand prescription was influenced by advertising and detailing, indicative of physicians’ preference for branded drugs over generic drugs. Narendran and Narendranathan 29 reported that physicians in India were influenced by the largesse or samples provided by sales persons, which makes the physicians biased towards prescribing the specific brand being promoted. An overwhelming tendency for prescribing drugs by brand names (99%) by the physicians was observed in India. 56 Mikhael and Alhilali 31 performed a survey of specialists in Iraq and found that physicians are influenced by MRs’ promotional literature when they prescribe the brand drugs. Similarly, a survey study carried out by Lieb and Scheurich 26 in Germany suggested that physicians who never participated in funded events had a lower number of on-patent branded drug prescriptions, a lower proportion of branded drugs, a higher proportion of generic drugs, and a lower expenditure on off-patent branded drugs per patient. An experimental study 35 carried out in Denmark revealed that physicians do not appear to prescribe brand drugs and thus recommended the removal of promotion inducements for physicians to prescribe brand drugs in order to increase the use of generic drugs.
Physicians’ loyalty to brand medicines
Three studies10,11,28 evaluated the replacement of generic prescribing, brand persistence, and brand as a marketing tool. An experiment study by Janakiraman et al. 11 reported that physicians in the US persistently prescribe branded drugs (under patent protection) even when a cheaper generic drug is obtainable, implying that physicians may not be making the most economical decision, but rather take therapeutic effectiveness into consideration. Similarly, a cross-sectional study carried out in Greece by Karayanni 10 reported that branded medicines are less important than prescription loyalty to a particular brand. El-dahiyat et al. 28 showed that 50–80% of physicians in Jordan working in the private sector were more likely to oppose replacement of branded with generic drugs, possibly because of their strong loyalty to the brand name.
Physicians’ willingness to switch from brand to generic drugs
A cross-sectional survey conducted in Slovenia by Kersnik et al. 21 examined attitudes of general practitioners (GPs) towards prescribing the generic drug. The study found that 96.3% of physicians were disposed to switching from brand drugs to relatively cheaper generic drugs if the price was lower by 25–35%. Similarly, a recent survey in Iraq carried out by Mikhael and Alhilali 31 showed that the prescription disposition of physicians significantly shifts from brand to generic drugs because of marketing efforts such as gifts.
Physician’s age and experience on prescribing generics drugs
Shrank et al. 38 evaluated the physicians’ perceptions towards generic medicines in the US. The age of respondents was associated with physicians’ perception of generic medicine. Older physicians (than of age of 55 years old) were more than three times as negative to generics drugs as younger physicians. The youngest physicians aged below 35 years were negative towards the quality of generic medicines. They further reported a personal preference for generics drugs or to suggest them to their family.
An additional study in the US found that older doctor, as well as those who work in small practices, were more likely to be persistent with a branded drug when a cheaper generic is available. 11 A study which surveyed GPs in Malaysia revealed that respondents’ age and years of practicing were significantly associated with prescribing of generic drugs. GPs older than 60 years and those who have more than 30 years of medical practice were considerably less likely to prescribe generics drugs than those who were younger and have practiced for less than 30 years. 39
In Poland, Lewek et al. 40 carried out a survey to examine the opinions of primary care physicians on generics drugs and to determine the factors which may affect prescribing generic. While this study confirmed that generic and brand name drugs are equally effective, no correlation was found between physician age and opinion on the efficacy of generics, or physician age and preference for generics. In Greece, Tsiantou et al. 41 investigated the profile of doctors and other factors that influence prescribing generics decision. The study suggested that older physicians were more likely to prescribe generics drugs than younger ones. Others factors such as specialty and work of experience were not significant. Although physicians seemed to be positive about generics drugs, they were preferred to prescribe the brand medicines.
A study in Saudi Arabia examined doctors’ perceptions and their attitudes towards generic prescribing. The study found that 75% of younger physicians aged between 30 and 40 years were less likely than older physicians (93%) aged between 40 and 50 years and 89% of those above 50 years to report that they knew enough about the therapeutic value of generics drugs to prescribe them and to show this value to patients and peers. Also, the results suggested that primary care physicians were significantly more likely to prescribe generic drugs than hospital and private physicians. 42
Another study in Pakistan suggested that GPs who have more than 10 years of medical experience expressed their doubts towards the prescribing of low-cost brands. Physicians who aged 41–50 years and have practice more than 16–20 years showed higher positive perception towards the safety and affordability of generic medicines. In contrast, senior general practitioners expressed a greater sense of discomfort to prescribe all local generic drugs when compared to their younger and middle-age counterparts. Highly experienced and senior general practitioners expressed their concern about the quality check of locally manufactured generic medicines. 43 Furthermore, El-dahiyat et al. 28 examined factors that affect physicians’ prescribing of generic drugs in Jorden. The study found that doctors working in public tended to accept generic substitution more compared with physicians working in private sector.
Specialists’ attitude towards switching from brand to generic drugs
Using a public web survey in Italy, Fabiano et al. 44 found that GPs and family pediatricians were less confident in prescribing generics equivalents instead of branded drugs, and therefore, the prescribing of generic medicines were low. Only 14% of physicians reported that more than half of their patients have treated with generics drugs. Nearly half of them usually proposed to patients the substitution of a “branded” with a generic medicine and the majority declared to explain to their patients the characteristics of generic drugs regularly. In addition, 54.4% believed that reason for limited prescription of generics was a still too diffuse skepticism about them. In contrast, 20.4% believed that knowledge about generic drugs was still insufficient. Further key issues related to preventing generic prescribing are the safety of switching from brand drugs to generic equivalents. The study concluded that more information about generic medicines is required to increase the prescribing of the generic medicines among Italian family pediatricians.
Gossell-Williams 45 examined the attitudes of physicians from various specialties (mostly general/family practice physicians) towards generic substitution in Jamaica; 49% of the physicians were mostly prescribed generic brands willingly when the cost of generic substitutes was a significant factor. Furthermore, half of the physicians felt that the bioequivalent of generics drugs were therapeutically equivalent to those branded drugs. However, 33% mentioned that they could identify at least one case related to the clinical problem of generic medicines in previous years and also indicated that this did not happen with the brand medications.
Berg et al. 46 evaluated the perceptions of physicians and patients on generic of branded antiepileptic drugs (AED) substitution. Of the physicians surveyed, 88% of respondents were worried about a rise in breakthrough seizures in patients who switched from a brand AED to a generic. Further, nearly two-thirds of respondents have linked breakthrough seizures to generic AED substitution, but at the same time, 75% were concerned about efficacy. Only half of respondents were very likely to request that brand AEDs not be substituted with a generic. Nevertheless, the physicians’ perceptions do not align with the FDA position that generic AEDs have the same effectiveness and safety profile as branded AEDs.
Haskins et al. 47 conducted a telephone survey in five developed countries such as France, Spain, Germany Canada, and the United Kingdom (UK). Overall, the study revealed that 65% of AED prescriptions were for brand name drugs. The greatest proportion of prescriptions for branded AED was written in France (98%) and Spain (91%) and the least in Canada (53%) and the UK (54%). However, 55% of physicians were opposed to generic substitution without physician consent. The greatest proportion of opposition was among physicians in Germany (70%) with the least opposition in France (15%). Furthermore, 27% of doctors, 18% of GPs, and 38% of neurologists believed that they had a patient who experienced a breakthrough seizure likely caused by switching from a branded to a generic AED. Nevertheless, 89% believed substitution should not be allowed in certain indications, and 76% felt pharmacies should be allowed to substitute a generic AED only with their consent, and nearly 47% believed the pharmacy should have patient consent.
Physicians’ attitudes towards generic prescribing of biosimilar generics drugs
Physicians’ attitudes towards generic prescribing of biosimilar should not be neglected. Seven articles in this review investigated the attitude of doctors towards generic biosimilar drugs.48–54
In Canada, Grabowski et al. 48 carried out a survey to evaluate attitudes towards biosimilars drugs among rheumatologists. Only 31% of physicians were familiar with biosimilars. Doctors who had more than 20 years of practice were significantly more likely to be very with biosimilars than the respondents with less than 10 years or 10–20 years of experience. Furthermore, 32% agreed or strongly agreed that they would be comfortable with indication extrapolation. Finally, 88% were highly concerned if a pharmacist had the ability to substitute a biologic drug for a biosimilar without the physician’s approval.
Based on the online survey, Molinari et al. 49 examined physicians’ attitudes from various specialties toward biosimilars medicinal products in the US, Latin America (Colombia, Mexico, Brazil, and Argentina) and Europe countries (Italy, France, Germany, UK, and Spain). Overall, the study revealed that the majority of respondents were familiar with biosimilars and wanted to be notified of substitutions. US physicians were 20% and 3% more likely to be familiar or very familiar with biosimilars drugs than Latin American and European doctors, respectively. And 80% of physicians from the US, 87% from Latin America, and 77% of Europeans believe that receive notification when the biosimilar is replaced is critical. Moreover, physicians in the US lack technical knowledge about the effects of biosimilars drugs sharing the same non-proprietary name.
Farhat et al. 50 surveyed professional healthcare in the Arab countries, Iran, Belgium, and Italy to understand the impact of various factors on the acceptance and future prescription of biosimilars drugs. Overall, 65.8% out of respondents had knowledge about biosimilars, and 63.2% agreed that biosimilars in these countries were already marketed. Only 41% confirmed that they prescribe biosimilars while 32.5% do not prescribe them. The main driver for prescribing biosimilars drugs was the drug’s approval by the FDA, the European Medicines Agency (EMA) (68.8%), a lower price (64.6%), bioefficacy (47.9%), safety (41.7%), and reputation of the manufacturer company (31.3%).
Hallersten et al. 51 evaluated physicians’ preferences from seven specialties on the type, detail, and sources of information of the biosimilar label when prescribing biologics drugs including biosimilars in seven European countries namely the UK, France, Germany, Spain, Italy, Poland, and Sweden. Overall, physicians prefer more product-specific information in the biosimilar label. The label for biosimilars drugs is the main source of information used by doctors. For 68.8% of doctors who prescribe biosimilars, the main prescription driver was the drug’s approval by the FDA followed by the lower price (60.7%).
Beck et al. 52 evaluated the knowledge, experience, and opinions of rheumatologists with biosimilar medicines in France. Overall, the majority of physicians reported that they had little knowledge and a lack of available information about biosimilar drugs. Only eight rheumatologists reported that they prescribed biosimilars drugs. However, 98.3% had at least one issue related to these medicines. Seven out 10 of physicians mentioned problems related to substitution, iatrogenic effects, or cost savings that might be achievable. Finally, the majority of the respondents were expressed a negative opinion about generic substitution by the pharmacist.
Bokemeyer et al. 53 evaluated gastroenterologists’ experiences and their views on biosimilars drugs in Germany. Only 61 % of the respondents reported that they prescribed Infliximab biosimilars drugs. However, 15 % considered themselves to be very experienced with biosimilars. Furthermore, 71 % indicated that the lower price is the most significant advantage of biosimilars comparison to the originator. Nevertheless, 68 % requested specific gastroenterological trials and registries to increase the data available on biosimilars drugs.
In an additional study in the US, Cohen et al. 54 assessed physicians’ awareness, knowledge, and perceptions of biosimilars medicines in the US. Overall, the majority of doctors have heard about biosimilars drugs but, at the same time, appeared to have a low knowledge of the fundamentals of biosimilars. Although physicians across specialties have positive attitudes toward biosimilars, some of them such as dermatologists and rheumatologists showed to be less enthusiastic and still had concerns regarding the safety of biosimilars. The authors concluded that more information regarding biosimilars drugs was required to address current concerns.
Discussion
This study identified 21 studies that examined the perceptions and attitudes of physicians towards brand drugs worldwide. The findings revealed that physicians are inclined to have mixed views as regards prescribing brand medicines. Related studies conducted in developed countries such as the US, 37 high-income countries, for example, Greece and Cyprus 34 , and medium-income country such as Thailand 20 indicate that physicians have a tendency to prescribe generic medicines over brand medicine due to the positive perception of generic medicines among physicians in these countries. This positive perception may be attributable to the fact that these countries observe a strict bioequivalence acceptability criteria for generic medicines, which are set by their relevant drug organizations. Moreover, these countries have more dependable public control procedures for producing and dispensing generic drugs to ensure better bioequivalence requirements for generic medicines. This deduction is consistent with a recent review by Toverud et al., 14 who found that medical professionals in European countries possess a high level of trust in the bioequivalence of generic drug with the branded analog regarding active element, dosage, and therapeutic effects.
In contrast, physicians in low-income countries such as Yemen, Bangladesh, and Ghana are inclined to heavily prescribe brand drugs.24,25,2736 This tendency has been attributed to the perceived safety and efficiency of branded drugs as well as the uncertainty over the quality of the generic drugs in these countries. Also, there is the perception that generic medicines are easily counterfeited, which may harm patients. Then again, marketing efforts provided by pharmaceutical companies to a physician may be a more plausible reason for brand prescribing in developing countries. The wide use of brand drugs results in increased cost of drug and healthcare expenses. Thus, the disparity in perception and attitude of physicians towards drug prescribing stems from considerable differences in the healthcare system, drug policies, the level of advertising by pharmaceutical firms, and drug information sources between developed and developing countries.
Based on the evidence presented, this review deduced that brand has an influence on physician prescribing decision. One plausible reason is that brand can create justifiable points for distinguishing competing drugs and thus influence physician decision to prescribe the drug. However, there is no unanimity in the literature supporting the notion that brand is a significant factor influencing the prescription decision. This may be attributable to the drawback of previous studies on physician prescribing behavior, where aspects of the brand were measured rather than the actual brand of the drug. Hence, it is difficult to confidently attach weight to the brand variable.
Furthermore, this review found that the promotions constantly advertised in the pharmaceutical industry play the key role in encouraging physicians to prescribe brand medicines. This is confirmed by the fact that physicians who never participated in sponsored events had a relatively lower number of branded drug prescriptions compared to those who did. 26 Moreover, this review points out that the effect of MRs in altering the prescription of brand medicines by physicians should not be ignored in low-income countries. For instance, studies have shown that the gifts or samples given by MRs put physicians under a certain level of commitment to prescribe the promoted brands.29,31 Other studies revealed that marketing endeavors of the pharmaceutical industry had an influence on prescribing patterns of branded drugs.25,36
This paper reviewed three studies that assessed the perceptions of physicians towards brand medicine in high-income countries11,10 and low-income country. 28 As a whole, the studies reported that physicians have a tendency to be loyal to brand medicine because of their therapeutic efficacy and safety and creating barriers to prescribing a new drug. It was also inferred that physicians find it difficult to change their perceptions towards certain brands. 11 This shows the influence of brand loyalty created by persistent and persuasive pharmaceutical marketing. Therefore, the effect of marketing efforts of pharmaceutical companies on brand loyalty is an area that needs to be further explored. Another plausible reason for brand loyalty is proven efficacy based on the experience of physicians with the drug. Thus, the brand is continually prescribed by physicians to ensure full recovery of their patients.
Nonetheless, a few studies in this review reported that physicians were more willing to switch from brand to generic medicines under certain conditions such as price and marketing efforts. This further confirms the notion that physician prescribing is always influenced by marketing efforts and price.
Physician’s age and experience on prescribing generics drugs were variable and occasionally contradictory. Studies suggest that younger doctors in the US, Pakistan and Malaysia with fewer years of practice were more likely to prescribe generic drugs than older physicians. In contrast, older physicians in Saudi Arabia and Greece were more likely to prescribe generic drugs more than younger, and in Poland, the age was not associated with the perception the physicians to prescribe or preference generic drugs. This might reflect differences in how the healthcare systems work or in differences in the consistency of medical instruction content about generic and brand name drugs over time.
Furthermore, these differences may be due to differences in the lack of doctors’ knowledge of generic medicines during their education and clinical practice as well as the inadequate regulatory framework of the generic market in the country. 41 The review also found that there were differences in the opinions of physicians on prescribing generic medicines in public and those of physicians on the private sector. Doctors in the public sector are likely to accept the substitute of the generic drugs more than those who were working in the private’s sector. Overall, the review suggests that there were significant differences in the prescribing generic drugs use by physicians among different age, years of practice, or different practice settings.
From the present review, four studies from high-income and middle-income countries indicate that knowledge on switching from a branded to a generic among specialists of family physicians, epilepsy and pediatrics and others. Although general/family physicians and pediatrics were more likely than physicians who treat patients with epilepsy to suggest switching from the brand to generic drugs to their patients, they expressed greater concern about the safety of switching to generic equivalents. In contrast, the physicians opposed generic substitution of antiepileptic drugs without physician’s approval. The reason for these results could be that the physicians were worried about the therapeutic equivalency of interchangeable medicines, breakthrough seizures after switching, and pharmacists’ ability to substitute safely.46,47 Generic substitution of antiepileptic drugs is still a matter of controversy and concern among physicians.
From the current review, there were seven articles, six from high-income countries and one from the middle-income country was accessed in which knowledge of prescribing biosimilar drugs. Overall, all studies reported that the majority of physicians were familiar with biosimilars drugs although that they had a low level of knowledge of the basis of these drugs across countries in worldwide. Thus, the biosimilar generic prescribing drugs were low. Another interesting result was that physicians, regardless of the lower price of biosimilar drugs, expressed concerns over the effects and safety of prescribing biosimilar drugs. There was some evidence about the negative views of physicians towards biosimilars drugs. The physicians appeared to be worried about substitution by the pharmacist or switching between different generics should not be recommended medicines.
As mentioned above, physicians in the US49,54 had a low level of knowledge regarding the effects and fundamentals of generic biosimilar drugs compared to their counterparts in European countries and an early-stage healthcare system like Arabic countries. This may be attributed to the fact that views of physicians in the US who most likely did not yet have any practical experience in the prescribing biosimilars drugs since no biosimilar was authorized in this country before March 2015. On the contrary, doctors in the Europe countries have more practical experience with the biosimilar drugs, because, for several years, the European Union countries has been the first and only jurisdiction in the world to adopt a regulatory framework for the authorization of biosimilars drugs. 51 Overall, this review concludes that there is a lack of confidence among physicians towards biosimilars generics, and knowledge is one of the most factors to be improved for higher prescribing of biosimilars generics drugs. Therefore, the review of the literature in this area highlights a significant need for more information and education about biosimilars medicines for physicians across countries.
Strength and limitations of the review
This study provides a comprehensive review of the perceptions of physicians towards brand medicine and the effects of the brand on drug prescription. This study is considered novel, given that there is no similar review conducted on this particular topic. Although a recently published systematic review by Hassali et al. 13 focused on perceptions of physicians towards drug prescription in low- and middle-income countries, the study only focused on generic medicines. In addition, Toverud et al. 14 reviewed the perspectives of physicians and pharmacists on the use of generic drugs. However, the review found little evidence on the perception of physicians towards brand medicines as well as the effect of drug brands on prescribing decisions. Therefore, this current review has expanded the results of preceding reviews regarding perceptions of physicians towards brand drugs, the effects of the brand on prescribing decisions, the influence of marketing efforts on the prescription of brand drugs, physician’s age and their experience on prescribing generic drugs, switching from branded to generic equivalents among specialists, and attitudes of physicians towards biosimilar generic drug prescribing.
Despite the use of established methodologies by this review, several limitations arose. First, this review only considered recent studies from the year 2000 and onwards; however, this is justified by the higher relevance of current findings compared older studies. Second, most of the reviewed articles are survey papers, which have design limitations such as small sample size, some non-validated questionnaires, and pilot tests, in addition to the difficulty of directly measuring the brand. Other limitations relate to brand medicine, where only results from studies regarding the perception of physicians and effects on prescribing were extracted. This review excluded the results about perceptions towards generic medicines, although numerous studies have been conducted on generic medicines. Hence, the perceptions of physicians for towards brand and generic medicines in different countries should be compared in future studies.
Furthermore, because the current review was focused on the opinions of specific physicians’ populations, the patients or the general public were not examined in the area of switch brand to generic among specialists such as epilepsy and pediatrics. Research on this subject was limited and fragmented, and most studies investigated public opinions, patients, pharmacists, the pharmaceutical industry, and using different populations in distinct settings.
Implications for policy makers and practice
Research on perceptions of physicians towards brand medicines has implications for drug control policies and practices. Based on this review, marketers and health decision-makers can have an insight into physicians’ perceptions of brand drugs compared to perceptions of generic drugs. This will help them to determine alternative marketing strategies in order to increase brand trust and boost the effects of branding on the prescribing decision as well as to improve overall brand perception and image especially in developing countries. On the other hand, examining the brand loyalty and the switching of the brand to generics is a key to understanding the generics paradox for generics manufacturers and policy makers. This review also provides critical information that will be valuable to researchers evaluating the effects of brand drugs on physicians’ prescription behaviors.
The review found evidence of the lack of an inadequate knowledge on biosimilar drugs needs more information to address the effects and safety of these drugs. To develop such a policy, more information on biosimilar generics to physicians during their education and clinical practice should be implemented. Also, promotional efforts for the pharmaceutical industry should be conducted to promote the bioequivalence for biosimilar generic medicines to doctors.
Conclusion
This paper is a novel study on physicians’ perceptions towards brand drugs and its effect on the prescription decision. The perceptions of physicians towards the brand drugs were found to differ in relation to the nature of healthcare system and level of development. The physicians prescribed more generic drugs than brand drugs in countries with reliable public control routines for drugs as well as better bioequivalence requirements concerning generics. The review showed that drug brand can influence the prescribing decision of physicians. The majority of physicians acknowledged that their prescribing decisions could be influenced by marketing efforts of pharmaceutical industry, while some physicians showed loyalty to a specific brand. Some physicians asserted that they are willing to switch from brand to generic drugs, due to the notion that their prescribing decisions may be affected by promotional efforts or prices of the drugs.
The review suggests that there were significant differences in the prescribing generic drugs use by physicians among different age, years of practice, or different practice settings. The studies reviewed indicate that general/family doctors and pediatricians were more likely than physicians who treat patients with epilepsy to suggest switching from the brand to generic drugs to their patients. Physicians regardless of specialty expressed greater concern about the safety of switching from brand to generic. All studies reported that the majority of physicians were familiar with biosimilars drugs although that they had a low level of knowledge of the basis of these drugs across countries in worldwide. It appeared that, although the physicians were prescribing biosimilars generics, they still had concerns about the effects and safety of prescribing biosimilar drugs. Therefore, biosimilar generic prescribing drugs were low. This highlights a significant need for more information and education about biosimilars medicines for physicians across countries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.