
Abstract
Background
One possible mechanism for lowering expenditure on drugs and increasing their accessibility is by prescribing generic drugs, which are less costly and have equivalent safety and effectiveness profile as brand drugs. However, in Addis Ababa brand-prescribing practice is so common to the extent of making the health department administration of the city to write letters to subcities and hospitals discouraging brand prescribing. This study tried to identify the magnitude and factors affecting brand prescribing in the city. Objective: General objective of this study was to assess magnitude and associated factors of prescribing drugs by brand names at Addis Ababa.
Methods
An institution based analytical cross-sectional study design was employed from May to August, 2022, using a sample of 485 prescribers. The hospitals were selected by using simple random sampling method and prescribers from different departments were selected by using systematic random sampling method. Data was collected using semistructured, self-administered questionnaire and entered into Statistical Package for Social Sciences version 25 for analysis. The data was described using percentages, graphs and tables. Mean and standard deviations were calculated to identify measures of central tendency and dispersion. Association between dependent and independent variables was checked using bivariate and multivariable logistic regression models. Statistical significance was declared at 95% confidence interval and p < .05.
Results
The magnitude of prescribing drugs by their brand names was 54.0%. Being trained on good prescribing practice (AOR: 6.81; 95%CI: 2.08-22.28), confidence on Ethiopian Food and Drug Administration Authority (AOR: 18.18; 95%CI: 6.78-48.80), and knowledge about generic drugs (AOR: 11.86; 95%CI: 4.76-29.55) were found to be independent predictors of prescribing drugs by their brand names.
Conclusion and recommendation
Brand medicine prescribing is positively associated with training on good prescribing practice and knowledge about generic drugs. Hence, training prescribers on good prescribing practice and educating them about generic drugs can minimize brand prescribing.
Introduction
Drugs are essential components of health care delivery that produce the desired effect of improving illness when used rationally. The 1985 World Health Organization (WHO) meeting of experts on the rational use of medicines requires that “patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period, and at the lowest cost to them and their community’’. The irrational use of drugs on the other hand leads to the prolongation of illness, development of adverse effects, inefficient allocation of limited resources, and unnecessary expense.1–3 One possible mechanism for lowering expenditure on medicines is prescribing and dispensing generic drugs. In favor of this fact, different local and international organizations and different studies recommend prescribers to prescribe medicines by their generic names rather than brand names.3–8
Generic drugs are drugs produced after an innovator drug following the expiry of the patent of the company that produced it. Generic drugs will be sold under different brand names and are not exactly the same in look, color, taste, and shape as the brand name drugs for purpose of branding. Generic drugs contain the same quality active ingredients as the brand name drug and they should have equivalent safety, effectiveness, dosage, safety, strength, stability, and quality as that of the original innovator brand drug as all drugs must comply with strict directives and supervision of the Food and Drug Administration (FDA) in the US and equivalent institutions in other countries.9,10
World health organization strongly recommends the use of the generic (nonproprietary) name of medicines for prescribing. Among the mentioned reasons are generic prescribing enhances adherence to medication by improving access to medicines at relatively low cost, facilitates education and information, doesn’t allow prescribers to express their opinion about a particular brand of the drug, and enable pharmacists to maintain a more limited stock of drugs, or dispense the cheapest drug. 4 Groups who are pro-generic prescribing also suggest generic prescribing results in competition among generic manufacturers that reduce prices of medicines in addition to mentioning the fact affordable price encourages good patient compliance, which improves treatment outcome and protects against the emergence of drug resistance.4,11,12
Prescribing drugs by brand names, which is prescribing medicines other than their international non-proprietary name (INN), should be discouraged because it is expensive (accounting for half of all prescriptions and 80% of the billions of US dollars spent on them). Because of its increased cost brand prescribing affects patients’ affordability and their by treatment compliance and treatment outcome. The US Department of Health and Human Services estimated, dispensing generics instead of all branded drugs with generic equivalents in the Medicare Part D program, the program and its beneficiaries would have saved US$2.8 billion in 2016 alone.8,13
Another reason for discouraging use of brand names for drug prescribing is it may become a reason for cross-prescribing drugs with similar names, which creates unnecessary risk to the patient in addition to resulting expenditure for no potential benefit. 14
Although generic medicine prescribing is suggested to minimize expenditure on medicines, prescribing drugs by their brand name appears to be more prevalent than ever. 14 Studies indicated physicians from high-income countries have positive views whereas those from low and middle-income countries have mixed views regarding generic medicines. 15
Different factors were identified to affect the decision of physicians to prescribe drugs by brand or generic names. Some of the factors identified in studies include prescribers’ lack of awareness about the cost of medicines, patients’ lack of awareness of generic medicines, knowledge of prescribers about generic products, the attitude of prescribers towards safety and effectiveness of generic products, getting different types of incentives in cash or in kind from pharmaceutical companies and pharmaceutical industry.16–33
International organizations and regulatory bodies like WHO and FDA encourage generic prescribing.3–8,34 Many countries of the world including Ethiopia have made generic prescribing and generic substitution part of their health policy to discourage brand prescribing.3,7,12 As one indicator of pro-generic drug use, the Ethiopian government in its 2015 health sector development plan introduced the vision to increase the proportion of essential drugs procured from local manufacturers from 25% to 60% in 2020. 35 The AA City Health Bureau (AACHB) disseminated letters to hospitals and sub-cities asking physicians to prescribe drugs by their generic names. However, looking at patients and caregivers searching for medicines written by brand name is common in AA, which not only consumes the time of patients and caregivers but it also poses a threat to cost-effective medicine distribution and availability in the city.
Even though generic drugs are less costly and have equivalent effectiveness in disease treatment, our experience shows prescribing drugs by their brand name is common in AA. A letter written by AACHB to sub-cities and hospitals requesting physicians not to prescribe drugs by brand names for community-based health insurance users in part evidences the commonness of brand prescription in AA.
Even though problem of brand medicine prescribing is common in AA, there are no studies conducted in city that indicate the magnitude of the problem and the different factors affecting it. In addition, study reports from different parts of the world are not consistent regarding both the magnitude of the problem and the factors associated with it. Therefore, this study tried to examine the magnitude and associated factors of prescribing drugs by their brand names among prescribers in selected hospitals of AA.
Objectives
General Objective
The general objective of this study was to assess the magnitude and associated factors of brand drug prescribing practice among prescribers at selected hospitals in AA, Ethiopia.
Specific Objectives
• To assess the magnitude of prescribing drugs by their brand names among prescribers working at hospitals in AA in the study period. • To determine the factors associated with prescribing drugs by their brand names among prescribers working at hospitals in AA in the study period.
Methods and Materials
Study Area
This investigation was carried out in selected hospitals of AA. The study was carried out in AA because the city is showing indicators of the problem, but neither its size nor its root cause have been proven by studies. Given that the city is the largest in the nation and is home to the majority of the nation’s medical facilities and professionals, it was anticipated that the study’s findings would shed light on the severity of the issue there and serve as a starting point for a study of the issue at the national level.
The city serves as both Ethiopia’s and the regional state of Oromia’s capital. The city’s population was expected to be 2,739,551 people in the 2007 census. 36 The city, which is the largest in the nation, is also the nation’s most developed and significant center for the arts, finance, and culture. 37
There are 15 public hospitals in the city, according to AACHAB officials. AACHB is in charge of six of them. They include the Tirunesh Beijing Hospital, Menilik II Hospital, Yekatit 12 Hospital, Zewditu Memorial Hospital, Ghandi Hospital, and Ras Desta Hospital. Black Lion Hospital, St Paul’s Hospital Mellenium Medical College, AABET Hospital, St. Peter Hospital, Ethiopian Armed Forces Hospital, Police Hospital, Amanuel Hospital, Ekakotebe Hospital, and Alert Hospital are among the additional public hospitals. 38
Data from AA City food and drug administration (AAFDA) indicated the city has 21 private hospitals. These are Afran Hospital, Legahar General Hospital, Teklehaymanot General Hospital, Amin General Hospital, Tezene’a Hospital, Bethezatha Hospital, Grum Hospital, Zenbaba Hospital, Kadisco Hospital, Hallelujah General Hospital, Addis General Hospital, EthioTebib Hospital, Hayat Hospital, St. Yared Hospital, Myungsung Christian Hospital, Genet General Hospital, Bethel Hospital, Yerer Hospital, Silkroad Hospital, LandMark General Hospital, St. Gebriel Hospital, and Addis Hiwot Hospital. 39
There were a total of 2427 physicians, 4944 nurses, 635 midwives, 589 pharmacy professionals, 606 laboratory professionals and 237 anesthesia professionals in government hospitals of AA(38). On the other side there were 323 physicians, 1125 nurses, 140 midwives, 137 pharmacy professionals, 176 laboratory professionals and 71 anesthesia professionals working in private hospitals of AA(39).
Study Period
The study was conducted from May 1 to July 31 /2022 G.C.
Study Design
The design of this study was institution based cross sectional study.
Population
Target Population
The target population for this study was all prescribers (physicians, anesthetics, and dentists) working in AA during the study period.
Source Population
The source population for this study was all prescribers working at selected hospitals of AA during the study period.
Study Population
The study population for this study was all prescribers working in selected hospitals of AA and included in this study.
Inclusion and Exclusion Criteria
Inclusion Criteria
This study comprised prescribers who had worked on the selected hospital for at least 6 months, were able to complete the questionnaire, and were permanent hospital workers.
Exclusion Criteria
Those prescribers who were not directly involved in prescribing (such as radiologists), those prescribers who were employed by the hospital but were not actually working there as clinicians, and those who had any open business relationships with pharmaceutical companies were omitted from this study.
Health officers were also excluded from this study despite being prescribers because they were majorly supposed to work in health centers and their number in hospitals is very limited.
Sample Size and Sampling Technique
Sample Size
The sample size for this study was calculated by using both single population proportion formula for the magnitude of brand prescribing and the formula for estimating difference in two proportions for the associated factors. Out of the two formulas, the one that produced the larger sample size was used for the final study.
For single population proportion the following formula was used to calculate the sample size by taking p value of 28% (prevalence of prescribers who prescribe drugs by their brand names).
29
, using a 95% confidence interval (z = 1.96) and margin of error of 5 %.
n – Sample size
Zα/2 – The standardized normal distribution value at the 95% confidence interval level (1.96)
p – The prevalence of physicians who prescribe drugs by their brand names in Mekelle study entitled factors affecting physician’s adherence to generic drug prescribing practice in private health facilities, Mekelle city, northeastern Ethiopia
D – The margin of error taken as 5%
The calculated sample size was 308
For estimating difference in two proportions (like magnitude of practice of prescribing medicines by brand names on those working on public and private institutions, magnitude of the practice on those who were knowledgeable about generic drugs and those who were less knowledgeable about generic drugs and other factors) the following formula was used to calculate the sample.
Where; n = sample size
Z = the standardized normal distribution value at the 95% confidence interval level (1.96)
D = the margin of error taken as 5%
Q1 = 1-p1
Q2 = 1-p2
Out of the different factors that were found to affect brand prescribing habit, we considered only the sector the prescriber was working (private or public) to calculate sample size as we didn’t get clear information about prevalence of brand prescribing habit among the different groups who had difference in work experience, post graduate study, knowledge about prescribing, attitude towards generic prescribing and others.
For the sector the prescriber was working we selected finding from Philippines study where P1 (prevalence of brand prescribing habit among prescribers working in public sector (10%)) and P2 (prevalence of brand prescribing habit among prescribers working in private sector (19.07%)). 22 The sample size obtained was 368
The larger sample size from the two (368) was taken to get the final sample size. Because the number of prescribers in hospitals of AA (N) was less than 10, 000 (it was 2750), sample size adjustment formula for finite population was considered.
Where: n0 is the sample from an infinite population.
Using the formula the final sample size was obtained to be 326
As there was multistage sampling, the obtained sample size was multiplied by 1.5 in consideration of design effect. Finally, 10% adjustment was considered for non-response rate and final sample size was 538 (326*1.5 + 49).
Sampling Technique
A total of six out of the 21 private hospitals (Ethiotebib hospital, Afran Hospital, Teklehaymanot General Hospital (TGH), Amin Hospital, MyungSung Christian Hospital, Bethezatha Hospital) and three out of the 15 public hospitals (Saint Paul’s Hospital Millennium Medical College, Minilik II Hospital, Ethiopian Armed Forces Hospital) were included in this study. The hospitals included in the study were clustered in to private and public hospital. Included hospitals were identified by simple random sampling technique. The total sample was proportionately divided to the private and public hospitals based on the total number of prescribers in each sector. The total sample allocated both to public and private hospitals were further proportionately divided to each hospital based on total number of prescribers in each hospital. After reaching the hospital the total sample allocated to that specific hospital was further proportionately divided to each department in the hospital based on total number of prescribers in each department. The list of prescribers in each department of the hospitals was used as a sampling frame and the total number of allocated prescribers from each department was obtained by systematic random sampling technique after getting the first sample by simple random sampling technique (Figure 1). Schematic presentation of the sampling in AA from May to July/2022.
Study Variables
Dependent Variable
Prescribing drugs by their brand name.
Independent Variables
Sociodemographic variables (like age, sex, marital status, monthly income, educational status), work experience as a prescriber, specialty, visit by pharmaceutical company promoters, loyalty of prescriber to brands from specific drug manufacturers, knowledge about generic medicines, attitude towards generic medicines, perception of prescriber towards effectiveness of brand drugs, perception of prescribers about cost of brand drugs, perception of prescriber about safety of brand drugs, perception of prescriber about availability of drugs, major factor considered by prescribers while prescribing drugs other than the safety and efficacy of drug, the level of trust the prescriber had on EFDA.
Operational Definition
Prescribing drugs by their brand names: Prescriber who always, often and sometimes prescribe drugs by their brand names in the last 6 months.
Brand names of drugs: all names of drugs other than the international non-proprietary names of drugs.
Knowledgeable about generic drugs: study participant was considered knowledgeable about generic drugs when correctly answers 50% or more of the 11 knowledge questions.29,40
Positive attitude towards generic drugs: study participant who had scored more than or equal to the mean of mean Likert scale score to the 10 attitude questions.29,40
Prescriber was considered to have confidence on EFDA when he/she agree or strongly agree to the statement ‘I have belief that EFDA adequately checks fulfillment of safety and efficacy of generic drugs before import and marketing of drugs’.
Prescriber was considered to be loyal to brand when he/she agree or strongly agree to the statement ‘I mostly prescribe medicines produced from certain factories’
Prescriber was considered to think drugs were expensive commodities when he/she strongly agree or agree to the statement ‘drugs are expensive commodities for most segments of the AA population’.
Prescriber was considered to think drugs were easily available commodities when he/she strongly agree or agree to the statement ‘drugs are easily available commodities’.
Prescriber was considered to think generic drugs were as effective as brand drugs when he/she strongly agree or agree to the statement ‘generic drugs are as effective as brand drugs’.
Prescriber was considered to think generic drugs were as safe as brand drugs when he/she strongly agree or agree to the statement ‘generic drugs have similar safety profile as that of brand drugs’.
Data Collection Tools and Procedure
Data was collected using semi-structured self administered questionnaire which was developed by the investigator using other related studies as a base.20,21,27,29,31,41–43 The questionnaire used had four parts. The first part of the questionnaire addressed sociodemographic characteristics of respondents. The second part was about questions related to brand drug prescribing and reasons for brand prescribing. The third and the fourth parts were knowledge about generic drugs and attitude towards generic drugs, respectively.
Four data collectors who had BSC degree in pharmacy and with good communication skill were recruited for data collection. One day training was given by the investigators to the data collectors and supervisors on how to approach and communicate with the selected prescribers.
Knowledge about generic drugs was measured by asking knowledge questions obtained from other similar studies and marking the response correct and incorrect. Attitude towards generic drugs was measured on a five-point Likert scale (strongly disagree, disagree, neutral, agree and strongly agree).
Data Quality Control
The data collection tool which was prepared in English language was pre-tested for its accuracy, completeness, and consistency prior to the actual data collection on 5% of the sample population at TikurAnbesa Hospital and Kadisco Hospital and the necessary adjustments was made to the questionnaire following the pretest. Furthermore, two supervisors who had MSc degree and good experience in conducting research were recruited. The supervisors observed and gave feedback to the data collectors on daily bases. Completeness, accuracy, and clarity of the collected data were checked carefully by the supervisors and the investigators and any error was addressed.
Data Management and Analysis
Data was cleaned, coded and entered to statistical package, IBM®SPSS® Statistics, version 25. The data was described using percentages, graphs and tables. Mean and standard deviations were calculated to identify measures of central tendency and dispersion. Bi-variate analysis was employed to see the crude association between the independent and dependent variable. Multivariate analysis using multiple logistic regression technique was done to evaluate independent effect of each variable on brand drug prescribing by controlling the effect of other variables. The strength of association between dependent variable and independent variables (covariates) were expressed by adjusted odds ratio with 95% confidence interval. Statistical significance was declared at 95% confidence interval and p
Ethical Clearance
The proposal was reviewed for any unethical issues by the ethical review board of Saint Paul’s hospital millennium medical college (SPHMMC) and ethical review board of selected hospitals. Permission to conduct the study was obtained from selected hospitals. Participants’ information like name and address was not recorded and coding was used in the questionnaires. All data was kept confidential and used only for the purpose of this research. Written consent was obtained and all participants were clearly informed that they had the right not to participate if they were not willing. The right of those individuals who wanted not to participate even after the data collection was protected.
Results
Sociodemographic Characteristics
This study intended to include a total of 538 study participants. A total of 485 of them completed and returned the questionnaire, yielding a 90.2% response rate. Although 53 study participants got the questionnaire to complete, they were not taken into account in the data analysis step. Thirteen of them made the suggestion of leaving AA for a longer time, while the other 40 did not answer calls that were made repeatedly
Sociodemographic characteristics of study participants in AA from May to July; 2022 (N = 485).
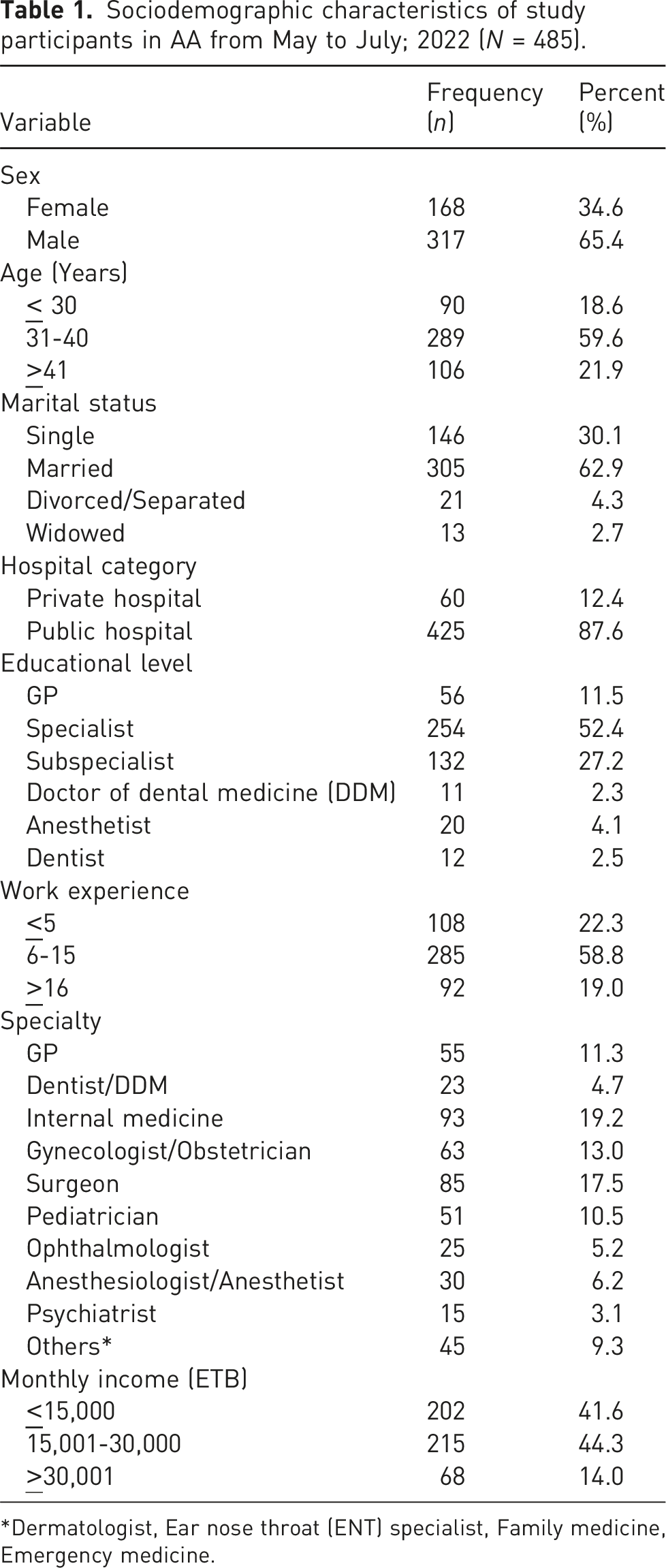
*Dermatologist, Ear nose throat (ENT) specialist, Family medicine, Emergency medicine.
Considerations by Prescribers while Making Prescribing Decision
This study found that, in addition to drug safety and effectiveness, the availability of the drug (166(34.2%)) and its cost (140(28.9%)) were the two main considerations for prescribers when making prescription recommendations (Figure 2). The major factor the prescriber considered while prescribing drugs other than the safety and efficacy of the drug in AA from May to July; 2022 (N = 485).
This study found that more than three-fourths (422(87.0%)) of prescribers thought that the rising cost of medications was a serious problem for the health sector’s budget. In addition, this survey found that 349(72.0%) of prescribers had never received training in effective prescribing practice after graduating.
Visit of Prescriber by Pharmaceutical Company Promoters and Obtained Benefits
This study found that in the previous year, pharmaceutical company representatives contacted 326 (67.2%) of survey participants. Three hundred sixty one (74.4%) of prescribers said they had benefited in some way from pharma companies over the previous year.
Items (such as pens, books, gowns, and watches) and free meals at hotels, in addition to the aforementioned items, were the main benefits gained among individuals who acknowledged receiving at least one form of benefit (Figure 3). Types of benefits obtained from pharmaceutical companies in AA from May to July; 2022 (N = 361).
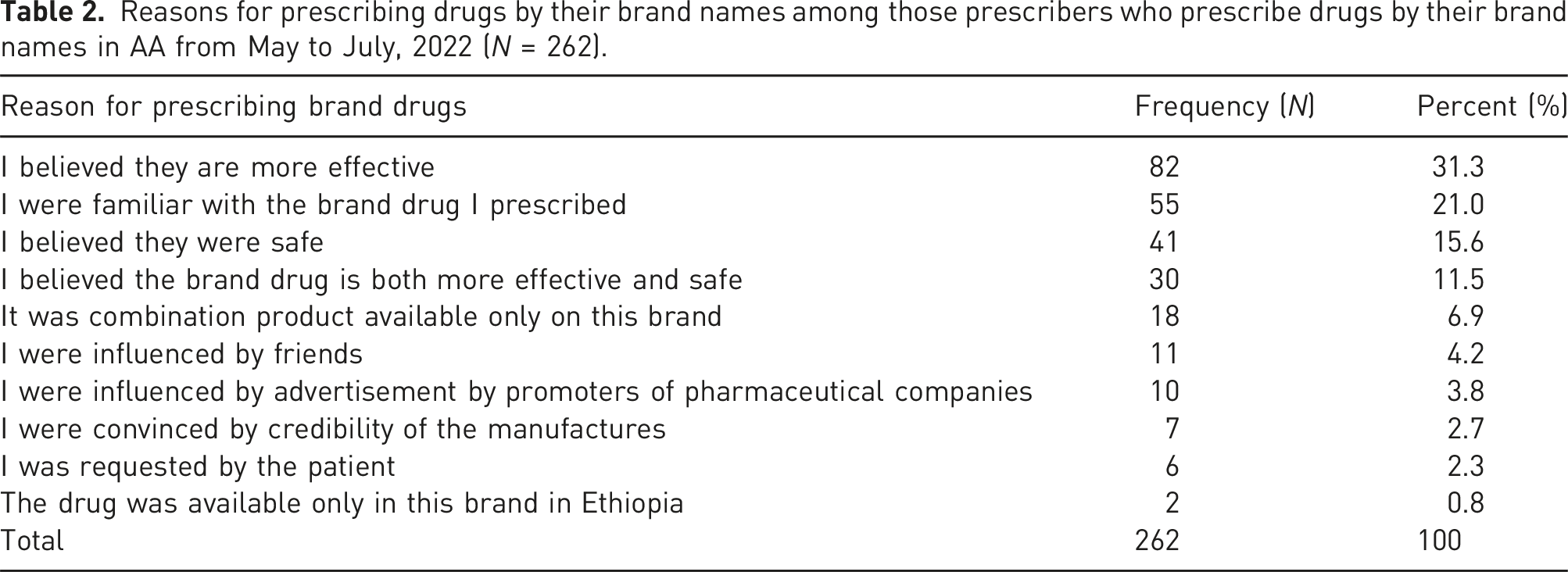
Brand Drug Prescribing and Mentioned Reasons for Brand Prescribing
According to this study’s findings, two hundred sixty two (54.0%) of prescribers use the brand names of the medications they were prescribing in the past 6 months. The rest prefer the generic names of medications while prescribing.
Among those prescribers who prescribe drugs by their brand names (190(72.5%) do so only sometimes. Fifty-seven (21.8%) often use brand names while prescribing. The remaining 15 (5.7%) always prefer the brand names of drugs while prescribing.
Reasons for prescribing drugs by their brand names among those prescribers who prescribe drugs by their brand names in AA from May to July, 2022 (N = 262).
Reasons for not prescribing drugs by their brand names among those prescribers who didn’t prescribe drugs by their brand names in AA from May to July, 2022 (N = 223).

The three most often prescribed pharmacologic classes of drugs by their brand names were antibacterial medications (69(26.0%)), analgesics (57(21.7%)), and glucocorticoids (22(8.5%)) (Figure 4). Pharmacologic class of drugs prescribed by brand names among those prescribers who prescribe drugs by their brand names in AA from May to July, 2022 (N = 262). * Alpha blockers, prostaglandin analogues, sex hormones, antihistamines, antithyroid drugs, benzodiazepines, antipsychotics, antifungal drugs, sunscreens, tricyclic antidepressants, selective serotonin reuptake inhibitors, local anesthetics, vasodilators, ketamine, anticholinergics, angiotensin converting enzyme inhibitors, antiplatelets, Oxytocin.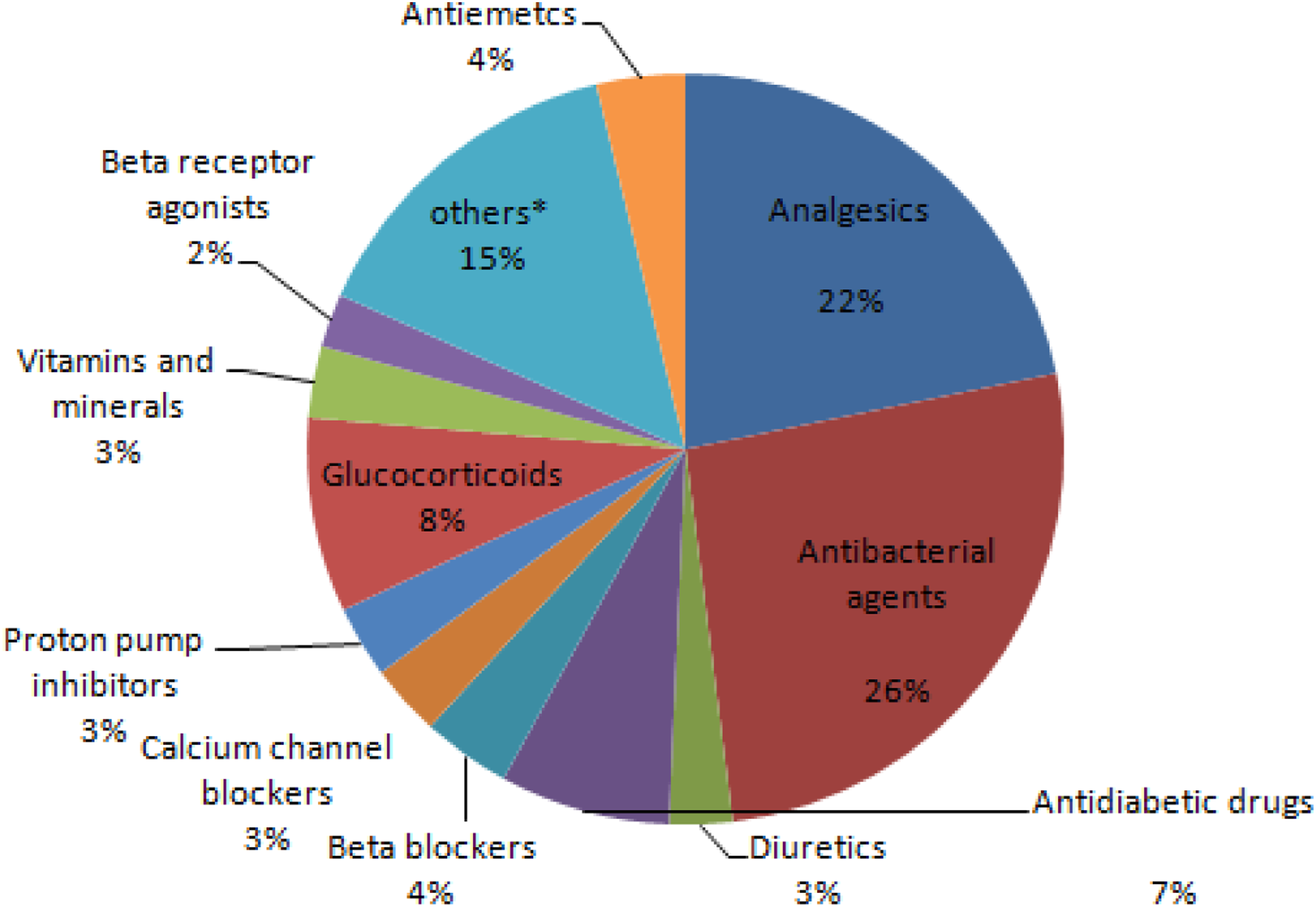
Trust in EFDA, Brand Loyalty, Drug Availability and Cost, Safety and Effectiveness of Generic Drugs
Response of study participants to statements related to trust in EFDA, loyalty to brand, view about cost of drugs and belief on effectiveness and safety of generic drugs in AA from May to July; 2022 (N = 485).

Knowledge and Attitude towards Generic Drugs
The response of study participants to knowledge questions in AA from May to July; 2022 (N = 485).

In this study, 244(50.3%) of study participants were judged to be not knowledgeable about generic pharmaceuticals since they could not accurately answer at least 50% of the knowledge questions. The remaining 241(49.7%) correctly answered at least 50% of the knowledge questions and were considered to be knowledgeable about generic drugs.
Rating of study participants to attitude questions in AA from May to July;2022 (N = 485).

About half (245(50.5%)) of study participants had scored mean attitude score of equal to or more than the mean of mean attitude score and were considered to have positive attitude towards generic drugs. The rest 240 (49.5%) had a mean attitude score of less than the mean of mean attitude score and were considered to have negative attitude towards generic drugs.
Factors Affecting Brand Drug Prescribing
Model logistic regression was checked to identify the different factors affecting prescribing drugs by their brand names.
The results of binary logistic regression analysis revealed presence of association between the practice of prescribing drugs by their brand names and variables like hospital category, sex, educational level, prescriber specialty, monthly income, and the main considerations the prescriber takes into account when making a drug recommendation in addition to the medication’s safety and effectiveness. Getting benefits from pharmaceutical companies, trusting that EFDA checks the safety and efficacy of generic drugs, brand loyalty, belief in effectiveness of generic drugs in comparison to brand drugs, belief in the safety of generic drugs, receiving training on proper prescribing techniques, considering the rising cost of drugs as a serious problem for the health sector budget, getting benefits from pharmaceutical companies, knowledge about generic drugs, and attitude towards generic drugs were other factors that have shown association to brand prescribing on binary logistic regression analysis.
Factors affecting prescribing drugs by their brand names in AA from May to July; 2022 (N = 485).

**Dermatologist, family medicine, emergency medicine, ENT (Ear Nose Throat) specialist.
*There is statistically significant association.
According to this study, those study participants who didn’t consider the increasing cost of drugs as a serious problem for the health sector budget were 8.67 times more likely to prescribe drugs by their brand names than those who believed the increasing cost of drugs as a serious problem to the health sector budget (AOR = 8.69; 95%CI:1.79-42.17).
Those study participants who didn’t receive training about good prescribing practice after their graduation were 6.81 times more likely to prescribe drugs by their brand names than those who were trained after their graduation (AOR = 6.81;95%CI:2.08-22.28).
Those study participants who had no trust in EFDA in checking the safety and efficacy of generic drugs before their import and marketing were 18.18 times more likely to prescribe medications by their brand names than those prescribers who had trust in EFDA (AOR = 18.18;95%CI:6.78-48.80).
This study revealed study participants who were not knowledgeable about generic drugs were 11.86 times more likely to prescribe medications by their brand names than those who were knowledgeable (AOR = 11.86;95%CI:4.76-29.55).
This study further indicated prescribers who had negative attitude towards generic drugs were 19.79 times more likely to prescribe drugs by their brand names than those who had positive attitude (AOR = 19.79;95%CI:1.52-255.94).
Discussion
Replacement of more expensive brand-name drugs with their generic counter parts while prescribing is considered one of the most effective ways to reduce the financial burden of patients and their families on drug expenditures. This approach is rational because generic drugs pass under the same regulatory and testing standards as that of brand drugs and thus, share the same effectiveness, safety, and adverse effect profile as their brand-name counterparts. Even though generic prescribing is known to improve the effective utilization of healthcare resources and has an impact on improving drug compliance among patients, this study revealed generic prescribing is very low in AA.
This study revealed the prevalence of prescribing drugs by their brand names in AA was 54.0%. This finding is higher than findings from Jordan, Philippines, Saudi Arabia, Srilanka, Tanzania, Hawassa, Jimma, and Mekelle where the prevalence of generic prescribing was 77.4%, 83.3%, 72%, 89.9%, 85.5%, 98.7%, 75.2% and 72%; respectively.22,29,31,41,44–47 In contrast, the prevalence obtained in this study was lower than findings from Armenia, USA, Tanzania, Greece, and Nepal where the prevalence of prescribing drugs by their brand names was 82%, 68%, 71.6%, 70.8% and 97.1%; respectively.16,42,48–50 The reasons for these variations may be differences in study population, method of data collection, differences in health policies of the countries, differences on the emphasis given about brand prescribing on medical curricula of the countries and definitions of brand prescribing. The findings from Jimma, Hawassa and Mekelle are lower than this finding because these studies were prescription audits majorly from government health institutions and they might not show the real magnitude of the problem.
The major reasons mentioned for prescribing drugs by their brand names in this study were believing brands were more effective than generics, being familiar with the prescribed brand and believing brand drugs were more effective than generic drugs. This demonstrated the enormous amount of work required to increase prescribers’ awareness of generic medications and their attitude toward prescribing generic medications. In a research conducted in the Philippines, comparable justifications, such as worries about quality, personal experience, a lack of regulatory oversight, and a preference for prescription medications by their brand names, were highlighted. 22
Those prescribers who prefer generic prescribing mentioned reasons like believing generic pharmaceuticals were just as safe and effective as brands, thinking brand drugs were more expensive than generics, and desire to follow established national treatment recommendations for generic prescribing. This gives a hint about working on knowledge on generic drugs and trials to implement the national health policy might improve generic prescribing. This finding is almost identical to the one from Mekelle, where adherence to generic prescribing was mostly cited as a result of trusting the quality, accessibility, and affordability of generic medications. 29
About half (49.7%) of study participants in this study were knowledgeable about generic drugs. This finding is almost similar to a finding from Pakistan where 53.0% were knowledgeable about generic drugs. 51 In contrast, the knowledge score about generic drugs obtained in this study was lower than a finding from Jordan where 64.3% of study participants had satisfactory knowledge about generic drugs. 31 The reasons for these differences might be differences in the operational definition of being knowledgeable about generic drugs, differences in study subjects, and study setting.
Contrary to a study conducted in Pakistan, where highly experienced and older people prescribed pharmaceuticals by their brand names more frequently than those with less experience, this study found no correlation between job experience and the prescription of brand-name drugs. 51
Similar to a Sri Lankan study where there was no correlation between working in the private sector and brand prescription prescribing, this study found no relationship between the prescriber’s hospital sector of employment and brand medicine prescribing. 41 In contrast to working in public hospitals, studies from Jordan and the Philippines found a favorable correlation between brand drug prescribing and involvement in the private sector.22,31
This study found no correlation between a promotional visit from a pharmaceutical corporation and the prescription of products by their brand names. Also, there was no correlation between prescribing medications by their brand names and receiving any kind of advantage from pharmaceutical corporations. This result differs from one from the USA, where payments for educational training were linked to a 4.8% rise in the rate of brand-name prescribing and brand-name prescribing increased by 0.1% for every US$1000 in total payments received. 28 In this study, prescribers may have been more prone to provide a response that was seen acceptable by society due to Ethiopia’s health system’s ban on brand prescriptions.
This study’s findings indicate that training in effective prescribing practices after graduation increased the prescribing of generic drugs while decreasing the prescribing of brand-name medications. The training may improve prescribers’ awareness of generic medications and change their attitudes toward prescribing them, which could be the cause of this.
This study found that participants who did not trust the EFDA to examine the safety and efficacy of generic medications were more likely to prescribe medications by their brand names than those who did, out of concern that the safety and efficacy of generic medications were not adequately monitored. Findings from the Philippines and Sri Lanka, where worries about the quality of medicines were linked to more brand-drug prescribing, reinforce this.20,22 The Philippines study explicitly suggested brand medicine prescribing is positively impacted by regulatory body inaction. 22
This study showed no significant association between brand loyalty and brand drug prescribing in contrast to the Srilanka study where there was a positive association between brand loyalty and brand drug prescribing. 20 The reason for this difference might be the majority of prescribers (83.3%) claimed they were not loyal to a brand and those who were loyal might not be adequately represented.
This study discovered a significant link between prescriptions for generic medications and knowledge of those medications. Similar to this, a study from Armenia found that being knowledgeable about generic drugs increases the likelihood of prescribing them while lowering the likelihood of prescribing brand-name drugs. 42
This study also showed that prescribing of brand-name drugs was substantially correlated with negative attitudes toward generic drugs. This is also corroborated by a study finding from Armenia, where prescriptions for generic medications were lowered due to misguided perceptions, while prescriptions for brand-name medications increased. 42
This study has limitations. The potential that respondents gave socially acceptable answers and the incidence of recall bias were among the study’s limitations. Additionally, because of the cross-sectional nature of this study and the lack of a temporal link between the covariates, it is impossible to deduce causation. Nevertheless, the present study has also strengths. The fact that we used the right sampling methodology and enough sample size to represent AA prescribers working in hospitals is one of the study’s strengths. In order to reduce biases, the data was evaluated using appropriate statistical methods and tests. In addition, this study was the first of its kind to be conducted among prescribers of the city.
Conclusion
Based on the result of the study the following conclusions were drawn.
Prescribing drugs by their brand names is high in AA in relation to both the WHO’s and the nation’s health policy standards.
Prescribing medications by their brand names is less likely to occur if the prescriber considers the rising cost of drugs as a serious issue for the health sector budget.
Getting training about good prescribing practices after graduation decreases the probability of prescribing drugs by their brand names. Additionally, having adequate trust on EFDA in monitoring the safety and efficacy of generic pharmaceuticals makes prescribing drugs by their brand names less likely.
This study further indicated being knowledgeable about generic medications and having a favorable attitude toward them increased the likelihood of prescribing generic medications rather than brand-name medications.
Footnotes
Acknowledgements
We like to thank all prescribers who participated in the study. Our sincere gratitude also goes to the administrators of the institutions included in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.